
Abstract
Stress management activities that older adults can efficiently perform at home are needed. We therefore created a home-based expressive writing for older adults focusing on habituation and conducted a randomized controlled trial. Participants were randomly assigned to the expressive writing group (n = 42) and the active control group (n = 40). The expressive writing group wrote about stressful events for 15 to 30 minutes 3 times each day at home. The active control group wrote about what they bought the previous day on three different days. Twenty six participants were included in the final analysis. The results showed that rumination, a risk factor for depression, decreased in the active control group compared to the expressive writing group. Our findings suggest that older adults can efficiently perform writing sessions at home. Also, a task such as cognitive training, rather than writing about stressful events, decreased rumination in older adults concerned about their forgetfulness.
Introduction
In 2015, the percentage of people with depression was reported as being 4.4% in Japan. Moreover, the percentage of older adults with depression is estimated to be higher than younger people (World Health Organization, 2017). Furthermore, the percentage of those over 65 years of age with worries and stresses was estimated to be 49.2% (Ministry of Health, Labour and Welfare, 2016). It is known that daily life stressors are not only related to depression (Kraaij et al., 2002), but they are also related to decline in physical health condition (Piazza et al., 2013) and cognitive function (Aggarwal et al., 2014; Rickenbach et al., 2014). Therefore, stress management is important in the daily life of older adults.
Mindfulness mediation and exercise interventions are typical techniques for managing daily stress. The effectiveness of mindfulness meditation has been reported in meta-analyses (Geiger et al., 2016; Grossman et al., 2004; Khoury et al., 2013). However, it takes about 20 to 30 minutes a day and 5 to 6 weeks to effectively conduct mindfulness meditation (Foulk et al., 2014). In addition, due to limitations faced by older adults (e.g., physical limitations, health problems, time constraints, restricted ability to travel), modifying protocols may sometimes be necessary to increase feasibility (Geiger et al., 2016).
WHO defines physical activity as any bodily movement produced by skeletal muscles that requires energy expenditure (World Health Organizaion, 2021). In their review, Kadariya et al. (2019) reported the frequency of exercise interventions (e.g., yoga, tai chi) was 1 to 4 times per week. Each session lasted 20 to 120 minutes, and the duration of exercise programs ranged from 6 to 40 weeks (Seo & Chao, 2018). This review demonstrated that physical activity as a stress management method can be used for physically healthy people. Indoors activities should be developed for a wide range of participants, including those that may have physical limitations.
Expressive writing is one method that meets these requirements (Pennebaker, 1997). Expressive writing is a stress management method that can be conducted alone in a short time either outdoors or indoors (Burton & King, 2008). The typical procedures include writing about facts and feelings related to stressful events that one experienced during 3 days or more, for 15 to 30 minutes at a time. Pennebaker and Beall conducted expressive writing with university students and reported that the mean frequency of visiting a doctor in 1 month decreased (Pennebaker & Beall, 1986). Since 1986, studies have been conducted with various participants on expressive writing; including university students (Frattaroli, 2006; Smyth, 1998), unemployed people (Spera et al., 1994), and patients (Merz et al., 2014; Smyth et al., 1999).
Expressive writing consists of processes such as attention, habituation, and cognitive restructuring (Lepore et al., 2002). Attention is the first stage in which participants face incidents that they have been avoiding. Participants directly face their stressors in this stage. Habituation occurs when the confrontation with a negative memory of an emotional event leads to the person’s emotional and physiological responses to the stimulus to decrease over time. Through the habituation process, participants do not feel sadness or anger when they recall past events over time (Foa & Kozak, 1986). Expressive writing consists of several sessions. In most previous studies, no instructions have been provided as to whether the content of descriptions should be identical or different among sessions. Specific studies have indicated that expressive writing is more effective in groups that describe the same event in every session, compared to the control group that described different or neutral event (Lepore, 1997; Sloan et al., 2005), suggesting the process of habituation contributes to mainly physical health promotion (Low et al., 2010). Although habituation has been found to primarily improve physical health (Low et al., 2006), Low et al. (2010) found effects on intrusive thoughts in women with breast cancer who had limited social support resources. This finding implies that habituation may contribute to mental health depending on the individual’s circumstances.
Cognitive restructuring is the third stage in which participants reappraise the incidents. Indices of cognitive restructuring are assessed by using the number of categories of written words. Participants with advanced cognitive restructuring increasingly wrote words in the following categories: positive emotion words (e.g., happy, joy), causal words (e.g., because, reason), and insight words (e.g., understand, realize) (Pennebaker et al., 1997). Causal words reflect the process of thinking about the causes of an incident and trying to rationalize it. Insight words reflect the degree of referring to cognitive processing related to thinking (Pennebaker & Seagal, 1999).
In recent years, several studies have been conducted on middle-aged and older adults (Mills et al., 2020; Schmidt et al., 2018), but few studies deal with older adults living in the community. Populations are aging on a global scale, and it is predicted that the number of older adults who are concerned about forgetfulness will increase. Therefore, it is essential to have an easy and inexpensive method to ease the concerns of many older adults. Although expressive writing is expected to be a method to meet such needs, there is no validation of the effectiveness of expressive writing for older adults who are anxious about forgetfulness.
Furthermore most of the expressive writing interventions have been conducted in laboratories, workshop-style settings, or Internet (Chippendale & Bear-Lehman, 2012; de Medeiros et al., 2007; Heffner et al., 2013; Lamers et al., 2015; Mackenzie et al., 2007). As expressive writing is a low-cost and simple intervention method, it should be more developed as a home-based daily stress management tool. Furthermore, although some studies conducted biographical writing intervention (Chan et al., 2013; Freitag & Schmidt, 2016; Mills et al., 2020; Schmidt et al., 2018), expressive writing focused on habituation for older adults has not been examined to date. It might be possible to improve the effectiveness of expressive writing by giving instructions that would facilitate habituation. Facilitating habituation has been effective in promoting cognitive restructuring (Low et al., 2006; Sato, 2012). Moreover, it is considered essential to instruct participants to describe the same content in every session for facilitating habituation. Based on the above considerations, this study investigated the efficacy of expressive writing intervention on mental health indices of community-dwelling older adults through instructions to promote habituation.
The effect of expressive writing on mental health variables such as Rumination and Well-being has been reported (Gortner et al., 2006; Lamers et al., 2015; Lepore et al., 2002; Nolen-Hoeksema & Morrow, 1991;). Rumination has been defined as the tendency to think about causes and results repeatedly, and it is regarded as one of the major risk factors for depression (Ito & Agari, 2002; Nolen-Hoeksema & Morrow, 1991). Based on the Zeigarnik effects (Zeigarnik, 1938), writing about the same experience and solving participants’ worries may decrease the frequency of rumination, because unfinished tasks foster rumination (Syrek & Antoni, 2014). Over 70% of older adults experience rumination (Tait & Silver, 1989). Previous studies have reported that expressive writing was effective for rumination (Gortner et al., 2006).
The purpose of this study was to examine the effects of a home-based expressive writing technique on rumination, with instructions facilitating habituation. Writing about the same content may facilitate resolution and reduce rumination. Decreasing rumination may also increase well-being. Confirmation of this hypothesis may lead to the widespread use of home-based expressive writing for older adults.
Method
Participants
In 2015, we partnered with a municipality to recruit older adults experiencing forgetfulness. We advertised in the municipality newsletters and conducted the health checkups in Tokyo, Japan (n = 102, 24 men and 78 women, mean age = 75.60, standard deviation = 6.34, age range = 65–90).
Measures
Characteristics
Participants’ characteristics such as gender, age, and years of education were inquired. The Mini-Mental State Examination (MMSE) (Folstein et al., 1975) and the Japanese version of the Montreal Cognitive Assessment (Fujiwara et al., 2010) were used to assess a wide range of the participants’ cognitive functions. The MMSE is composed of orientation to time, orientation to place, immediate and delayed recall of three words, calculation, object naming, sentence repetition, three-step orders, written orders, spontaneous writing, and figure copying. The range of scores was 0 to 30 and a clinical cut off score of 23/24 (Sakurai et al., 2021). The MoCA-J is a screening instrument to detect mild cognitive impairment. The range of scores was 0 to 30 and a clinical cut off score of 25/26.
Primary Outcome
Rumination was assessed using the Negative Rumination Scale (Ito & Agari, 2001) that consists of two factors and 11 items, including 7 items assessing Negative Rumination Traits (NRT, Cronbach’s α = .73) and 4 items assessing Uncontrollability of Negative Rumination (UNR, Cronbach’s α = .81). The NRT assesses the frequency with which negative thoughts come to mind and the length of time these thoughts persist (e.g., the tendency to ruminate on the same negative idea). The UNR measures “how out of control” one is when a negative event occurs in mind. The statement “e.g., even when I think of something unpleasant, I do not lose myself in it and take some action” is affirmative. Therefore, all scores for this factor were reversed and summed. Participants were required to respond using a 6-point scale that ranged from 1 = Never to 6 = Very often. Higher scores on this scale indicate more negative tendencies. The range of NRT was 7 to 42 points and UNR was 4 to 24 points.
Secondary Outcome
Well-being was assessed using the WHO-5-J (WHO-5; the Japanese version of WHO-Five Well-Being Index, Cronbach’s α = .87) (Awata et al., 2007), consisting of 5 items, which inquired about the mood in the past 2 weeks. Participants are required to respond using a 6-point scale; 1 = All of the time to 5 = No time. All the items in the scale are processed in reverse, and 0 to 5 points are added. The score range is 0 to 25 points with higher scores indicating better health. In normative data for Japanese older adults aged 65 to 84, there was no gender difference in the scores. However, the scores tend to be lower starting at age 80 (Iwasa et al., 2014).
Procedures
The 102 community-dwelling older adults who had health checkups in this study were concerned about forgetfulness and interested in the prevention of dementia. Because of ethical considerations, the active control group consisted of participants engaging in memory tasks. The intervention as well as the assessment of the effect indices by answering the questionnaire were conducted at home. Participants’ characteristics and pretest scores were assessed at the health checkups site. Fifteen participants declined because they were not interested in this intervention study; five participants who had psychosis or did not answer the question on psychosis were excluded. Participants who were receiving counseling or consulting with psychotherapists were instructed not to participate in the survey either orally or by instructions written on the manual. The 82 participants that gave their consent to participate in the study were allocated to the expressive writing group (n = 42) or the active control (n = 40). The random number generation method with the RAND function in Microsoft Excel 2010 was used for randomization (i.e., simple randomization) by the first author.
Participants in the writing group were instructed to describe the same incident in three sessions to facilitate habituation. Following previous studies, participants were given a set of instructions, and interventions were conducted at home (Ogawa et al., 2016; Sloan et al., 2007). First, we introduced expressive writing to community-dwelling older adults that had health checkups. It was introduced as an easy stress management method that could be used at home. The expressive writing manual, worksheet, and a questionnaire regarding mental and physical health were distributed to the expressive writing group members. The manual explained the outline of expressive writing, points to note, and how to conduct the task.
Participants were instructed to describe “upsetting or unsolved experiences of their entire life (such as interpersonal problems, what they would worry about in the future)” for 15–30 minutes each day. Participants were required to write the date and time of conducting expressive writing on the front cover of the worksheet. Based on the record, we confirmed that the participants conducted the task. They were required to describe the same content in all 3 times. The instructions were developed based on previous studies (Ogawa et al., 2016; Sloan et al., 2007). If the participant had a traumatic reaction at home, we could not provide immediate clinical care. Although this risk was improbable, we asked the participants not to describe overly shocking events for prevention.
The active control group members were requested to recall what they had bought the day before and write the name and prices of the items they had bought. The manual, worksheet, and questionnaires regarding mental and physical health were distributed to them. The session was conducted 3 times for 15 to 30 minutes each day. Participants were requested to send back the front cover of the worksheet and questionnaire to the researcher using the enclosed envelope. We confirmed that the participants had conducted the tasks based on the date written on the front page of the worksheet.
Instructions
Writing Group
The First Day
For the next 3 days, we would like you to write about the most upsetting or most unsolved experience of your entire life. In your writing, we want you to really let go and explore your very deepest emotions and thoughts. Whatever you choose to write about, it is critical that you really delve into your deepest emotions and thoughts. Ideally, we would also like you to write about significant experiences or conflicts that you have not discussed in great detail with others. Remember that you have three days to write.
Please write and try not to stop for fifteen minutes at least. Don’t worry about grammar or spelling.
The Second Day
Today, please continue to write about the same experience that you wrote about last time. Today we really want you to explore your very deepest emotions and thoughts. We don’t want you to copy the essay you wrote the first day.
The Third Day
Today is the last writing session. In your writing, we again want you to explore your deepest thoughts and feelings about the most upsetting or most unsolved experience of your entire life. Remember that this is the last day and so you might want to wrap everything up. For example, how is this experience related to your current life and your future? But feel free to go in any direction you feel most comfortable with and delve into your deepest emotions and thoughts. We don’t want you to copy the essay you wrote on the first or the second day.
Active Control Group
“For the next 3 days, we would like you to try to remember the prices of the commodities you bought the previous day. If you can remember the prices, please write them down on the worksheet. It may be difficult to remember the commodities or prices at first, but you may remember them in a few minutes. If you finish remembering as much you can, you may look at the receipt to check the answers. You can also challenge yourself. For example, some people remember only the name of commodities, others remember both commodities and their prices. Please do not look receipt soon. We would like you to do your best to remember. Please remember what you did yesterday, if you did not buy anything.” We instructed them to recall the TV/radio program they watched/listened to the day before if they had not bought anything.
The participants were required to respond to questionnaires about their mental and physical health after completing each session. The questionnaires included the negative rumination scale and WHO-5-J. Participants were requested to send back the worksheet and questionnaires to the researcher using the enclosed envelop.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki (1983). Tokyo Metropolitan Institute for Geriatrics and Gerontology approved the research protocol (No. 98, February 24, 2014). Written informed consent was obtained from all participants before intervention.
Analyses
The sample size was calculated with G*Power (Faul et al., 2007) for repeated ANOVA for a medium effect size (f = 0.25) (Cohen, 1988), α = .05, and a power of 0.80. The sample size calculation indicated that total sample size required was n = 34. Also, previous studies demonstrated that data from 40 to 45% of recruited older adults was analyzed in the end (Ogawa et al., 2016; Schmidt et al., 2018). Therefore, we set a goal to recruit about 85 older adults.
Differences in characteristics of the participants and the time spent conducting the task between the two groups were analyzed. Gender differences were examined using Fisher’s exact test. Age, years of education, MMSE scores were examined using a t-test. The time spent conducting the task was examined using the Mann-Whitney-U test. Intervention effects were examined using Analysis of Variance (ANOVA). When the interaction was significant, changes in the effect indices of each group were examined. As the effect size of ANOVA,
Results
Of the remaining 82 participants, 41 conducted the task and sent back their answers (expressive writing group = 20, active control group = 21, resulting in a response rate of 50.0%), and 41 did not send back their answers. Among them, the data of those that entered the date on their questionnaires were analyzed if we could confirm that the date was after conducting the task. The number of participants whose data were analyzed included 13 in the expressive writing group and 13 in the active control group (Figure 1).

CONSORT flow diagram of the study procedure.
Shapiro-Wilk test was performed to check that the distribution of scores were normal. The results show that years of education, MMSE, MoCA-J, and the time of engagement of the task did not have a normal distribution; therefore, we applied Mann-Whitney-U test. Residual change scores (Time 2-Time 1) were created for NRT, UNR, and WHO-5-J. These scores had a normal distribution, so we applied the t-test to compare the residual change scores of both groups.
Table 1 shows the baseline characteristics of the participants, including the time spent on the task each day for each group, and the results of the t-test and Mann-Whitney-U test. In both groups, most participants were female. One participant in the expressive writing group scored less than 24 points on the MMSE. No participant in the active control group scored less than 24 points on the MMSE.
Characteristics of Participants.

Note. p-Values indicate the results of t-test, the Fisher’s exact test, and Mann-Whitney-U test. Chi-square test was used for gender. T-test was used for age. Mann-Whitney-U test was used for years of education, MMSE, and MoCA-J. M = mean; SD = standard deviation; Me = median; IQR = interquartile range; MMSE = mini mental state examination; MoCA-J = the Japanese version of the montreal cognitive assessment.
Seven participants in the expressive writing group and six participants in the active control group scored less than 26 points on the MoCA-J. The results imply that the data in this study included participants with mild cognitive impairment. However, there were no statistical differences in all baseline characteristics and the time spent engaged in the task between the two groups.
To examine the intervention effects on the expressive writing group, each residual change scores were analyzed using t-test (Table 2). The results indicated that the NRT score decreased in the active control compared to the expressive writing group, t (24) = 2.25, p = .034, Cohen’s d = 0.88. The residual scores of UNR, t (24) = 0.00, p = 1.000, Cohen’s d = 0.00, and WHO-5-J, t (24) = 1.67, p = .105, Cohen’s d = 0.66, did not differ significantly between the two groups.
Means and Standard Errors of Mean Outcome Variables and t-Test Results.
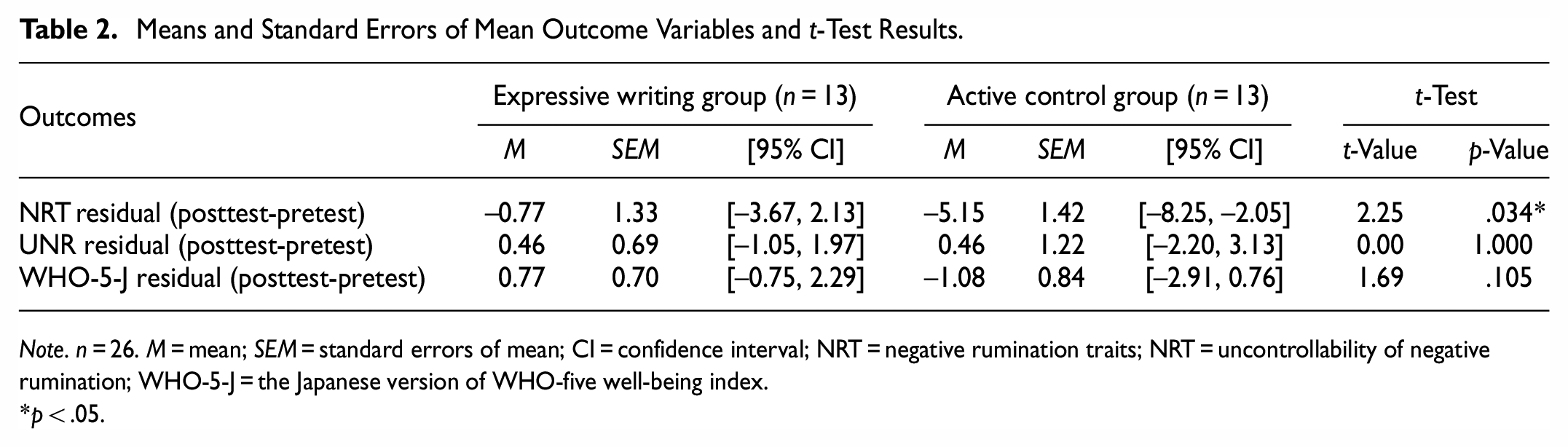
Note. n = 26. M = mean; SEM = standard errors of mean; CI = confidence interval; NRT = negative rumination traits; NRT = uncontrollability of negative rumination; WHO-5-J = the Japanese version of WHO-five well-being index.
p < .05.
Discussion
This study examined whether expressive writing decrease rumination and improve well-being with home based expressive writing for older adults. The results showed that the participants in the active control group, whose task resembles cognitive training, exhibited a reduction in rumination. The expressive writing group did not show any significant reduction, which contradicts our hypothesis. However, because of the small sample size, the results of the final analysis should be interpreted with caution.
In some previous studies, the participants are instructed to describe severe traumatic events (Birrer et al., 2007; Gerger et al., 2021). Traumatic or intrusive memories are related to rumination (Birrer et al., 2007; Williams & Moulds, 2008). It might be difficult or impossible for such a severe event to be solved in daily life. Recent studies targeted people with specific illnesses such as breast cancer or cell carcinoma (e.g., Chu et al., 2020; Milbury et al., 2017), and the researchers specified what participants should write. In other words, essay content which participants wrote and the event causing rumination might have been consistent. These studies indicated that the content of the participants’ essays and rumination tended to be consistent. On the other hand, the participants in the present study were asked not to write about traumatic events that would lead to Posttraumatic stress disorder (PTSD). Essay content in the present study was limited to daily life events.
It is not clear whether the described content might have caused rumination in this study. If the content of rumination and that of description were consistent, intervention effects might have been demonstrated. In the active control group, rumination decreased, which might be caused by the consistency between the description content and rumination content. Participants in this study were interested in the prevention of dementia. For them, training for preventing forgetfulness is useful for solving their worries. To write what they bought the day before might have become a training for directly resolving the rumination content, which might have played a role as problem-focused coping strategy, because resolving their worries or problems is way of decreasing rumination. Although the effectiveness of the task of the active control group was not expected, it might have corresponded to the needs of the population who care about their forgetfulness. In fact, a previous study conducted with caregivers showed that the group that described issues related to time-management showed a higher effect on mental health than the group conducting expressive writing (Mackenzie et al., 2007).
Regarding the WHO-5-J scores, significant effects of the intervention on the expressive writing group were not indicated. The WHO-5-J comprehensively inquires mental health conditions in the past 2 weeks; for example, the extent to which sleep and lifestyle conditions were positive. In previous studies, people with WHO-5-J scores of less than 13 were considered unhealthy (Awata et al., 2007). The participants in this study had an average WHO-5-J score of approximately 16 and were relatively healthy (Iwasa et al., 2014). Therefore, expressive writing group tasks may not have contributed to improved mental health.
This study has the three major limitations. Firstly, we could not confirm whether the participants honestly described the same content for 3 days. Out of consideration for the participants’ privacy, the written content was not collected, which would have been helpful for the participants in conducting the task. Additionally, we were concerned that participants would not want us to see what they had written, which would reduce the collection rate. However, the procedures’ accuracy was not ensured. Some participants in both groups submitted what they wrote. Therefore, future studies should consider collecting the submissions to check whether similar content is described in previous sessions, while still maintaining confidentiality.
Secondly, the follow-up period was rather short. Many participants responded to the questionnaire on the same day as the last day of the description. Effects of expressive writing tend to become significant during an extended follow-up, and how the effects are indicated tend to be different based on the index (Pennebaker & Chung, 2011). This study could not demonstrate the possibility that expressive writing is instantly effective for maintaining mental health and preventing its decline. However, a long-term follow-up might have identified significant intervention effects. Future studies may examine whether the length of the follow-up is related the degree of the effect of expressive writing. Moreover, the selection of participants that are appropriate for expressive writing interventions should be investigated.
Thirdly, the sample size and the spread of expressive writing was a limitation of the study. Among the participants that agreed to participate in the survey, 52.7% returned the results (expressive writing group, 53.2% and the active control group, 52.2%). Unlike the usual case, a reward was not given to the participants, which might have been one cause of the low response rate. The design of the study should be improved to increase the motivation of older adults, regardless of rewards, to increase the popularity of the expressive writing technique and to make it available in the daily life of the increasing numbers of older adults. Moreover, because some participants answered the questionnaires before conducting the task, we could not analyze those data. We recommend researchers explain the procedure for the older adults more politely than for younger adults. Finally, characteristics of participants that tend to use expressive writing should be investigated in future studies. This is expected to ensure a sufficient sample size, which would more clearly elucidate the mechanism of expressive writing.
Conclusion
In conclusion, among community-dwelling older adults who care about their forgetfulness, remembering their daily actions (e.g., what they bought the previous day) could decrease rumination. On the other hand, those who wrote about their most upsetting or most unsolved experience could not decrease rumination. Although easiness is a merit of expressive writing, merely describing worries might not demonstrate the maximum possible effect of expressive writing. It would be necessary to give appropriate instructions corresponding to their needs in order to increase the effects of expressive writing. Our study therefore suggests that direct problem-focused strategy was effective for coping with rumination.
Footnotes
Acknowledgements
We are very thankful to Toshima city’s staff members and all participants in this study.
Availability of Data and Material
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Trials Registration
Clinical trials registration number: UMIN000040439 2020/05/18
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MEXT KAKENHI Grant Number 15K13156