
Abstract
This article presents results from an exploratory study of what college students from northern Ontario think about and do to manage their mental health. Data gathered in semistructured interviews were analyzed using the constant comparative method. The purpose of the study is to advance our understanding of the ontogeny, substantive nature and deployment of mental health literacy (MHL). MHL has hitherto been defined as “knowledge and beliefs about mental disorders that aid their recognition, management or prevention.”. This definition effectively translates to knowledge of the contents of the Diagnostic and Statistical Manual of Mental Disorders, currently in its fifth edition. Results of the study suggest that the current definition of MHL is overly narrow, that individuals use knowledge of various types from various sources to manage their mental health, and that the literacies that inform mental health management practices are developed through iterative engagement in autologous knowledge-translation, at the core of which are cultured resonance, meaning-making, metacognitive evaluation, and heuristic experimentation. MHL is redefined as the self-generated and acquired knowledge with which people negotiate their mental health. Broadening the definition of MHL has potential to enhance the capacity of individuals and communities to manage mental health effectively.
Keywords
Introduction
The success of health literacy enhancement campaigns in Canada and other countries has given rise to a proliferation of initiatives intended to improve the level of mental health literacy (MHL) among general populations (Francis, Pirkis, Dunt, Blood, & Davis, 2002; Pape & Galipeault, 2002). These initiatives are premised on the conventional medical orientation to mental health and define MHL as “knowledge and beliefs about mental disorders that aid their recognition, management or prevention” (Jorm et al., 1997, p. 1). In its enunciation of mental disorders as its core frame of reference, this definition of MHL effectively translates to knowledge of the contents of the Diagnostic and Statistical Manual of Mental Disorders (DSM), now in its fifth edition. Although the intent of these initiatives is positive, there are strong reasons to argue for further circumspection regarding use of the DSM as the groundwork for MHL.
Notwithstanding the arguments regarding its inherent limitations (Caplan & Cosgrove, 2004; Houts, 2002; Jensen & Hoagwood, 1997; Kusan, 2011; Kutchins & Kirk, 1997; Laungani, 2002; Malik & Beutler, 2002; Szasz, 1974), the primary reason the DSM is problematic as the basis for MHL is that it is silent on mental health. That is to say that as a literature solely concerned with illness, the DSM does not account for the health-oriented literacies (e.g., resilience strategies, salutogenic principles, self-regulatory techniques, etc.) that individuals use to protect, promote, or recover their mental health. The inattention to these literacies is owing to the logical positivist ideal and the predisposition of its subscribers to define mental health as the absence of mental illness. This dichotomous and still dominant view of mental health has profoundly influenced mental health policy, research, and practice, and in no small measure has narrowly defined the public consciousness as to the workings and possibilities of the mind (Kusan, 2011).
Proponents of the current framing of MHL seek to bring people’s beliefs, attitudes, and understandings regarding mental health in line with the prevailing medical model. Global adoption of this definition would consolidate the DSM’s reification and further inculcate the public with the biases that predispose the biological determinist view. That biological factors comprise an essential piece of the mental health puzzle is universally accepted—there can be no thought, emotion, or behavior without a physiological host and the biochemical processes that occur within it. Nonetheless, acknowledgment of biology as a particular essence of all living things does not concede to it a function within the human equation as the singular determinate of human operations. Rather, the goal of achieving a comprehensive understanding of mental health, including insight into the etiologies of mental coherence and disorder, obliges us to take account of mind, body, and place as interdependent variables and as codeterminants of mental health.
The literature review for the study initially involved a search of the CINAHL, ERIC, Academic Search Complete, Social Work Abstracts, and Medline databases for English language articles dated from 1997 to 2011 that contain the term mental health literacy and found 207 distinct studies on MHL and three reviews of the MHL literature. The complete contents of the three literature reviews and at a minimum the abstracts for all 207 identified studies were examined. The studies were conducted in a variety of settings and varied in size. The larger studies focused on MHL enhancement projects, however, the majority involved a one-time assessment of knowledge and attitudes relating to mental disorders or a particular mental disorder within a given population. All 207 projects used Jorm’s DSM-based definition of MHL as a basic frame of reference informing the study’s purpose, methods, and interpretation of results. None of the studies questioned the appropriateness or completeness of the Jorm’s definition of MHL and none directly focused on the mental health effects of enhanced MHL (notwithstanding tenuous claims of reduced stigma). Rather, all of the studies proceeded on the assumption that enhanced knowledge of mental disorders represents improvement in itself, this by virtue of the more fundamental assumption that such knowledge positively correlates to enhanced mental health.
However, there is an expanding body of evidence that mental health and mental illness are not merely opposite sides of the same coin, and that learning to grow mental health predicts better outcomes for individuals and populations than does giving emphasis on avoiding mental illness (Keyes, 2002). Studies on “mindfulness” and the effects of metacognition on mental health consistently show that enhanced knowledge of one’s cognitive-emotional processes helps prevent mental disorders and improves mental performance and life satisfaction (e.g., Barahmand, Abolghasemi, & Jahanmohammadi, 2008; Carmody, 2009; Grossman et al., 2004; Kabat-Zin, 1982; Linehan, 1993; Segal, Williams, & Teasdale, 2002). Research on the mental health effects of place and social space suggest that people’s interpretations of information produced by and within the local physical and social environments profoundly influences their worldview, mental health management practices, and mental health status (e.g., Basso, 1996; Gatrell, Popay, & Thomas, 2004; Hudson-Rodd, 1998; Kelly, 2003; MacIntyre, Ellaway, & Cummins, 2002). Research on meaning-making tells us that people’s interpretations of environmental and internal events are significantly shaped by the knowledge (and attendant literacies) they bring to such interpretations which inevitably impact their mental health (e.g., Bruner, 1990; Frith, 2008; Seligman & Kirmayer, 2008).
In light of the evidence of the critical role of literacy within the meaning-making process and the fundamental importance of meanings made to the individual’s mental health management practices and their outcomes, it is crucial that we proceed to a better understanding of the origins, ontogeny, and substantive nature of the literacies individuals use to manage their mental health. Correspondingly, we must also seek to gain further insight into the mental health effects of place and social space. Toward that end, this study explores the types of knowledge, thinking processes, and behaviors that lay persons who have shared long-standing exposure to a common geo-cultural environment use to protect and promote their mental health.
Method
Two primary questions are explored in the study: What do college students from northern Ontario think about and do to protect and promote their mental health? What literacies do people draw on to manage their mental health and how are these literacies acquired and used?
A purposive sampling strategy was used in determining the site for the study and in the recruitment of participants. The Sudbury campus of Cambrian College was chosen to recruit participants based on its northern Ontario location, diverse student population and accessibility to the researcher over several months. Basic selection criteria required that participants be adult age, long-term residents of northern Ontario (minimally 5 years immediately preceding the study and all of the primary school years), available for minimally 2 interviews of 2-hr length each, and amenable to articulating the processes and substantive knowledge she or he uses in the management of her or his mental health.
In addition to meeting basic selection criteria, to reduce bias and gain multiple perspectives on mental health management, recruitment was conducted with the objective of achieving maximum variation in the sample. Accordingly, the sample comprised 9 men and 11 women of various adult ages representing cohorts in their second, third, fourth, fifth, and sixth decades of life and various cultural-linguistic backgrounds, including aboriginal, allophone (defined as having a first language other than English, French, or an Aboriginal language), anglophone, and francophone. Varied academic and career orientations were represented by recruiting participants from 10 discrete academic programs. Four of the participants were funded through the Second Career Initiative (designed to help unemployed workers transition to new careers in growing areas of the economy); four participants had accessed their current academic program through the Academic Upgrading Program (designed to enable students to obtain an Academic Career Entrance Certificate to subsequently gain admission into a mainstream academic program); and four participants were receiving services from the Glenn Crombie Centre (a Cambrian College agency providing a range of services to students with physical and or learning disabilities)—one with a learning disability, one with a physical disability, and two with a physical disability and a learning disability.
The recruitment strategy involved the placement of wall posters in high student-traffic areas of the college, direct appeals to students through class presentations, and snowballing via emails to faculty and information sharing among students. The majority of the eventual participants were initially apprised of the study’s purpose, requirements, and ethical considerations during the classroom presentations and all participants were provided this information when screened for eligibility. Notwithstanding the inclusion of individuals receiving Glenn Crombie Centre services, no information pertaining to the mental health history or mental health status of the participants was gathered during eligibility screening.
Two semistructured interviews were conducted with each participant during the second semester of the Cambrian College 2009-2010 academic year. The interviews were audio-recorded and subsequently transcribed verbatim by a third party. The first interview with each participant began with a brief review of the purpose of the study, namely, to explore what the participant thinks about and does to protect and promote her or his mental health. To facilitate discussion, concrete definitions of “protection” of mental health and “promotion” of mental health were read to each participant. When indicated, further explanation of the terms was provided. A prestudy review of the literature on MHL and related topics was conducted to aid with the formulation of a topic guide for use in the first interview. The intent of the Topic Guide was to provide a flexible structure for the interview while ensuring that each participant would have an opportunity to articulate his or her views on the nature of mental health and describe the knowledges, processes, and behaviors comprising his or her mental health management practices. Each participant was advised that although questions had been prepared in advance to help guide the interview, it was expected that in the main the questions asked would be based on her or his answers to previous questions.
Data collection effectively began with the researcher reading aloud the first question from the topic guide and inviting the participant to respond. A dialogic exchange would ensue with the researcher utilizing various interviewing techniques intended to maximize content originating with the participant. Questions from the topic guide were not always asked verbatim. Typically, the conversation would follow where the participants’ comments would lead, segueing from subject to subject across the topic guide as opportunities to do so arose. All of the participants were interviewed once before any participant was interviewed a second time. Based on a preliminary analysis of first-interview audio-recordings, transcripts, and memos, a topic guide for the second interview was uniquely constructed for each participant. The individualized second-interview topic guide served to provide the participants with an opportunity to clarify and expand on their previous responses and ensure comprehensive canvasing of the subject areas of interest.
The findings were arrived at through constant comparative analysis. In the present context, constant comparative analysis refers to the cross-case comparison of participant-generated data and the comparison of concepts emerging from the data with related concepts found in the literature. The literature, then, was consulted throughout the study and selected on the basis of topics emerging from the participants’ descriptions of their mental health management processes and practices. In addition, memoing (conceptual note taking) was undertaken during data collection and throughout the phases of analysis. The analysis involved inductive and deductive processes and utilized three progressive stages of coding—open, axial, and selective, as advanced by Strauss and Corbin (1990). Verification of the findings was based on researcher reflexivity, member checking, and triangulation with the literature.
Ethics approval for the study was obtained from the Research Ethics Boards of Laurentian University and Cambrian College prior to recruitment. Informed consent had been obtained from the participants prior to data collection, which included each participant’s consent to dissemination of anonymous in vivo data.
Analysis and Findings
Memos taken during the interviews and subsequent line-by-line analysis of the transcripts significantly contributed to the coding of data. The following memos describe key concepts that emerged from the data. Immediately below each memo are samples of the in vivo data from which it derives. For confidentiality purposes the names attached to the excerpts are pseudonyms.
Memos
Beliefs/epistemology
Participants’ beliefs about the nature of mental health tended to reflect their previous exposure to information related to mental health and the sources of this information. Participants who had been exposed to classroom training in psychology or health sciences tended to indicate a positivist, dichotomous view of mental health, at least in their expressed conceptualizations of it, if not at a practical level. Participants who had not received formal mental health education showed greater variance in their conceptualizations of mental health. Among this latter group, those suggesting a positivist epistemology tended to include vague descriptions of mental illness in their constructs of mental health, whereas those whose characterizations of mental health suggested a constructivist orientation typically did not include a reference to mental illness.
Participants commonly perceived physical and mental health as distinct but interdependent aspects of overall health, and in some cases also stipulated spiritual health as a unique and important component of health:
[Mental health is] basically how you take care of your psyche and how you perceive things . . . I definitely think that your physical health has a lot to do with it; they work hand in hand. (Chantelle) I think there’s four ways you know to be healthy—physical, emotional, mental and spiritual . . . good mental health is the balance of all of those things. (Tom)
The majority of the participants had not been previously exposed to formal mental health education. Those that had received this type of education tended to attach some measure of importance to it; however, for each of these participants the integration of this knowledge into their mental health management practices tended to be limited to maintaining a low level of vigilance regarding signs or “symptoms” of mental health complication:
I’m aware, my courses made me aware . . . we have learned a lot from therapists and nurses who worked with my mother . . . I got the bigger picture in my classes . . . a lot I already knew but I gained perspective . . . learned about theory . . . I pay close attention to what I eat and how much rest I get, I believe in that . . . I know the symptoms and won’t let myself get there. (Nicole) I haven’t taken anything on mental health . . . My mind is not curious about that . . . When I was 15, 16, 17, I didn’t know my direction, not really crazy . . . I was drinking and not getting along with people . . . When I was 19 I started to learn the Teachings . . . My emotions are in balance with my body and my spiritual self [when] I follow the Teachings of the Seven Grandfathers. (Tom)
Self-knowledge
All of the participants rated their present level of mental health at 6 or higher on a scale of 1 to 10, with 10 being the highest possible level of mental health. Most of the participants who had not previously received formal mental health education had a higher self-rating than any of those who had received this type of education. The positive self-ratings across the sample suggests that all of the participants had at least a functional measure of confidence in the knowledge and attendant literacies they bring to bear in the management of their mental health. The participants’ explanations of their self-ratings partially revealed their beliefs about how mental health is achieved and provided indications of the sources and types of knowledge they perceived as being relevant to its management:
Probably a 6 right now . . . It’s just sometimes the timing and the buildup of things that are the 4 missing [points on the self-rating scale] . . . I would say just right now because I am in school that kind of brings it down a little bit because that does stress me out even though I do well . . . having a job helps me get out and being with my friends helps me kind of stay normal, balanced. (Krysta) Yeah, 11, 12. Ok, 10. I don’t know . . . I’m a very happy guy. I don’t think there is anything I could improve about my mental health right now . . . This is where I accept science . . . what you put into your body is important. You are what you eat kind of thing and mentally what you put in your mind; it’s what’s important to your mental health. (Tom)
In addition to their beliefs about the nature of mental health, the participants’ self-ratings typically reflected a combination of objective self-knowledge and self-esteem. Participants invariably considered their physical composition (sex, physical dimensions, and attributes) to be a factor affecting their mental health. Relatedly, all of the participants perceived gender as a factor influencing their mental health and its management; albeit, the degree of emphasis consciously assigned to it varied considerably and attributions were often indirect. Participants’ descriptions of the mental health implications of gender involved various forms of personal knowledge (e.g., beliefs, values, objective self-knowledge) as well as propositional and procedural knowledge (see subsequent section on Open Coding for definitions). Although idiosyncratic differences between male and female participants’ characterizations of the relevance of gender are evident, no clear differences emerged between the sexes regarding sensitivity to gender or valuation of its level of impact on mental health.
My youth definitely contributes to what I think about my mental health . . . it’s definitely a plus towards my mental health . . . my gender is a minus towards my mental health . . . Women, from personal experience, are prone to having problems maintaining their mental health . . . Some of my personality traits I can attribute to my gender and so it affects my mental health to be a woman . . . We’re just more easily distraught and anxious because we care more about what other people think. (Chantelle) We’re judged by our gender and we judge ourselves that way too . . . I don’t try to be a so-called man’s man or lady’s man but it’s cool if women are attracted to me . . . there’s a way to be to have that . . . I don’t worry about it the way I used to and that’s working better for me and my mental health is better. (Shane)
Cultured-resonance
Participants described taking information on board when it had resonance. The data suggest that resonance is not ultimately determined by the inherent qualities of material objects or symbolic text, but rather by the individual evaluating these. Resonance of this kind is “cultured” in that it derives from the convergence of cultivated noticing skills and the availability of intelligible information that is perceived as being interesting and/or useful. Participants indicated that cultured resonance occurs in degrees and is affected by personal history and by present circumstances and goals:
I pay attention to information that relates to my life. I give more thought to information if I decide I’m going to use it. I have to have interest in it to learn it. (Alex)
Participants indicated that their contextualization of information affected their prioritization of it and their motivation for its assimilation. All of the participants described instances of straining to pay attention to information of low resonance (owing to marginal intelligibility) based on its high, contextualized valuation. Difficult to understand academic material was commonly cited as an example:
If it doesn’t make sense to me I just try harder. It usually works, but if I can’t get it I just move on and put it behind me. (Nicole)
Participants’ prioritization of information imparted to them by other persons invariably involved evaluation of the message and the messenger. Participants indicated that information coming from an intimate is more likely to have high resonance:
You’re more apt to change or listen when information comes from someone you care about. (Karene)
Some participants described evaluating the messenger based on a geographical valuation:
I’m more interested in information told to me from people from here [northern Ontario] who I can relate to. (Arvo)
Heuristics/strategies
Participants’ descriptions of their practices commonly indicated that heuristics were central to their process of evaluating and consolidating information. The formation of their heuristics typically included metacognitive activity such as self-talk:
I try to recognize what I might be saying, before it comes out of my mouth, evaluate it and maybe say it in a different way or not say it at all. Like everything else, I try to think about what’s happened before and not make the same mistakes. I’ve always done that with my emotions and everything else. (Janna) There are times when I’m alone I’ll say something out loud, it changes to hear what you’re thinking, it changes it and allows you to look at in a different way, but usually I do it silently. I talk to myself when I’m driving or at night when I’m at home . . . I’ll be devil’s advocate to myself . . . Usually it’s about school or relationships, friends, family or my girlfriend. I observe what I think and I try to understand it. The next day I try something different if I have to, or I just keep going and I’m ok with it. (Robert)
The participants typically did not associate affirmative mental health strategies with mental health, per se:
I guess I pay more attention to my mental health when I feel sad or maybe if I’m stressed out for a long time . . . I don’t normally think about it, say tell myself I’m going to think about my mental health . . . I try to do things to be happy but I just do them because I like doing them and so I feel good when I do them. (Jessica)
Mindfulness
Participants’ engagement in preferred activities typically involved heightened levels of mindfulness which yielded immediate and residual mental health benefits:
I’m in another headspace when I’m playing my guitar. Writing music too . . . I don’t have any self-consciousness, not jamming, playing for people . . . if I’m alone my thoughts are completely there . . . I’ve been anxious in class because I’m being criticized . . . you’re not free to just play your best. You’re thinking about mistakes, not just playing . . . I know I have to not think about be graded and just play. (Curtis)
Intuition
All of the participants described experiencing spontaneously occurring ideas as possible solutions to emotionally or instrumentally challenging situations. Some participants regarded “gut feelings” as being an important aspect of their mental health management:
I follow my gut feelings on everything, what people’s emotions are doing, what I need to do about it . . . My gut lets me know to change my emotions. (Robert)
Sense of coherence
Participants commonly identified a need to have a sense of coherence (cognitive and emotional) as being a core aspect of positive mental health:
I can handle a lot of pressure. I don’t get stressed out easily . . . if I know what’s going on, what it’s for, I can usually manage to at least get by. (Alex) Well the main thing to keep going, to be strong mentally is to be able to make sense of things . . . Don’t let things get out of hand where it’s chaos theory or whatever. (Amy)
Inverted synergy
All of the participants described at least short periods of time when their thoughts and emotions had become complicated and difficult to regulate. Episodes of this kind were most often experienced following a loss such as a relationship break-up, or a perceived failure, or the anticipation of failure at something perceived as important. The episodes involve iterative scanning of the existing frame of reference for a way of restoring equilibrium. From within such space, participants’ thoughts and feelings would typically escalate in intensity and become increasingly complicated until an idea for reestablishing cognitive-emotional terra firma was intuited, remembered, or offered by another person. Participants’ strategies for resolving these episodes of “inverted synergy” typically included reaching out to a trusted person: I couldn’t sleep because my thoughts were going a million miles an hour . . . It can be spooky . . . I try to make sense of my thoughts and the things I’m experiencing . . . I try to be imaginative to change my thoughts . . . I try to distract myself . . . I have to remember that I’ve been through this before. (Karene) Sometimes I get down in the dumps and feel like it will get the best of me . . . I don’t know what to think . . . I think there is nothing I could say to myself that would make things better . . . I felt that I couldn’t control what I was thinking . . . I talked to my mother and it helped . . . I ask myself how can a thing make me feel so upset and confused . . . Surrounding myself with good people helps. (Margaret)
Environmental influence
All of the study participants described their local cultural and physical environments as being influential with respect to their mental health. In some cases, the description suggested a good fit with the environment that facilitated mental health. In other cases, the description suggested a complicated relationship with the environment that necessitated contingencies for managing mental health:
When I’m in the city it’s just like the earth is completely scraped out, there’s like nothing to look at, there’s just cement and boxes everywhere . . . I’m happy here [northern Ontario], not here [Sudbury], at home . . . I can live the way we are supposed to. (Tom) With places around northern Ontario you might go to visit there’s always the sense of that it’s not so large to be beyond comprehension. A town like Toronto would be very difficult to make sense of . . . I think it has a bearing on how you perceive the world around you . . . It’s not that you’re more important but you’re there, you’re something that’s not invisible. (Robert)
Participants indicated that influences from afar tend to be filtered through local events, norms, and requirements:
I think we’re not separate from the rest of the world anymore . . . we’re all affected by what’s going on in the world . . . it’s what happens at home, especially between me and my husband that really determines how I feel. (Wendy) You’re going to be influenced the most by where you are, just to get along and get by . . . I read the textbooks I have to . . . what I think comes from what I have to do, day to day. (Alicia) All of the participants referred to “touchstones” of one kind or another (e.g., local or widely known aphorisms and symbolic structures, events and practices) as a type of knowledge they frequently draw upon to manage their mental health: I know I’ve made it home safely when I can see the big stack . . . I relax then, I’m not anxious anymore. (Wendy) My father always says “you have to know how to make your own fun.” (Jacques) I look forward to having dinner together at home . . . that was a special time in my family . . . It’s not always easy to manage, well sometimes it’s nice to do something different, but if we eat out or separately a lot it makes me feel that life is chaotic . . . Now it’s my husband, I always refer to him as my island and when things get kind of crazy I just go to my island. (Wendy)
Benefits of learning about mental health
All participants reported that their mental health benefited in some way from their involvement in the study:
I was never asked before whether I think about what I think. The question made me change how I think . . . I’m going to think differently about the way I feel and what I can do about it. (Dominique) It’s [participation in the study] definitely made me want to research it more [mental health] and look into improving it because not everything works well for everybody . . . I already have ideas about what I can do differently to make it easier for myself. (Jean-Marc) This has helped me be able to say that I am healthy; it reassured me. (Tom)
Open Coding
During the initial phase of coding, audio-recordings, data transcripts, and memos were examined for salient categories. The participants’ descriptions of what they think about and do to manage their mental health clustered into three basic categories—Knowledge Types (KT), Knowledge Sources (KS), and Autologous Knowledge-Translation (AKT).
Three subcategories of KT emerged from the data—personal knowledge, propositional knowledge, and procedural knowledge. Three types of personal knowledge were identified—personal beliefs, personal values, and objective personal knowledge. Participants’ beliefs included their opinions about themselves (self-esteem), their religious or spiritual beliefs, their beliefs about the nature of mental health, and how knowledge is acquired (ontological/epistemic), and personal touchstones, the latter comprising significant memories, idiosyncratic phrases, and personally symbolic features of the local landscape (chronotopes). Values commonly held by participants included personal health, success (achievement of personal goals), and being connected to and valued by family, friends, and their respective communities of practice. Participant’s objective personal knowledge refers to factual knowledge they have of themselves and of other persons.
Propositional knowledge refers to knowledge of facts. Objective personal knowledge can be understood as a type of propositional knowledge; however, in the aggregate this form of knowledge is distinguished by its uniqueness to the individual. Two types of propositional knowledge were identified—local knowledge and global knowledge. Local knowledge refers to knowledge of local services and amenities, knowledge of local cultural events, practices and norms, knowledge of natural and built local environments, and other situated knowledge. Global knowledge refers to knowledge that transcends place and social space and whose intended meaning is universal. Knowledge of English is an example of global knowledge held commonly among the participants.
Procedural knowledge refers to knowledge of the processes for acquiring, evaluating, organizing, and deploying personal and propositional knowledge. Procedural knowledge invariably involves some propositional knowledge; however, propositional knowledge does not necessarily involve procedural knowledge. For example, knowing that one thinks and that one can change one’s thinking is propositional knowledge, whereas, knowledge of how to change one’s thinking is procedural knowledge (Figure 1).

Knowledge Types (KT; Open Coding).
KS comprises two subcategories—informal sources of knowledge, and formal sources of knowledge. Informal sources include family members and others among the participants’ social orbit, informal media, and the individual himself or herself. Formal sources of knowledge include school, formal media, and health professionals. Informal media refers to unedited, informally edited, or commercially edited information accessed via electronic media (e.g., Internet-based social networks, compact music disks, television and radio advertising, and entertainment-oriented programming), or certain print media (e.g., editorialized magazine and newspaper articles and advertising). Formal media refers to peer reviewed or accredited educational material accessed via the Internet and “hard news” reported via electronic and print media (Figure 2).
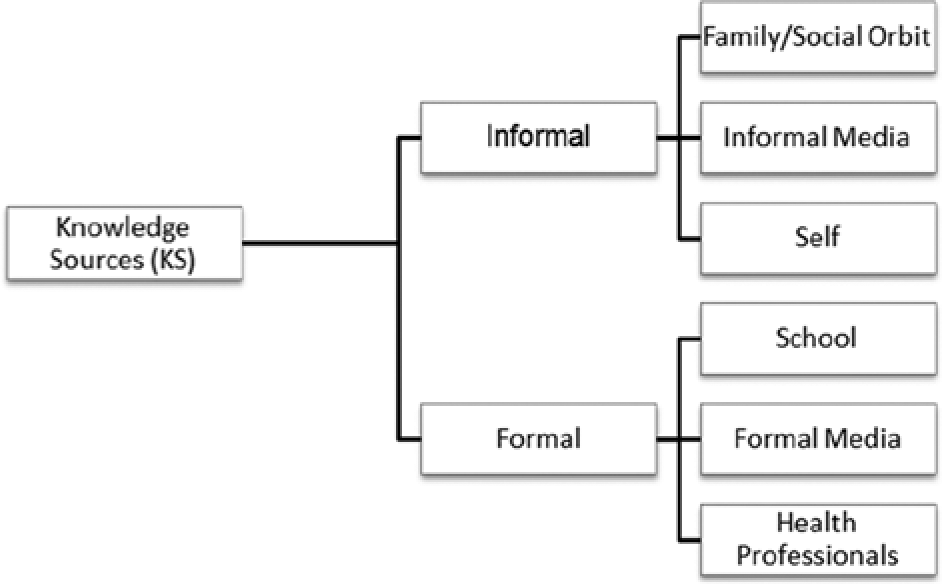
Knowledge Sources (KS; Open Coding).
Health researchers define knowledge translation as a dynamic and iterative process that includes the synthesis, dissemination, exchange, and application of knowledge to increase the effectiveness of the health care system and improve the health of individuals. This multilevel process is understood to take place within a complex system of interactions between researchers and knowledge users (Graham, 2010). In the present context, the term “Autologous Knowledge-Translation” (AKT) has been adopted to categorize how the study participants acquire, generate, and utilize knowledge to protect and promote their mental health. For the purposes of the study, the analysis of AKT focuses on its relation to MHL; however, it is suggested that the concept can be applied globally, that is, it is logical to surmise that the organismic level process depicted by this term is not exclusive to knowledge brought to bear in the management of mental health, nor is it limited to any particular knowledge concern. This formative process involves the iterative acquisition, production, and application of knowledge of all types for all manner of purpose, and is the first and primary level at which knowledge translation of any kind occurs. Researchers, as individuals, engage in AKT as a precursor to collaborative efforts at knowledge translation intended to advance science, and all individuals, as knowledge producers, engage in AKT for adaptation, relational, and actualization purposes (Figures 3 and 4).

Autologous Knowledge-Translation (Open Coding).

Substantive open codes.
Axial Coding
The second phase of coding involved reviewing the database to gain further insight into the categories generated through open coding and, if indicated, identify new categories. In particular, this phase of analysis involved going back and forth between the data set, memos, tentative diagrams of the substantive codes, and the literature to identify the contexts and intervening conditions that shape the development and deployment of MHL. This procedure inevitably directed the focus of analysis to AKT processes and their relation to KT and KS.
Each participant provided examples of utilizing information obtained from interpersonal communications, informal and formal media, and the classroom to regulate and improve their mental health. The participants commonly expressed having respect for knowledge obtained from formal sources; however, based to a large extent on its overlapping relational significance and related heightened psycho-emotional resonance, they perceived their mental health practices to be most influenced by knowledge obtained from trusted individuals within their immediate social orbit.
All of the participants’ described a cultured form of resonance as a precursor to their acquisition of knowledge, that is, they discriminately took information on board that was for them intelligible and in some way significant. The significance of the assimilated information is not always readily apparent; however, where some sensory information is ignored other sensory information excites a cognitive response based on its vague or specific familiarity and perceived potential for use. This type of resonance is distinct from sensory resonance in its requirement of resonating with the individual’s established global cognitive framework. Accordingly, “cultured resonance” represents a metacognitive process and outcome and initiates and mediates the meaning-making process.
The participants revealed themselves to be inveterate meaning-makers, continuously assigning meaning to endogenous, interpersonal, and other environmental events. Meaning-making involves drawing on one’s accumulated knowledge and understandings to interpret events as they arise. The participants indicated that the immediate intent of meaning-making is to preserve, enhance, or recover a sense of coherence. They unanimously expressed a need to make sense of events on a discrete basis and coherently integrate their interpretations into their global cognitive framework. This finding is consistent with Antonovsky’s (1985) salutogenic model which features “sense of coherence” as a necessary goal of mental health management and as a primary determinant of mental health outcomes.
The participants prioritized cognitive and emotional coherence to the extent that they would persist in their attempts to achieve it even when their efforts caused distress. Each participant described at least short periods of time when their thoughts and emotions became increasingly troubling and difficult to regulate as they attempted to make sense of a recent or unfolding event. During such periods, one anxiety inducing thought would lead to another and so on, increasing the intensity of the anxiety as the sequence progressed. These episodes of “inverted synergy” tended to occur in response to a dissonance invoking event, such as an unexpected relationship break-up or failing at something perceived as being important. Reversal of this inverted synergy would sometimes only begin when a threshold was reached at which the participant’s desire for coherence overmatched his or her preference for self-direction, resulting in reaching out to a trusted person. The motivation for confiding in another person invariably involved a desire for emotional support, but also had the strategic purpose of gaining an alternative perspective. All of the participants related experiences in which their unpleasant feelings were moderated by the words and gestures of others when their own attempts to effect similar improvement had been counterproductive.
The participants not only thought about their thinking in moments of distress but in various circumstances and emotional states. They routinely engaged in metacognitive activity (e.g., self-talk or introspection) that involved a dialectical exercise in which she or he would play “devil’s advocate” to their present thoughts and inclinations. Participants would entertain an idea (or thesis) and then propose to themselves counterideas (or countertheses) and counters to their counters with the aim of arriving at a position or synthesis with which they could proceed to practical experimentation with some measure of confidence. The participants’ success in deploying mental health strategies arrived at in this way would result in its incorporation into their mental health management heuristics.
The participants indicated that place and social space influences their day-to-day decision-making, activity, and mental health management. They filter information originating near and afar in accordance with local norms, requirements, and opportunities for success. In the present context, “success” refers to the attainment of personal goals or progress toward their attainment while preserving a sense of coherence. Local tolerances and preferences are among the factors participants described attending to in their efforts to maintain a sense of coherence.
All of the participants indicated that northern Ontario has influenced their worldview, self-identity, relationships, and mental health. A subtle common dialect is evident in the participants’ nearly unanimous and similarly intended references to “nature” as a defining feature of the region, as in “we have nature here,” and to northern Ontarians as “friendly” (i.e., open to spontaneous engagement by others, and more so than their “big city” counterparts) and “tough” (i.e., self-reliant and resilient as a consequence of relative isolation (geographical, economic, and social), minority political leverage, and longer, more severe winters, among other things). Most of the participants identified one or more structures within the built environment that they perceive to have iconic significance and as contributing to a shared sense of identity. For example, one participant commented that the “super stack” (the world’s tallest chimney) represented “home” to her, particularly when first seeing it after a period of being away. The participant elaborated on her use of the word “home” as a metaphorical reference to a defined and defining place and social space.
The study participants engaged in knowledge translation as a fundamental aspect of managing their mental health. This practice iteratively involved acquiring knowledge of various types from various sources and generating autologous knowledge through creativity and synthesis. The process is itself autologous given that the acquisition of knowledge is contingent on internal dynamics and formerly established content, that is, cultured resonance, meaning-making, and meanings previously made.
The participants did not rely exclusively on formal mental health knowledge (i.e., psychological knowledge or knowledge typically associated with mental health, per se) to manage their mental health, nor were they always consciously aware of the knowledge they used for such purposes. The data suggest that the participants were only occasionally deliberate in their application of knowledge for mental health purposes and were more typically either vaguely or negligibly aware of the diversity of knowledge they used to manage their mental health. Nonetheless, whether they did so consciously or unconsciously, all of the participants selectively drew from all of the knowledge at their disposal in their attempts to achieve preferred mental health outcomes with events as they arose. The participants’ strategies for regulating their emotions developed as they observed correlations between events and their emotions (which they continuously monitored). These observations resulted in the development of procedural knowledge and the adoption of mental health management heuristics (i.e., procedural habits based on consolidated trial and error experimentation; Figure 5).

Autologous Knowledge-Translation (Axial Coding).
Selective Coding
The final phase of analysis initially involved reviewing the entire data set, including earlier drafted memos, with a view to finding evidence to disconfirm the proposed MHL framework. This advanced stage reexamination of the data found no evidence to contradict previous interpretations. A flow diagram (Figure 6) was subsequently created to illustrate the core features of the framework and their interrelations as theorized, and to assist with constructing an integrated summary of the ontogeny and implications of MHL.

Ontogeny of the mental health narrative (selective coding).
Concisely, MHL can be understood to comprise all self-generated and acquired knowledge with which people negotiate their mental health. Participants described assigning meaning to and building literacies from experiences that impacted their mental health. The participants’ interpretations of events were influenced by and modified or confirmed their global cognitive framework (global meaning)—the aggregation of their knowledges and attendant literacies. The literacies possessed by the participants effectively circumscribed the possibilities for meaning-making in relation to events as they unfolded, and their level of MHL significantly impacted their decision-making with respect to their mental health management. A predictive quality emerges from this iterative cycle, in that it predisposes the individual to a trajectory of mental health management practices that conforms to their MHL. In effect, the study participants depicted global meaning specific to mental health as an a priori mental health narrative, and MHL and meaning-making as primary ontogenic coefficients in its ongoing construction.
Discussion
Research on language and mind (e.g., Frith, 2008; Muntigl, 2004) mindfulness (Kabat-Zin, 1982; Linehan, 1993), metacognition (e.g., Barahmand et al., 2008), place and social space (e.g., Gatrell et al., 2004), resilience (e.g., Fine, 1991; Hunter, 2001; Masten, 2001; Schoon, 2006; Wolff, 1995), the social construction of health (e.g., Dowbiggin, 2009), and various constructs associated with positive psychology (e.g., Peterson, 2006) has reconfigured the constellation of key mental health variables, situating meaning-making at its center. Interest in meaning has bourgeoned in recent years among scholars from various disciplinary orientations, including sociology (e.g., Lamont, 2000, 2001), cultural anthropology (e.g., Kurzman, 2008), and several branches of psychology, including clinical psychology (e.g., Hayes, Laurenceau, Feldman, Strauss, & Cardaciotto, 2007), cultural psychology (e.g., Mendoza-Denton & Hansen, 2007), and emotions (e.g., King, Hicks, Krull, & Del Gaiso, 2006; Wood & Conway, 2006).
Researchers have been particularly interested in the effects of meaning-making on adjustment to stressful life events. Multiple theories have been advanced from varying perspectives including those that emphasize cognitive processes and underlying structures (e.g., Bruner, 1990; Walker & Winter, 2007), the role of autobiographical memory, and allied concepts such as internal state language (e.g., Bluck & Habermas, 2001; Conway, 1990; Fivush & Baker-Ward, 2005; Nelson & Fivush, 2004), and the influence on and of personal narratives (e.g., Crossley, 2000; Gilbert, 2002; Muntigl, 2004; Nelson, 2003). The Park and Folkman (1997) developed an integrated model of meaning-making in the context of stressful life events that distinguishes meaning-making efforts from meanings made and situational meaning from global meaning. The Park and Folkman model, subsequently refined by Park (Park, 2010), is based on a set of tenets drawn from the major relevant theories. These tenets are summarized as follows: People develop cognitive frameworks (global meaning) with which to interpret their experiences; when confronted with a stressful event individuals assess the situation and assign meaning to it; distress arises in proportion to the degree of discrepancy between situational meaning and global meaning; the distress caused by discrepancy initiates a process of meaning-making intended to reduce the discrepancy and restore a sense of coherence and valued purpose; and when successful, this process facilitates adjustment to the stressful event (Park, 2010).
Park’s model is consistent with Antonovsky’s claim that it is not life’s stressors that cause distress, but whether such stressors violate one’s sense of coherence (Antonovsky, 1985, 1987). Antonovsky’s salutogenic theory infers that the basic objectives of meaning-making are to preserve or recover a sense of coherence and to develop and nurture a sense of purpose. This involves assigning meanings to events that confirm or modify, but ultimately cohere with one’s global meaning while permitting the construction of a narrative whose purpose is motivating and self-defined (Antonovsky, 1985, 1987, 1990; Langeland, Wahl, Kristoffersen, & Hanestad, 2007).
According to the Park–Folkman model, individuals continue their efforts at meaning-making when their initial attempts are unsuccessful (Park, 2010). Michael and Snyder suggest that individuals’ unsuccessful attempts at meaning-making are akin to rumination and distress (as cited in Park, 2010). This phenomenon is conceptualized in the present study as “inverted synergy” which emphasizes the process rather than content aspects of the rumination participants engaged in following a dissonance evoking event. All of the participants described experiencing at least one episode in which their thoughts became increasingly convoluted with a corresponding increase in the intensity of distress. The episodes described by the participants involved nonclinical obsession; however, it is not difficult to imagine the possibility of uncurbed inverted synergy eventually crossing a clinical threshold. Episodic inverted synergy does not imply organic impairment, nor is it an inevitable response to an unwelcome event. However, it may suggest naivety regarding present dynamics and/or the absence of cognitive strategies for their correction. In other words, inverted synergy may be at least partially explained by a lack of previous successful experience with situations similar to the present challenge and by the absence of the knowledge potentially obtained therein. Put yet another way, people think what they think knowing not of a better alternative (Kusan, 2010, 2011).
Beyond describing the dynamics of episodic escalation of counterproductive thoughts and dysregulated emotions, inverted synergy may also be a useful descriptor for the serial compounding of problematically assigned meanings over time. Each meaning made borrows from and confirms or revises one’s global meaning (the aggregation of all previously made meanings), consolidating or recalibrating the global cognitive-emotional frame from which new meanings are made. At any point in the evolution of one’s personal narrative the consolidated aggregation of meanings comprise a guidepost for decisions to be taken. For individuals drawing on impoverished or otherwise problematic literacies the likelihood of ineffectual and/or counterproductive mental health decision-making is undoubtedly increased, as is the likelihood of establishing a trajectory of mental health decision-making that is characterized by inverted synergy.
In rudimentary terms, meaning construction involves the attempt to cohere presently attending sensory information with established neurobiological praxis and cognitive-emotional schema. Meaning-making occurs, then, at the interface of intrasubject processes and the culturally coded object world (Bruner, 1990; Frith, 2008; Podolefsky & Finkelstein, 2008; Seligman & Kirmayer, 2008; Shore, 1991; Wexler, 2006). Data from the present study suggest that the locally coded object world has a profound impact on the individual’s construction of meanings. The study participants indicated that knowledge obtained in their immediate social orbit was likely to have greater resonance than knowledge obtained from afar. The data also suggest that global literacies permeate local culture through local filters, abetted by the individuals’ desire to be valued and accepted by family, peers, and the community (Kusan, 2011).
Russian philologist, Bakhtin (1981), used the term “chronotope” to depict the spatiotemporal matrix that governs linguistic acts, which are the construction blocks of personal and community narratives. Paraphrasing Bakhtin, Basso (1996) described chronotopes as “points in the geography of a community where time and space intersect and fuse . . . as monuments to the community itself, as symbols of it, as forces operating to shape its members’ images of themselves” (Basso, 1996, p. 62). The participants consistently described northern Ontario as a distinct geo-cultural entity whose essential character derives from the unique combination of prominent features of the natural, built, and social environments. Participants commonly referred to “touchstones” (typically symbolic features of the local physical environment) as a type of knowledge they repeatedly draw on to manage their mental health. These findings are consistent with previous research that identifies place and social space as among the key determinants of mental health (e.g., Gatrell et al., 2004; MacIntyre et al., 2002).
Regardless of the origin of information obtained by the study participants, the acquired information was vetted through behavioral experimentation, introspection, and metacognitive practices such as self-talk. Metacognition has been implicated as being integral to the processing of information at the interface where biological and cultural grammars are conjoined (Fernandez-Duque, Baird, & Posner, 2000; Flavell, 1979, 1987; Moses & Baird, 1999; Schwartz & Begley, 2003; Shimamura, 2000; Wexler, 2006). Metacognitive knowledge refers to beliefs and literacy about the workings and limits of cognitive enterprise (Moses & Baird, 1999). Knowledge of the factors that affect the course and outcome of cognitive enterprise undoubtedly qualifies as a fundamental example of MHL—one which has a profound influence on the acquisition and deployment of other mental health literacies individuals use. Individuals with even basic literacy regarding their own cognitive processes (whether formal or self-constructed) are able to use this knowledge for self-regulation and to exert control over the environment.
Research conducted over the past several decades has established health literacy as an important predictor of individual and population health (Canadian Council on Learning, 2007). It has also led to an expanded definition of health literacy that includes the social determinants of health and the knowledge and abilities that people use to negotiate their physical and mental health (Bourget & Chenier, 2007). Movement toward a comprehensive, pluralized concept of health literacy has been consistent with developments in the field of literacy studies which have broadened the concept of general literacy to include a range of skill sets from basic reading and writing to critical analysis (Bourget & Chenier, 2007; Kickbusch, 2001; Nutbeam, 2000; Rootman, 2002; Tones, 2002). Broadening the DSM-based definition of MHL similarly recognizes that individuals use knowledge of various types from various sources to manage their mental health. At a global level, expanding the definition of MHL acknowledges research on resilience, salutogenesis, and other topics under the broad rubric of positive psychology as important examples and wellsprings of MHL. At the organismic level, widening the lens through which individuals view MHL encourages building mental health management knowledge and skills, and expectedly would result in an increased personal capacity to act on such knowledge.
Further study of MHL, particularly from a transdisciplinary perspective, has potential to improve our understanding of such fundamental psychological and social concerns as gender relations, and the significance of gender regarding the individual’s identity formation and mental health management, race relations and race as factor in personal identity and mental health management, the mental health effects of place and social space, and the litany of factors, some yet to be identified, relating to how individuals protect, promote, and recover their mental health.
In the clinical context, juxtaposing the intent of traditional approaches to psychotherapy (namely, shrinking mental illness) with treatment approaches whose explicit intent is to grow mental health is instructive. All talk-therapy approaches must achieve resonance with the client to socialize him or her in the therapeutic model and to successfully convey the wisdom in its tenants. A prerequirement of any therapeutic engagement, then, is the present capability of the client to understand and make use of the therapist’s words. The strengths that engender this capability are the fulcrum on which any positive change is advanced. Indeed, it can be argued that shrinkage of mental disorder is in actuality a corollary of cognitive and psycho-emotional growth toward health. The literacies introduced to clients, whether predetermined and offered expertly as with the positivist/medical-model orientation or emerging through dialogue as with the constructionist approach, must resonate and promote the expansion of existing strengths to effect the desired change. Even the “unlearning” of maladaptive patterns of thinking and behaving is achieved by amending problematic literacies and their attendant understandings with those that are consistent with healthier patterns and outcomes. In the final analysis, learning how not to have symptoms, whether preventatively or as treatment, proves inevitably to be a matter of learning how to be healthy (Kusan, 2010).
In the classroom context, students rely on their current knowledge to interpret, integrate, and synthesize the information newly introduced by the instructor or classmates. In school as with all contexts of learning, new insights and more adaptive perspectives become possible when information is intelligible and has relevance within the individual’s current complex of understandings. Participants in the study indicated that such cultured resonance is a prerequisite and precursor to any targeted expansion, modification, or substitution of these understandings. They also indicated that enhanced knowledge of their own mental health processes helped expand their repertoire of mental health management strategies, and gave them an increased sense of control. Beyond the obvious implications for mental health management, these findings (which are fundamentally consistent with previous research on meaning-making and mental coherence; for example, Antonovsky, 1985; Park, 2010) have, by logical extension, profound implications for overall health management.
Literacies that better enable people to optimize their mental hygiene and mental functioning would certainly at least facilitate effective physical and mental health management at various levels and stages of its operationalization, including those pertaining to interpretation, motivation, decision-making, and behavioral and self-regulatory practices. In support of this claim is the substantial and compelling evidence accumulated over the past decades that the individual’s apprehension of and conscious actions pertaining to his or her heath, in all of its aspects, significantly derive from the knowledges and literacies he or she is able to bring to bear (e.g., Bateson, 1972; Carmody, 2009; Foucault, 1982; Park, 2010; Schwartz & Begley, 2003; Seligman & Kirmayer, 2008). Much of the same evidence relatedly stresses the influence of personal beliefs on health and the trajectory of the personal narrative generally (e.g., Bateson, 1972; Foucault, 1982; Park, 2010). It is widely accepted and often reflected in policy that the benefits of educating people regarding the ontogeny and consequences of their beliefs can potentially reduce acts of violence, whether motivated by temporarily dysregulated emotions or for grandiose reasons with intent to invoke widespread terror. With the inclusion of knowledge of the ontogeny and potential consequences of personal beliefs, among other knowledges, in the definition of MHL, it can be reasonably argued that enhancing MHL at organismic and population levels potentially represents our best hope and strategy for redressing many of the debilitating intrapersonal, interpersonal, and environmental problems with which we are confronted.
Limitations of the Study and Recommendations for Future Research
In any qualitative inquiry, the mind of the researcher is at once a research instrument and a variable as the researcher’s interpretation and codification of data is filtered through that variable instrument. Thus, the findings of the present study represent an interpretive synthesis of participants’ descriptions of what they think about and do to manage their mental health. Member-checking, triangulation with the literature and researcher reflexivity were undertaken to minimize interpretive error and bias. Nonetheless, there remains here, as with all qualitative investigation, a degree of subjectivity in the findings.
Where quantitative methods seek to confirm hypotheses about phenomena, predict variation, and causal relationships, and are subject to statistical assumptions and conditions, qualitative methods seek to explore and describe variation, extract and ascribe meaning, and rely on an iterative process of gathering data, whereby, questions are adjusted according to what is learned (Creswell, 1994, 2007; Dorsten & Hotchkiss, 2005; Patton, 2002; Stebbins, 2001). Rendering probabilistic generalizations is not the purpose of exploratory qualitative research (Creswell, 2007; Popay, Rogers, & Williams, 1998); however, based on the participants’ provision of relevant and sufficiently rich data with which to build theory, the conceptual framework advanced by this study can serve as groundwork for future research whose intentions may include statistical assessment of the validity of the advanced concepts and their generalizability.
Undoubtedly, the use of a topic guide had a delimiting effect on the cognitive orientation of the respondents and the content of their answers. However, in contrast to a priori coding whereby analysis is limited by predetermined codes (Creswell, 2007; Marshall & Rossman, 2006), the substantive codes identified in the present study were determined through an open analytic process and emerged entirely from the data.
The relatively small sample was composed of students whose availability was restricted due to academic commitments during the academic season and employment commitments or other plans during the summer break. Although the participants were generous with their time in making themselves available for two lengthy interviews, their limited availability also limited the opportunities to gather data. Furthermore, the eligibility criteria for the sample did not include or exclude persons with a psychiatric history and no such history was taken during or subsequent to eligibility screening. Given the relatively high level of mental health consistently reported by the study participants, the findings may not adequately account for the ontological processes, content, and deployment of MHL operating within clinical populations. Further research on the findings of this study and on MHL generally is critically needed. In addition to quantitative designs for confirming or disconfirming concepts emerging from the study (such as “cultured resonance,” “inverted synergy,” and AKT), comparative studies, whether of quantitative, qualitative or mixed-methods designs, are needed to investigate possible differences in MHL development and utilization between healthy individuals and persons with identified psychiatric problems. Additional qualitative studies that are sufficiently resourced to achieve complete data saturation are also needed to expand on the present findings and otherwise address their limitations.
It would be appropriate and useful going forward to recognize the various literatures produced by research on mental health, its ontogeny and methods for its protection, promotion, and recovery, as essential content of MHL. Some of the many possible specific areas of interest for future research on MHL include: mental performance optimization strategies (including mindfulness/metacognition); the language, rules, and dynamics of effective parenting; formal languages, dialects, and oral traditions as mediators of mental health; and the uses and effects of art as symbolic MHL. It would also be useful in terms of availing individuals and communities of the potential benefits of MHL to incorporate MHL enhancement programming (broadly defined) into formal systems of public education.
Conclusion
MHL has hitherto been defined as “knowledge and beliefs about mental disorders that aid their recognition, management or prevention” (Jorm et al., 1997). This definition effectively translates to knowledge of the contents of the DSM and reflects the dominant biomedical orientation of the mental health field. Results from this study indicate that the current definition of MHL is overly narrow and that individuals use knowledge of various types from various sources to manage their mental health. The findings also suggest that individuals acquire and self-construct mental health literacies which they modify, as necessary, via metacognitive practices and behavioral experimentation. The findings further suggest that the individual’s level of MHL, particularly in relation to mental health processes, is among the key determinants of his or her mental health status and may predict the trajectory of his or her mental health narrative.
MHL is redefined as “the self-generated and acquired knowledge with which people negotiate their mental health.” The expanse of this definition reflects the innumerable literacies potentially available to individuals for the management of their mental health. Literatures on resilience, salutogenesis, and mindfulness among other topics associated with positive psychology have not previously been identified as MHL, per se, despite their intent to promote literacies that can be drawn on to enhance mental health. Further research that integrates these literatures and continues to uncover taxonomies of MHL as well as the connections between and transactional nuances within them is required, particularly from an emic perspective. Broadening the definition of MHL has the potential to enhance the capacity of individuals to manage their mental health effectively and, correspondingly, has positive implications for treatment and prevention of mental disorders.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.