
Abstract
Parent-adolescent communication about sexual and reproductive health (SRH) issues is associated with healthy sexual outcomes in adolescents. The increasing evasion of this discourse at the home front in sub-Saharan Africa is receiving greater academic and public health attention. In many Nigerian households, adolescents lack access to informative and undiluted communication with their parents, a situation that is worse for adolescents dwelling in slums. This study documented SRH issues and patterns of parent-adolescent communication in selected slums of Ibadan, Southwestern, Nigeria. A mixed sequential explanatory research was carried out in 10 selected slums in Ibadan, Oyo State, Nigeria. A structured questionnaire scripted on open data kits (ODK) and vignette for Focus Group Discussion (FGD) were used to obtain data from parents and adolescents. A sample of 796 parent-adolescent dyads was interviewed for the quantitative strand, and 8 FGDs were conducted for the qualitative component. Analytical techniques utilized for quantitative data included descriptive (frequency counts and percentages) and inferential (chi-square) statistics, while descriptive and interpretative analyses were adopted for qualitative data. Communication regarding SRH issues occurs in many households, but indirectly. A higher proportion of mothers discuss all SRH issues with their adolescents and better than fathers. While female adolescents engage their parents only on limited topics, the consequences of sexual behaviors are the least discussed. The chi-square values for each topic were not significant for parents and adolescents, however, only the discussion of preventive sexual practice was significant for parents (0.042) at a significant level of 0.05 and adolescents (0.000) at a significant level of 0.01. The findings of this study suggest that sexual education training intervention is germane to enhancing parent-adolescent communication on SRH issues for parents and adolescents.
Introduction
The literature has consistently established that adolescents engage in sexual risk behavior such as early sexual activities, multiple sexual partnerships, unprotected sexual intercourse, and irregular contraceptive use, which predispose many of them to reproductive health challenges like unintended pregnancies, early childbearing, STIs/STDs, HIV/AIDS, and unsafe induced abortions (Izugbara, 2008; Morris & Rushwan, 2015). The World Health Organization reported that adolescence is a transitional phase of life that presents multiple sexual and reproductive health (SRH) challenges to adolescents (WHO, 1999), yet many of them lack access to appropriate information, knowledge, and services to meet their peculiar needs during this phase. As they transition from childhood to adulthood, parents play a significant role in socializing their adolescents, especially on SRH issues. An important aspect of this socialization is communication about issues of SRH because it promotes good SRH choices and behaviors (Grossman et al., 2018; Wamoyi et al., 2010). SRH issues were identified in this study as topics discussed by parents and their adolescents (e.g., puberty, menstruation, relationships with opposite sex/dating, sexual behaviors, preventative strategies, and repercussions). Evidence has shown that adolescents who engage in SRH communication with their parents are more likely than others to delay engagement in sexual activities (Steinberg, 2007). Such communication provides an avenue for parents to ingrain in their children, the SRH values and ensure that adolescents are accustomed to responsible sexual behaviors (Izugbara, 2008; Zamboni & Silver, 2016).
In sub-Saharan Africa (SSA), communication about SRH issues is highly controversial due to cultural and personal challenges (Bastien et al., 2011). Many parents find it problematic to broach SRH issues with their children (Dessie et al., 2015; Manu et al., 2015; Yadeta et al., 2014). This is implied in the culture of silence surrounding sexuality, which often makes an open conversation about SRH issues an illusion (Izugbara, 2008; Mutema, 2013). Again, the conservative norms and taboos around sexuality typically in Africa, as well as ill-preparation, also limit parental involvement and engagement in SRH conversation with their children (Dessie et al., 2015; Nundwe, 2012;). While some parents are conscious of the need to dialog with their adolescents, many parents and adolescents seem confused or anxious about what and how to discuss SRH issues. Sometimes, when open or responsive discussions occur, such conversations are largely opportunistic, arising only when the situation presents itself (Berg et al., 2012). Many times, parents gloss over critical SRH issues while others engage in verbal threats/warning with their adolescents rather than engaging in discussions on such matters.
In Nigeria, there is a paucity of research on the role of parents in delivering timely, adequate, and relevant SRH information to adolescents. The few studies available on SRH discourse between parents and adolescents are limited in scope, differ in their focus on parent-child communication about SRH issues, and their submissions. For instance, a study by Ojebuyi et al. (2019) focused on prevalence and how demographic variables influence parent-child communication about HIV/AIDS, and SRH issues in Nigeria using data from the 2012 National HIV/AIDS and Reproductive Health Survey (NARHS) Plus II. A similar study had earlier used 2007 NARHS data but examined constructs that are associated with parent-adolescent communication about AIDS/STIs and sexual relationships ( Berg et al., 2012). Also, Iliyasu et al. (2012) and Obono (2012) investigated the patterns of reproductive health communication between mothers and daughters (same-sex discussion and hardly father-daughter or father-son) in Northern and Southern Nigeria, respectively. Again, Ojo et al. (2011) explored parental perception, attitude and the influence of socio-economic and demographic factors on willingness to engage adolescents in SRH communication while Titiloye and Ajuwon (2017) documented parents’ knowledge and quality of communication relating to adolescent reproductive health between parents and their adolescents in Southwest, Nigeria.
These available studies have either focused on the prevalence or determinants of parent-child communication or sought information from parents and adolescents separately without matching parents with their adolescents. Also, these studies assumed parents and adolescents to be homogeneous groups, respectively, especially in urban areas, without due consideration for parents and adolescents who dwell in slums. Besides, none of the studies in Nigeria targeted specific topics of concern to both parents and adolescents on SRH issues. Hence, very little is known about SRH issues and patterns of parent-adolescent sexuality communication in urban slums where adolescents are vulnerable to poor SRH outcomes due to inadequate knowledge of SRH and low life skills. Studies have shown that adolescent slum dwellers were more likely to initiate sexual intercourse at an early age and subsequently graduate to risky sexual behaviors compared to non-slum dwellers (Dodoo et al., 2007; Kabiru et al., 2010; Marston et al., 2013). Consequently, adequate parental exchange and swift response to SRH communication needs have the capacity to promote good SRH choices and responsible SRH behaviors. The purpose of this study was to investigate specific SRH topics discussed and the patterns (direct or indirect or none) in which such topics were discussed between parents and adolescents’ slum dwellers. Understanding parent-adolescent discussion about SRH and its patterns in urban slums is critical to evidence-based programing aimed at improving adolescents’ SRH. To achieve this objective, the following research questions were examined:
Do parents and adolescents in the urban slums of Ibadan discuss SRH issues?
What are the specific SRH issues being discussed by parents and adolescents in the urban slums of Ibadan?
What communication patterns exist between parents and adolescents when discussing SRH issues in the urban slums of Ibadan?
Theoretical Underpinning: Social constructivism
The key research questions underpinning this study emanate from the underlying assumption of Berger and Luckmann’s (1991) Social constructivism theory. Social constructivism is a theory of knowledge in sociology and communication with an emphasis on shared meanings, understanding, and significance among interacting individuals within human society. This theory has its roots in Alfred Schutz’s social phenomenology and Lev Vygotsky’s sociocultural theory of human learning. The core tenet of Berger and Luckmann’s (1991) theory is that language-based communication is an essential system for how people construct their reality. The main objective is to understand people’s lived experiences within their social contexts.
In line with this assumption, parents and adolescents should share the same understanding around SRH issues if communication is to occur. It is equally expected that they must have mutual trust and confidence in each other for such communication to be effective. The lack of such a belief or distrust coupled with other socio-environmental factors may severely hinder conversation on SRH issues. Meaningful learning occurs when parents and adolescents have similar interests about the need to engage in transparent and responsive communication around SRH issues. In part, this dialog is contingent on the fears and readiness of parents to swiftly respond to adolescents’ SRH needs. Failure to respond to these needs appropriately can endanger adolescents’ SRH behaviors. For instance, parents may be interested in abstinence and the danger of unprotected sexual intercourse while adolescents’ interests may revolve around issues of contraceptive and how to handle multiple sexual partners. The information needed at this point may vary as parents may be supplying wrong information of complete abstinence when the child is sexually active. Adolescents may erroneously think of this communication as inappropriate and perceive their parents as being excessively protective and disrespecting their privacy. According to some studies, most parents find it challenging to accept that their adolescents are sexually active (Kunnuji, 2012; Ojo et al., 2011; Olasode, 2007). Therefore, the attitude of parents and adolescents toward sexuality communication must be positive for effective communication to occur.
Methods
Study Settings and Period
Ibadan, the capital of Oyo State in southwest Nigeria and a metropolis with an estimated population of 3,383,000 as of 2018 (Population Stat, 2018), was the setting of this study. Like every other State in Nigeria, Oyo State is subdivided into Local Government Areas (LGAs) for administrative convenience. Ibadan has five LGAs out of which 2 LGAs (Ibadan South-East and North-East) with the highest concentration of slums (Adedimeji et al., 2007; Fourchard, 2003; Makinde, 2012) were selected. In the two LGAs, a total of 10 slums were selected: Beere, Oja-Oba, Agbongbon, Oranyan, and Elekuro from Ibadan South-East; and Aremo, Irefin, Agugu, Okea-Adu, and Ayekale from Ibadan North-East. Generally, slum dwellers suffer material deprivation, which could compromise adolescents’ SRH outcomes (Kamndaya et al., 2015; Maina et al., 2020) and may present multiple problems that could motivate parents to talk to their adolescents about SRH. The selected slums attract many people from different tribes with poor incomes because of their low living costs. This study was conducted from April to June 2018.
Research Design
The study adopted a sequential mixed-method design involving both quantitative and qualitative approaches to explain specific SRH topics and patterns of conversation between parents and adolescents in the selected slums. The aim of using mixed methods is to benefit from the diversity that both procedures bring to the study and the opportunities to unravel the complexity of discussing SRH issues between parents and their adolescents. This design comprised two distinct but complimentary phases of data collection. The first phase entailed the use of a structured questionnaire in generating the quantitative data, while a structured vignette story for the focus group discussion (FGD) was employed in the qualitative phase. The selection of vignettes and the identification of themes that were critically explored in the FGD sessions were based on the preliminary findings of quantitative data. The quantitative participants were different from the qualitative participants, although they were drawn from the same communities. Because the study was largely quantitative, the quantitative approach was given precedence, with qualitative being used as a follow-up to better comprehend the quantitative results.
Population and Sample Size
The target population included adolescents aged 10 to 19 years and their parents (biological or guardians) of both sexes having at least one adolescent, and residence in the selected slums. It is crucial to capture parent-adolescent dyad perspectives to have a balanced and comprehensive assessment of SRH conversation. In contrast, the study excluded participants who were not residents of the selected slums. Also, parents and adolescents who were unwilling to participate, married adolescents and pregnant adolescent girls were ineligible, visitors during the data collection period were unsuitable for this study.
The computation of the sample size was based on a single proportion formula;
For the qualitative strand, a total of eight FGD sessions were held. Each FGD session included a minimum of eight and a maximum of 14 participants. Only 76 participants participated in the FGDs because some participants left in the middle of the conversation. The participants were recruited with the help of a community leader and a gatekeeper, with the criteria being parents and adolescents that are known to be living together for 2 years and above.
Sampling Procedure
A multi-stage sampling technique guided the recruitment of survey participants. Stage one involved a purposive selection of two LGAs with a high-density of slums (Ibadan Northeast and Ibadan Southeast). In stage two, a random selection of five slums from a list of slum localities in each LGA was done which translated to 10 slums in the two LGAs. Stage three entailed a random sample of four Enumeration Areas (EAs) in each community, which added up to 40 EAs in the two LGAs after which a household listing was done in each EA. EA is the division of the entire country into smaller, manageable regions with well-defined and identifiable boundaries, demarcated by the National Population Commission (NPC) for the 2006 Population and Housing Census in Nigeria. The fourth stage employed a systematic random sampling using a random number generator (RNG) software to select between 18 and 21 eligible households from the list of households that met the selection criteria in each selected EA. This was determined by the number of households in an EA. At this point, parent-adolescent dyads were chosen within the selected households until the desired sample size was reached for each LGA. For qualitative data, a purposive sampling approach was deployed to obtain discussants for the FGD sessions. A total of eight FGD sessions, four from each LGA comprising parents FGD (one male and one female groups) and adolescents FGD (one male and one female groups) were conducted in the two LGAs.
Data Collection Procedure
Quantitative data were obtained electronically using a structured questionnaire encrypted on the Open Data Kits (ODK) and retrieved with an Android-enabled smartphone. The instrument was prepared in the English language and translated into the local language (Yoruba language). A pre-test of the instrument was done in Ile-Ife, Osun State among selected parent-child pairs for modification and finalization before the actual survey. Trained research assistants (RAs) went from one eligible house to another to administer the structured questionnaire to the participants after obtaining their consent and assents. A separate private session was held for parents and adolescents with the assistance of supervisors. After a preliminary analysis of quantitative data, the vignette for FGD was developed from the quantitative findings for further exploration. Some of the issues earlier captured by the questionnaire were re-examined using vignette stories. This was done to gain in-depth understanding of earlier issues. The vignette was employed to discuss SRH issues from non-personal perspectives and allowed the participants to express their views by considering issues in the lives of others. The FGDs were held based on gender. The discussion was facilitated and moderated by two experienced male and female postgraduate students for male and female groups, respectively,at central locations close to the participants. All the FGD sessions were conducted in the local language and tape-recorded. The FGDs lasted for an average of 1 hr: 45 min.
Instruments
The study linked the parents’ questionnaire to the adolescents’ questionnaire which contains similar questions. The questionnaire covered questions on socio-demographic characteristics, household variables, parent-child communication on SRH issues, and patterns of parent-adolescent communication on SRH issues. Many questions were adapted from earlier studies on parent-child communication about sexuality (Dessie et al., 2015; DiIorio et al., 1999; Guilamo-Ramos et al., 2012; Manu et al., 2015; Nundwe, 2012), while other questions were introduced by the researchers, although guided by the theory (Social constructivism). Once complete, the questionnaires were sent to two experts to check for face validity.
Additional insights into SRH issues and patterns of conversation between parents and adolescents were explored using a structured vignette for FGDs. Based on Adio and Abeni’s stories, questions were generated for discussions, and probe were used to enrich the understanding of the quantitative results. The vignettes were carefully translated from English to Yoruba for parents and adolescents. The same vignettes were used for parent and adolescent groups. A sample of the vignette used is as follows: “A 14year old Adio (a boy) lives with his father, mother, and other siblings in a single room. Adio has an intimate relationship with Abeni (a girl) who lives in the same community. One day, Abeni was found with condoms and the parents were uncomfortable with this. When questioned, she informed her parents about her intimate relationship with Adio.”
Measures
SRH communication between parents and their adolescents was measured using sexual and reproductive health topics discussed by parents and adolescents. The assumption was that parents and adolescents only discuss issues they are anxious about. This was assessed using multiple choice on five topical issues ranging from puberty to the consequences of sexual behavior, which stemmed from available studies. A sample question includes, “Which of the following have you discussed with your adolescents in the last 12 months?.”
Patterns of parent-child communication: this was restricted to parents and adolescents who responded “yes” to the question “have you had SRH communication with your adolescent?.” The scale used for communication patterns was adapted from the literature (Lehr et al., 2000; Raffaelli & Green, 2003) and modified to measure direct and indirect communication patterns. Parents and adolescents indicated their agreement or disagreement to 17 different statements on SRH communication with responses ranging from strongly agree (5) to strongly disagree (1) as shown in the literature (Raffaelli & Green, 2003). A sample question is “My child should learn about SRH to be able to take informed decisions.” This sample question shows child readiness to learn and parents’ sensitivity to it. Composite score was derived and the total possible scores ranged from 1 to 85 points with the benchmark score being 43points. Any parent who scores 43 and above was assumed to use a direct communication while a lower score below 43 indicated an indirect communication pattern. The measurement of direct, indirect, and no communication has been reported earlier in a previous study (Aliyu & Aransiola, 2021). Thus, the following explanation was derived from the authors’ study.
Direct Communication Pattern: the direct communication was conceived as the ability of parents and adolescents to freely or openly discuss and address SRH issues without prejudice or judgment from the parents. The discussion could be initiated by either parents or adolescents in the form of questions, explanations, or counsel, as long as it is mutually engaging (Aliyu & Aransiola, 2021).
Indirect Communication Pattern: this was described as when adolescents’ participation in discussions about SRH issues is limited or restricted, or when parents solely provide instructions, warnings, threats, or punishment based on their own worldview without recourse to adolescents’ worldview. This dialog might be one-way, with parents talking to their children without engaging them, or parents taking a chance on providing SRH information to their children based on current events or situations. This communication may be less open or vague at times, or it may use fictitious names for SRH issues. On the other hand, indirect communication occurs when adolescents make allusions to what they have heard, read, seen, gossiped, or inquired about individuals or events in their environment (Aliyu & Aransiola, 2021).
No communication: this was seen as the lack of or non-existence of communication about SRH issues between parents and adolescents, either directly or indirectly, especially when the parent-adolescent dyad both replied “No” to SRH communication (Aliyu & Aransiola, 2021).
Analysis
Quantitative data collected was downloaded from the ODK server on a laptop and coded on an excel sheet. The data was imported into STATA package version 14 for cleaning and analysis. A data analysis plan (DAP) was developed to guide data analysis. Descriptive and inferential analytic techniques were employed to analyze data at univariate and bivariate levels. Thus, frequency counts and simple percentages were utilized at the univariate level while Chi-square was used at the bivariate level. A chi-square test is a statistical test for categorical data and a measure of association between variables. Since the outcome variable, which is parent-adolescent communication, is categorical, a chi-square was used to examine the association between parent-adolescent SRH communication and the explanatory variables. Kappa statistic was also used to estimate the level of agreement between parents and adolescents’ responses about SRH communication. Thus, this data does not follow any specific distribution.
Data from the FGD was transcribed verbatim, and the transcripts were word processed and edited using Microsoft Word. The transcripts were translated back end by language experts from Yoruba to English language. Thereafter, the translated transcripts were carefully read and edited by the researcher to ensure original meanings were not lost to translation. Transcripts were read and reread carefully to gain a general familiarity of what the participants were saying and how participants depict their realities. Next, nodes/codes were generated using a deductive approach to coding. The analysis was facilitated using NVIVO 11 pro software where descriptive and interpretative analyses were applied. To ensure inter-coder reliability, the researcher and a qualitative expert coded separately. Code books were compared for similar nodes/codes and discrepancies in coding. Code names and meanings were discussed, consensus was reached, and discrepancies were resolved. Thus, the qualitative findings were presented along with quantitative findings and verbatim quotations to express the world-view of the study participants regarding parent-adolescent SRH conversation.
Ethical Consideration
This study obtained ethical clearance from the Institutional Review Board of the Obafemi Awolowo University, Ile-Ife (HREC NO: IPH/OAU/12/983). Participants’ identities were protected during this study, and it was ensured that the study did not leave any harmful impacts on them. This was done by briefing at the beginning and debriefing at the end of the study, the aim of the study to make the participants feel at ease. Voluntary informed consent was obtained from parents and adolescents (aged 18 to 19 years) while assent was obtained from adolescents less than 18 years after explaining the study objective, design, and potential cost and benefits. Participants were assured their freedom of participation and the choice of opting out of the study at any point without giving further explanation. Confidentiality of participants’ responses and privacy of participants were emphasized and were maintained during data collection. All other ethical considerations were given due considerations and followed strictly including disclosure of researchers’ identity.
Results
Background Characteristics of Participants
Socio-Demographic Characteristics of Respondents (Parents and Adolescents)
The socio-demographic characteristics of the study participants have been described in the Aliyu & Aransiola (2021) study. The study engaged a total sample of 796 parent-adolescent dyads (Table 1). The parents’ ages ranged from 25 to 75, with the majority in the age group 30 to 49. The participants’ mean age was 42 years, with a standard deviation of 10 (SD = ±10). Only 13.3% of parents had no formal education, while the vast majority (86.7%) had some form of education. The majority (98.6%) of the respondents were of Yoruba ethnic extraction. More than half of the parents (57.9%) practised Islam, compared to a little under half (40.5%) who practised Christianity. The occupation showed that more parents worked in the informal sector than in the formal sector (those who earn a living through self-employment or work for those who are self-employed). Only 14.1% of the parents were unemployed, compared to 52.0% who were business or trade owners. This suggests that people who live in slums experience socioeconomic disadvantages, such as a lack of education, which may have compelled them to work in menial jobs, trades, or low-paying jobs.
Socio-Demographic Characteristics of Parents and Adolescents.

Source. Aliyu & Aransiola, 2021.
Also, Table 1 summarizes adolescent socio-demographic characteristics. Adolescents’ ages vary between 10 and 19 years. More than half of them (54%) are between the ages of 15 and 19, with a mean age of 15 and a SD of 3 years (SD = ±3). This implies that the majority of adolescents were aged 12 to 18 years. The gender distribution revealed that female adolescents constitute 51.8% of the population, while male adolescents make up 48.2%. The majority were unmarried (84.5%), with 63.6% having completed primary school and 3.0% having no formal education. The adolescents’ religious and ethnic affiliations were comparable to those of their parents. The Islamic and Christian religions were mostly practiced by 57.9% and 40.5% of adolescents, respectively. The majority of the adolescents (98.6%) were Yoruba.
Socio-Demographic Profiles of Focus Group Discussants
Table 2 offers a summary of the background characteristics of the FGD participants. Thirty-three parents (fathers and mothers) participated in homogenous vignette-based FGDs. Seventeen of the parents were from the Ibadan Northeast LG, while 16 came from the Ibadan Southeast LG. The age group showed that 23 out of 33 discussants were around 40 to 49 years old. Their marital status showed that 22 of them were married, compared to a very small number who were either divorced or widowed. All the parents (33) had some form of education ranging from basic to secondary levels. The majority them (20) had between four and six children. Fourteen of the parents are Christians, and 19 of them are Muslims. Their main means of livelihood were business or trading, as 22 participants fell into this category.
Socio-Demographic Profile of FGD Participants (Parents and Adolescents).
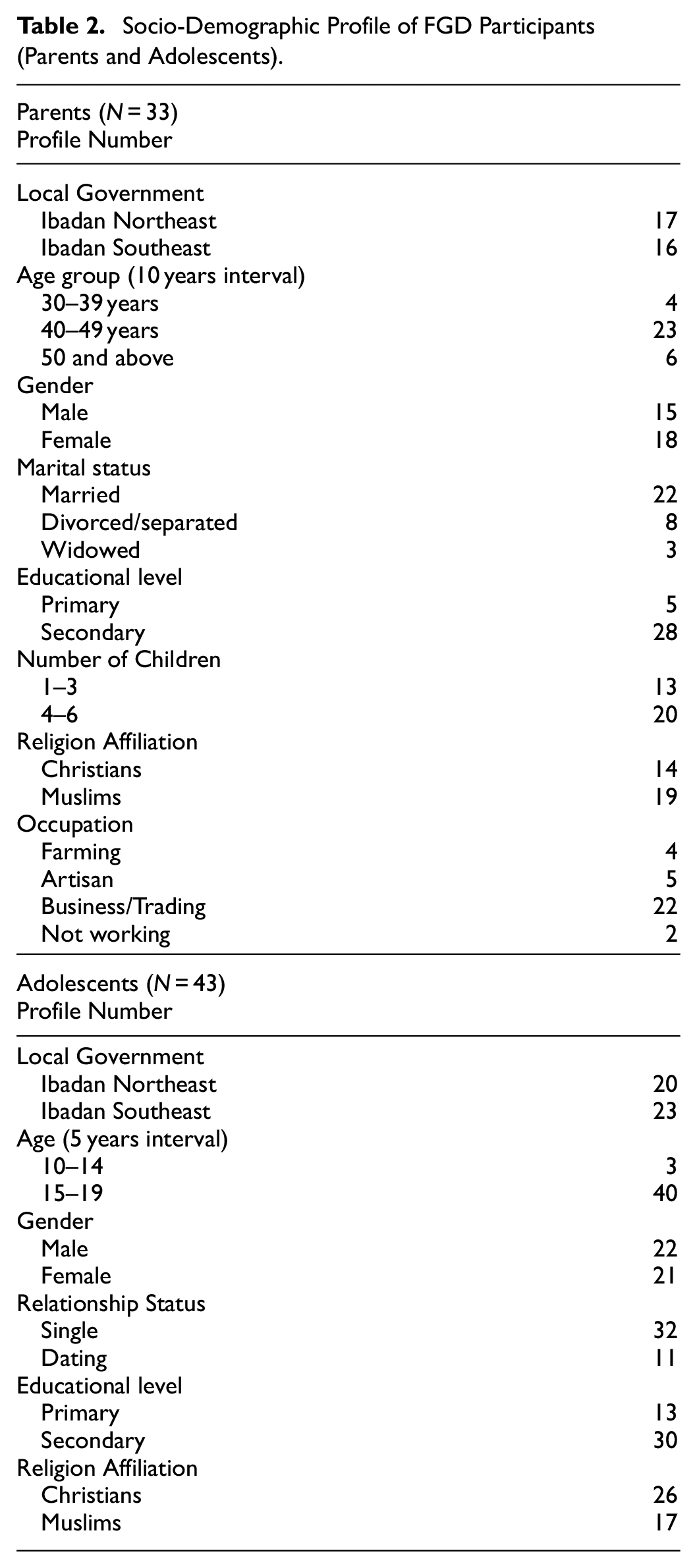
Table 2 also provides a summary of the characteristics of the adolescent participants in the FGD. A total of 43 adolescents participated, with 20 from Ibadan Northeast and 23 from Ibadan Southeast. The majority (40) were in their late adolescence (15–19 years). They had a fair representation of genders, with 22 boys and 21 girls. Most of them (32) were single, and 11 of them admitted to dating. Thirty (30) of them were enrolled in high school, while 13 had barely completed elementary school. According to their declared religions, 26 of them are Christians, while the other 17 follow Islam.
Discussion of Sexual and Reproductive Health Issues by Parents and Adolescents
Respondents were asked if they have ever discussed SRH issues in the last 12 months with a “yes” or “no” response for parents and adolescents. As demonstrated in Table 3, out of the 796 parent-adolescent dyads, three out of every five parents (61.9%) and above half (56.9%) of the adolescents have had discussions on SRH issues. This implies that parent-adolescent conversations about SRH issues were common. In contrast, a substantial percentage of parents and adolescents reported not talking about SRH-related issues, which translates to about two out of every five parents and adolescents. This is of concern, although not different from what has been reported in the literature due to contextual barriers to parent-child communication around sexuality. The table further explained the agreement of SRH discussion between parents and their adolescents using Kappa coefficient. The analysis merged parents who said (yes) with adolescents who equally said (yes) to discussion of SRH issues. Parents and adolescents’ reports showed a substantial level of agreement (0.80). This suggests that communication on SRH issues exists between parents and their adolescents, however the degree of communication may vary by specific issues or topics discussed.
Percentage Distribution of Parents and Adolescents by Discussion of SRH Issues and Their Level of Agreement.

Specific SRH Issues Discussed by Parents and Adolescents and Their Level of Agreement
Depicted in Table 4 are the specific SRH topics discussed by parents and adolescents—indicating their interest in each topic. Discussions on specific topics by parents with their adolescents range from 29.5% to 81.3%. From the six items investigated, puberty was the most frequently (81.3%) discussed topic. Relationships with the opposite sex appeared as the second most discussed (75.6%) topic. The reports on menstruation and preventive practices showed that around half (50.2%) and somewhat more than half (58.3%) of parents had such conversations with their adolescents. The least discussed topic was sexual issues (29.5%). Contrastingly, adolescents’ reports of communication on specific topics range from 28.1% to 76.0%. Over three-quarters of the adolescents had communication with their parents about puberty (76.0%) and relationships with the opposite sex (74.0%). Also, slightly above half (52.5%) have discussed menstruation. The least discussed topic among adolescents was the consequences of sexual behaviors (28.1%).
Distribution of Specific SRH Issues as Discussed by Parents and Adolescents.

n was based on parents and adolescents’ agreement (yes-yes) of SRH discussions.
Kappa compares agreement between parents and adolescents report of communication.
Based on the parents’ and adolescents’ reports, three dimensions of communication can be discerned. One, parents discussed four of the six topics more with their adolescents, while adolescents only discussed three. Second, both parents and adolescents have fair agreement on discussions of puberty, menstruation, and relationships with the opposite sex compared to other sensitive issues such as sexual issues, preventive practices, and consequences of sexual behaviors. Third, parents reported that sexual issues were the least communicated, while adolescents reported that the consequences of sexual behavior were the least discussed. Furthermore, Table 4 reveals the level of agreement between parents’ and adolescents’ reports of dialog on SRH issues. The kappa coefficients for parents and adolescents’ communication on SRH issues range from 0.39 to 0.64, depicting fair agreement to substantial agreement. Parents and adolescents had substantial agreement on menstruation (0.64) and puberty (0.62), whereas moderate agreements were recorded for the relationship with the opposite sex (0.58) and preventive practices (0.56), while sexual issues fell into the fair agreement benchmark (0.39).
The results in Table 4 show that parents and adolescents addressed nearly similar SRH issues. However, there was a little difference in the number of specific SRH issues they discussed. This provided a basis to explore further the SRH issues as expressed by the study’s participants using a qualitative approach. Thus, the FGD participants stated that they had discussed SRH issues like menstruation, puberty, sexual activities, pregnancy, abortion, and STIs/STDs. HIV/AIDS, and preventive practices such as condom use and abstinence. An overwhelming majority of the parents expressed that they have discussed one or more SRH issues.
In reaction to the vignette characters, FGD participants acknowledged that many adolescents engage in risky sexual practices that could put their future on hold, rejuvenate the cycle of poverty, and result in undesirable outcomes for them. In general, parents opined that as early as age 12 to 13 years, adolescents were exposed to sexual activities without protection. The consequences of these early sexual activities, as explained by the parents, are unplanned pregnancy, HIV/AIDs, STIs/STDs, and abortion. Parents put into words that “a closed mouth do not get fed”—that is, when they (adolescents) do not approach them for SRH discussion, we cannot force them to do so. It was evident from the discussions that parents wished that their adolescents talk to them on some of these issues so that they can guide them appropriately. Parents reported that their children felt they were “old school” (traditional in views) and may judge them when they initiate a conversation around SRH issues. The possibility was expressed in some of the FGD sessions, in Ibadan Southeast, a man revealed that:
………Some of these children do not want to discuss sex with us, they believe we are old school but when they refuse to talk, what do you think we can tell them? Of course, “a closed mouth can’t be forced to open,” we can only tell them general things about sexuality. If we do not tell them, they can contract HIV or even gonorrhea. So, parents must let the child be aware because most females have males as friends and vice versa……. (Participant 4, 45year old man, FGD with men, Ibadan Southeast)
Another opinion from a woman from Ibadan Northeast reads:
Parents should monitor their adolescents because some of these small boys, what they ought not to know at age 20, they are doing at age 12. Imagine a boy of 14 years impregnated a girl of 12 years, the product of such pregnancy becomes an unwanted child in the street, an unwanted child in the town, and an unwanted child in the society at large. A girl living a wayward life will be treated as such. So, a 12-year-old child that got pregnant, when she is 13 years, she will give birth…. (Participant 1, 42year old woman, FGD with women, Ibadan Northeast)
Some parents’ interests included condom use, diseases, HIV/AIDS, and associated deaths, as evidenced by their expression:
My concern is that many of the diseases talked about are usually contracted through sex because most of them hardly use condoms and will not go to the hospital for a check-up. Even when given money, they will not go, especially those who are not civilised. Yet they will not tell their parents at home that they had sex with a girl that day. Though the fear is there and we have seen such, which resulted in death, he keeps harbouring disease, of which AIDS is a part, and other diseases that are difficult to mention; one can even think it is malaria, and before one gets to the hospital, the situation may get worse. So, this is why we warn them.… (Participant 7, 52year old man, FGD with men, Ibadan Northeast)
Other parents were worried about the spate of adolescents’ sexual activities and associated consequences:
The fear of parents is the increasing rate of sexual activity among girls today, which may result in an unwanted pregnancy, abortion, or damage to her womb, as well as encourage her to continue in sexual activities. Imagine such children! Some girls believe that if they do not have sex every day, their bodies cannot be healthy. However, it is the parents’ fault, especially the mothers. They will have to talk to her so that she will not turn to “Olosho” at her age (Participant 3, 39year old woman, FGD with women, Ibadan Southeast).
When adolescents were asked about what they expect parents to discuss with them, they submitted that they want to know everything about sexual issues. They argued that parents should be free to discuss sex, how it is being done and the consequences with them. They also emphasized that they expected parents to discuss issues of HIV/AIDS, condom use, pregnancy, abortion and STDs/STIs with their adolescents. They opined that if parents equipped adolescents with requisite information about SRH, adolescents would make informed decisions about their lives rather than living them in the dark. Adolescents’ expectations about SRH discussion emerged in the participants’ reflections of what Adio’s and Abeni’s parents should discuss with them (the characters in the vignette):
Abeni’s parents should discuss sex with her, how they do it, and advise her not to have sexual intercourse with a guy. They should educate them on the importance of using a condom and the consequences of not using one in a sexual relationship. Abeni’s parents may also be the cause of Abeni’s attitude, because I think Abeni’s parents were not supposed to have sex in the presence of their children, and I think this is what led Abeni to having sex with Adio (Participant 2, 16 year old girl, FGD with adolescent females, Ibadan Northeast)
Adolescents from Ibadan Southeast expressed their SRH issues of interest. In their words:
The challenge Adio and Abeni may face is that if the two of them have sex and Abeni gets pregnant, they may want to abort the pregnancy. During the course of the abortion, the womb may be destroyed or the person may die. The challenge the parents may have is that they should not assume that they have not been having sex, like some of our parents would assume. They should exercise caution and dialogue with the children because if anything happens to them, it will affect the parents. Parents should talk to them early, even before they see a condom with them; they need to know about these things. It is not new anymore, so parents should not hide it “joo” (Participant 5. 18 year old boy, FGD with adolescent males, Ibadan Southeast)
At this point, many adolescents emphasized the need for parents to advise or talk to their children generally on sexual behaviors and securing their future. According to one of them:
They should discuss sexual health issues with Adio and Abeni. They should advise a female child who is on her period to be careful with men and be patient. They should advise her not to engage in sexual intercourse with any man when having her monthly period; even if the two of them were friends, she should be mindful of the conversations they have and not indulge in any filthy acts. They should also advise the boy not to have sex with any girl or else he will get her pregnant, and with that, her education would be disrupted, and she may suddenly become a homemaker. They should advise the boy to be careful not to impregnate a girl at that stage, saying that he is not mature enough to impregnate a girl, although he has attained the adolescent stage…. (Participant 3, 18 year old Female, FGD with adolescent females, Ibadan Northeast)
From the foregoing, adolescent girls and boys need to know about SRH to reach their full potential. As embodied reality (SRH issues), the constructions of SRH issues by parents and adolescents are influenced by societal, cultural, and individual interpretations of specific SRH issues, as well as the need for conversations concerning them. Evidence from the FGDs supported the quantitative data. Both quantitative and qualitative indicated that parents and adolescents had and should have conversations around SRH issues irrespective of social and cultural depiction. There was consensus on discussing STIs/STDs and HIV/AIDs, contraceptive use, puberty/menstruation, preventive practices, consequences of sexual activities (such as pregnancy and abortion), but for parent and adolescent FGD participants, a greater emphasis was placed on sexual activities.
Discussion of SRH Issues by Parents and Adolescents in Relation to Their Gender
Table 5 displays the SRH issues discussed by parents and adolescents in relation to their gender. A total of 493 parents and 453 adolescents declared they had dialog on SRH issues. Table 5 revealed that puberty is the most discussed, of all SRH issues. Among those parents who have discussed SRH issues with their adolescents, 86.1% of mothers (n = 330) and 67.5% of fathers (n = 163) had communication on puberty. A similar trend occurred among adolescents, where 76.6% of female (n = 273) and 72.2% male (n = 180) adolescents reported to have had discussions on puberty. Responses about relationship with the opposite sex and dating were the next and showed, 77.9% for mothers and 73.6% for fathers while 76.1% male and 72.2% of female adolescents mentioned communication around the relationship with the opposite sex and dating.
Distribution of Specific SRH Issues Discussed by Parents and Adolescents in Relation to Their Gender.
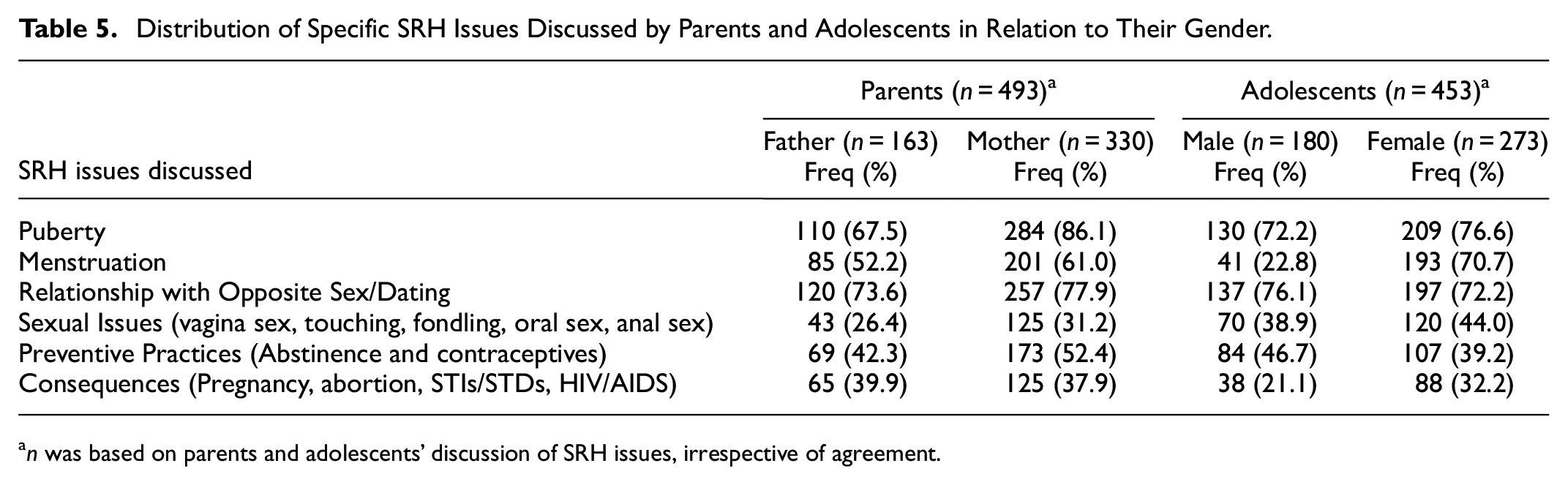
n was based on parents and adolescents’ discussion of SRH issues, irrespective of agreement.
The dialog about menstruation indicated that 61.0% of mothers and 52.5% of fathers had talked about menstruation. Among adolescents, the discussion of menstruation was higher for females (70.7%), while it was lower among male adolescents (22.8%). This is expected as the issue of menstruation is within female adolescents’ domain. However, male adolescents equally require education on menstruation so that they can give necessary support to adolescent girls. Table 5 also illustrates that 52.4% of mothers had communication on preventive practices such as abstinence and contraceptives while among fathers, 42.3% have had such discussion. In contrast, preventive practices were more communicated among males (46.7%) than females (39.2%) adolescents. This is quite interesting because adolescent girls are more vulnerable; thereby, they require more information on preventive sexual practices to lead a healthy life. In all, most of the discussions were done by and with mothers than fathers.
Patterns of Communication Between Parents and Adolescents on SRH Issues
Data presented in Table 6 indicated that one-third (38.0%) of the total population of parents had no communication about SRH with their adolescents. The percentage was higher among adolescents, as nearly half of them mentioned having no communication with their parents. Indirect communication on SRH issues has been reported by slightly more than half (56.2%) and 51.8%) of parents and adolescents, respectively. It can be inferred that parents and adolescents adopted an indirect pattern of communication rather than a direct pattern of communication.
Percentage Distribution of Patterns of Parent-Adolescent Communication about SRH Issues.

In relation to patterns of communication between parents and their adolescents about SRH issues, FGD participants expressed diverse views on the patterns parents should adopt when having dialog with their adolescents. In general, parents stated that they usually advise their adolescents on SRH issues and noted that it should be done step-wisely. Many parents and majority of adolescents agreed on a direct pattern of communication about SRH issues. From the parents’ perspective, two distinct positions emerged from the discussion of Adio and Abeni’s sexual behavior vis-à-vis the possible patterns of SRH communication between parents and adolescents.
The first position asserted that parents should adopt a direct pattern of communication when in dialog with their adolescents about SRH issues. Some participants felt that parents should “call a spade a spade and not a tool for digging” that is, explain openly issues of sex, condom use, menstruation, puberty, pregnancy, abortion, STDs/STIs and HIV/AIDS to their adolescents. According to the participants, discussing these issues openly should not be considered disgusting but rather be seen as an avenue to educate adolescents. They emphasized that parents are in the best position to guide their adolescents about SRH issues. It was further submitted that adolescents will know better and be able to take informed decisions when information about these issues is communicated in an engaging manner and not vaguely. They noted that although the conservative norm around sexuality may serve as a constraint, parents should come out of their shell to face the new realities around sexuality and advise their wards accordingly. Many parents lamented that contemporary SRH issues that were in existence now were non-existent in their adolescent days. The following excepts illustrate some of the positions articulated by the participants:
If a child has attained adolescence, one should sit him or her down and talk to them in a frank way so that he/she will express what they are experiencing. It is also important to inform the child so that he is aware of the situation. Nowadays, things have changed, and one should not sit back and watch the children just like that. One should advise them every time on how to behave and pray that they listen (Participant 1, 47year old woman, FGD with women, Ibadan Southeast)
Buttressing this view, a man from Ibadan Northeast stressed the important role of parents that:
…It is in the hands of the parents to train their children because the teachings are in the Quran and the Bible. When a child is 7 years as a girl, the teachings should be different from when the child is a boy of age 7. The training of girls is different from that of boys. We should give them space to talk to us while also talking to them. Like my child now, I’ve been talking to her mother about what to do and what not to do when a girl has her period ever since I noticed she’d started having her monthly period. (Participant 6, 40year old man, FGD with men, Ibadan Northeast)
Supporting this notion, some adolescents lamented that they prefer open or direct patterns of SRH communication with their parents. When reacting to Adio and Abeni’s story, they submitted that parents should sit them down and engage Adio and Abeni openly so that they can understand the message. They opined that parents should not use a fear approach or threat, castigate them based on other adolescents’ experiences, or use parables when they want to talk to their adolescents on SRH issues. They believed that rather than engagingly addressing the adolescents’ SRH needs, such a discussion would merely confuse them. One thing that was made obvious in their response was the need for a conversation between parents and adolescents concerning SRH issues, with parents taking the initiative. The following are the typical statements made by the adolescent’s participants:
They should sit her down and encourage her to express her concerns, but they should not react to the situation. They should not try to put fear in her mind; otherwise, she will not understand the message… (Participant 9, 17 year old girl, FGD with adolescent females, Ibadan Southeast)
Another participant submitted that:
Although it may be difficult for Adio’s parents to start the discussion, they should sit him down and educate him on sexual behaviour in general. They do not need to be harsh on him because being harsh will not make him listen to them. All they should do is talk to him in a way that will make him pour out his mind to them. That is the best (Participant 4. 16 year old boy, FGD with adolescent males, Ibadan Southeast)
One adolescent echoed that parents must live with the reality that the world is changing, and their parents must flow with the trend. According to him:
Sometimes parents need to come to the realisation that their children are not young anymore. Adio and Abeni have their lives to live, and their parents should respect that. They should bring it up normally so that they can both discuss the issues. They should talk to Adio with love so that he will not feel as if they are blaming him. They will make him curious about it if they blame him or talk indirectly about it. (A 17 year old boy, FGD with adolescent males, Ibadan Northeast)
Also, a female adolescent explained that discussion should be done in the form of question and answer without being harsh. She said:
If I were a parent, I would know that not every time you cane a child, that child will respond to your correction. When they saw her with a condom, they were supposed to sit her down and talk to her. I will ask her why she has a condom in a friendly manner, and if she tells me about it, I am not supposed to beat her. I am supposed to advise her because she already has the condom and probably has already started having sex, so no one can stop her. I will have to advise her on how to use the condom to prevent her from getting pregnant or contracting STDs. (Participant 2, 18 year old girl, FGD with adolescent females, Ibadan Northeast)
As a counter reaction to a direct pattern of communication, most men and women participants affirmed that parents should communicate indirectly with their adolescents on SRH issues. In the FGD with parents, the participants suggested diverse ways of passing SRH information across to the adolescents, which included warning, threat, beating or scolding, storytelling, words of God, and advice. The participants lamented that, despite several warnings, threats, and punishments, adolescents still indulge in indiscriminate sexual activities and other risky sexual behavior. Although most parents felt uncomfortable discussing SRH-related issues openly with their adolescents, they noted that adolescents may want to experiment when SRH issues are discussed in a direct way. Thus, parents are cautious in engaging their adolescents in SRH discussion. In general, most parents think that adopting a direct communication pattern would make them promiscuous or spoil them rather than benefit them, hence they wait until an opportunity presents itself for such a discussion. As opined by the participants:
What I see is that before one can talk to a male child about such issues, it is common that the female child is the most corrupt. My little boy was called in by a girl in my area. When I caught them and wanted to beat them, my child refused, claiming that the girl had summoned him to bring out his penis. So, it’s girls that seduce boys. So, in my opinion, one will have to use an iron hand on the boys and talk to girls from ages 12 and above (Participant 5, 47 year old man, FGD with men, Ibadan Southeast)
In a similar vein, when responding to Adio and Abeni’s story, only a few adolescents conceded that some parents usually adopt an indirect pattern of SRH communication. As articulated by the adolescents:
If it is me, my mother will beat me like mad. Because I remember when my brother did something like that, they beat him and put him in the house and told him he couldn’t leave for three days and three nights. That’s what I know about it (Participant 2, 18-year-old boy, FGD with adolescent males, Ibadan Northeast).
It can be deduced from participants’ conversation that realities around SRH issues are constructed differently. In relation to patterns of SRH discussion, a dissonance was noted in the quantitative and qualitative results. When interrogating the data, it was clear that a different proportion of participants in the quantitative and qualitative confirmed the adoption of either a direct pattern or an indirect pattern of communication. However, a dominant pattern of communication noted in the quantitative data was an indirect communication pattern while a direct communication pattern was echoed by the qualitative participants. The reason for this may be the vignette used for data collection, as all the participants may have given socially desirable responses about SRH communication pattern.
SRH Issues and Patterns of Communication
Table 7 showed the cross-tabulation of participants’ SRH discussion with communication patterns about specific SRH issues. As demonstrated in the table, parents and adolescents were interested in the six domains of SRH issues, namely, puberty, relationship with opposite sex/dating, sexual issues, preventive practices and consequences of sexual behavior. For all these SRH issues, Table 7 clearly illustrates that most parents and adolescents had adopted an indirect pattern of communication on all six domains of SRH. The chi-square values for each topic were not significant for parents and adolescents, however, only discussion of preventive sexual practice was significant for parents (0.042) at a significant level of 0.05 and adolescents (0.000) at a significant level of 0.01. This implies that parents and adolescents were more interested in preventive sexual practices compared to other topics.
Distribution of Specific SRH Issues Discussed by Parents and Adolescents and Patterns of Communication.

p < .01. *p < .05.
Discussion of Findings
The results of this study provide insights into the reality of SRH communication between parents and adolescents. It also revealed specific SRH issues parents and adolescents discussed; and patterns of SRH discussion in the urban slums of Ibadan, Southwest, Nigeria. The findings showed that 69.1% of parents and 56.9% of adolescents have had a conversation around SRH issues in the selected slums of Ibadan. This concurred with earlier findings by Iliyasu et al. (2012) and Kunnuji (2012) from Nigeria and similar findings from Ethiopia (Dessie et al., 2015) and Tanzania (Wamoyi et al., 2010) about the dynamics of SRH communication between parents and their adolescents.
Findings from specific topics of communication revealed that parents were interested in: puberty, menstruation, relationship with the opposite sex and preventive sexual practices. Adolescents, on the other hand, indicated that they had discussed three SRH issues, which include; puberty, menstruation, and relationship with the opposite sex. Therefore, common SRH issues that parents and their adolescents discussed were puberty, menstruation, and relationship with the opposite sex. Two standpoints can be discerned in this finding. First, there exists a consensus on three SRH topics of discussion between parents and adolescents. This indicates a changing stance in the conversation around SRH among parents and adolescents. Such dynamics might be connected to changing parental values and the possible impacts from ongoing campaigns on sexual health education at school level in Nigeria (Orji & Esimai, 2003). The evidence that parents are gradually engaging their adolescents on SRH issues has been earlier reported by Manu et al. (2015) in Ghana. The issues the parents in Manu et al. (2015) study were discussing with their adolescents appear synonymous with what emerged from this study. This consensus again resonates the tension and issues parents go through based on cultural values and beliefs and their sense of what would benefit their adolescents. Second, parents emphasized preventive sexual practices, which reflect a disconnection between parents’ expectations and adolescents’ expectations. The possible explanations for this disconnection may be due to contestation between sexual regulations and sexual rights. Parents may conceive sexual regulation from the point of abstinence and feel adolescents are unripe to exercise their sexual rights. In contrast, adolescents’ worldview is gradually expanding with the advent of social media and seem to be questioning moral viewpoints of their parents about SRH issues. Adolescents may feel choked by their parents’ worldview and struggle to exercise their sexual rights. This gives the adolescents limited opportunity to engage their parents in the discussion of sensitive SRH issues. Parents have a role to play in ensuring that adolescents build confidence around them by displaying a liberal worldview that accommodates adolescents’ worldview around SRH issues.
However, the finding that parents discussed sensitive topics with their adolescents negated the finding of Nundwe (2012) in Ghana. Nundwe documented that parents fail to communicate sensitive SRH issues such as condom use, puberty, STIs, and physical development but do so on less sensitive ones such as the effects of HIV with adolescents due to some barriers. These barriers have been documented by Bushaija et al. (2013), Nundwe (2012), Velazquez (2014), Velcoff (2010) as cultural norms and taboos, gender differences, and religion were linked to inadequate parent-child communication on SRH issues in SSA. This could indicate parents’ inability to break away from the conservative norms around sexuality and may be uncomfortable broaching these issues or believe that the discussion of such could lead adolescents into sexual immorality. Hence, the general trend suggests that parents were interested in their adolescents’ SRH safety. This further reinforces the need to change the culture of silence around sexuality and educate adolescents appropriately on SRH issues.
Also, this study established that even when communication about specific SRH topics occurs, it is often not direct as the pattern employed is devoid of engaging dialog between parents and adolescents. Parents’ and adolescents’ reports indicated that they have engaged in indirect patterns of communication concerning SRH issues. These indirect patterns include the use of warnings, instructions, threats, other adolescents’ experiences, stories, books, among others, without the opportunity for dialog. Similar findings were reported in a study conducted in Ghana by Kumi-Kyereme et al. (2007) that communication between parents and adolescents often takes the form of instruction from parents to adolescents rather than dialog. In the same vein, another study from rural Tanzania submitted that SRH discussion between parents and their children was often unidirectional, initiated by parents and took the form of warnings or threats or sometimes gossip (Wamoyi et al., 2010). As noted by Kajula et al. (2014) parents were naturally inclined to discuss HIV/AIDS with their children because there is no cure available. However, they submitted that when parents employ scare tactics, it may induce anxiety and thereby discourage adolescents from asking relevant questions. The implication is that when adolescents do not have the opportunity to ask questions, they are denied the chance to get clear and consistent information about what seem to be complex SRH issues. Therefore, it can be concluded that adolescents may not benefit fully from such communication compared to when parents give clear explanations and directions on “what to do and how” and especially when such discussion is mutually engaging.
The empirical evidence is consistent with the idea of Berger and Luckmann’s (1991) theoretical postulate that communication is an essential system through which humans construct their reality. The theoretical exposition further emphasized that learning is embedded in, and should be treated as a product of social interaction. This proposition plays itself out in understanding parent-adolescent SRH communication in the selected urban slums. As social-actors-in-context (parents and adolescents), culture or society may have dictated what the topics of discussion could be. However, the reality of adolescents may warrant a reconstruction of meaning around SRH issues to foster active learning as postulated by social constructivism theory. As a precondition of social constructivism theory, parents and adolescents must have good rapport and share a similar understanding of SRH issues for responsive communication to occur. Parents need to live with the current reality that most adolescents are sexually active. They both live in the fast-growing information age and in a world that is much different from that of their parents, hence, require appropriate SRH information to live a healthy life. Concerning the findings of this study, parents were well aware of the need for SRH communication between them and their adolescents, although they both adopted an indirect communication pattern. Inference from FGDs shows that parents wanted their children to be well informed about sex, sexual health, and relationships. Parents believed that factual SRH information could only come from them to their children. Adolescents also acknowledged that they expected more information from their parents. The finding of this study is exciting and encouraging as the topic of SRH discussion is increasing between parents and adolescents—an indication that the culture of silence about sexuality in Nigeria, and by extension, in Africa is gradually being broken.
Strengths and Limitations
The study provided insight into the common SRH topics discussed by parents and adolescents. The use of a mixed-method approach to parent-adolescent communication on SRH issues provides robust data from the quantitative and qualitative mix, especially the use of a vignette to obtain information on sensitive SRH issues compared to employing either approach. Again, the inclusion of parent-adolescent pairs made it possible to explore the dynamics of parents’ and adolescents’ perspectives on SRH communication.
However, the following limitations should be taken into consideration when interpreting the findings of this study. First, a dichotomous scale of “yes” and “no” was used to measure topic-specific SRH discussion between parents and adolescents as well as the existence of such communication. This may have imposed some limits on the validity and reliability of the measure. Second, the a priori statistical power was never estimated for the sample size but implied, which may have affected the significance of the study’s findings, although the intention was never to test any hypotheses but to establish the existence or otherwise of parent-adolescent communication about SRH issues in slums. The use of a mixed methods research design mitigated this. Third, recall bias could have affected the retrospective measurement of parent-adolescent communication adopted in this study. The limitation was perhaps mitigated by using a vignette. Fourth, social desirability could have also shaped the responses and views expressed in a way. Fifth, because the study was conducted in a relatively homogenous social setting inhabited mostly by Yoruba people, the findings may not be generalized to other social contexts or non-slum settings that are inhabited by diverse ethnic groups. A similar study among the various ethnic groups in Nigeria might show some variation.
Policy Implication
The findings of this study have implications for policy. From the perspectives of the parents and adolescents who live in slums, researchers, policymakers, and program experts may be able to develop interventions that are socially and culturally acceptable as well as contextually relevant. Of necessity, the generational gap in cultural perception and interpretation of SRH issues must be closed. Critical areas of concentration should include developing enduring relationships between parents and their adolescents through trainings and community outreach. Radio and television programs that foster family contexts where SRH issues are discussed can be developed via the broadcast media. These programs should take into account the slum context by reflecting their SRH realities. As a result, the parent-adolescent bond will be strengthened, SRH-related communication will be improved, and a sense of community that is supportive of adolescents will be promoted. Furthermore, the results of this study have practical implications that merit further investigation. To identify the communication style between parents and adolescents that supports adolescents’ SRH discussions, more study is needed. Future studies should give adequate attention to parents and adolescents from various ethnic backgrounds who live in urban slums. This would provide a comprehensive understanding of how SRH communication may be influenced by parents’ and adolescents’ diverse cultural beliefs and orientations.
Conclusion
This study concludes that the SRH issues that parents and adolescents discussed were similar in several ways. In their conversations about SRH issues, both parents and adolescents have adopted an indirect communication pattern. Thus, there is a need for a mutually engaging avenue to explore discussions on SRH issues between parents and their adolescents so as to address adolescents’ SRH needs in the slums. The findings of this study indicate the need for interventions (sexual health communication training) that will strengthen and improve parent-adolescent communication around sensitive SRH issues in urban slums. Such interventions should target appropriate delivery strategies for SRH issues and encourage communication to begin early between parents and adolescents slum dwellers. Also, the intervention should address barriers to SRH communication and find the middle ground between parents and adolescents by considering and balancing parent expectations of adolescents’ SRH and adolescents’ rights to appropriate SRH information. This will encourage parents to easily break away from the conservative norms around sexuality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Consortium for Advanced Research Training in Africa (CARTA). CARTA is jointly led by the African Population and Health Research Center and the University of the Witwatersrand and funded by the Carnegie Corporation of New York (Grant No. G-19-57145), Sida (Grant No:54100113), Uppsala Monitoring Center, Norwegian Agency for Development Cooperation (Norad), and by the Wellcome Trust [reference no. 107768/Z/15/Z] and the UK Foreign, Commonwealth & Development Office, with support from the Developing Excellence in Leadership, Training and Science in Africa (DELTAS Africa) program. The statements made and views expressed are solely the responsibility of the Fellow.