
Abstract
Many nurse managers actively developed mentoring programs to shorten the acclimation period of new nurses in hospitals. The main aim was to develop a negative mentoring experience questionnaire (NMEQ) and test its validity and reliability. A cross-sectional study was employed. This study adopted questionnaire-survey method with new nurses of Taiwanese hospitals. In the main study, this study adopted reliability analysis, content, validity, construct validity and criterion-related validity analysis. 255 participants were collected, with 87.93% response rate. A total of 29 items of five-dimension scale of NMEQ were proposed: four nursing manager items, four institutional items, three other medical staff items, 12 mentor items, and six mentee items. Each dimension demonstrated a reliability of 0.72 to 0.96. Exploratory factor analysis and Confirmatory factor analysis results indicated that NMEQ had acceptable convergent and discriminate validity. Correlation analysis indicated this scale and mentoring function scale exhibited a significantly negative correlation (p < .05). NMEQ is reliable and valid for hospital nurses. It also can help clinical nursing managers to clarify the possible negative experiences and strengthen the adaptability and mental health of new staff nurses in mentoring programs. Nursing policy planners can use NMEQ to measure the negative experience of new nurses, monitor the performance of mentoring program, and further revise mentoring policies.
Introduction
The high turnover rate of nurses is a serious problem for clinical nursing care (Cao et al., 2021; Tarhan et al., 2022). Many studies also found that new staff nurses have a higher turnover rate than other nurses(Hallaran et al., 2021). The high turnover rate of new staff nurses is usually caused by difficulty adapting to a new environment, a low sense of professional accomplishment, the difference between expectations and reality, and a high level of work-related stress(Hallaran et al., 2021; Tarhan et al., 2022). In order to solve the problem of adapting new nurses to the new work environment, mentoring programs that aim to shorten the acclimation period of new nurses have been implemented in many hospitals. The programs involve establishing positive work attitudes and career outlooks, as well as strengthening the competence to adjust to the workplace and their work efficiency, therefore lowering turnover rates(Horner, 2020; Pham et al., 2019).
Past research has found that conflicts do exist in the interactions between mentors and mentees occasionally (Davey et al., 2020; Fernandez et al., 2018). When accumulated over a long period of time, the resulting negative experiences not only have the possibility to reduce the efficacy of mentoring programs, but also help to undermine the effects of knowledge transferring in mentorship. Eventually, it would result in mentoring dysfunction and diminishing relationship effectiveness (Jacobsen et al., 2022; Liao et al., 2020; Pham et al., 2019). Liao et al. (2020) indicated that mentees sometimes are assigned to a mentor they do not feel comfortable with. If anyone in a mentorship does not trust the other, it would lead to limited communication and more conflicts between mentors and mentees. In addition, if hospitals lack clearly defined accountability for new nurses and mentors. This would result in negative impacts on mentoring programs. Kakyo et al. (2022) also found if new nurses could not overcome the challenges of the complex and dynamic nursing environment, new nurses are easy to generate negative feelings.
There are both negative and positive experiences coexisting within the course of interactions. Many new staff nurses confronted negative mentoring experiences (NMEs) (Jacobsen et al., 2022; Liao et al., 2020; Pham et al., 2019). Particularly, the negative effects of these negative experiences sometimes would exceed the positive effects of the mentoring program. The NMEs usually caused mentees multiple effects like lower psychological and career support, poor learning experience, lower work satisfaction, greater work-related pressure, a higher level of workplace frustration and high turnover tendency etc. (Fernandez et al., 2018; Jacobsen et al., 2022; Kakyo et al., 2022). When mentees had too many negative experiences in the mentoring program, they may possibly decide to withdraw from the mentorship and strengthen their intention to leave the nursing profession (Pham et al., 2019).
Serious NMEs often leaded to severe disappointment of the new staff nurses and thus made them leave their job. Thus, if a proper scale can be developed to help nurse managers aware and analyze negative experience in the early stage, it’s possible to develop proper methods to detect the sources of potential NMEs, thereby reducing their intention to quit among new staff nurses. Consequently, to assess mentees’ NMEs is important theoretically and practically.
Mentoring programs can provide psychological and career support for new staff nurses (Devey Burry et al., 2020; Horner, 2020). Despite of providing benefits for the mentee, negative mentoring outcomes might happen on both the mentors and mentees during the mentorship period. NMEs, arising between mentor and mentee, would inhibit the ability and the willingness of the mentors to teach their mentees (Bambi et al., 2019; Davey et al., 2020; Liao et al., 2020). According to the findings of previous studies, we found NMEs should include the following five important dimensions. First, an institutional dimension encompassing negative experiences caused by the mentoring program. Second, a mentor dimension in which the mentor initiates negative experience. Third, a nursing manager dimension, where nursing managers cause negative experience. Fourth, an other medical staff dimension, in which other medical staff (physicians, physician assistants, administrative staff, etc.) instigate negative experience. Finally, a mentee dimension in which the mentee instigates negative experience within their relationship with their mentor (Bambi et al., 2019; Fontes et al., 2019; Gong & Li, 2019; C. Y. Huang et al., 2013; Liao et al., 2020; Nelson et al., 2021; Pham et al., 2019; Vandal et al., 2018).
Little attention has been given to develop the tools with theoretical basis and practical implications to evaluate NMEs such as NME questionnaires since many past studies only tried to explore mentoring function in nursing workplaces (C. Y. Huang et al., 2016; Jacobsen et al., 2022; Liao et al., 2020). Therefore, the aim of this study tried to establish a negative mentoring experience questionnaire (NMEQ) with theoretical base for hospital nurses as an important tool for nurse managers and test its validity and reliability.
Methods
Design and Sample
A cross-sectional study was adopted to collect data. The subjects were new staff nurses who have been in mentorship programs and had been working for less than 2 years in two regional Taiwanese hospitals. After obtaining institutional review board approval (Ethical Board of Show Chwan Memorial Hospital, Taiwan, ID 1021205), questionnaires were employed to collect the study data. This study divided the data collection into two stages. First, in the pilot study, drafting preliminary items, expert validity examination and reliability analysis were included. Expert validity examination was conducted by five representative nurse managers with plenty of mentoring experiences. After that, 30 new staff nurses were collected from two hospitals. The purpose of the stage was to revise the draft of NMEQ according to the results of expert examination and reliability analysis. In the main study, 290 samples in total were distributed with self-report questionnaires with a convenience sampling method. Two hundred fifty-five subjects were collected, with 87.93% questionnaire response rate.
Questionnaire Design
This study defined NMEs as the sum of dysfunctional mentoring outcomes would occur during the mentorship program and adopted the assertions of previous studies to develop the draft of NMEQ(Bambi et al., 2019; Fontes et al., 2019; C. Y. Huang et al., 2013; Liao et al., 2020; Nelson et al., 2021). Two scholars who majored in nurse mentoring programs were involved in developing the draft items. We use a 5-point Likert scale to evaluate the level of agreement with the items on the NMEQ (5 = strongly agree; 1 = strongly disagree).
Data Analysis
Descriptive statistics were adopted to analyze sample characteristic. Exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were used to examine the construct validity of the NMEQ while Cronbach’s alpha value was measured to evaluate the reliability. EFA could be adopted to identify the factor structure of a set of observed variables but CFA could be used to confirm the factor structure of a set of observed variables. In our study, we employed EFA to explore the fundamental factor structure of all NMEQ items and used CFA to confirm the factor structure of all NMEQ items. Finally, this study used Pearson’s correlation coefficient to test criterion-related validity. used the scale of C. Y. Huang et al. (2016) mentoring function scale as a criterion and The analyses were conducted using SPSS 22.0 and AMOS 18.0.
Results
First Stage
The study proposed 48 preliminary items first and then invited five senior nursing managers with multi-year mentoring experience to perform the expert validity test. The relevance of each item was rated by the experts. A score of 0 denoted “not relevant or somewhat relevant” and a score of 1 denoted “quite or highly relevant.” We attempted to test content validity by computing the content validity index (CVI), the one which was less than 0.8 would be removed. An average score of 0.92 was computed from 33 items and the remaining 33 items were included into a reliability test. All samples in the pilot study were female, 35 respondents were unmarried, with 40% between 26 and 30 years old, 54.90% had worked for the hospital for between 1 and 2 years, and 35 respondents with a Bachelor of Science degree. According ot the results of reliability analysis, three items were deleted because the values of item-to-total correlation of these items were less than .5. The remaining 30 items were included in the second stage (Cronbach’s α = .92).
Second Stage
In the main study, Of the 255 new staff nurses, 248 participants were female, 85.5% were unmarried, with 60.39% between 20 and 25 years old and 67.84% held a BSc degree or higher. All of sample had been working in hospitals for less than 2 years and 45.9% had been working in hospitals for less than 1 year. 52.16% said that they usually interacted with their mentors. 59.61% were instructed by the mentors with Level III and 71.37% of mentors had experience of mentoring other nurses (See Table 1).
Sample Characteristics (n = 255).
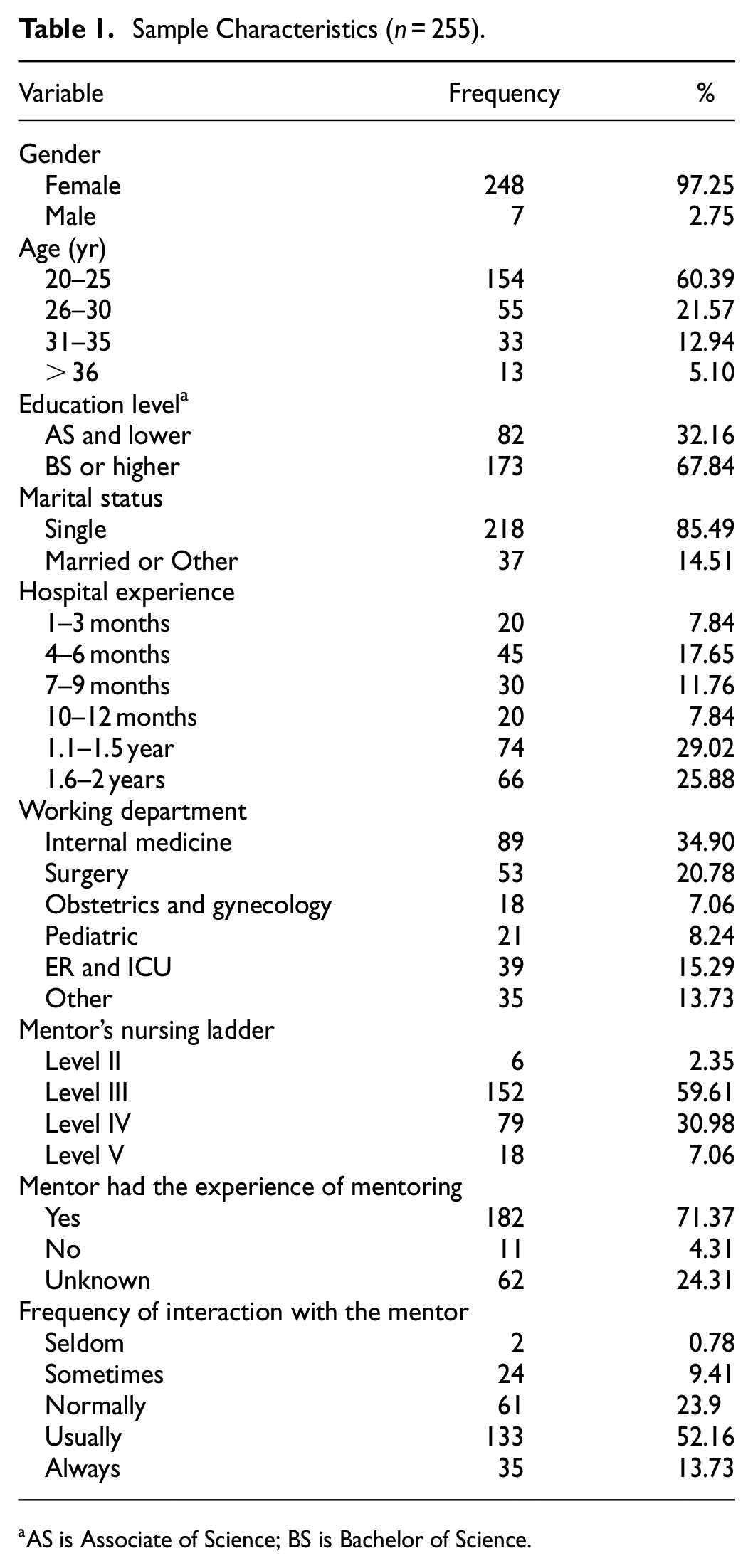
AS is Associate of Science; BS is Bachelor of Science.
Exploratory Factor Analysis
The present study used the Kaiser-Meyer-Olkin (KMO) test and Bartlett’s test of sphericity to evaluate sampling adequacy. The value of KMO was 0.924 and the significance of Bartlett’s test was less than 0.01, showing that EFA could be applied to our data. A principal component analysis was adopted to extract initial factors, and varimax factor rotation was then used. The number of extracted factors were the factors with eigenvalues ≥1 and items with factor loadings of 0.5 or higher were considered as appropriate ones to measure factors. Accordingly, the results showed that a total of five factors were extracted and these factors accounted for 70.05% of the total variance. Finally, 29 items were kept after deleting G1 item that have factors loadings on two factors reached 0.5. The details are listed in Table 2.
Exploratory Factor Analysis Results (n = 255). a
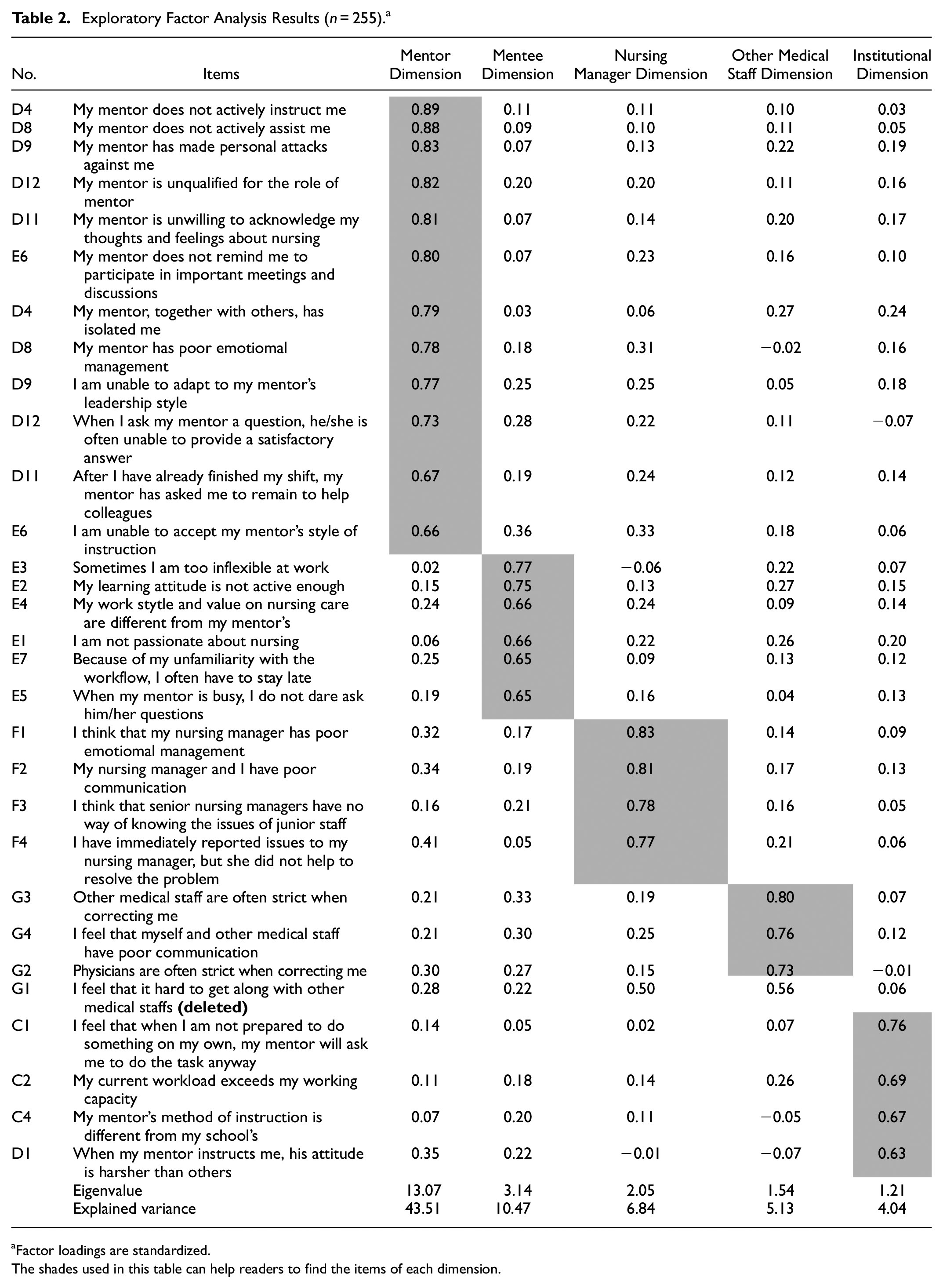
Factor loadings are standardized.
The shades used in this table can help readers to find the items of each dimension.
The first factor was included in 12 items, explaining for 43.51% of the variance, and was named the “mentor dimension” (Cronbach’s α = .96) due to these items indicate a negative experience caused by the mentor. The second factor consisted of six items, accounting for 10.47% of the variance, and was named the “mentee dimension” (Cronbach’s α = .84) because the items deal with negative experiences caused by the mentee. The third factor, “nursing manager dimension,” included four items. The explained variance was 6.84%, and the Cronbach’s alpha value was .92. The forth factor consisted of three items, accounting for 5.13% of the variance, and was named the “other medical staff dimension” (Cronbach’s α = .88) because these items imply negative experiences caused by staff other than nurses. The fifth factor, “institutional dimension,” included three items. The explained variance was 4.04%, and the Cronbach’s alpha value was .72.
Confirmatory Factor Analysis
In order to avoid the subjective character of decision-making when different exploratory factor solutions are compared, confirmatory factor analysis (CFA) should be further adopted to exam the structure of psychological questionnaires. They conducted EFA and CFA with the same sample. Therefore, we conducted CFA and obtained a good fit of the measurement model of NMEQ (
Assessment of Convergent and Discriminant Validity (n = 255). a

Factor loadings are standardized.
AVE, average variance extracted.
p < .01.
Criterion-Related Validity
The mentoring function scale of C.-Y. Huang et al. (2016) was employed as an inverse criterion for NMEQ, positive mentoring experience. This scale was composed of three elements of psychosocial support function, role modeling function, and career development function. In Table 4, NMEQ has reported sufficient criterion-related validity because the results of Pearson’s r correlation showed that NME and all dimensions of NMEQ had significantly negative correlation with all dimensions of mentoring function (See Table 4).
Correlation Matrix of Variables (n = 255). a

Pearson’s correlation coefficients.
p < .05. **p < .01.
Discussion
The empirical results of this study show that NMEQ in this study has sufficient reliability and validity, as is explained below for each dimension. The institutional dimension refers to negative experience caused by institutional elements, which includes hospital institutions, human factors, and education institution factors. New nurses often did not see their schools’ methods for providing clinical care as practical in the nursing care(Cao et al., 2021; Hallaran et al., 2021). New nurses in hospitals often have difficulty applying their knowledge to a clinical nursing environment; a problem manifesting itself in poorer care(Liao et al., 2020; Powers et al., 2019). C. Y. Huang et al. (2013) also found that new nurses did not see their schools’ methods for providing clinical care as practical in the real world. The mentor dimension indicates negative experiences inflicted on the mentee by the mentor, and includes questions about workplace bullying, verbal communication, instruction methods, and mentor personality. The phrase “workplace bullying” is used to define workplace incidents of verbal abuse, exclusion, or other acts that have a negative impact on the victim. Previous studies have shown that workplace bullying often happens in the nursing field, and when new nurses encounter such behavior in the workplace, they often choose to leave(Bambi et al., 2019; Fontes et al., 2019).
The mentee dimension refers to negative experiences caused by the mentee themselves. NMEs are not necessarily caused by mentors; mentees can also cause NMEs. In the mentorship, mentors would react to mentees in a negative way when they felt that mentees were making complaining, showing disrespect, shirking their responsibilities, and lacking learning motivations. NMEs caused by the mentee can be divided into three categories: interpersonal problems, destructive relational patterns, and performance problems(Jacobsen et al., 2022; Kakyo et al., 2022; Wurmser & Kowalski, 2020). NMEs caused by the demeanor of nursing managers or their poor interaction with mentees are classified under the nursing manager dimension. Low-quality communication and poor interaction between new nurses and nursing managers often happened and new nurses were also often unable to find effective ways of handling these conflicts(Fontes et al., 2019; Fowler et al., 2021). Because the other party in the conflict was their own nursing manager, many new staff nurses were unwilling to address the conflict for fear of suffering negative consequences. This inability to find effective solutions to conflicts contributed to negative experiences. Finally, the other medical staff dimension indicates that negative experiences can be caused by poor communication between other medical staff and the mentee. Nursing often requires interaction and collaboration with other medical staffs other than mentors. Some medical staffs may have a poor attitude toward new nurse and then it would cause negative experiences for mentees(Ma et al., 2021; Tarhan et al., 2022).
Conclusion
NMEQ of this study for hospital nurses is reliable and valid. This scale contained five dimensions and 29 items. The results of CFA showed NMEQ had good convergent validity and discriminant validity. Correlation analysis also indicated that NMEQ have good criterion-related validity.
Implications of Practice and Policy
NMEQ can be used as an important tool for nurse managers in hospitals. It allows nurse managers to pay more attention to the new staff nurses’ negative experiences in the mentorship. NMEQ also can be used as an important management tool in the process of monitoring and managing mentoring programs. Upon using NMEQ, the nurse managers could clearly measure the effectiveness of mentoring program, knowing which aspect the negative experiences of new staff nurses come from, and keep abreast of the right directions to improve mentoring program in the future. In addition, the both positive and negative experiences of mentoring programs could be assessed and analyzed at the same time. Thus, the empirical results of this study provides abundant important evidence for nursing human resource theory and a practical reference for those in the field.
NMEQ also can help clinical nurses understand and evaluate the categories and the level of negative experiences that new nurses are would confront during the process of mentoring programs. Thus, it can help new nurses strengthen their adaptability and mental health in nursing workplaces. Finally, what the study has found was a significant contributor to negative experiences that there is an apparent phenomenon of workplace bullying and poor interaction between mentors, mentees, nursing managers, and other medical staff. Accordingly, the present research suggested that nurse managers could develop mentorship training programs in order to improve interaction between mentees and others. Nursing policy planners can use NMEQ to regularly measure the negative experience of new nurses, monitor the performance of mentoring program, and further revise mentoring policies based on the empirical results.
Limitations and Suggestions for Future Research
This study only chose the new staff nurses of Taiwanese hospitals as its samples. To further clarify the implications arising both from different kinds of nursing program, we suggested that future researchers investigate a large-scale dataset from other national nursing contexts. In addition, we explored NME from the points of view of mentees; therefore, only single-side mentoring experience was explored. It is suggested that future researchers can continue to explore NME from other stakeholders’ views, for instance, mentors and nurse managers. This study has not tested the inter-rater reliability of NMEQ. Future research can continue to collect samples to test this reliability in this study
Footnotes
Acknowledgements
The author would like to thank the editor and the anonymous reviewers for their constructive comments and recommendations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Ministry of Science and Technology in Taiwan (NSC102-2410-H366-015).
Ethical Statement
The study was approved by the appropriate ethics committees of the hospitals in Taiwan. Ethical approval was obtained from the Institutional Review Board of Show Chwan Memorial Hospital (reference number: 1021205).