
Abstract
This study tests General Strain Theory (GST) as an explanation for associations between adverse childhood experiences (ACEs) and risk of violent and suicidal behaviors. Data comprise a census of archival information about the lives of 2,195 delinquent boys who resided at a U.S. treatment facility between 1975 and 2019. Logistic regression tests the effects of 12 combined ACEs, anger, low self-control, depression, race/ethnicity, and poverty on violent and suicidal behaviors. Interactive associations predicted by GST are examined by Zmediation and χ2 analyses. Nearly 93% of residents experienced at least one ACE, and 87% had ≥4. ACEs increase risk of violent and suicidal behaviors net of controls. They interact with low self-control and anger to increase risk of violence, and anger and depression mediate risk of suicidal behaviors. Rehabilitative programming for troubled boys should begin with thorough assessment of these experiences, and both outcomes require equal consideration in the ACEs research.
Keywords
This study examines the effects of adverse childhood experiences (ACEs) on violence against others and on suicidal behaviors of adolescent boys (ages 13–18) with a history of troubled behaviors. Agnew’s (2006) general strain theory has been offered as theoretical explanation for the effects of ACEs on suicide (Sharp et al., 2012), and to explain why ACEs increase risk of violence against others (Castellvi et al., 2017; Fox et al., 2015; Malvaso et al., 2018; Miller et al., 2011). To date, no study tests general strain theory as an explanation of both behaviors in the same study of justice-involved adolescent boys utilizing current conceptions of ACEs.
An ACE index is a simple preliminary diagnostic tool. Originally constructed in the medical field, ACEs point to possible health risks. In that field, the ACE index is not intended to direct treatment absent other medical tests and interventions. The same is true of the index’s utility in juvenile justice. A simple, short questionnaire administered to youth as they enter the juvenile justice system may be advantageous for identifying who may be in need for further diagnostic testing and intervention. Understanding why and how ACEs increase risk of suicide and violence against others may inform individualized treatment plans for justice-involved youth.
This study addresses several questions that remain in the ACEs research. What exactly can an ACE index predict? What experiences must be included in it to successfully predict adolescent behaviors? It is also important to examine whether ACEs mediate or precede unhealthy behaviors, and if their effects wane in the presence of traditional controls. These questions require a review of conceptualization and measurement in the ACEs literature.
Adverse Childhood Experiences (ACEs)
In 1995 and 1996, Felitti et al. (1998) collected retrospective information from 9,508 adults in a standardized medical evaluation by Kaiser Permanente about what they called adverse childhood experiences (ACEs). Each participant was later mailed a survey with seven dichotomous questions pertaining to their own childhood psychological, physical, or sexual abuse, violence against their mothers, whether they had lived with people who abused substances, were mentally ill, suicidal, or imprisoned. A single indicator of ACEs was constructed from these indices such that the presence of each ACE counted as an additional ACE in the index. Felitti et al. (1998) learned that having these experiences before adulthood significantly adversely affected adult physical and emotional health. This landmark study sparked hundreds of other studies on the ill effects of ACEs.
ACE Correlation, Clustering, and Dose Response
Felitti et al. (1998) formulated their hypotheses from decades of research on childhood trauma and abuse. Instead of attempting to create a thoroughly detailed diagnostic tool, they identified the presence or absence of childhood experiences that may increase negative outcomes later in life that require further diagnoses and treatments. Prior research consistently found that abuses and traumas were strongly correlated, which was confirmed by Felitti et al. (1998). Where there was one ACE, more were likely to co-occur. Dong et al. (2004) found that on average, 87% of those with one ACE reported at least one additional ACE. Clustering also occurred, for example, Felitti et al. (1998) found that 56% of those who had no poor outcomes also had no ACEs, while only 14% of persons with ≥4 ACEs had no poor outcomes. Additionally, there was a dose-response such that as the frequency of ACEs increased, problem behaviors increased (Chapman et al., 2004; Dube et al., 2003; Felitti et al., 1998; Taillieu et al., 2016). ACE correlation, clustering, and dose responses are examined throughout ACEs research on various outcomes.
The ACE Instrument for Justice-Involved Youth
In the ACEs research on troubled youth, ACEs encompass two categories; child abuse and household dysfunction, which is consistent with early ACE studies that predicted health risk behaviors (Felitti et al., 1998). Indices for each of these two categories have varied. Nearly all studies have included measures of physical and sexual abuse. Most have also included emotional/psychological abuse, and emotional/physical neglect. Some form of family violence among parental figures has been included, although some studies focused solely on the child witnessing the abuse firsthand, and at least one study measured it as abuse against the mother (Bielas et al., 2016). Household substance abuse, incarceration of household members, and mental illness have also been included. Divorce, separation, or single-parenthood have been included, but this variable has been somewhat problematic. Wolff et al. (2018) omit it because over half of their sample had only that ACE.
Less often, other measures of abuse have been included; household burglary, bullying, witnessing a shooting, and theft or physical abuse at school (Connolly & Kavish, 2019). DeLisi at al. (2017) included gang involvement and childhood violence against household members. Miller et al. (2011) included physical illness. Malvaso et al. (2018) and Miller et al. (2011) included the death of a parent. Bonner et al. (2020) and DeLisi et al. (2017) included measures of household over-crowding and family members moving in and out of the household. Connolly and Kavish (2019) included parenting style, and DeLisi et al. (2017) included poverty. Most studies have included measures of socioeconomic status, but as a control, not as part of the ACEs index (Steele et al., 2016). By 2015, Malvaso et al. (2016) found that half of all maltreatment studies included socioeconomic status with mixed results.
Most studies have constructed an ACE index of from 7 to 12 indices from other standardized measures, particularly the Positive Achievement Change Tool (PACT), which is an assessment tool for risk of reoffending. Bielas et al. (2016) used the Multidimensional Clinical Screening Inventory (MCSI) for delinquent juveniles. Some studies relied on official data from social services sources (Clarkson Freeman, 2014). Others used a mixture of official sources and interviews for the ACE index (Bonner et al., 2020; DeLisi et al., 2017). Researchers have typically constructed ACE indicators from indirect sources since self-reports from this population can be problematic (Thornberry & Krohn, 2000).
The Effects of ACEs on Juvenile Justice-Involved Youth
Early studies found that about 60% of the adult population had experienced at least one ACE, and 16% had experienced ≥3 (Merrick et al., 2019). Delinquent populations experience greater prevalence of ACEs than the general population (Basto-Pereira et al., 2016). One national study of justice-involved adolescents found that 62% had experienced at least one ACE by the age of 5, and “one-third of youth report(ed) exposure to multiple or co-occurring trauma types each year into adolescence” (Dierkhising et al., 2013, p. 2). Baglivio et al. (2014) discovered that 27.4% of males and 45.1% of females reported ≥5 ACEs. Almost 97% of males and over 98% of females reported at least one ACE. Evidence clearly indicates that ACEs are common among justice-involved youth, but answers about how ACEs impact delinquency, and through what mechanisms, remain unresolved.
Malvaso et al. (2022, p. 5) reviewed 124 studies on ACEs and delinquent youth and found that about 21% of them “were based on data collected from the same facilities.” About 13% (n = 16) of the studies used the FDJJ data source, and six of them used the same sample. Data for these studies included 64,329 youth who aged out of the FDJJ between 2007 and 2012. In this data, ACE scores were constructed from the Positive Achievement Change Tool (PACT). This fruitful data source has significantly contributed to the knowledge base for understanding how ACEs affect this group, and researchers have employed an array of analytical strategies. Their contributions should not be underestimated; however, they should be balanced against findings from other justice-involved populations.
One study from this data source found four indicators increased recidivism; physical neglect, family violence, household substance abuse, and an incarcerated household member (Baglivio et al., 2014). Further analysis found direct and indirect effects of ACEs through negative emotionality (Wolff & Baglivio, 2017a). Wolff and Baglivio (2017b) discovered that higher ACE scores shortened time between prior and later arrests. Narvey et al. (2021) found that empathy buffered the effects of ACEs on recidivism. A higher number of ACEs predicted earlier first arrests, increased likelihood of arrest and offending (Baglivio et al., 2015). Fox et al. (2015) compared serious, violent, and chronic offenders and those who committed just one offence. They gauged the utility of using the ACE index (eliminating parental separation) as an effective screening tool for justice-involved youth to identify these potential future behaviors. “For each additional ACE that a child experience(d), the odds of becoming (a serious, violent, or chronic) offender increase(d) by 35% even when controlling for gender, race, age of onset, impulsivity, peer influence, and family income” (Fox et al., 2015, p. 169). Similarly, Perez et al. (2018) found both direct and indirect effects of ACEs on serious, violent or chronic behaviors through aggression and impulsivity and deviant peer imitation, school difficulties, substance abuse, and mental illness. Wolff et al. (2018) identified five typologies from the same nine indicators used in Fox et al. (2015) and introduced community-level characteristics as controls. Community disadvantage correlated with the highest ACE adversity type. Zettler et al. (2018) assessed the impact of ACEs on residential placement and found that several factors (higher ACE scores for males, Blacks, and Hispanics) increased the likelihood of residential placements prior to age 17. Baglivio et al. (2021) gauged the effects of ACEs on victim selection. They found that higher ACE scores increased violent offences against family members and decreased them against strangers. Studies from this data source found that ACEs increase juvenile justice involvement, but other studies on this population produced mixed results.
One of the earliest national ACE studies looked at their effects on adolescent dating relationships (Miller et al., 2011). In this study, 5,130 adults from the National Comorbidity Survey Replication were asked about dating violence they experienced or perpetrated against others before the age of 21. They found that their ACE index accounted for more than half of the physical violence in dating relationships. Another national study found that ACEs at as young as five increased delinquency in adolescence and 75% of respondents had ≥1 ACE, while 12% had ≥4 (Jones & Pierce, 2022).
Not all studies on at-risk youth have supported ACE’s impacts on behavior. Pierce and Jones (2022) assessed gender differences and found that ACEs explained delinquency for girls, but not for boys. Bonner et al. (2020) and DeLisi et al. (2017) studied 2,520 adjudicated males in an intake center in 2009 and introduced the concept of chaotic homes indicative of crowded living conditions and frequent moving in and out of the house by family members. Bonner et al. (2020) combined those effects with sexual, physical, and emotional abuse to predict homicide, sexual offences, and serious property offences, and could not predict offence type. Connolly and Kavish (2019) studied siblings from the National Longitudinal Survey of Youth, 1997. Their nine-item adversity index differed from items traditionally used in ACE studies and included victimization by bullying and the style of parenting, for example. ACEs explained more immediate self-reported delinquency but not later onset delinquency controlling for genetic and shared environmental effects (Connolly & Kavish, 2019).
Some ACE studies on justice-involved youth analyzed smaller, localized samples, and they too produced mixed results. Bielas et al. (2016) studied 130 males in a juvenile detention center in Zurich between 2010 and 2012 to see if ACEs predicted disruptive behavior disorders, substance use disorder, and several mental disorders. Controlling for the effects of irritability and other covariates, ACEs were unsuccessful for predicting disruptive behavior or substance use. Clearly more research is needed in the ACE literature on justice-involved youth.
The Effects of ACEs on Violence Against Others and Suicidal Behaviors
Suicidal behaviors are studied more often than violence against others in the ACE research, and ACEs are shown to increase risk (Dube et al., 2001, 2003; Elkins et al., 2019; Felitti, 2002; Felitti et al., 1998; Kaess, 2019; Kaess et al., 2013; Perez et al., 2016; Springe et al., 2016). Dube et al. (2003) assessed health impacts of ACEs across four birth cohorts back to 1900 and found that regardless of historical cultural changes in the country, ACEs increased suicide risk. Felitti (2002) found a 1,220% increase in attempted suicide between persons with an ACE sore of zero and ≥4. Brockie et al. (2015) found an increase of 37% in attempted suicide per ACE in a sample of Native American youth. Castellvi et al.’s (2017) meta-analysis found a combination of exposures to interpersonal violence significantly predicted suicidal behaviors, and risk of suicide doubled with exposure to child abuse (Castellvi et al., 2017). Several other studies found association between physical child abuse and later suicidal behaviors (Dube et al., 2001; Franklin et al., 2017; Sigfusdottir et al., 2013). Some evidence suggested that ACEs also lead to non-suicidal self-injury (Kaess et al., 2013). Much of the ACEs research has found it leads to depressive symptoms (Anda et al., 2002; Elovainio et al., 2015; Schilling et al., 2007; Tsehay et al., 2020). Depression is a conclusive risk factor for suicidal behaviors (Carballo et al., 2020; Chapman et al., 2004). Yu et al. (2017) found that violence against others increases with earlier diagnoses of depression in three longitudinal cohort studies of adolescents. Depression may mediate the effects ACEs on suicidal behavior such that when depressed individuals also experience ACEs, both forms of violence may increase.
ACEs not only increase suicide risk, but they are also conducive to violence against others. Widom (1989) first explained the phenomena whereby abused children are likely to grow up and be abusive to others as the “cycle of violence.” Since her seminal research, the association has been studied in multiple disciplines, and the evidence is strong for this association (Alfaro, 1981; Baldry, 2003; English et al., 2002; Grebstein & Van Wyk, 2016; Lansford et al., 2007; Paperny & Deisher, 1983; Rivera & Widom, 1990). In a review of the literature, Maas et al. (2008) concluded that child physical abuse was the most persistent precursor for youth violence. Exposure to parental interpersonal violence (PIPV) combined with child abuse, exacerbates violence (Cuevas et al., 2013; Hamby et al., 2011; Herrenkohl & Herrenkohl, 2007; Listenbee et al., 2012). Malvaso et al. (2018) examined the independent effects of ACE measures on violence in a study of convicted youth in Australia between 1995 and 2012 and found that persistent maltreatment increased the likelihood of violence against others by 33%. Brumley et al. (2017) found that the effect of ACEs on violence was mediated by college and fatalistic expectations.
A single study has assessed ACE dose effects on violence against others and suicidal behaviors in the same study. Duke et al. (2010) used self-report data from school children from 2007 and constructed an ACE index of physical and sexual abuse, witnessing abuse, and family substance abuse. They found that the risk of violence against others increased for boys with ≥4 ACEs by 2.7 times, and it increased suicidal behaviors 10-fold (Duke et al., 2010). Some evidence suggests that suicidal behaviors and violence against others are correlated (Flannery et al., 2001). Violence against others and suicidal behaviors may have ACEs in common and this link is understudied.
General Strain Theory and ACEs
Several theories have explained the relationship between ACEs and delinquency, but one is particularly adept for explaining why a higher dosage of ACEs is more likely to result in violent rather than non-violent behavior in adolescence. In Agnew’s (2006) general strain theory, strains are akin to adverse childhood experiences. They introduce something unwanted, remove something wanted, or block a goal. They are more likely to lead to violence against others when they are frequent, recent, are expected to continue for a long time, or they block core needs. Strains that are unjust, weaken ties to legitimate traditional relationships, or create opportunities or pressures to resolve them through violence increase its risk. Hay and Meldrum (2010) argue that some general strain theory studies may have overlooked self-directed violence and it too can be an outcome of strain in the same way as violence against others. Walls et al. (2007, p. 222) argue that suicide “may represent a clear-cut yet irreversible escape from strain and the negative emotions associated with it, as well as an emotion-driven reaction to the inability to escape.” Strains in childhood tend to include parental rejection, child abuse, and neglect (Agnew & Moon, 2018). They can also come from cultural patterns such as poverty or racism, so that Blacks, Hispanics, and Native Americans, who tend to face intersectional oppression, may be more likely than others to experience strains. Males are socialized to experience the kinds of strain that are conducive to violence (Agnew & Moon, 2018).
Agnew and Moon (2018, p. 455) explain that “the high magnitude of strains conducive to violence reduce the ability of individuals to cope in a legal manner.” They experience anger, which makes it more difficult to negotiate conflict, and reduces perceived costs of violence. Since angry children are much more difficult to control, parents lose their ability to enact social control. Angry children are forced out of conventional circles and into friendship networks that consist of others like them, where they learn how to resolve strain with violent behavior. There is evidence to support the idea that anger may condition the effects of maltreatment on violence (Widom et al., 2006).
Low self-control may also mediate the effects of strain on delinquency (Agnew, 2005). “High magnitude” strains are ones that are seen as unjust and are more likely to lead to crime than others, especially when they “are associated with low self-control,” and/or “create some pressure or incentive to engage in criminal coping” (Agnew, 2005, p. 27). Gottfredson and Hirschi (1990) explained that low self-control is a composite of immediate gratification, an inability to plan, a preference for physical rather than cognitive activities, risk-taking, self-centeredness, avoidance of complex tasks, and minimal tolerance for frustration. People with low self-control are often irritable and aggressive (Agnew, 2005). Taken together, these characteristics increase the chances of violence (Agnew, 2005). Gottfredson and Hirschi argued that low self-control results from ineffective socialization early in life, which is consistent with ACEs. Layne et al. (2014) found that ACEs increased risky behavior in a sample of adolescents who reported at least one type of trauma, and ACEs increase irritability (Bielas et al., 2016). Low self-control and anger may mediate the effects of ACEs on violence, but traditional studies on general strain theory garner little empirical support.
Mazerolle and Maahs (2000) argued that tests of strain theory often fail to produce significant results because researchers focus on a single factor instead of assessing the cumulative effects that produce chronic strain. Sharp et al. (2012) contradict this assumption finding no differences in the explanatory power of individual strains versus cumulative strains conceptualized as ACEs on substance use of female prisoners. In each study, a strain scale was created. Mazerolle and Maahs (2000) divided it into high, medium, and low strain. Then they assessed the effects of each of the three levels of strain on general delinquency mediated by delinquent peers, behavioral propensity, and moral belief. They also examined the effects of each level of strain on delinquency controlling for mediating conditions. They confirmed that strain increases delinquency, and the more chronic the strain is, the higher the likelihood of delinquency. Mazerolle and Maahs’ (2000) analytic strategy adheres to the same general logic of ACEs research when in most studies, researchers assess the cumulative and dose effects of ACEs. General strain theory explains why certain kinds of strain/ACEs increase the chances of violence against others and suicidal behaviors, and under what conditions. “General Strain Theory is based on a simple idea: if you treat people badly, they may respond with violence” (Agnew & Moon, 2018). The same logic applies in ACEs research.
The Current Study
The current study measures the impact of ACEs on violence against others and on suicidal behaviors for troubled adolescent boys. ACEs are identified as strains, and low self-control, anger, and depression are assessed as mediating factors. Three hypotheses that are derived from general strain theory and research on ACEs are tested. (1) Dose effects of ACEs on violence against others and suicidal behaviors increase the likelihood of these outcomes; (2) These dose responses remain when controlling for other pertinent variables (race/ethnicity, age, poverty, anger, self-control, and depression); and (3) low self-control, anger, and depression interact with ACEs to increase risk of violence against others and suicidal behaviors.
Method
For this study, data come from the Ocean Tides database. Ocean Tides is a fully accredited school and residential facility for troubled adolescent boys. This database is described in Van Wyk (2021).
From 1975 through 2015, the residents were sentenced to serve on further order of the court (FOC) in temporary community placement (TCP) from the Rhode Island Training School (RITS), the youth prison in the state. Since 2017, 17 (<1%) of the residents were not adjudicated delinquent, but were incorrigible at home; on probation, referred from Diversionary Court, or they were designated as youth in need of residential treatment by the Rhode Island Department of Children, Youth, and Families (DCYF). They spend their days alongside the resident population and are very similar to the residents at Ocean Tides on FOC/TCP. Court officials, in conjunction with Ocean Tides staff make decisions to place boys at the facility. It is a non-locked facility that includes an in-house school, vocational, and rehabilitation programs. Residents are males ages 13–18 ( Data includes information on 2,195 court adjudicated boys who entered the Ocean Tides program to serve 3 to 12-month terms since 1975 through December 2019. When Ocean Tides accepts a new resident, they receive information from DCYF and the juvenile court that includes police and court records, educational records and test scores, counseling transcripts, social worker and home visit reports, and health records. Ocean Tides gathers further information via intake interviews with each boy and his custodial parents. They also administer behavioral tests. Since its inception, these have included the Youth Self-Report, the Ohio Youth Problems, Functioning, and Satisfaction Scales, and the Child and Adolescent Needs and Strengths assessments. To create the Ocean Tides database, a codebook was created that corresponded to the information in the boys’ files. Then, each resident’s hard-copy file was culled by researchers for information to record into an electronic database (p. 14).
It is an archival retrospective study that does not rely on recall from informants since the source of information is documents that were written in real time by different people and agencies involved in the boy’s life.
Each completed file took approximately five hours to record. IRB approval has been maintained on the project since its inception in 2003 and continues today. Data entry personnel are trained and supervised to maintain uniformity, reliability, and validity. The Ocean Tides database is not a sample but a census of all the residents across 44 years. This database is not yet available to the public but results for this study are available upon request (Van Wyk, 2021, p. 14).
This database “offers unique benefits for studying the effects of ACEs. First, the information was cross-checked for accuracy against multiple sources (by social workers, police, teachers, home visits, clinical reports, diagnostic results, interviews with parents, and interviews with the boys)” (Van Wyk, 2021, p. 10). As such, it is unlikely that ACEs or behaviors as serious as violence against others or suicidal behaviors were missed. Even though some behaviors such as witnessing abuse between parental figures were not considered as child abuse as early as the 1970s, it was still culturally unacceptable to fight in front of children and so these events were recorded in the files by someone, usually a social worker, clinical counselor, or the resident. The data is not subject to social desirability in the way that only self-reports are. The information for each resident is not dependent on the recall of a single informant, and it is not subject to false negative reports as are retrospective adult surveys on ACEs (Hardt & Rutter, 2004). Thirdly, although there is a single datapoint for each variable, this is not a typical cross-sectional study but instead gleans information in real time from the resident’s lives as incidents occurred. “The Ocean Tides database is also not a traditional panel … study of a single group of respondents,” and “so it does not suffer from attrition problems” (Van Wyk, 2021, p. 10).
This is a study of troubled male adolescents. Prevention and intervention programs should be gender-specific since evidence suggests that ACEs are more likely to lead to delinquency for girls than for boys (Pierce & Jones, 2022). Consistent with strain theory, certain kinds of strain may lead to violence for boys, but not for girls (Agnew & Moon, 2018). “Limiting the study to males allows for a fuller exploration within this population” (Van Wyk, 2021, p. 10).
Dependent Variables—Violence Against Others and Suicidal Behaviors
Flannery et al. (2001) found that violence against others and suicidal behaviors are strongly correlated, and there is some evidence that they may share precursors. General strain theory can explain how and why ACEs may increase self-directed and other-directed violence. Certainly, in the ACE literature, there is a preponderance of evidence suggesting that ACEs increase suicidal behaviors (Dube et al., 2001, 2003; Felitti, 2002; Felitti et al., 1998; Kaess, 2019; Kaess et al., 2013; Perez et al., 2016), and ACEs increase risk of violence against others (Castellvi et al., 2017; Malvaso et al., 2018).
A single suicidal behavior variable is constructed that includes attempts and self-harm having occurred within 1 year leading up to sentencing. In the original database, suicidal attempts and self-harm were also coded as having occurred while the resident was under the care of Ocean Tides (1.8%, n = 39), and prior to 1 year leading up to sentencing (6.2%, n = 136). Suicidal behaviors were indicated as such by clinicians or admitted by residents in their responses to standardized assessments. Where there was not a clear indication that the resident wanted to die, self-inflicted harm was coded as such. Accidental or minor self-harm, such as injuring a hand during a fight, was not included in this measure. Suicidal attempts and self-harm that occurred within the year prior to sentencing were used instead of all past suicidal behaviors to control for time ordering between ACEs and these behaviors. Suicidal behaviors that occurred while the boys were in the care of Ocean Tides were excluded since evidence suggests that incarceration of any kind may increase risk of suicidal behaviors. In fact, 30 (76.9%) of the 39 boys who did engage in suicidal behaviors while sentenced to Ocean Tides had never before exhibited these behaviors. It is important to note that the boys in the Ocean Tides program are on weekend passes and the data does not specify where the behavior occurred. Boys who had experienced either an attempt, self-harm, or both within the year preceding sentencing were coded as 2 (4.4%, n = 96) and those who did not were coded as one. Descriptive information is presented in Table 1.
Descriptive Information.

Violence against others while in the care of Ocean Tides are included in this study instead of all past violence to control for time ordering between ACEs and violence against others. In the original database, there is no record of exactly when past violence occurred. For this study, VAO is coded as 2 for violence constructed from all sources in the database (n = 576, 26.2%). Residents’ behavior is supervised by staff and teachers on weekdays and monitored during weekend home passes. Violent arrests while in the care of Ocean Tides included simple assault, aggravated assault, attempted murder, robbery, and sexual assaults (n = 84, 3.8%). These arrests are included in the VAO variable. Other acts of violence that residents were not arrested for were included: physical fights and other violent altercations that were not considered as self-defense. Arguments and general poor behavior were not recorded as violence against others. Just 11.3% (n = 89) of boys who had not previously behaved violently, did so at Ocean Tides for the first time, and 65.4% (n = 921) of boys who had acted violently before, did not do so at Ocean Tides.
Independent Variables—Strain/ACEs
Research on ACEs and general strain theory inform the selection of independent variables. They include 12 dichotomized variables whereby a score of 2 indicates the presence of the experience. They are neglect, parental interpersonal violence (PIPV), physical, emotional (including verbal), and sexual abuse, family mental illness, loss by death, family substance abuse, family instability, household overcrowding, residential instability, and family incarceration. All instances that occurred prior to the boy’s residency at Ocean Tides were included.
Neglect is physical abandonment (except by death, as this is captured in another variable) and/or emotional rejection by a biological parent or intentional economic neglect (not produced solely by economic disadvantage) by a parental figure (n = 1,307, 59.5%). Parental figures include anyone, related or not, who served in that role at any time during the boy’s lifetime. Parental interpersonal violence is measured as either witnessing, overhearing, or otherwise knowing about physical and/or sexual violence between parental figures (n = 410, 18.7%). Three more forms of child abuse are measured; physical (n = 446, 20.3%), sexual (n = 34, 1.5%), and emotional (n = 1,261, 57.4%). The original child abuse variables in the database are independent of one another such that physical child abuse, for example, is not also measured as emotional abuse.
Family mental illness includes any form of mental illness or depression for anyone living in the child’s household in his lifetime leading up to sentencing (n = 428, 19.5%). Loss by death is measured as the loss of anyone with whom the boy felt an emotional connection (n = 682, 31.1%). Family substance abuse includes abuse of alcohol, prescriptions, and/or illegal drugs, and includes measures for parental figures and all other relatives (n = 1,010, 46.5%). Family instability refers to the changing structure of the family and recognizes that some single-parent families are stable and supportive, whereas traditional measures of divorce, separation, and single-parents are less sensitive to diverse conditions. A stable family is one in which the family structure did not change for at least 5 years of the boy’s lifetime. Since the boys are 13 to 18 years old, this means about one-third of a resident’s lifetime. Otherwise, the family is considered as unstable (n = 1,187, 54.1%). A household is considered as overcrowded when there is not a bed for each member of the household or each romantic couple in the household (n = 157, 7.2%). Residential instability is measured as the boy having changed residences at least five times in his young lifetime (n = 498, 22.7%). Family incarceration is a relative who the boy felt emotionally close to in his lifetime who was separated from him by incarceration (n = 867, 39.5%). A single ACE index combines all 12 indicators and ranges from 0 to 12 counting each type of exposure for each case (
Mediating and Control Variables
Informed by general strain theory, anger, and self-control may mediate the effects of strain on violence against others, such that strain lowers self-control and increases anger, which each in turn, increase violence against others. There is some evidence that aggression may also influence suicidal behaviors (Perez et al., 2016), but anger is slightly different from aggression. Someone can be aggressive; bullying others, but that does not necessarily mean that they are angry. Aggression is a behavior, while anger is an emotion that often, but not always drives aggression. Therefore, aggression should not be included in the anger variable. There is an anger variable in the database, but there is also a measure of having a bad temper that is quick to ignite that could also be construed as anger. These measures come from all sources, including self-assessments. Anger and bad temper were originally coded as a slight, moderate, and severe problem. A combined anger variable for this analysis is coded 1 (36.3%, n = 796) for no sign of anger or bad temper, 2 (9.2%, n = 202) for having a slight problem with one or both, 3 (28.7%, n = 630) for moderate problem with one or both, and 4 (25.8%, n = 567) for a severe problem with one or both, defined as interfering with functioning and responsibilities. A second anger variable dichotomizes this construct so that 1 is no anger problem (n = 796, 36.3%) and 2 is at least a slight problem with anger (n = 1,399, 63.7%).
Low self-control is constructed from impulsiveness, risk-taking behavior, and self-centeredness. Although having a bad temper is both an indicator of anger and low self-control, bad temper is only included in the anger variable to create independent measures. One combined low self-control variable for this analysis is coded as 1 (25.1%, n = 551) for no sign of impulsiveness, risky behavior, or self-centeredness, 2 (6.6%, n = 145) is a slight problem with any of them, but no more severe, 3 (29.4%, n = 645) is a moderate problem with any of them (but no more severe), and 4 (38.9%, n = 854) is a severe problem with any of them. Someone with a 4 for low self-control, for example, has a severe problem with at least one of these issues. A second self-control variable is dichotomized so that 1 is no problem with self-control (25.1%, n = 551) and 2 is at least a slight problem with it (74.9%, n = 1,644).
Depression may mediate the effects of ACEs on suicidal behaviors since evidence indicates that ACEs increase depressive symptoms (Tsehay et al., 2020), and depression is often associated with suicidal behaviors (Carballo et al., 2019). Depression is also associated with increased violence against others (Yu et al., 2017). Depression is a dichotomous measure of clinically diagnosed depression of all types at any point in the boy’s lifetime (n = 331, 15.1%). The measure does not include depression that was diagnosed at Ocean Tides since incarceration can often lead to depressive symptoms that may not be due to prior events (James & Glaze, 2006).
Control variables include poverty, age, and race/ethnicity. The most utilized controls in maltreatment-violence studies are age, gender, ethnicity, and socioeconomic status (Malvaso et al., 2016). Gender is already controlled by the data. Poverty is measured as a dichotomous variable such that a family living check to check that can provide basic family needs or one that is financially better off than that is 1, and 2 (n = 826, 41.5%) is a family that either lives on government assistance or no assistance but cannot provide basic family needs. Race/ethnicity is dichotomized so that 1 is white, non-Hispanic and 2 includes all racial minorities and Hispanics (whether white or non-white) since the strain literature regards all Hispanics as potentially suffering from systematic oppression that white non-Hispanics do not experience (Leeper Piquero and Sealock, 2010) (n = 887, 45.9%). Age is constructed by subtracting birth year from the year of arrival in the Ocean Tides program.
Results
Pearson correlations for ACE indicators, violence against others, and suicidal behaviors are in Table 2. Most forms of child abuse in this study, family mental illness and family substance abuse each independently correlate well with the dependent variables, although family substance abuse produces a weak result. Family instability, household overcrowding, residential instability, PIPV, and incarcerated family member perform poorly in association with both dependent variables. Since these variables do correlate with other ACE indicators, and their influence in the ACEs index is theoretically important, they were retained as ACE indicators (analysis not shown, but available upon request). Physical abuse and death are correlated with violence against others, but not suicidal behaviors, but all other variables perform similarly by violence against others and suicidal behaviors (neglect, sexual and emotional abuse, family mental illness, and family substance abuses).
Pearson Correlations for ACEs and Outcomes (N = 2,195).

p ≤ .05. **p ≤ .01.
Data is missing only for age, race/ethnicity, and poverty. Van Wyk (2021, p. 21) explains the following: In the original construction of the Ocean Tides database, the presence of conditions and/or events was recorded. If no indication was noted in the boy’s file, then that case was recorded as null for that variable. Clearly, this process is not fool proof as some positive cases may have been recorded as negative if the information was not included in the boy’s file. Age, race/ethnicity, and poverty could not be coded in this manner since there was no way to assess these characteristics if no information about them was included in the file or if contradictory evidence from two or more sources prevented clarification.
Race/ethnicity is missing for 263 cases (12%), poverty status is missing for 204 cases (9.3%), and age is missing for 0.5% (n = 14) of the cases. Missing data is handled by listwise deletion. All analyses are completed using SPSS, v27.
Bivariate correlations for the main variables in the analyses are presented in Table 3. The ACEs/strain index significantly correlates with the outcome variables. The first hypothesis is confirmed. ACEs produce dose effects on violence against others and suicidal behaviors. As the number of ACEs increase, there is a corresponding increase in these outcomes.
Bivariate Correlations Among Independent, Moderator, and Dependent Variables.

p ≤ .05. **p ≤ .01.
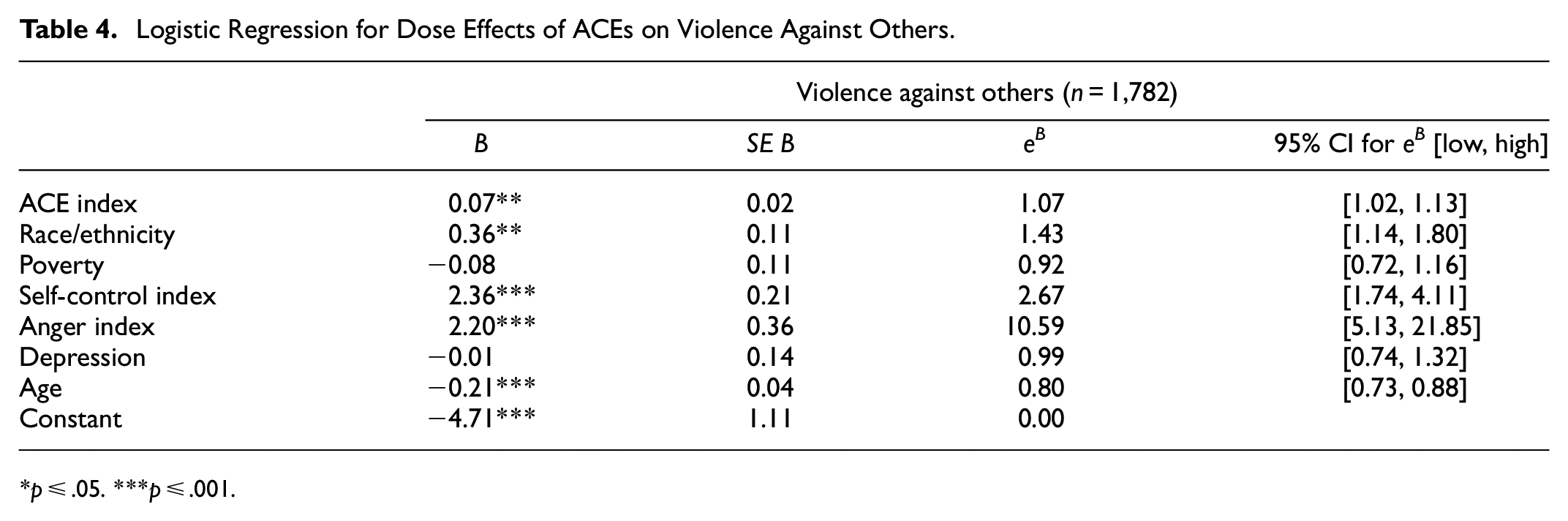
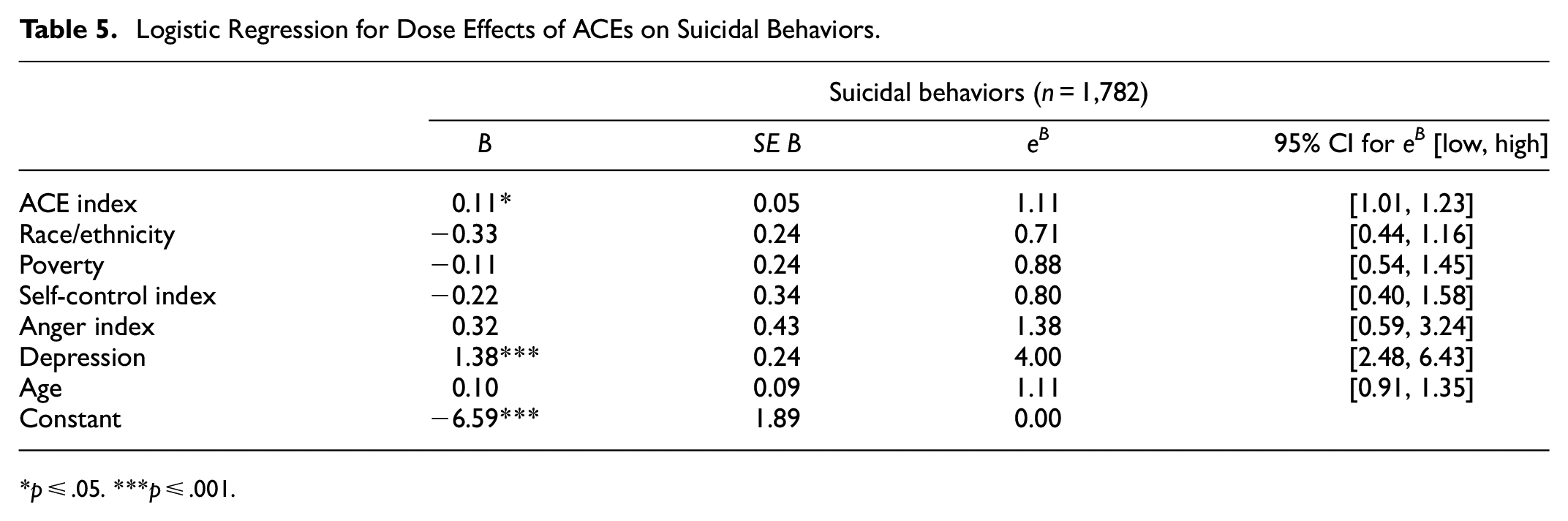
Separate logistic regression models are assessed for the effects of ACEs on violence against others and on suicidal behaviors (Tables 4 and 5). The second hypothesis is supported, that controlling for other pertinent variables (race/ethnicity, age, poverty, anger, self-control, and depression), dose responses of ACEs increase risk of violence against others (ACE, eB = 1.0, p =. 003, 95% CI [1.02, 1.13]) and suicidal behaviors (ACE, eB = 1.11, p = .029, 95% CI [1.01, 1.23]). Risk of violence against others increases for racial/ethnic minorities (eB = 1.43, p = .002, 95% CI [1.14, 1.80]), low self-control (eB = 2.67, p < .001, 95% CI [1.74, 4.11]), and anger (eB = 10.59, p < .001, 95% CI [5.13, 21.85]). Younger boys are at greater risk for violence against others than older ones (eB = 0.80, p < .001, 95% CI [0.73, 0.88]). Poverty and depression do not influence violence against others in the model. Depression (eB = 4.00, p < .001, 95% CI [2.48, 6.43]) is the only control that along with ACEs, predicts risk of suicidal behaviors in the full model.
Logistic Regression for Dose Effects of ACEs on Violence Against Others.
p ≤ .05. ***p ≤ .001.
Logistic Regression for Dose Effects of ACEs on Suicidal Behaviors.
p ≤ .05. ***p ≤ .001.
Assessing mediation when the conditional or dependent variable is categorical is tricky, particularly when these variables are dichotomous. In 2012, five leading statisticians highlighted and debated appropriate methods for dealing with issues presented in this type of analyses in a series of papers that appear in one volume of the Journal of Consumer Psychology. In this volume, Iacobucci’s (2012, p. 582) solution was presented and since then has been widely vetted and accepted by a host of “geeky rock stars” who together validate its accuracy and reliability for closely meeting necessary statistical assumptions. The same formula is used to test for mediation regardless of how each variable in the model is measured. MacKinnon and Cox (2012) point out that separate statistical packages are designed to do essentially the same thing, but Iacobucci (2012) manages to provide detailed, step-by-step instructions for calculating this simple formula that can be easily understood by ordinary researchers who are not statistical geniuses or do not have the resources to purchase multiple statistical software programs.

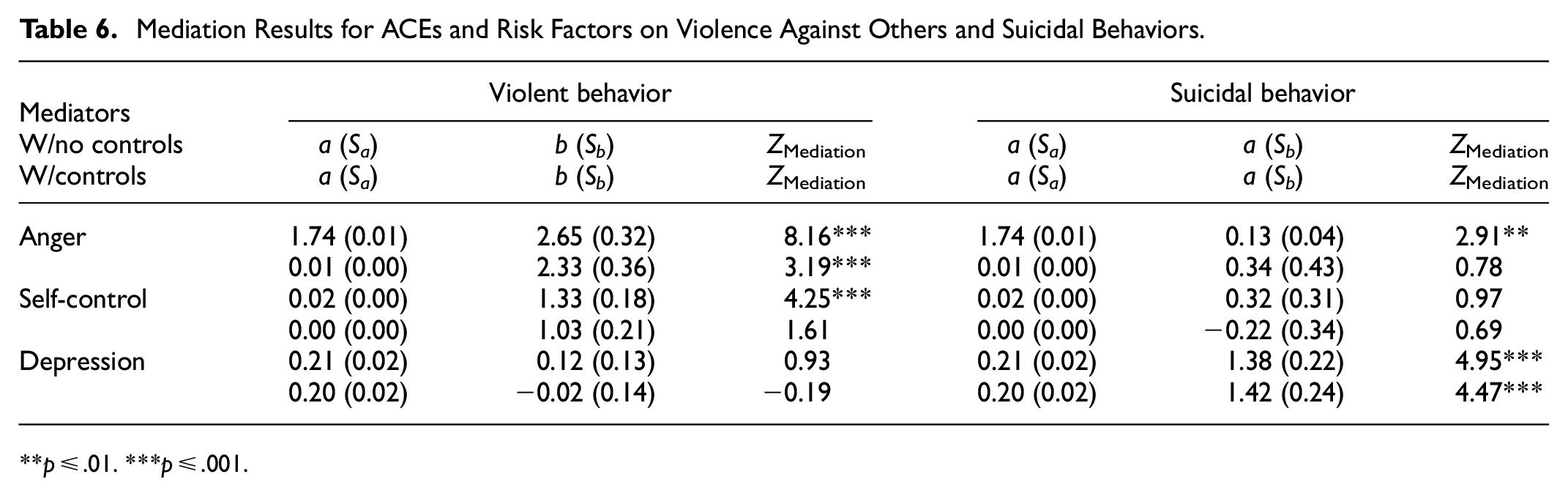
Iacobucci’s (2012) Zmediation formula uses results from two tests to calculate the statistical significance of mediation. In the model, X is the independent variable, M is the mediator, and Y is the dependent variable. As they pertain to the first test in the current analysis, X (ACEs) is measured as an ordinal-level variable that Iacobucci (2012) argues can be treated as a continuous one in the analysis, M (anger) is also treated as a continuous variable, and Y (violence against others) is dichotomous. To calculate the formula, a is the parameter estimate and Sa is the standard error from a linear OLS regression analysis (because the ACE index is being treated as continuous) for the direct effects of X (ACEs) on M (anger), b and Sb are similar statistics for M from a logistic regression analysis of the effects of X (ACEs) and M (anger) on Y (violence against others). These results are presented in Table 6.
Mediation Results for ACEs and Risk Factors on Violence Against Others and Suicidal Behaviors.
p ≤ .01. ***p ≤ .001.
The ZMediation score for anger is 8.16, which when compared to the standard normal significance cutoff for the two-tailed test of significance results in a significant p-value of <.000. This result means that anger at least partially mediates the relationship between ACEs and violence against others. An increase in ACEs produces an increase in anger, which increases the risk of violence against others. When Za and Zb are calculated from models that include all other controls (self-control, depression, race/ethnicity, and poverty), ZMediation = 3.22, (p = .001). So, controlling for the effects of the other variables, anger still mediates the relationship between ACEs and violence against others. Self-control mediates the relationship between ACEs and violence against others (ZMediation = 4.25, p < .000), but loses significance in the full model (ZMediation = 1.61, p = .107). Depression does not mediate the effects of ACEs on violence against others in either model (ZMediation = 0.93, p = .350, and in the full model, ZMediation = −0.19, p = .849).
The first column in Table 6 for suicidal behaviors is the same as the first column for violence against others because a and Sa represent the parameter estimate and standard error for ACEs on each of the mediators. Although anger mediates the relationship between ACEs and suicidal behaviors (ZMediation = 2.91, p = .003), this effect diminishes in the presence of controls (ZMediation = 0.78, p = .432). ACEs and suicidal behaviors are not mediated by self-control (ZMediation = 0.97, p = .327). Consequently, the full model produces similar results (ZMediation = 0.69, p = .489). Depression mediates ACEs on suicidal behaviors both in the independent (ZMediation = 4.95, p < .000) and full models (ZMediation = 4.47, p < .000). It is safe to say that results for the third hypothesis, that low self-control, anger, and depression mediate the relationship between ACEs and violence against others and suicidal behaviors are mixed.
Mazerolle and Maahs (2000) use an analytical strategy for assessing mediation that presents a more vivid illustration of the interactions tested in the previous analyses, although full models cannot be tested this way. These results are in Tables 7 and 8. All variables in these tables are dichotomized for ease of interpretation. The measure of ACEs is none, or ≥4 as prior research on ACEs has found differences in outcomes tend to be more prominent at this level (Duke et al., 2010; Felitti, 2002). In the first column of each table are baseline percentages that are used for comparisons in the analysis. Baseline results in Table 7 mean that 30.1% of boys with ≥4 ACE are violence against others compared to 13.5% who had no ACEs (χ2 = 19.59, p < .001). For high ACEs, risk of violence against others increases from the baseline to 34.5% for low self-control, to 37.8 for anger, to 32.1% for depression. Analogously, for those with no ACEs, 13.5% were violence against others compared to 17.9% for low self-control, 24.4% for anger, and 18.2% for depression. In this analyses, all three mediators partially condition the effects of ACEs on violence against others.
Crosstabulations for Mediating Influences on Violence Against Others (n = 1,338).

p ≤ .05. **p ≤ .01. ***p ≤ .001.
Crosstabulations for Testing Mediating Influences on Suicidal Behaviors.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Within each category of ACEs there is a greater risk of violence against others for those with low self-control, who are angry, or depressed. For example, 3.5% who had no ACEs and were not angry were violence against others compared to 24.4% who had no ACEs and were angry (χ2 = 15.11, p < .001). For high ACEs, 11.0% who were not angry were violence against others compared to 37.8% who were angry (χ2 = 82.30, p < .001). This same pattern exists for all three variables holding ACEs constant at zero or high levels. Differences within categories of ACEs are statistically significant for low self-control and anger, but not for depression, which reiterates individual findings from the Zmediation scores presented earlier, but the crosstabulation provides a more detailed picture of individual relationships. Each analytical strategy has its merits and shortcomings.
The third row of the table holds mediators constant to asses impacts of ACEs on violence against others within each mediator category. For example, the effect of ACEs on violence against others for boys with high self-control is not significant (χ2 = 3.50, p = .061) which means that high self-control slightly buffers the effects of ACEs on violence against others. For boys with low self-control, ACEs significantly increase risk of violence against others, which is consistent with general strain theory. Angry boys are slightly more likely to act violently when they have high ACEs (χ2 = 5.57, p = .018) than non-angry boys are (χ2 = 4.39, p = .036). For boys who have never been depressed, high ACEs increase risk of violence against others (χ2 = 17.88, p < .001), but for boys who have been depressed, ACEs have no impact on violence against others (χ2 = .94, p = .332).
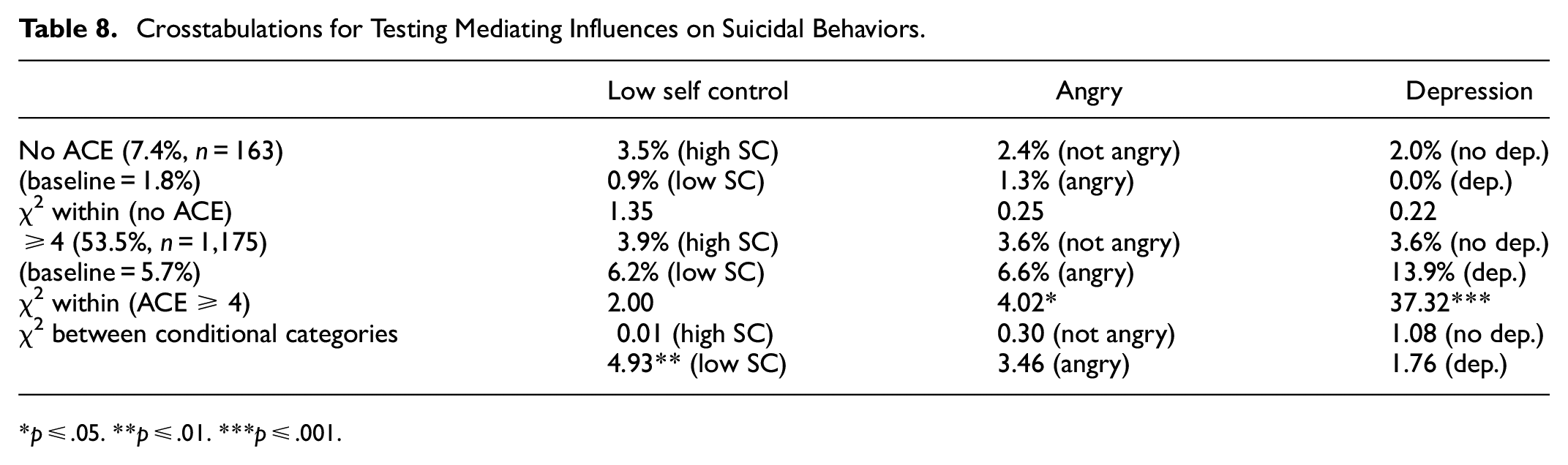
The same kinds of assessments are illustrated in Table 8 for suicidal behaviors. Just 1.8% of boys with no ACEs engage in suicidal behaviors, while 5.7% with ≥4 ACEs do (χ2 = 4.30, p = .038). For boys with no ACEs, history of depression has no impact on suicidal behaviors (χ2 = .22, p = .638). For boys with ≥4 ACE, 3.6% without a history of depression are at risk for suicidal behaviors compared to 13.9% with a history of depression (χ2 = 37.32, p < .001). Interestingly, holding depression constant (third row of Table 8), ACEs have no impact on suicidal behaviors for boys with no history of depression (χ2 = 1.08, p = .297), or for history of depression (χ2 = 1.76, p = .184). Although self-control exerts no discernable influence on suicidal behaviors holding ACEs constant, for those with low self-control, ACEs increase risk of suicidal behaviors (χ2 = 4.93, p = .026). So, boys with low self-control are at increased risk of suicidal behaviors when they experience ≥4 ACEs.
Discussion
Just 10.3% (n = 227) of the Ocean Tides residents experienced a single ACE. Over four times as many residents experienced two to four ACEs, and 82% of those who experienced one ACE, had at least one additional ACE. For those with only one ACE, family instability was most common (n = 54, 23.8%) followed by a history of family drug abuse (n = 47, 20.7%). Nearly 93% of residents experienced at least one ACE. These findings are consistent with the high occurrence of ACEs in justice-involved and other at-risk populations. Baglivio et al. (2014) found that 97% of males had at least one ACE, while Jones and Pierce (2022) found that 75% of at risk-youth had at least one.
Results suggest there is merit in questions Finkelhor (2018) raised about the utility of dose effects for predicting behavior, especially for justice-involved youth. Consistent with other studies, in this study physical, emotional and sexual child abuse, and neglect explain a greater proportion of risk for problematic behaviors than other ACEs, so simply summing events without weighting some of them may jeopardize predictability. Furthermore, all justice-involvement is not alike. Family instability, household overcrowding, residential instability, PIPV, and having an incarcerated family member do not correlate well with the dependent variables, possibly because the care they receive at Ocean Tides cushions these conditions of home, and perhaps in other types of care facilities, this pattern may not arise. These adverse experiences may have more immediate effects on violence against others that are not captured in the violence that occurs while in the care of Ocean Tides, or some other type of facility. This assumption is consistent with general strain theory which predicts that violence against others is at higher risk immediately following strain (Agnew, 2005). Another reason why family instability, household overcrowding, and residential instability were unsuccessful for predicting the outcomes may be that some boys whose families are unstable, reside in crowded conditions and move around a lot are emotionally supported by the host of people in their lives, while for those who experience these situations sporadically, this is a source of strain. This explanation is consistent with the immigration paradox. Marks et al. (2014) explain that first generation immigrants are less likely to engage in criminal behavior than are second generation immigrants because later generations lose protective factors. The insulation of first-generation immigrants protects them against risk factors. First generation immigrants would rely more heavily on extended family, move more often, and live in more crowded conditions than those who are U.S.-born (Marks et al., 2014).
When ACE indicators are combined into a single variable, ACEs increase risk of suicidal behaviors and violence against others controlling for self-control, anger, depression, race/ethnicity, age, and poverty. Mediator effects were tested and illustrated by Zmediation and χ2 analyses, and overall indicate that self-control, anger, and depression each partially mediates the relationship between ACEs and suicidal behaviors and violence against others. These relationships are complex, and they vary by the introduction of controls, and by which measure of ACEs is used. For regression and Zmediation analyses, the continuous measure of ACEs was used, and for the χ2 analyses, the dichotomous measure was employed. This also means that the sample slightly changed between the two procedures since boys with one to three ACEs were not included in the χ2 analyses.
The relationship between high ACEs and violence against others is partially mediated by anger and low self-control, while anger and a history of depression partially mediate the effects of ACEs on suicidal behaviors. Juvenile justice-involved boys who experience ≥4 ACEs and have low self-control are nearly 52% more likely to be violent. Boys with high ACEs who are also angry are nearly 65% more likely to act violently, and 20% more likely to engage in suicidal behaviors. Zmediation results find that the presence of controls weakens the mediation effects of anger on violence against others. High ACEs combined with a history of depression increase risk of suicidal behaviors by 100%, but closer inspection via crosstabulation of interactions among ACEs, depression, and suicide find interesting results. Whether someone has a history of depression or not, does not change the effects of ACEs on suicidal behaviors. However, boys who experience ≥4 ACEs are 25% more likely to engage in suicidal behaviors if they have a history of depression. For boys with high ACEs, the presence or absence of depression may at least partially explain why one boy might react violently against others while another boy may engage in suicidal behaviors instead. It could also be true that boys with high ACEs who are not depressed engage in attempts and self-harm, but people who are depressed actively commit suicide. Of course, this relationship cannot be tested with the current data.
As predicted by general strain theory, racial minorities and Hispanics are at increased risk of violence against others when controlling for other risk factors. general strain theory explains that people in poverty encounter biases (strains) that may make them angry and reduce inhibitions against violence against others (Agnew & Moon, 2018). The same explanation for increased risk of violence against others for boys in poverty is not supported in this study. Again, Ocean Tides may serve as a buffer against the effects of poverty, at least temporarily, but the effects of racial/ethnic biases run deeper. Younger boys are at greater risk of violence against others. Race/ethnicity, poverty, and age do not affect risk for suicidal behaviors. Race/ethnicity effects on suicidal behaviors contradict prior research that consistently finds whites are at higher risk (Stone et al., 2017), and they contradict predictions by general strain theory that whites would be at lower risk (Agnew, 2005). However, these patterns in other studies are typically rather weak. Their effects on violence against others and suicidal behaviors wane in the presence of ACEs. However, economic hardship and experiences of systematic oppression are also adverse childhood experience. Instead of controlling for the influences of these experiences, they may need to be included in the ACE index. Some ACE studies do include poverty in their ACE indexes with some success (Hughes & Tucker, 2018). However, it was outside the scope of this paper to assess comparisons between ACE indexes that included poverty and race/ethnicity and controlling for them instead.
Study Limitations
Precise control over timing of some of the variables is not possible. Suicidal behaviors occurred within the year preceding sentencing, and some ACEs (PIPV, child abuses, family incarceration, and/or the death of a loved one), and depression may have also occurred in the year preceding sentencing. However, timing is only an issue for cases where these things occurred for the first time in the boy’s lifetime during that year. The U.S. Department of Health & Human Services (USDHH, 2021, p. 21) reports that over a quarter of all child maltreatment occurs by age 2 and the “rate of victimization decreases with the child’s age.” Ninety-three percent of all child maltreatment reported in the United States occurs by age 8 (USDHH, 2021). The average age of Ocean Tides residents is 16, so it could be argued that at least most of the suicidal behaviors in this population occurred after these kinds of adverse childhood experiences occurred. Anger and self-control are lifetime measures that include the boys’ residencies at Ocean Tides. Although violence against others represents only violence at Ocean Tides, we cannot be certain that anger or self-control did not occur after violence at Ocean Tides. It is also possible that anger and low self-control could have been present prior to ACEs and that these conditions could increase the chances of strain/ACEs occurring (Agnew, 2005). However, based on theoretical predictions from general strain theory, we would expect ACEs to occur first and then possibly initiate the reciprocal occurrence of future events. In sum, some of the variables overlap within a 12-month period in the boys’ lives, so perfect sequencing of events is not possible.
Another concern about the data is that the Ocean Tides facility does not accept boys into the program who are extremely violent or suicidal at the time of adjudication or referral (Grebstein & Van Wyk, 2016). So, some of the most serious behaviors could not be assessed. Based on the patterns discovered in the current analysis, the omission of serious outcomes should have weakened the results of this study, not produced false evidence that supports the effects of ACEs on violence against others and suicidal behaviors.
Finally, ACEs do not explain all the variance in behavioral outcomes, no matter how ACEs are measured. Further, some research has tested the possibility that the effects of ACEs on negative outcomes are confounded by a combination of genetics and other familial variables. In this research differences in the effects of ACEs on negative outcomes (poor health, violent victimization, and antisocial behaviors) later in life between siblings and twins are assumed to be genetic, although specific genotypes are not identified. These studies have found that a combination of certain family characteristics among sets of twins attenuate the effects of ACEs on negative outcomes (see Connolly, 2020; Schwartz et al., 2019). Sibling information was not available in the current study, nor were more direct genetic measures.
Conclusions
The current study makes several important contributions to the ACE literature. First, it empirically general strain theory’s ability to explain the effects of ACEs on violence against others and suicidal behaviors. The research identifies shared risk factors for these outcomes (sexual and emotional abuse, family mental illness, and substance abuse), and confirms that violence against others and suicidal behaviors are correlated. Future research on ACEs should include violence against others and suicidal behaviors as outcomes, especially since they are both considered public health issues, and the intent of the original ACE research was to address public health. This study found that it is important to watch for suicidal behaviors in the presence of violence against others, and to monitor violence against others where suicidal behaviors may be anticipated.
Future research should explore weighting the effects of personal abuses such as neglect, physical, emotional, and sexual abuses in the ACE index, but to date, no systematic weighting process has been introduced in the literature. Future studies should also test the utility of including measures of poverty and race/ethnicity in the index instead of controlling for these effects. Researchers should also consider differentiating between anger as an emotion and aggression as a behavior.
Results from this study may guide strategies for preventing destructive behaviors. One finding in particular should be considered for juvenile justice-involved populations—that the presence of both anger and ACEs may increase risk of suicidal behaviors and violence against others. Juvenile justice strategies for the care of delinquent populations should include thorough testing for levels of anger, self-control, and the level, frequency, and duration of ACEs. However, thorough testing upon intake is not always possible, and that kind of testing may produce more accurate results later once trust is established between juveniles and their caretakers. A simplified testing tool like the ACEs index, may be easily administered early in the intake process or in diversionary efforts that could go a long way in protecting youth at risk of suicidal behaviors and violence against others. Jeske and Klas (2016) argued that functionaries in family court should learn about the effects of ACEs because adverse childhood experiences may interfere with someone’s ability to interact with and trust those who attempt to help them. Likewise, Larkin et al. (2014) encouraged social workers to do the same. It is important to reiterate that nearly 93% of the Ocean Tides residents had at least one ACE and 87% had ≥4. Malvaso et al. (2022) found that in most ACEs research, the percent of justice-involved youth with ≥4 ACEs ranged from 36.5% to 100%. These boys are just 13 through 18 years old and it is disheartening that they had to commit juvenile offences to receive the individual and family services they need to recover. It is time to start thinking proactively to reach families in need long before children strike back against others or against themselves.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by the State of Rhode Island and Providence Plantations, Rhode Island Justice Commission, Juvenile Justice and Delinquency Prevention/Intervention (JJDP) Grant # GR-7808 and 7580; also, from Grant No. 2015-JF-FX-0062 awarded by the Office of Juvenile Justice and Delinquency Prevention, Office of Justice Programs, U.S. Department of Justice. The opinions, findings, and conclusions or recommendations expressed in this publication are those of the author(s) and do not necessarily reflect those of the funding agencies.
Ethics Statement
This research has maintained IRB approval from the University of Rhode Island since 2003. The current expiration date is October 18, 2023. FWA: 00003132, IRB: 00000599, IRB Reference #: 1286943-12, Local Reference #: HU1718-220, Study Title: Ocean Tides Project: Ongoing Data Collection.