
Abstract
The purpose of the study ¿Confías en mi? (Do You Trust Me?) was to identify three characteristics—expertise, trustworthiness, and accessibility—of Latino parent–adolescent communication. We examined how these characteristics may influence communication about romantic relationships and sexual risk reduction strategies (i.e., abstinence, contraception). A total of 21 parent–adolescent dyads (N = 42) completed a brief demographics survey and a set of scales to obtain quantitative measures related to parental characteristics that may influence the adolescent’s perception of parental advice. An in-depth, semi-structured interview was then conducted with each parent, followed by the adolescent. Findings demonstrate that parents talk to their children, but overall conversations are not specific or comprehensive enough to support adolescents’ informed decision making about sexual health or building positive romantic relationships. Community organizations such as churches, schools, and medical settings can support families by providing brief seminars that not only provide technical information about sexual health but also allow parents to practice how to initiate communication about sex and how to gauge their child’s receptivity to discuss the topic further. Recommendations include encouraging parents to actively engage their adolescent in shared communication over time, respond to questions openly and accurately, and demonstrate concern in the teen’s life happenings.
Parental communication becomes particularly important as adolescents begin to make choices related to dating and exploration of sexuality. This communication should start early given that the prevalence of sexual intercourse increases with age, with some children starting very young, and a substantial number of youth not using protection against sexually transmitted infections or unwanted pregnancies. According to the 2013 Youth Risk Behavior Survey, the proportion of high school students who reported ever having sexual intercourse increased systematically from 30% in ninth grade to 64% in 12th grade. In all grades, a small proportion of students (6%) reported having sexual intercourse before 13 years of age. Most worrisome from a public health perspective is that, of those who reported being sexually active, 41% did not use condoms during last sexual intercourse and the majority (75%) were not using other forms of birth control (Centers for Disease Control and Prevention [CDC], 2014). Although most adolescents report some communication with their parents about saying no to sex or about using methods of birth control (CDC, 2011), the characteristics of this communication from the perspectives of the parents and the adolescents need further study. Communication with parents is essential in an age when adolescents are constantly accessing media messages that may not align with their parent’s values.
Specific risk factors for teenage pregnancy and sexually transmitted infections have been associated with Latino youth. Latino adolescents are less likely to use contraception than their non-Hispanic White counterparts, and condom negotiation skills among Latino women are low (CDC, 2012; Gilliam, 2007; Romo, Lefkowitz, Sigman, & Au, 2001). In some studies, Latino males have reported a dislike for using condoms or have stated that birth control is a woman’s responsibility (Benavides, Bonazzo, & Torres, 2006; Gilliam, 2007). Latina adolescents and young adults have reported little or no knowledge about sex or contraception because communication about these topics did not occur in the home, particularly for those who indicated having “strict parents” (Adolph, Ramos, Linton, & Grimes, 1995; Erickson, 1999; Gilliam, 2007; Romo et al., 2001). Among those who did communicate with their family, Gilliam noted that incorrect information from parents—such as a mother telling her daughter about unfounded adverse effects of birth control pills—may increase susceptibility to pregnancy.
In this study, we examined three parental characteristics that may influence communication about sexual health: expertise, trustworthiness, and accessibility. Expertise is critical for two reasons: (a) Parents need to know enough information or at least know where to access information to provide advice, and (b) parents who believe that the school provides sufficient or better instruction than they could give may choose to avoid talking about sexuality with their child. A possible impact of this decision is the child’s belief that the parent does not have enough knowledge and therefore may choose not to ask the parents. Trustworthiness refers to how much perceived expertise a parent has and the extent to which teens feel that the parents will answer sensitive questions honestly. Accessibility relates to whether the parent is available and willing to talk with the adolescent if the child is interested. Together, these three characteristics enable the degree to which specific topics are addressed, the frequency of the conversation, and the extent to which the adolescent accepts the content of the conversation (Guilamo-Ramos, Jaccard, Dittus, & Bouris, 2006).
The purpose of this study was to identify the characteristics of Latino parent–adolescent communication—expertise, trustworthiness, and accessibility—that may influence communication about romantic relationships and about reducing risks associated with sexual behaviors (i.e., abstinence, contraception). In-depth interviews were conducted separately with parents, followed by their adolescents. Both parents and adolescents completed a set of scales. This article presents findings from one of the scales, and excerpts from interviews are used to support categories set by the scales.
Method
Participants
The sample was recruited from a community clinic located in a county with a large Latino population in Southeastern United States. The clinic is one of the few that provides access to mental health services to Spanish-speaking Latinos. In addition to treatment and intervention programs, the clinic also sponsors primary prevention programs aimed at fostering positive and productive life paths for youth and their families. Thus, a wide range of Latino families attended the clinic. Eligibility criteria for this study were as follows: Latino parents of adolescents aged 12 to 17 years and their respective son or daughter attending a program at the community clinic. Each participant completed a short survey and a semi-structured interview.
Procedures
The university’s institutional review board approved all procedures. Clinic staff distributed a study flyer and informed possible participants about the purpose of the study and eligibility criteria. The first author called clients who had voiced an interest in participating to confirm interest and eligibility and arrange a meeting at the clinic. Parents signed an informed consent, and adolescents signed an assent form. Each parent–adolescent dyad received a US$50 gift card on completion of the session. Parents and adolescents were surveyed individually. Adolescents were interviewed last to increase their trust and assure confidentiality of their reporting.
Measures
The Adolescent Sexual Experience (Romo, Lefkowitz, Sigman, & Au, 2003) measure has five items that indicate increasing levels of sexual involvement. The stem of the questions was “Have you ever” followed by kissed someone, touched someone over the clothes, touched someone under the clothes, touched someone’s genitals, and had sex. Students who reported that they had had sex answered a follow-up question about whether they had had vaginal, oral, or anal intercourse. Response categories were Yes/No.
The Parental Expertise, Trustworthiness, and Accessibility (PETA; Guilamo-Ramos et al., 2006) measures the parent’s and adolescent’s perception of parental expertise, trustworthiness, and accessibility (12 items, three items for each construct; alpha = .82 for the parent scale and for the adolescent scale). Expertise refers to the perception that the parent is credible and gives sound advice. Trustworthiness refers to the perception that the parent is honest and wants the best for the child. Accessibility refers to the perception that the parent is available to spend time with the child and has conversations as needed. Parents and children completed the survey independently. The items vary to reflect the respondent. For example, an item measuring parental expertise is “my child thinks I give good advice” for the parent survey and “my mother gives good advice” for the youth survey. Respondents indicated the level of agreement with each statement, in a 5-point Likert-type scale (strongly disagree to strongly agree). Scale scores were calculated as the mean of the items. Thus, scales ranged from 0 to 4, where higher scores reflect a stronger support of the construct.
Data Analysis
Descriptive statistics and scale means were used to compare parent and child responses and triangulate data obtained from the interviews. As we examined scale data, we used interview transcripts to understand how participants elaborated particular issues. The constant comparative method was used to analyze interview data and identify patterns within dyads. Constant comparison allows the researcher to build an understanding of a social process through a theory grounded in data (Boeije, 2002; Charmaz, 2006; Kozma, 1985).
Results
A total of 21 dyads (42 people) composed of a parent and a child participated in the study. The majority of participants were mothers; only two fathers chose to participate. The large majority reported being married or living with a partner. The sample of parents was fairly young (<40 years), and all but one were born outside the United States, primarily in Mexico. Foreign-born parents had lived in the United States between 11 and 19 years. Parents came from diverse educational backgrounds (no high school diploma = 5, high school diploma = 2, some college = 5, college graduate = 5). Most parents reported working outside the home, with an annual household income at or less than US$35,000. A majority (14) of parents reported not having health insurance. All but one of the parents reported ascribing to a religious faith they practiced weekly or monthly. The majority of parents (15) indicated that Spanish was the primary language spoken in the home.
The adolescent sample was composed of 12 girls and 9 boys ranging in age from 12 to 17 years. Slightly more than half of the children (11) were born in the United States, and the others were foreign-born: Mexico (6), Puerto Rico (2), and Central or South America (2).
Table 1 depicts mean scores in the PETA scale for each parent–child dyad and the sexual experience reported by adolescents. To protect participant confidentiality, data were grouped by adolescent age range and the parent gender was not identified. None of the adolescents reported having touched someone’s genitals or that they had anal sex. Thus, adolescent sexual experience was grouped as follows: none, kissed, touched on top of or under clothing, oral sex either given or received, and sexual intercourse with vaginal penetration.
Means in the PETA Subscales Within Dyads and Child Sexual Experience by Age Group of Child.

Note. PETA = Parental Expertise, Trustworthiness, and Accessibility Scale. Bold indicates higher score. Scores range from 0 to 4; high scores indicate more parental expertise, trustworthiness, and accessibility.
Overall, parents reported slightly higher perceptions of expertise (parent M = 3.22; child M = 3.00) and trustworthiness (parent M = 3.30; child M = 2.90) than their adolescents. Interestingly during interviews, most parents reported they did not have sufficient expertise to speak with their children about sexual health topics and in some cases felt intimidated by their children’s knowledge. Compared with parents, adolescents overall perceived higher levels of parental accessibility (parent M = 2.23; child M = 2.62).
Younger adolescents (12-13 years) reported little to no sexual experience, primarily kissing, compared with older adolescents (14-17 years) who ranged from having no sexual experience through sexual intercourse with vaginal penetration. One of the adolescents who reported having sexual intercourse had a full-term birth.
In a few instances, concurrence was noted in expertise (Dyads 2, 13, and 18), trustworthiness (Dyads 5 and 18), and accessibility (Dyad 9). Only one dyad (18) demonstrated concurrence on at least two dimensions: expertise and trustworthiness. During interviews, this dyad reported sharing comprehensive sexual education, and both parent and child were satisfied with their level of communication. The parent in this dyad was also the only one who chose to conduct the interview in English.
Regarding expertise, most of the dyad means were not too divergent suggesting fairly even perceptions between parents and teens. Five dyads (5, 6, 8, 10, and 16) had a wider gap in their perception of expertise. Parents in these dyads reported higher perceived expertise; however, the adolescent in Dyad 10 reported a higher perception of parental expertise. Adolescents in these five dyads were almost evenly divided between the two age groups: younger and older, negating an age-related influence on perception. Sexual experience reported by adolescents in these five dyads ranged from no experience to touching.
On the dimension of trustworthiness, slightly more dyads had wider gaps in parent–child means (3, 4, 7, 8, 10, 11, and 13). Two of these dyads (8 and 10) also reported wide gaps in expertise. The interviews with the parent and child in Dyad 10 were consistent with the scale results: Mother and daughter confirmed that they did not communicate about sexual health. However, the parent in Dyad 8 reported very specific conversations she had with the son about contraception and respecting partners although the child did not recall those during his interview. In addition, this dyad’s divergent scores may reflect that the communication by the parent did not resonate with him resulting in low perceived expertise and trustworthiness. Similar to expertise, the adolescent age groups represented by these dyads were almost evenly divided (four younger and three older), and sexual experience reported by these teens ranged from no experience to touching.
Adolescents more often than parents reported higher perceived accessibility. Twelve dyads (1-5, 7, 12-15, 17, 18) evenly divided between older and younger adolescents demonstrated wide gaps in the mean scores of accessibility. Four of these dyads (3, 4, 7, and 13) also had large gaps in trustworthiness. Although it is possible that an association exists between perceived accessibility and trustworthiness, there is insufficient support based on mean scores. When comparing the level of sexual experience reported by teens in these 12 dyads to perceived parental accessibility, sexual experience ranged from no experience to touching; and one teen reported having oral sex. Interestingly, of the three teens (19-21) who reported sexual intercourse, gaps between parent and child means on any of the three dimensions were not large. However, their mean scores for accessibility were low. In the case of Dyad 21, which represented the teen that had a full-term birth, all three dimensions were at or below the average for the groups.
Case Examples
We use case examples (Tables 2 to 4) to demonstrate the variation observed in parental characteristics. Comparisons are based on mean scores from the PETA Scale. A dyad was classified as “high” when parent and child mean scores were between 3.0 and 4.0 and as “low” when mean scores were at 2.0 or below for both parent and child. “Parent higher than child” refers to a noticeable gap in mean scores where the parent perceived demonstrating more of that characteristic than the child did. A quote by each parent and child is used to support the comparison score. As these tables demonstrate, the interview data highlight variations in participant responses and provide a useful context for scale scores described earlier in this chapter.
Case Examples of Parental Expertise by Level of Concordance in PETA Scale Scores.

Note. Parental expertise refers to the perception that the parent is credible and gives sound advice. PETA = Parental Expertise, Trustworthiness, and Accessibility Scale; STD = sexually transmitted diseases.
Case Examples of Parental Trustworthiness Perceived High or Low by Both Parent and Child and Perceived Higher by Parent Than Child.
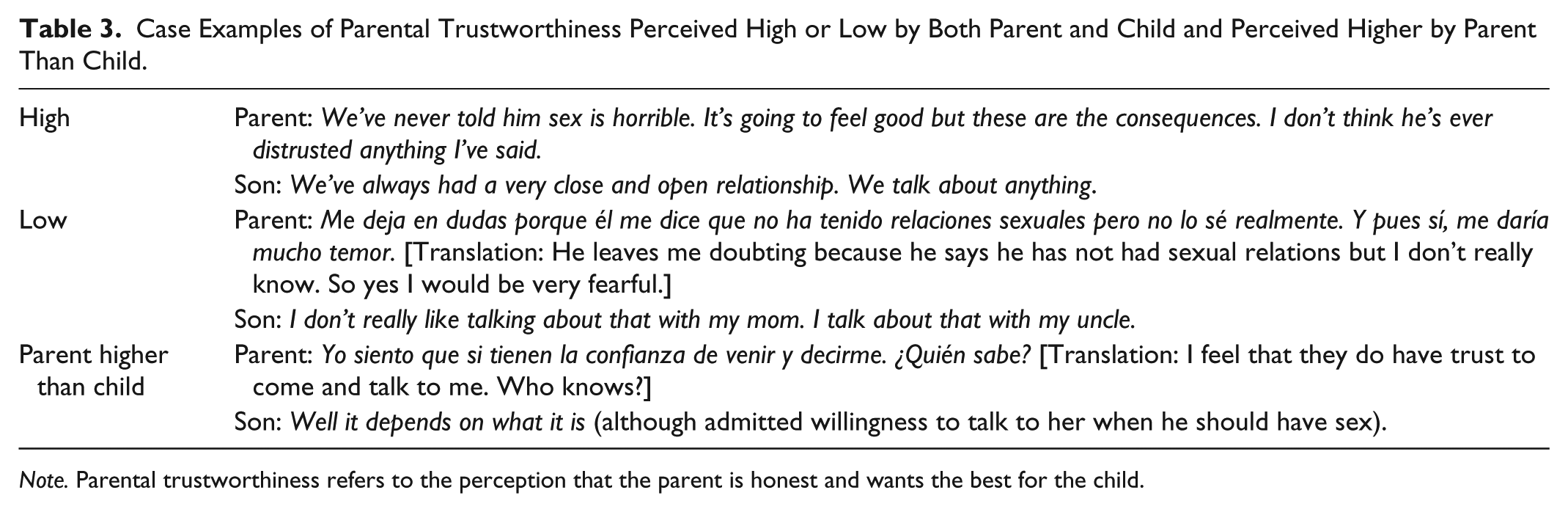
Note. Parental trustworthiness refers to the perception that the parent is honest and wants the best for the child.
Case Examples of Parental Accessibility Perceived High or Low by Both Parent and Child and Perceived Higher by Parent Than Child.

Note. Parental accessibility refers to the perception that the parent is available to spend time with the child and has conversations as needed.
Discussion
Using scales and interviews, we examined how parental characteristics affected the adolescent’s knowledge of sexual health, perception of the message, and ultimately his or her sexual behavior. Findings demonstrate that parents talk to their children, but overall conversations are not specific or comprehensive enough to support adolescents’ informed decision making about sexual health or building positive romantic relationships.
Parental characteristics examined in this study were expertise, trustworthiness, and accessibility. Interview data suggest that two of these, expertise and trustworthiness, particularly influenced communication between parents and adolescents. Interestingly, scale data suggest that when both the parent and adolescent perceive the parent is not accessible, it may affect older adolescent’s decision making about sexual intercourse.
Expertise
Despite most parents reporting high perceived levels of expertise on the PETA Scale, parents who reported lower levels of education during interviews were likely to feel they lacked the necessary knowledge to communicate with their adolescent about sex. The inconsistency may be related to perception of expertise, however. The items measuring expertise relate to giving advice, whereas the discussion of expertise during interviews focused on knowledge to answer questions about sexual health and disease prevention. Therefore, this subtle difference in perceived meaning of expertise prevents comparison between methods but suggests an expanded construct that can be explored further.
Many parents in this study believed their child received what was needed from school and did not require their further input. Future studies may consider adding a knowledge scale to measure parent knowledge about sexual health. However, some adolescents prefer receiving information about contraceptives from parents, followed by a health education class (Hacker, Amare, Strunk, & Horst, 2000). Therefore, parents need to equip themselves to support and elaborate on what their teen learns in school.
Latino immigrant parents with low economic resources favor receiving resources that can improve familial ties, particularly those that involve face-to-face interaction with peers and culturally tailored information (Allen et al., 2013; Hurwich-Reiss, Rindlaub, Wadsworth, & Markman, 2014; Villalba, Gonzalez, Hines, & Borders, 2014). Community organizations such as churches, schools, and medical settings can support families by providing brief seminars that not only provide basic technical information about sexual health but also allow parents to practice a skill such as how to initiate communication about sex and how to gauge their child’s receptivity to discuss the topic further. Applied workshops are particularly helpful for Latino parents who may not speak English or may have low educational attainment from their country of origin (Orpinas, Ambrose, et al., 2014; Orpinas, Reidy, Kogan, Londoño-McConnell, & Powell, 2014).
Trustworthiness
Messages to parents about the importance of communication should emphasize that consistent and open discussions with adolescents can improve trust and closeness. Families that demonstrate high functioning relationships report more parent and child communication about sex (Malcolm et al., 2013). Specifically, good parent–child relationships are important in reducing unprotected intercourse particularly among younger adolescents, delaying intercourse initiation, and increasing diagnosis of a sexually transmitted infection (Deptula, Henry, & Schoeny, 2010). Parents who actively engage their adolescent in shared communication over time, respond to questions openly and accurately, and demonstrate concern in the teen’s life happenings increase the probability of being seen by the adolescent as an expert and trusted source. However, a belief that hindered some parents from talking with their children was that providing information, particularly about contraception, would encourage sexual behavior. Yet, research has shown that adolescents who receive comprehensive sex education compared with those who receive an abstinence-only education are at 50% lower risk of teen pregnancy (Kohler, Manhart, & Lafferty, 2008). In addition, sex education that includes abstinence and birth control information positively influences contraception behaviors, partner selection, and reproductive health outcomes (Lindberg & Maddow-Zimet, 2012). When parents talk with their children about sex, it builds trust, increases closeness, and reinforces protective behaviors related to sexual health.
Accessibility
Quantitative data from the PETA Scale indicated that among the three older teens who reported having sexual intercourse, both parents and teens scored low in accessibility. It should be noted that there were other dyads among the older teen group that had similarly low means, except the sexual experience of those teens had not progressed beyond touching. An association between perceived accessibility and teen sexual intercourse cannot be properly determined based on data collected in this study. However, this finding suggests an aspect that can be examined in a larger study.
This study has limitations. Although saturation, the point when no new information emerges from coding (Saldaña, 2009), was achieved and it is an adequate tool in qualitative studies to determine when to cease recruitment, findings based on the scales were limited as a result of the sample size. A larger and more diverse sample that includes more fathers would have enhanced findings and possibly suggested new relevant themes or clarified existing ones.
Another limitation was that recruitment occurred in one community clinic representing an at-risk population seeking mental health and substance use services, predominantly from a lower socioeconomic level. Study participants reported experiences with domestic violence, childhood abuse, mental health conditions, and a variety of other relational challenges that may have affected how they responded. Therefore, findings from this study may not be applicable to a broad Latino population and thus limit generalization.
Implications for Practice
Findings from this study support three recommendations for parents to enhance communication about sexual health with their adolescent children. First, parents are encouraged to have open and accurate communication to build trust and reinforce protective behavior. In this study, parents who answered their teens’ questions as they arose reported more open communication compared with parents who planned to talk when they observed their child demonstrate romantic interest in another teen. Using external cues, such as questions asked, parents have the opportunity to answer honestly and factually. If parents do not have the answer to a question, they can refer to factual resources to explore answers with their child and thereby reinforce trust. Second, parents should discuss the characteristics of good relationships and model how one demonstrates respect for a partner. Initiating conversation early in a child’s life about showing respect for family and friends, and later transitioning the conversation from friends into a romantic partner, can reinforce trust in the parent–child relationship and facilitate communication about more sensitive topics as the child matures, such as sexual health, pregnancy, and disease prevention. Third, parents should weave conversations about values and personal expectations for the adolescent’s future into routine communication. Most adolescents in this study had observed their parents struggle to make ends meet and were clear that parents wanted them to go to college and build a better life for themselves. However, adolescents who demonstrated the clearest sense of parental expectations also described how their parents shared personal life experiences. Most often, these were older adolescents and those who had chosen abstinence. Therefore, sharing values and beliefs in the context of a fact-based message can help promote protective behaviors such as delayed sexual debut.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.