
Abstract
This study aimed to determine the quality of life of family caregivers of patients with leukemia and the factors contributing to it. The RAND 36-Item was used to collect data from 152 caregivers. The mean scores of six dimensions of Quality of life (QoL) were low, indicating a limited health state. Caregivers’ educational level, age, number of admissions, time since diagnosis, relationship with the patient, and family income significantly predicted the caregivers’ QOL. This study confirms the need for ongoing interventions to improve caregivers’ quality of life. Particular attention should be paid to older caregivers, who have low education, are from a low socioeconomic background, and care for the patients for a long time. Oncology nurses must ensure that family caregivers receive the appropriate support and resources to care for their patients at home and to assess the areas of need to achieve a better quality of life for patients and their caregivers.
Keywords
The cancer diagnosis presented a significant crisis to the patient and the patient’s primary family caregiver. The involvement of family caregivers was essential for cancer treatment, ensuring the continuity of care, treatment compliance, and social support. Family caregivers usually assumed this role under extreme and unexpected circumstances, with minimal guidance, preparation, and support from the healthcare system (Ovayolu et al., 2014). Quality of life (QOL) was a multidimensional concept, including functional ability, physical well-being, social well-being, and emotional well-being. The QOL involved how a person measured the “goodness” of multiple aspects of their life. These evaluations encompassed one’s emotional responses to life events, sense of life realization, disposition, and contentment with relationships and work (Theofilou, 2013).
The GLOBOCAN 2020 estimates indicated 19.3 million new cancer cases and almost 10 million deaths from cancer in 2020. In Jordan, the number of new cases of leukemia in 2020 for both sexes and all ages was 569/11,559, accounting for 4.9% (307 (5.8%) were males and 262 (4.2%) females). Leukemia was the number five most frequent cancer for both sexes. The mortality rate from leukemia was 6.3% (393/569). Moreover, the 5-year prevalence for all ages was 15,557 (15.27/100,000; Sung et al., 2021).
Family caregivers of patients with leukemia had impaired social, physical, environmental, and psychological health (Pathirana et al., 2015). They were more likely to have depression and poor mental health and experience limited social functioning and family conflicts than caregivers of patients with other types of cancers. They also had significant differences in employment before and after diagnosing leukemia with their relatives, with more caregivers losing their jobs (Pathirana et al., 2015).
Overall, caregivers caring for leukemia patients perceived a lower level of QOL (Deniz & Inci, 2015). A high prevalence of depression was found in cancer patient caregivers, and several factors may have affected depression and the quality of life of cancer patient caregivers (Geng et al., 2018). Also, family members of cancer patients were at an increased risk of medically diagnosed depression (Cho et al., 2018). In England, a national study found that psychological morbidity and general health levels among a census sample of carers of people with cancer at the end of life were far higher compared to population reference data (Grande et al., 2018).
Caregiver’s characteristics were key factors that influenced perceived QOL; for example, the gender of caregivers, the degree of relationship to the patient, low economic status, disruption of family life, and working status resulted in poor caregiver outcomes (Cho et al., 2018; Deniz & Inci, 2015). Moreover, patient characteristics significantly influenced caregivers’ QOL; patient age, their condition, and the presence of another disease were associated with caregiver QOL (Al Qadire et al., 2020; Deniz & Inci, 2015).
In a recent study, Al Qadire et al. (2020) conducted research among 264 parents of children with cancer in Jordan to assess Jordanian parents’ burden level and predictors. The results showed that 75.4% of parents experienced mild to severe burden levels. The perceived burden levels were affected by the characteristics of both parents and children, such as having a chronic disease, financial constraints, high levels of anxiety and depression, a child with advanced cancer, and a child experiencing pain, nausea, and vomiting.
The study by Pop et al. (2022) aimed to review the literature and identify factors that influence the quality of life of primary caregivers of palliative patients. The authors conducted a narrative review and analyzed the findings of 38 studies. The study found that the quality of life of primary caregivers of palliative patients is influenced by various factors, including the patient’s symptom burden, functional status, and disease stage. The caregivers’ physical health, mental health, and social support were also identified as significant factors. Other factors that were found to impact the caregivers’ quality of life included their relationship with the patient, financial burden, and caregiver burden. The study also highlighted the importance of healthcare professionals in providing support and interventions to address the needs of primary caregivers of palliative patients. Overall, the study concluded that a comprehensive approach is needed to improve the quality of life of primary caregivers of palliative patients, including addressing their physical, psychological, and social needs.
Several studies have investigated the factors that influence the quality of life (QoL) of cancer patients and their caregivers. Pierzynski et al. (2018) found that age, sex, education level, smoking status, stage of cancer, treatment type, and genetic variations in certain genes significantly influenced QoL in lung cancer patients. Clarijs et al. (2022) reported that the QoL of caregivers of breast cancer patients was significantly lower than the general population, with factors such as higher age, female gender, caring for a patient with advanced cancer, and longer caregiving duration negatively impacting QoL. Choi et al. (2016) found that family caregivers of terminally ill cancer patients had a significantly lower QoL, with the main factors negatively affecting their QoL being the patient’s physical and psychological symptoms, caregiver’s financial burden, caregiver’s depression and anxiety, and caregiver’s perception of a lack of social support. Gessner et al. (2020) reported that the severity of the patient’s cancer significantly affected the QoL of caregivers of bladder cancer patients. Ng et al. (2021) found that physical activity, confidence, and QoL were positively associated with cancer patient-carer dyads, and confidence mediated the relationship between physical activity and QoL. Finally, Santin et al. (2022) highlighted the negative impact of the COVID-19 pandemic on the mental and physical health, QoL, and support needs of cancer carers. Overall, these studies emphasize the importance of addressing the QoL of both cancer patients and their caregivers, considering various factors that influence QoL, and providing targeted support during times of crisis.
The study was conducted to address the gap in knowledge regarding the quality of life (QoL) of caregivers of patients with leukemia in Jordan, as there were no previous studies on this topic. Previous research in Jordan had primarily focused on the QoL of cancer patients, with only one study examining the burden of cancer patients on their caregivers (Al Qadire et al., 2020).
This study aimed to assess the Quality of Life (QoL) of family caregivers of patients with leukemia and identify the factors that contribute to it. The following research questions were addressed in this study:
RQ1: What are the quality of life scores in the eight domains of family caregivers of patients with leukemia?
RQ2: What factors related to caregivers and the patients can be used to predict the QOL of caregivers?
Methods
Sample and Setting
In this study, a cross-sectional, correlational design was employed to recruit 152 caregivers. The study was conducted at a specialized cancer center in Jordan, where caregivers of patients were approached in the oncology in-patient and outpatient departments. Caregivers were eligible to participate if they were primary family caregivers (males or females) for patients (adult or pediatric) with leukemia receiving treatment from the selected cancer center, were of Jordanian nationality, resided in the patient’s home, were able to communicate in Arabic, and able to provide written consent. Primary caregivers in this study were responsible for taking care of their patients, whether children, seniors, or spouses with leukemia, including monitoring their health, keeping track of their vitals, noting changes in their health, and reporting differences to healthcare providers, ensuring they took their medication, attended appointments, and kept in touch with their doctors. Only caregivers who responded to the survey and signed the consent form were approached.
The A-priori Sample Size Calculator was used to estimate the minimum required sample size for multiple regression. The desired probability level (.05), the number of predictors in the model (13), which were the socio-demographic variables of family caregivers (marital status, educational level, working status, place of residence, age, income, relationship to the patient, and gender), and the patients (age, gender, number of admissions, time since diagnosis, and co-morbidity), the anticipated effect size by convention (medium = 0.15), and the desired statistical power level (0.8) were taken into consideration. Based on these parameters, the minimum required sample size was estimated to be 131.
Instrument
RAND 36-Item Short-Form Health Survey (SF-36) 1.0 Questionnaire
The Arabic version of the self-reported questionnaire developed by RAND Health was used to collect data from family caregivers. The 36-item Short-Form Health Survey (SF-36) was employed to measure self-reported health-related quality-of-life (HRQOL). The SF-36 is a generic health survey designed for use in the general population (patients and providers; Ware & Sherbourne, 1992) and was a subset of questions from longer instruments used in the Medical Outcomes Study (Hays et al., 1993). It consisted of 36 questions that covered eight health domains and two summary physical and mental component scores (PCS and MCS). These eight scales were “physical functioning (PF),”“bodily pain (BP),”“role limitations due to physical health problems (RP),”“role limitations due to personal or emotional problems (RE),”“general mental health (MH),”“social functioning (SF),”“energy/fatigue or vitality (VIT),” and “general health perceptions (GHP).” These eight SF-36 Scale Scores were scored from 0 (low) to 100 (high).
This instrument was validated and reliable in assessing QOL among Arab patients and caregivers (Ahmed et al., 2017; Shdaifat & Manaf, 2012). The previous study among the Arab population demonstrated high reliability (α = .72–.90) across the eight subscales (Sheikh, 2013). The Cronbach α for the current study was also high (.85–.93) across the eight domains. Most of the previous studies that examined the reliability of the SF-36 exceeded .80, and reliability in the physical and mental sections was above .90 (McHorney et al., 1994; Ware et al., 1993).
Scoring
The data obtained from the family caregivers were scored using the RAND 36-Item Health Survey, which was a two-step process. In the first step, the numeric values were recoded according to the scoring key for each scale, with each item scored on a scale of 0 to 100, where the lowest and highest possible scores were 0 and 100, respectively. In the second step, items in the same scale were averaged together to create the eight scale scores. Scores for each domain ranged from 0 to 100, with a higher score indicating a more favorable health state (Hays et al., 1993).
It was found that the SF-36 could not be used as a single index of overall health-related QOL because it measured two dimensions (physical and mental; Lins & Carvalho, 2016). According to the original instructions by Ware and Kosinski (2001), the summary scores (PCS and MCS) should always be compared with the eight-scale scores before drawing conclusions. However, the method used to derive the MCS and PCS scoring coefficients had been criticized, particularly when using the orthogonal model, which resulted in negative coefficients for some scales. In our study, we used the eight-scale scores to measure the QOL for family caregivers.
Socio-Demographic Variables
The researchers developed a socio-demographic sheet that included data about the caregivers (gender, marital status, working status, age, education level, place of residence, and family income) and patients (age, gender, the period since diagnosis, the number of hospital admissions in the last month, and the presence of another chronic disease (co-morbidity).
Data Collection Procedure
The study obtained approval from the research committee on human research at the authors’ institution and the cancer center. Additionally, permission was obtained from the managers of outpatient clinics and in-patient wards before data collection commenced.
Data was collected from caregivers in a private room. Each family caregiver was asked to sign an informed consent form after the purpose of the study was explained to them in both written and verbal formats and then given a questionnaire to complete in their spare time. Participants were asked to complete the questionnaire and place it in a box left in the room. The researcher conducted face-to-face interviews with participants who could not read and write. The patient characteristics were obtained from the patient record system.
Ethical Considerations
Approval was obtained from the IRB at the authors’ institution and the cancer center (No. 37/105/2017, research no. 194/2017). Participants who agreed to participate in the study were asked to sign a consent form and complete a QOL questionnaire. Participants were assured that their participation would be entirely voluntary and that their responses would remain confidential.
Data Analysis
The data were analyzed using the Statistical Package for Social Science (SPSS) SPSS®-PC version 25 for Windows. Descriptive statistics (frequencies, means, and standard deviations) were used for each item to describe the sample characteristics and the distribution of responses. Multiple linear regression analysis was performed to investigate the impact of participants’ variables (marital status, educational level, working status, place of residence, age, family income, relationship to patient, and gender) and patients’ variables (age, gender, number of admissions, period since diagnosis, and co-morbidity) on the total QOL score. A significant value was set at p < .05.
Results
Characteristics of the Participants
Table 1 displays the demographic characteristics of family caregivers. A total of 152 family caregivers participated in this study. Of 152 family caregivers, 40.8% (n = 62) were males, and 59.2% (n = 90) were females. The mean age was 37.73 years (SD = 8.60) and ranged from 20 to 59 years old. About 25% (n = 38) of caregivers were single, and 75% (n = 114) were married. More than half (54.6%, n = 83) of the caregivers had current jobs. According to the caregivers’ relationships with the patients, 41.4% (n = 63) were mothers, 14.6% (n = 25) fathers, 19.1% (n = 29) brothers, 11.2% (n = 17) sisters, and 11.8% (n = 18) others (i.e., son, daughter, wife). The total monthly family income ranged from 300 to 2,000 JD ($423–$2,820).
Characteristics of Family Caregivers (N = 152).

Characteristics of Patients
Patients’ ages ranged from 20 to 59 years old (M = 22.36, SD = 15.32), 69.7% (n = 106) of the patients were males, and 30.3% (n = 46) were females, the time since diagnosis ranged from 1 to 3 years (M = 1.79, SD = 0.66). The number of hospital admissions in the last month ranged from 0 to 7 (M = 1.97, SD = 1.013). About 59.2% (n = 132) of the patients had no other diseases than leukemia, and 13.2% (n = 20) reported having other diseases (Table 2).
Characteristics of the Patients (N = 152).

The Quality of Life for Family Caregivers
Table 3 shows the means, standard deviations, and ranges for family caregivers’ quality of life scores in the eight domains compared to the data from the baseline medical outcomes study (MOS). It was found that only the mean scores of physical functioning (PF; 70.66 vs. 70.61) and bodily pain (BP; 75.20 vs. 70.77) were high compared to the results of MOS. Indicated a good health state. However, all other dimensions (RP, RE, MH, SF, VIT, and GHP) have low mean scores compared to the data from MOS, which indicated a limited health state.
Means, Standard Deviations, and Range of the Scores for Caregiver’s Quality of Life Domains (N = 152) Compared to Baseline Data from the Medical Outcomes Study.

Data is from the baseline of the Medical Outcomes Study (N = 2,471).
Predictors of Caregivers’ QOL
Stepwise Multiple linear regression was conducted to examine factors predicting the QOL of the family caregiver. Each of the eight domains of QOL (PF, RP, RE, VIT, MH, SF, BP, GHP) was regressed on demographic variables of the caregivers (marital status, educational level, working status, place of residence, age, income, relationship to the patient, and gender), and patients (age, gender, number of admissions, time since diagnosis, co-morbidity; Table 4). The result for each scale is as follows:
Results of Multiple Linear Regression Analysis.
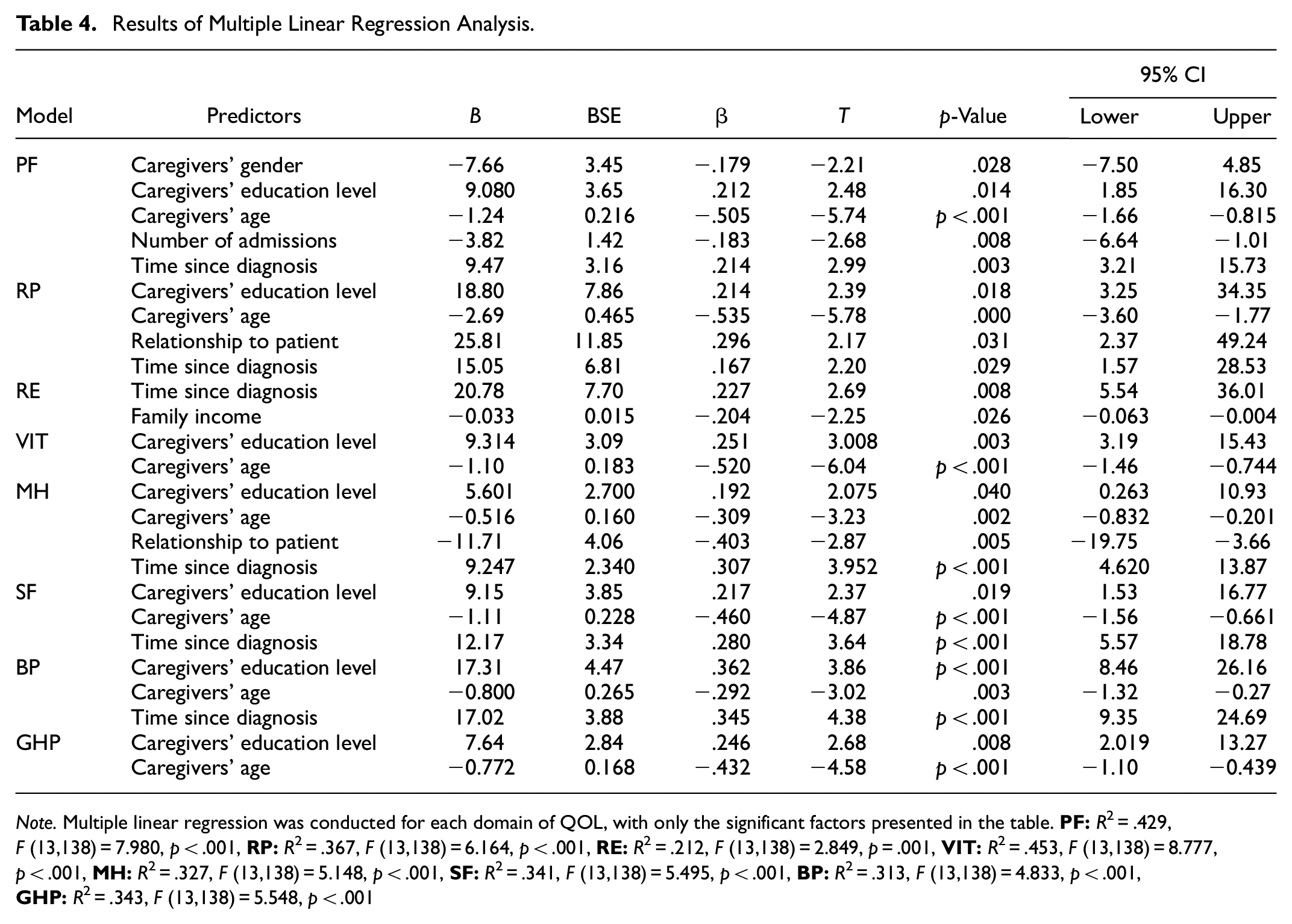
Note. Multiple linear regression was conducted for each domain of QOL, with only the significant factors presented in the table.
Physical Functioning (PF)
The overall regression was statistically significant (R2 = .429, F (13,138) = 7.98, p < .001). All variables in this model explained 42.9% of the variance in the score of PF. It was found that caregivers’ gender (β = −.179, p = .028), educational level (β = .212, p = .014), age (β = −.505, p < .001), number of admission (β = −.183, p = .008), and time since diagnosis (β = .214, p = .003) significantly predicted PF. However, none of the other variables were related to physical functioning. Caregivers’ age had a substantial weight in the model and explained 50.5% of the variances in the physical functioning domain.
Role Limitations Due to Physical Health (RP)
The overall regression was statistically significant (R2 = .367, F (13,138) = 6.16, p < .001). The standard partial regression coefficient (β) for this model indicated that caregivers’ educational level (β = .214, p = .018), caregivers’ age (β = −.535, p < .001), relationship to the patient (β = .296, p = .031), and time since diagnosis (β = .167, p = .029) were only predicted RP (Table 4).
Role Limitations Due to Emotional Problems (RE)
This model statistically significantly predicted the RE (R2 = .212, F (13,138) = 2.84, p = .001). Of all variables, time since diagnosis (β = .227, p = .008) and family income (β = −.204, p = .026) only predicted the score of RE and explained 23.2% of the variance in RE (Table 4).
Energy and Fatigue/Vitality (VIT)
The overall regression was statistically significant (R2 = .453, F (13,138) = 8.77, p < .001). It was found that caregivers’ age (β = −.520, p < .001) and educational level (β = .251, p = .003) significantly predicted VIT (Table 4).
General Mental Health (MH)
The overall regression was statistically significant (R2 = .327, F (13,138) = 5.14, p < .001) and explained 32.7% of the variance in mental health. Caregivers’ educational level (β = .192, p = .04), caregivers’ age (β = −.309, p = .002), relationship to patients (β = −.403, p = .005), and the period since diagnosis (β = .307, p < .001) were only predicted the score of MH (Table 4).
Social Functioning (SF)
This model was statistically significant (R2 = .341, F (13,138) = 5.49, p < .001), and all variables explained 34% of the variance in SF. Caregiver’s age (β = −.460, p < .001), the caregiver’s educational level (β = 0.217, p = .019), and the period since diagnosis (β = .280, p < .001) predicted the SF (Table 4).
Bodily Pain (BP)
The regression model was statistically significant (R2 = .313, F (13,138) = 4.83, p < .001), and all the variables in this model explained 31.3% of the variance in bodily pain scores. Caregiver’s educational level (β = .362, p < .001), the caregiver’s age (β = −.292, p = .003), and the time since diagnosis (β = .354, p < .001) only predicted the level of BP. (Table 4).
General Health Perceptions (GHP)
The variables in this model explained 36.1% of the variance in the general health score (R2 = .343, F (13,138) = 5.54, p < .001). This model revealed that the caregiver’s age (β = −.432, p < .001) and caregivers’ educational level (β = .246, p = .008) significantly predicted GHP (Table 4).
Discussion
This study showed that family caregivers’ quality of life scores in almost all domains (except for bodily pain and physical functioning) were low compared to the data from the baseline of the medical outcomes study. Consistent with our findings, previous studies found that caregivers of cancer patients experienced poor quality of life (Al Qadire et al., 2020; Cai et al., 2021; Cho et al., 2018; Deniz & Inci, 2015; Noghani, 2016; Tang, 2009). Most caregivers reported low quality of life and experienced a loss of control over their lives, mainly when caregiving affects economic stability, socializing, and family relationships. These low scores in quality of life could be explained by the need for long-term treatment of leukemia patients and long home care duration, resulting in more disruption in caregivers’ lives.
A leukemia patient experienced a loss of intact family unit and pre-treatment close relationships. The length of the treatment protocol and the intense attention that the sick patient needs from the family caregivers are obstacles that hinder attempts at any aspect of normalcy and stretch the family resources (Mcgrath, 2001).
Our study revealed that caregivers’ education level, age, patients’ number of admission in the last month, the period since diagnosis, caregivers’ relationships with the patients, and family income significantly predicted caregivers’ quality of life. Specifically, caregivers’ age and education level predict all quality-of-life domains except role limitations due to emotional problems. This result is consistent with previous studies (Geng et al., 2018; Shahi et al., 2014; Shdaifat & Manaf, 2012), which found that caregivers’ quality of life is highly linked with their age. However, a study among Jordanian parents of children with cancer showed no significant correlations between burden and the parents’ age or the child’s age (Al Qadire et al., 2020). The results of our study are also inconsistent with the finding of Lim et al. (2017) on Chinese family caregivers, who found no association between family caregivers’ QOL and their ages. The difference in lifestyle among populations could explain this difference in the results. Young family caregivers experience better physical and mental health than older caregivers. Chronic disease burdens additional duties and responsibilities on family caregivers, overloading them, especially older ones (Yang et al., 2012). In our study, age was negatively correlated with all domains of QOL, indicating that young caregivers reported higher scores in all quality-of-life domains than those who advanced in age. Thus, the advanced age of family caregivers is a cause for concern because it may directly influence caregivers’ QOL.
Furthermore, the caregiver’s education level contributed positively to the quality-of-life domains. This result is consistent with a systematic and meta-analysis study about the determinants of depression in caregivers of cancer patients, which indicated that caregivers’ education level was negatively associated with depression in caregivers (Geng et al., 2018). Family caregivers with higher education levels are more likely to have better jobs, an excellent income to achieve financial satisfaction, and a better quality of life (Yu et al., 2017). The concept of health-related quality of life and education integrates the bio-psychosocial perspective of health and the multidimensional potentialities of education for well-being. A study by Gil-Lacruz et al. (2020) showed that the higher the level of education, the better the health-related quality of life (HRQOL). The most significant impact of education was on the mental health dimension. Education level is always connected with the indicators of life satisfaction, such as income and other indicators of socioeconomic status (e.g., employment and marital status), which is considered a function of education, through which education can enhance or reduce overall life satisfaction (Powdthavee et al., 2015). A previous review of the benefits of education concluded that education was one of the most important predictors of one’s health status, employability, and probability of being married, all known as predictors of life satisfaction (Oreopoulos & Salvanes, 2011). Interestingly, this is supported in our study, which found that family income is negatively associated with the domain of role limitation due to emotional problems.
Our study found that family caregivers with adequate income reported better quality of life than those with low income. This finding is consistent with a study conducted by Duggleby et al. (2016), which found that caregivers with adequate financial support demonstrated higher quality of life scores than those with financial problems. Similarly, financial constraints were found to predict higher burden levels among Jordanian parents of children with cancer in a study by Al Qadire et al. (2020). However, our study results are inconsistent with previous studies that found no association between family caregivers’ quality of life and income (Li et al., 2016; Yang et al., 2012).
The difference in results may be due to the monthly payment amount. In our study, participants had inadequate income, which explains the poor quality of life scores. In Jordan, the average family income is insufficient to meet the family’s needs and the demands of caregiving, regardless of health insurance coverage for all Jordanian cancer patients. A qualitative study found that “Role adjustment and financial burden” were part of the analytical theme “challenges of caregiving” among caregivers of cancer patients (Cai et al., 2021). Caregivers had to earn more money to pay for the costs of daily life, such as food or school fees for their children, in addition to the high cost of cancer-related treatments, including medication, laboratory tests, overnight hotel stays, restaurant meals, and transportation to hospitals (Trevino et al., 2018; Yu et al., 2017). Caregivers were forced to adjust their full-time to part-time work or even abandon their job, resulting in more stress and anxiety about future healthcare coverage (Yang et al., 2012).
Our study found that the length of time since the patient’s disease diagnosis significantly predicted various aspects of quality of life, including physical functioning, role limitation physical, role limitation emotional, mental health, social functioning, and bodily pain. Caregivers who had been caring for patients diagnosed for a longer period of time reported lower quality of life compared to those who had been caring for patients for a shorter period. This finding is consistent with previous studies by Yang et al. (2012), which also found that the quality of life of family caregivers worsens with an increase in the time since patients’ diagnoses. However, Li et al. (2016) did not find any association between the duration of disease diagnosis and family caregivers’ overall quality of life. Several studies have shown that longer periods of caregiving were associated with lower QOL in physical, psychological, and environmental domains (Shdaifat & Manaf, 2012). A prolonged period of diagnosis often leads to an extended period of caregiving, which includes recurrent hospital admissions and long-term treatment. This can increase the burden on caregivers, leading to poor quality of life.
The findings of our study demonstrated that physical functioning was significantly affected by the number of admissions in the last month. As leukemia treatment is considered complex and intensive, it often results in frequent readmissions (Tran et al., 2020). This can not only have physical limitations on the patient but also create a financial burden on the caregivers, who may have to take time off from work to care for the patient. In Jordanian hospitals, it is common practice for family members to be responsible for the patient’s care, including personal hygiene and monitoring their condition, which can lead to fatigue, reduced sleep, and physical pain for caregivers.
Our study also revealed that the caregivers’ relationship with the patient predicted role limitations due to physical and mental health, with parents reporting lower quality of life compared to other family members. This is likely because parents often provide permanent care to their children with cancer. The study also found that mothers or fathers had worse quality of life than other family members. This is consistent with other studies that have found that caregivers’ bonding with the patient is negatively associated with depression (Geng et al., 2018). However, Mishra et al. (2021) found no significant difference in caregiver burden or quality of life between male and female caregivers of cancer patients on chemotherapy.
Limitations
The findings of this research provide valuable insights into the factors that affect the quality of life of family caregivers of leukemia patients. However, it is important to acknowledge certain limitations while discussing the results. The study was conducted in a single hospital in Jordan; therefore, the results may not apply to other settings. Additionally, using a cross-sectional design limits the ability to establish causal relationships between the variables examined and the quality of life of family caregivers. Self-reported data collection may be subject to response bias. Moreover, the study did not assess the patients’ quality of life, which may have had a significant impact on the quality of life of the caregivers.
Implications
The innovation of this research lies in its identification of predictors of quality of life in family caregivers of patients with leukemia. By examining factors such as time since diagnosis, number of hospital admissions, and caregivers’ relationships with patients, this study sheds light on the complex interplay between caregiver characteristics and the quality of life they experience.
The results of this study have been able to help improve the existing science in several ways. Firstly, it adds to the growing body of literature on the quality of life of family caregivers of patients with cancer. Secondly, it provides insights into the specific factors that influence caregivers’ quality of life, which can inform the development of interventions to improve caregiver well-being. For example, healthcare professionals can use this study’s findings to better understand family caregivers’ needs and tailor interventions accordingly. Additionally, the results of this study can help healthcare providers develop strategies to reduce the burden of caregiving, such as providing respite care and emotional support.
Overall, this research has contributed to the advancement of science by providing important insights into the factors that influence the quality of life of family caregivers of patients with leukemia, and by highlighting the need for tailored interventions to improve caregiver well-being.
Conclusion
The study presents important findings regarding the quality of life (QOL) of family caregivers of leukemia patients. The results indicate that both patient-related factors and caregivers’ factors contributed to low QOL domains among family caregivers. The study highlights the need for ongoing interventions to improve the QOL of caregivers, which can potentially impact patients’ health outcomes. It is essential to target older caregivers, those with low education, and from a low socioeconomic background, as they are at higher risk of having poor QOL. Further research is needed to identify effective interventions that can enhance the QOL of family caregivers of leukemia patients. Research should also focus on evaluating family caregivers’ competency to establish a comprehensive educational program to improve their QOL and reduce the burden of caregiving.
Footnotes
Acknowledgements
Our sincere gratitude to all participants for devoting their time to this study and all directors and staff at a targeted cancer center who facilitated data collection performance.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Nahla Al Ali, Amjad Eid, and Nabela Aljada. The first draft of the manuscript was written by Nahla Al Ali and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Deanship of Research sponsored this work at Jordan University of Science and Technology [Research Grant No: 194/2017].
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Jordan University of Science and Technology (No. 37/105/2017, dated 04/05/2017).
Data Availability
Data will be made available on request.