
Abstract
This article summarizes an investigation of the stigmatization of depression in Thailand to determine whether there is a relationship between depression literacy and personal stigma and perceived stigma. This mixed-method study utilized two questionnaires, the Depression Literacy Questionnaire and the Depression Stigma Scale, by Griffiths et al. and subsequently asked participants for their opinions of depression and stigmatization within the Thai context. About 914 online surveys were processed using correlational and descriptive analysis. Results indicate that the depression literacy score was moderate to average. Personal stigma, on average, was low to moderate. Perceived stigma, on average, was moderate to high. The correlation between depression literacy and personal stigma was a strong negative correlation, unlike in depression literacy and perceived stigma. The correlation between personal stigma and perceived stigma was a moderate positive correlation. The level of negative stigma was lower than the perceived stigma. This research indicated that depression literacy had a significant negative correlation with personal stigma but no correlation with perceived stigma. Other factors such as sex, level of education, religion, and prior experiences with people with depression play a moderate role in the level of depression literacy and personal stigma.
Introduction
Despite awareness of depression and its impact on Thai society, little is known about depression knowledge and the stigmatization of the depressed. Previous studies reported that high levels of depression knowledge are associated with positive attitudes toward depression (Mannarini & Boffo, 2014; Mingkwanjai et al., 2015; Ozmen et al., 2005; Pumpayung & Taifapoon, 2018). However, there is limited research on the relationship between depression knowledge and attitudes in Thailand, and the findings available are often contradictory (Mingkwanjai et al., 2015; Pumpayung & Taifapoon, 2018; Thadanukoonwattana et al., 2016). This study aims to contribute to the knowledge of Thai perceptions and stigmatizations of depression through the analysis of an online survey. The findings may prove beneficial for mental health workers, policymakers, and researchers in designing effective means to promote knowledge and reduce the stigma of depression in Thailand.
Literature Review
The concept of depression literacy originated as an offshoot of mental health literacy (MHL) which arose from health literacy. The World Health Organization (WHO, 2020) has defined MHL as the social, cognitive, and motivational ability of individuals to gain access to, accurately understand, and act on information positively, which promotes and maintains good health. Jorm et al. (1997) creation of the sub-set, MHL, focused on common conceptualizations of and beliefs in mental disorders, which consisted of the ability to recognize disorders, knowledge of causation, and risk factors associated with different disorders, knowledge of treatments and interventions, knowledge of psychological and psychiatric services available, help-seeking attitudes and knowledge of resources available to learn more about mental health (Jorm, 2000). Subsequent research indicates that adequate MHL assists with the help-seeking behavior (Eisenberg et al., 2009; Jung et al. 2017), prevention of relevant complications, and a reduction of long term harm (Arafat et al., 2019; Noroozi et al., 2018).
According to the WHO (2017), depression affects more than 300 million people worldwide. The specific focus on depression literacy is an important area of research. It can elucidate the public’s perception of depression and lend to creating prevention plans, assisting with diagnosis, intervention, and treatment (Burns & Rapee, 2006; Coles et al., 2016). Depression literacy includes knowledge about depression as a psychiatric disorder and the relevant epidemiology, etiology, symptomatology, treatment, and prognosis (Singh, 2019). The rationale for extending the MHL and developing depression-specific instruments was an integral component of assessing the public understanding of mood disorders (Kutcher et al., 2016). Another component that affects mental health literacy is the degree of stigmatization within any given society.
The World Bank Group and WHO (2017) claim that stigmatization reduces social acceptance, prevents the ability or willingness to seek professional help, reduces victims’ self-esteem and relationships, and can lead to isolation, self-harm, and loneliness. Further research indicates that stigmatization is a common trigger for suicide attempts among mental health patients (Carpiniello & Pinna, 2017). Additional studies have endeavored to clarify the sources of stigmatization of mental illness and have concluded that there are specific causal factors such as lower social class (Holman, 2015), educational stratification (Crisp et al., 2000), gender (Pascucci et al., 2017), and differences in socioeconomic status (Mascayano et al., 2015). In addition, psychological stigmas can influence patient treatment and lead to poor health consequences (Motlova et al., 2010). Early labeling theorist Goffman (1963) defines a stigma as “the situation of the individual who is disqualified from full social acceptance” (p. 3). Goffman argued that victims are concerned with others’ perceptions of them and may feel guilty if they cannot comply with social norms. Subsequent exploration of the stigmatization of marginalized groups revealed significant impacts on the LGBT community (Schmidt et al., 2011), individuals in wheelchairs (Cahill & Eggleston, 1995), and the physically disabled (Barg et al., 2010).
The additional academic inquiry has explored economic and social development in different countries, arguing that more developed countries are less likely to stigmatize mental illness than undeveloped countries (Lauber & Rossler, 2007). As a result, more research has begun within the Asian context to explore different degrees of stigmatization. For example, empirical investigations in China (Sun et al., 2013), Japan (Yamada et al., 2001), India (Zieger et al., 2016), Malaysia (Hanafiah & Bortel, 2015), and Vietnam (Ta et al., 2016) indicates a substantial degree of stigmatization.
The importance of stigmatization due to a lack of depression literacy is integral to help-seeking behavior (Coles et al., 2016; Deen & Bridges, 2011; Dias et al., 2018). Many studies (Gabriel & Violato, 2010) suggest that negative attitudes influence treatment choice. Stigma can also lead to discrimination (Corrigan, 2004) which is a tremendous challenge and a significant contributor to a negative quality of life (Choo et al., 2019; Tran et al., 2019). Overall, the impact of stigma in the Asian context is significant (Zhang et al., 2020). This impact is particularly relevant to Thailand (Yoelao, 2015). The Thai understanding of one’s attitude toward depression is vital to planning and providing adequate services for the patients (Mingkwanjai et al., 2015). In Thailand, the treatment of mental illness is generally associated with negative imagery, and the patients are seen as dangerous (Jansongsang, 2007). In addition, Thai depression is seen as “the disorder of the crazy, the losers or the weak” (Jandeekrayom, 2003 appeared in Chanapan, 2013, p. 15). This attitude contributes to negative beliefs about the treatment of depression (Ozmen et al., 2005) and hinders help-seeking (Jorm, 2000; Yap et al., 2013). The impact is that only 8.3% of patients with mood disorders seek professional help (Kitiratanapaiboon et al., 2016). However, greater exposure to information about mental health in Thailand, especially from online platforms, contributes to more positive attitudes toward intervention and treatment of mental illness (Pumpayung & Taifapoon, 2018).
Scholars further discuss how depression literacy affects stigmas toward depression. According to Jorm et al. (1997), mental health literacy is “knowledge and beliefs about mental disorders which aid their recognition, management or prevention” (p. 182). Depression, when properly informed, is likely to be associated with proper treatment, more positive beliefs, and low rates of rejection (Mannarini & Boffo, 2014; Mingkwanjai et al., 2015; Ozmen et al., 2005). Mental health literacy relates directly to the stigmatization of mental disorders. Studies (Jeon & Furnham, 2017; Jorm, 2000; Link & Phelan, 2001; Loo et al., 2012) that compared non-Western and Western countries have found that non-Western countries tend to have more stigmatization of mental health issues due to the lower levels of mental health literacy. In Thailand, the level of depression literacy varies according to different studies. Initial research on the role of stigmatization and health explored HIV/AIDS patients. It concluded that people living with HIV/AIDS in Thailand had experienced HIV-related stigmas, lack of social support, and internalized shame (Li et al., 2009; Ojikutu et al., 2016). It is also essential to be mindful of the Thai perceptions of health and varying approaches to causation and treatment. Within the Thai context, there are both scientific (psychosocial and biological explanations) and supernatural (spirit and karma) beliefs regarding the causes of depression (Chongpanish et al., 2014; Prukkanon et al., 2013). Identifying depression from other disorders also differed in studies of different social groups (Jansongsang, 2007; Namdej et al., 2018; Prukkanon et al., 2013). Pumpayung and Taifapoon (2018) found that more informed participants were more likely to have a positive attitude toward mental health. Nevertheless, a study by Thadanukoonwattana et al. (2016) suggested no significant correlation between depression literacy and stigmatization. As a result, more research has been conducted within Asian countries to explore different degrees of stigmatization, such as in China (Sun et al., 2013), Japan (Yamada et al., 2001), India (Zieger et al., 2016), Malaysia (Hanafiah & Bortel, 2015), and Vietnam (Ta et al., 2016).
There are also discussions regarding the interaction between personal stigma and perceived stigma. Those with and without depression have different perceptions and experiences toward depression (Lewis, 2009) and particularly different beliefs regarding the consequences of depression (Papageorgiou et al., 2015). Thus, attitudes are shaped individually, socially, and culturally (Lauber et al., 2002). Following modified labeling theory (Link et al., 1989), patients who are labeled with mental illness associate and internalize the cultural or societal concept of a “mentally ill person” (p. 402). As a result, they often expect rejection and respond to it in a self-defeating manner. This response indicates that the perceived stigmas and personal stigmas interact. A personal stigma reflects one’s attitude towards those with depression whereas a perceived stigma refers to one’s beliefs about the attitudes of others (Griffiths et al., 2004). Evidence suggests that the personal stigma is more common among men and the less educated (Crisp et al., 2005; Griffiths et al., 2008). Research further indicates that a lower degree of exposure to or knowledge of depression is correlated with a higher personal stigma (Grant et al., 2016; Griffiths et al., 2004; Pyne et al., 2004). The data on perceived stigma is not as consistent (Griffiths et al., 2008) as some research indicates women have a greater level of perceived stigma (Calear et al., 2011) while other studies found no association between gender and perceived stigma (Pyne et al., 2004). Pedersen and Paves (2014) found that people were more focused on perceived public stigmas than personal stigmas. Their results indicate a higher personal acceptance of mental health than perceived social acceptance.
In Thailand, a similar study reported that participants did not stigmatize people with mental illness and had more mental health knowledge than the rest of Thai society (Pitakchinnapong & Rhein, 2019). The current study aims to contribute to the field by identifying and analyzing depression literacy as it relates to Thai stigmas of depressive disorders. The research hypothesizes that higher levels of depression literacy will be related to more positive personal stigmas and more negative perceived stigmas toward depression. The data from this research is important to public health officials, mental health practitioners, and the general public as poor MHL and depression literacy influences help-seeking, stigmatization, treatment choice, and treatment compliance (Angermeyer & Dietrich, 2006; Lauber et al., 2003; Rüsch et al., 2011).
Theoretical Framework
Modified labeling theory (Link et al., 1989) suggests that mental health patients internalize social or cultural concepts of mental illness. The labeled then expect social rejection and responds self-defeating. This theory is based on symbolic interactionism, which argues that others construct the self through interaction (Moses, 2009). In this study, the focus is on the interaction between the social concept of mental illness and individuals. The social concept can be expressed in the form of depression literacy. At the same time, the stigmas from this study can reflect the self (personal stigma) and how individuals expect society to react to depression (perceived stigma) as discussed in Jorm et al. (1997) and Griffiths et al. (2004). Several studies implementing labeling theory within the Thai context (Anders et al., 2003) indicate that it is common to find individuals with mental illness being “othered.” Given the importance of MHL in regard to depression, the potential impact of stigmatization, and the increasing prevalence of mood disorders, this study attempts to address the paucity of empirical inquiry regarding depression literacy in Thailand.
Method
Instrument
This study employed a mix-method cross-sectional survey. An online self-administered survey created using Google Form was distributed to collect data. The two questionnaires developed by Griffiths et al. (2004) were implemented. The questionnaires were translated to Thai using forward-backward translation. The results were analyzed by correlational and descriptive analysis. The qualitative data was acquired by providing space for the participants to add their comments at the end of the survey. The questionnaire was divided into four parts. The first part was the Depression Literacy Questionnaire (n.d.) or D-Lit to measure individual depression knowledge. This was developed by Griffiths et al. (2004). The researcher contacted Kathleen Griffiths via email and asked for consent to use this survey following the translation from English to Thai. It was agreed upon the Thai version would be made available to the public following the completion of this research. The questionnaire contains 22 items about the signs and symptoms and the treatments of depression. The participants were asked to answer “true,” “false,” and “do not know” to each statement. However, the choice was limited to “True” and “False” in this study. One question from the original version, “Not stepping on cracks in the footpath may be a sign of depression,” was omitted as it was not culturally applicable within the Thai context (Table 1).
The Translation of Depression Literacy Questionnaire From English to Thai.

Source. Depression Literacy Questionnaire (n.d.) or D-Lit.
Additionally, the Depression Stigma Scale (n.d.) was used to access the participants’ stigmas. This scale was developed and used in a study by Griffiths et al. (2004). It measured the extent of the stigmas attached to depression in terms of personal stigma and perceived stigma, with nine items for each (18 items in total). A Likert scale of 0 to 4 was used, where 0 means strongly disagree and four means strongly agree. Question 1 focused on personal control of depression. Questions 2 and 3 related to weak-not-sick stigma. Question 4 was on dangerousness, 5 was about avoidance, question 6 was on unpredictability, and question 7 was on concealment or shame. Lastly, questions 8 and 9 were about discrimination against people with depression (Griffiths et al., 2004). The questionnaires were selected for the study as the developer had included the two aspects of stigma (personal stigma and perceived stigma) which aligned with the theoretical framework employed in this study. Moreover, the reliability of the stigma scales by Cronbach’s values was .76 for the personal stigma scale and .82 for the perceived stigma scale (Griffiths et al., 2004). As for the translated stigma scale, the Cronbach’s α values were .713 and .759, respectively (Table 2).
The Translation of the Depression Stigma Scale From English to Thai.
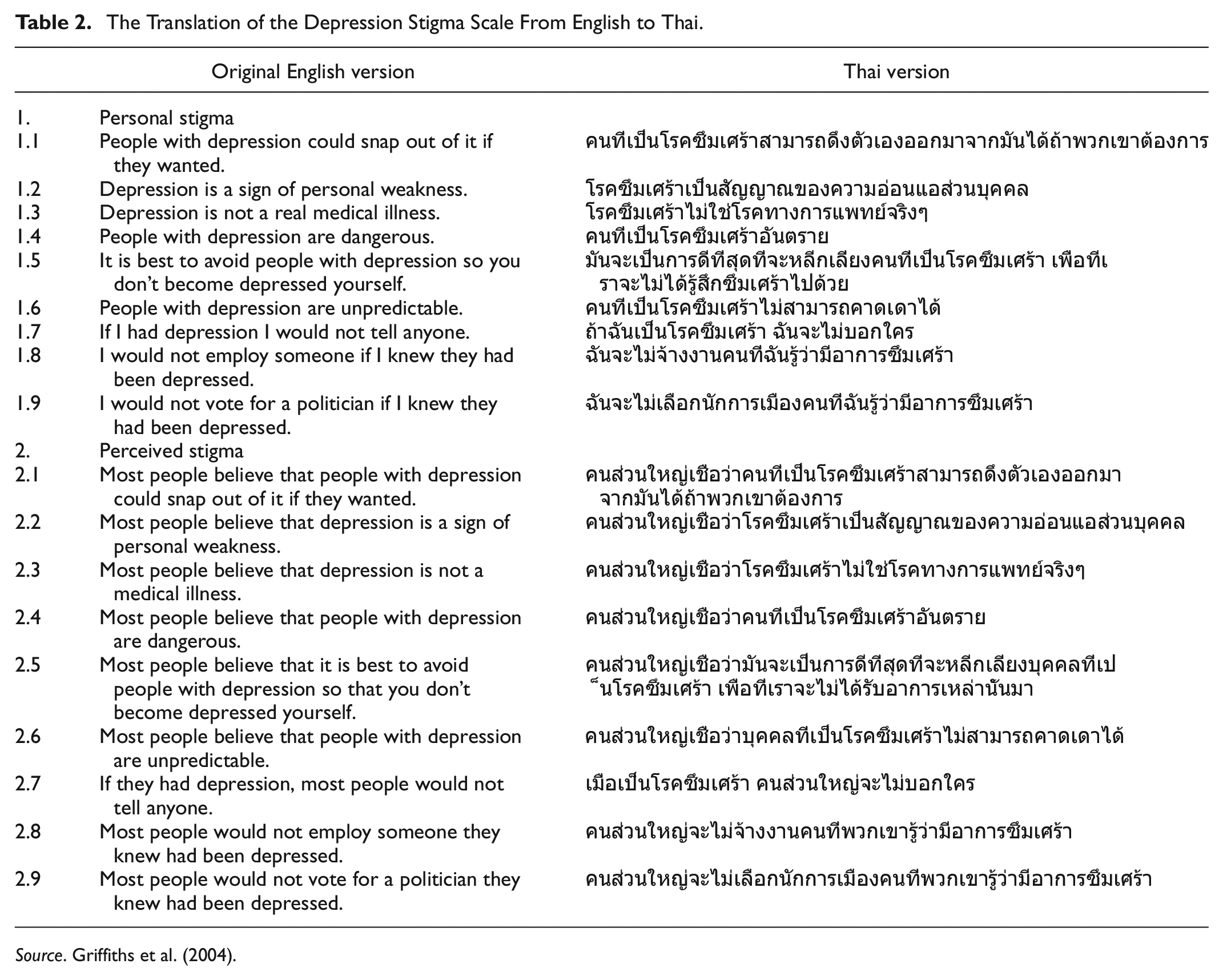
Source. Griffiths et al. (2004).
Sample
A combination of snowball and convenience sampling via online platforms such as LINE messenger application and Facebook were used to distribute the surveys. Questions regarding participant age, sex, province of origin, occupation, education level, religion, and experience with people with depression were asked. The survey also provided a section where the participants could voluntarily comment on or add their opinions about depression. This unstructured qualitative section aimed to explore the participants’ opinion on depression that may not be available from the questionnaires. The inclusion of qualitative data was necessary as the questionnaire may not cover some cultural aspects of depression in Thailand. The qualitative data was thematically analyzed.
Analysis
The statistical analysis was conducted with SPSS. Depression literacy, personal stigma, perceived stigma, age, and educational level were analyzed to assess potential relationships using Spearman’s correlation. The Kruskal Wallis test was utilized to analyze the effect of demographic factors (occupation, religion, and experiences with people with depression) on the depression literacy scores, personal stigma, and perceived stigma. The Mann-Whitney U test was used to analyze the effect of location and remoteness on the depression literacy scores, personal stigma, and perceived stigma.
Ethics
An IRB certificate was granted for this research, which included informed consent and briefings provided to participants at the beginning of the survey. The participants were informed about their rights to withdraw to prevent any discomfort that may have occurred during the participation. In addition, the participants were asked to retain anonymity by avoiding any personal references. The surveys from participants under the age of 18 were excluded from the final results to protect their rights and the participants that did not complete the demographic questionnaire. The participants were also informed of the channel to contact the researcher if any concerns regarding the survey.
Results
Descriptive Results
There were 927 returned responses, and 914 responses were valid (98.6%). The survey found that the participants’ age (excluding minors under 18) ranged from 18 to 77. The mean age was 39.62, and the median age was 39. There were 554 female participants (60.6%), 343 male participants (37.5%), and 17 participants who did not want to specify their sex (1.9%). The participants were from various parts of Thailand; 421 participants (46.1%) were from Bangkok. Most of the participants were Buddhist (91.6%). In addition, 580 respondents indicated that they had known people with depression (63.5%), 215 respondents said they had not (23.5%), and 119 chose “Not sure” (13.0%).
Depression Literacy
The survey results of depression literacy was 14.47 out of 21 or 68.90%, ranged from 6 to 21. The individual items in the Depression Literacy Scale reveal the areas in which the respondents have a high level of understanding of depression and areas which they misunderstood aspects of depression. The areas with more than 80% correct responses are from questions 2, 4, 10, 14, and 17. There are a few misunderstandings about depression regarding identifying people with depression and treatments. Only 35.45% of all participants answered correctly that people with depression do not have several distinct personalities (question 9). On treatments, two questions scored less than 50%, questions 15 and 16. The other questions on treatments are on moderate to a higher level of accuracy (Table 3).
The Results of the Depression Literacy Questionnaire.
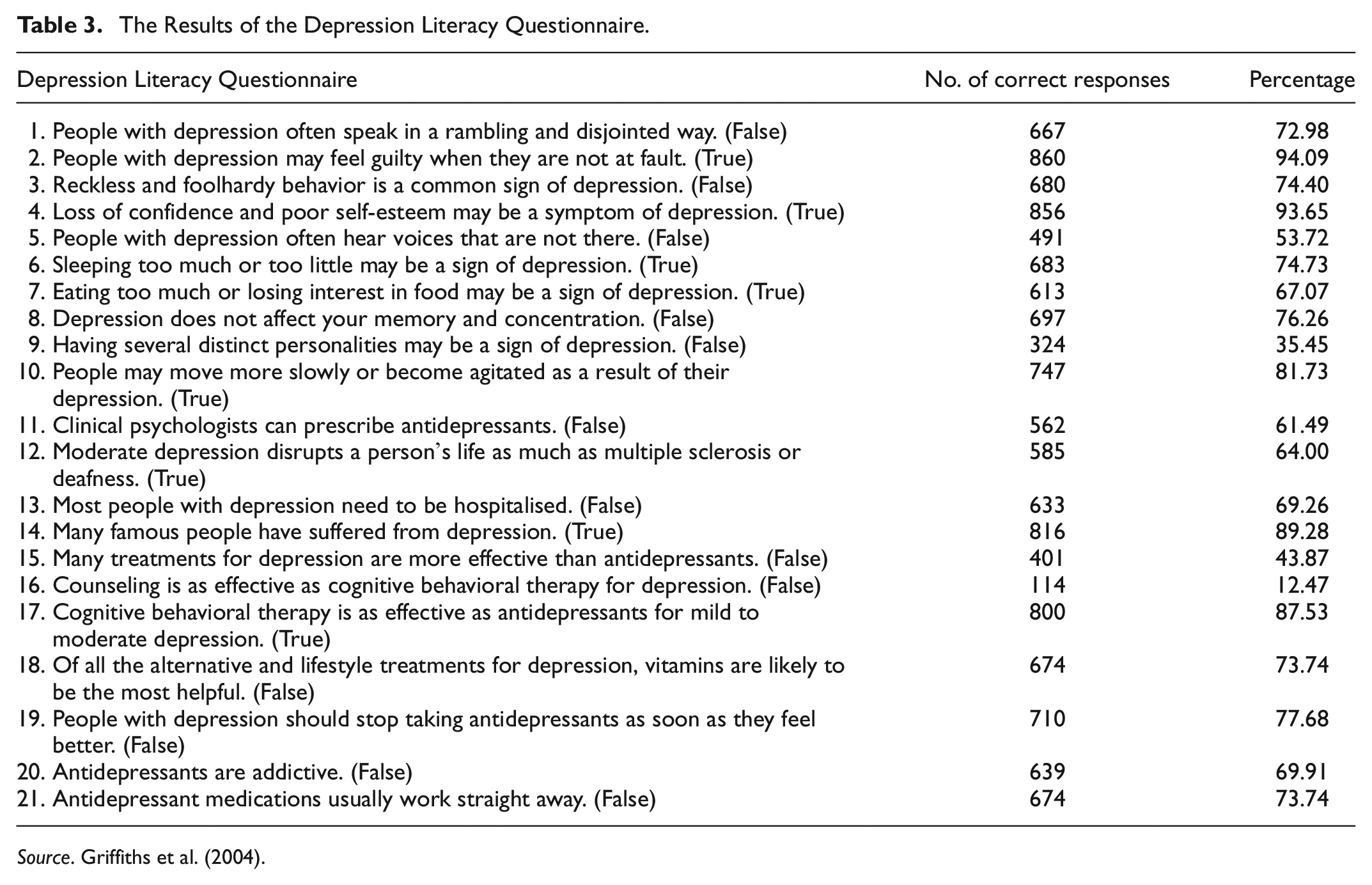
Source. Griffiths et al. (2004).
The Stigmas of Depression
Regarding the personal stigma, lower scores indicate lower depression stigmas. The average total score was 14.79 out of 36 (Table 4).
The Results of the Personal Stigma and Perceived Stigma.

The result of the personal stigma sub-items showed that the items on dangerousness (item 4), unpredictability (item 6), and discrimination (item 9) had an elevated mean scores above 2. On the hand, the results of other items are below 2.
The perceived stigma sub-items showed elevated scores compared to the personal stigma scores. Only items on medical illness (item 3) and avoidance (item 5) had an average score lower than 2. A Spearman’s correlation shows a significant correlation between total personal stigma and perceived stigma with a correlation coefficient of .285, p < .01. This suggests that a higher negative personal stigma toward depression may relate to a higher negative perceived stigma. When the data is statistically tested for the items’ pair, significant positive relationship (p < .01) were found except for item 7 (concealment and shame) (Table 5).
The Correlation Within Personal Stigma and Perceived Stigma Sub-Items.

Correlations Between Depression Literacy and Stigmas
To answer the sub-questions in this study, the correlations between depression literacy and stigmas were analyzed. As a result, the hypothesis on the relationship between depression literacy and personal stigma was confirmed. However, the results did not confirm the second hypothesis regarding the relationship between depression literacy and perceived stigmas.
Subquestion 1: How do different levels of depression literacy relate to personal stigma?
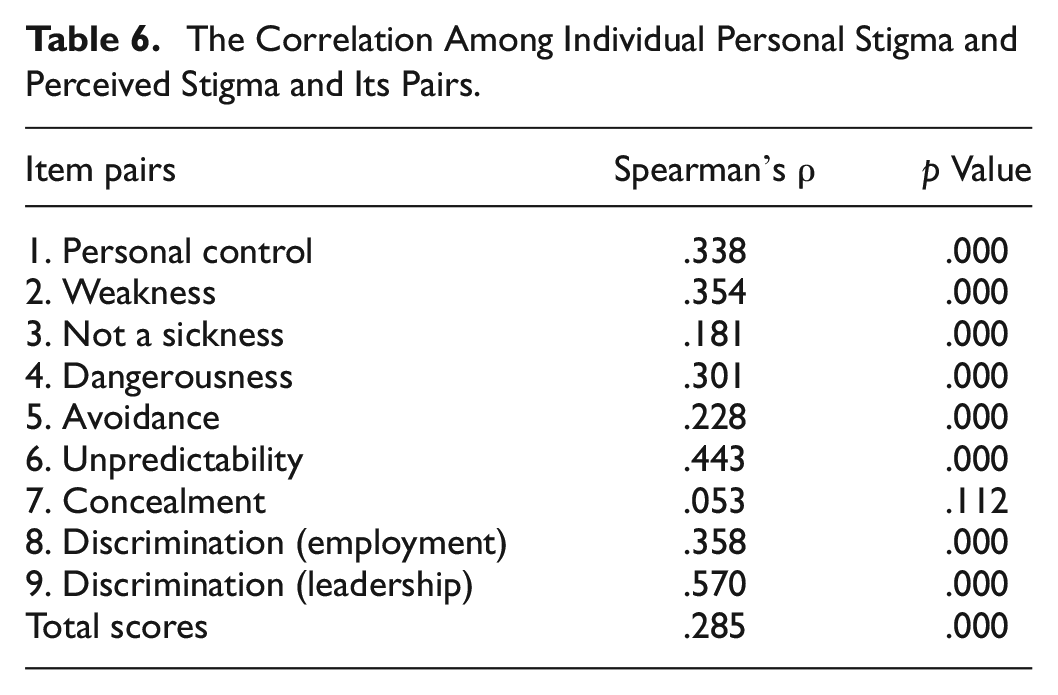
This sub-question was followed by the hypothesis that higher levels of depression literacy would relate to more positive personal stigmas. The findings confirm that depression literacy and personal stigma correlate with (−.535, p < .001). This correlation suggests that the higher the depression literacy, the more positive personal stigma (lower score on the personal stigma) toward depression. The correlation between depression literacy and personal stigma sub-items found a significant negative correlation for all items (p < .001) except for item 7 (concealment and shame, p = .325) (Table 6).
The Correlation Among Individual Personal Stigma and Perceived Stigma and Its Pairs.
Subquestion 2: How do different levels of depression literacy relate to perceived stigma?
This sub-question is followed by the hypothesis suggesting that higher levels of depression literacy would be related to a more negative perceived stigma toward depression. The findings indicate no significant correlation between the level of depression literacy and perceived stigma (rs = −.012, p = .707). However, there was a significant correlation between depression literacy scores with the sub-items related to dangerousness (item 4), avoidance (item 5), and unpredictability (item 6), with p-value ≤.001, and discrimination (8 and 9) with p-value <.05 (Table 7).
The Correlation Between Depression Literacy Scores and Stigma Scores.

Demographic Factors
Age
A Spearman’s correlation was conducted on age and the three main factors. There was a significant correlation between age and depression literacy scores (rs = −.164, p < .001) and personal stigma (rs = .268, p < .001). On the other hand, there was no significant correlation between age and perceived stigma (rs = −.052, p = .116) (Table 8).
The Correlation Between Age and the Stigmas.
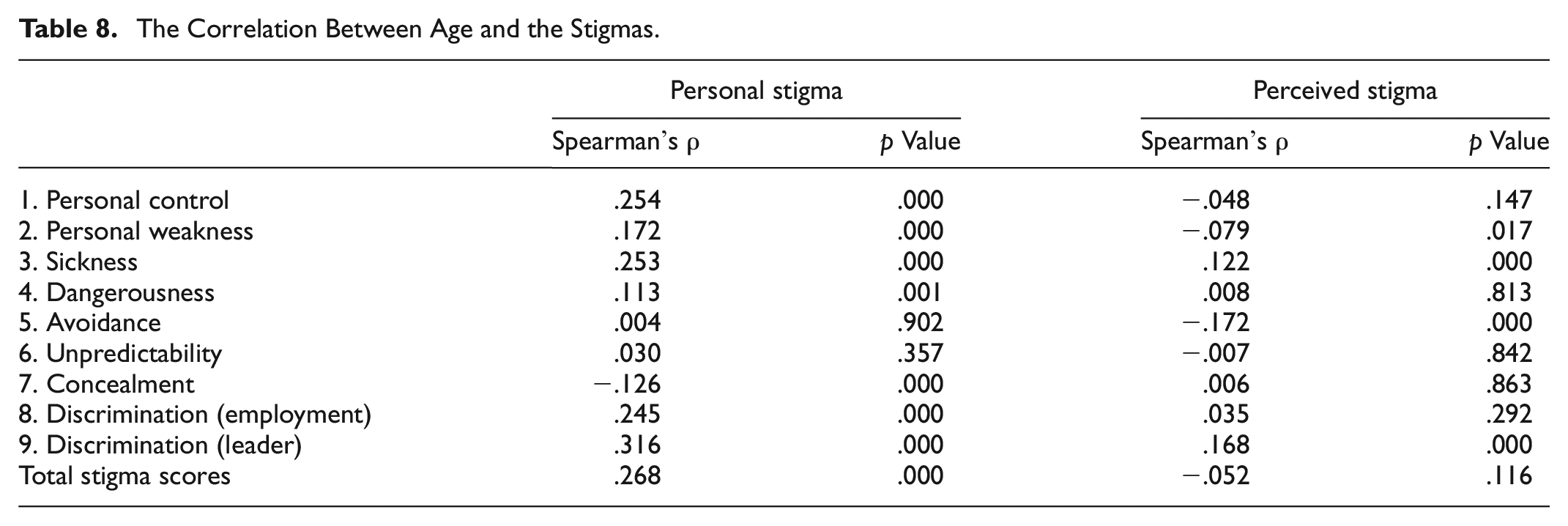
The Spearman’s correlation analysis was also used to analyze age and individual sub-item for each stigma scale. The result indicated a significant correlation between age and personal stigma sub-items on personal control (rs = .254), weak-not-sick (rs = .172 and rs = .253) dangerousness (rs = .113), concealment (rs = −.126), and discrimination (rs = .245 and rs = .316) items, p ≤ .01. However, there was no significant correlation between avoidance (rs = .001, p = .902) and unpredictability (rs = .030, p = .357).
As for correlation between age and perceived stigma sub-items, significant correlation was found with weak-not-sick item 2 (rs = −.079, p-value = .017) and item 3 (rs = −.122, p-value <.001), avoidance (rs = −.172, p < .001), and item 9 on discrimination (rs = .168, p < .001).
Sex
From a statistical test using Kruskal-Wallis test, the effect of sex and the level of depression literature was H(2) = 26.194, p = .000. On average, male respondents score lower than the other 2 groups (µ = 13.86, Mdn = 14). On the other hand, female and not-specify respondents score similarly on depression literacy (Female: µ = 14.86, Mdn = 15; Not-specify: µ = 15, Mdn = 15).
The effect of sexes on personal stigma was also statistically significant, H(2) = 19.333, p = .000. The sub-items that found a statistical significance were item 1 (personal control), item 2 (personal weakness), item 8 and 9 (discrimination). The statistical significance were H(2) = 18.199, 24.564, 8.565, and 10.676 respectively, p-value <.05. The median scores of male respondents for all items are generally higher than the other two groups, except item 8 where median scores were the same for all groups. However, when the mean scores was investigated for item 8, the findings were that the male (µ = 1.52) and not-specify (µ = 1.53) respondents scored higher than the female (µ = 1.25) respondents.
However, there is no effect of sexes on perceived stigma, H(2) = 1.729, p = .421. Similar results were found for sub-items of the perceived stigma scale except for the item 1 on personal control. The statistical test indicated an effect of sex on the personal control, H(2) = 7.427, p = .024. The median scores for male was 3 and for female and not-specify groups were 2.
Location and remoteness
The group was divided into the respondents who live in Bangkok and the respondentswho live outside of Bangkok. The data had eight missingvalues (0.9%) where the respondents answered two or more locations, not identify a location. By using Mann-Whitney test, the result indicated the non-significant difference between the location of the sample (living in Bangkok or outside of Bangkok) and depression literacy and personal stigma. However, there was a statisticaldifference between the location and perceived stigma,U(Living in Bangkok=421,Living outside of Bangkok = 485) = 94,199.5, z = −2.011, p = .044. The respondents living in Bangkok (Mdn = 22) scored lower in perceived stigma than those outside Bangkok (Mdn = 23).
Occupation
A Kruskal-Wallis test showed that occupation significantly affects depression literacy score, H(6) = 13.243, p = .039. The occupation that scored the highest on depression literacy was the education provider and health service provider (Mdn = 16.50), and the lowest score was from the retired respondents (Mdn = 13) (Table 9).
The Average Median Scores for Different Occupations and the Factors.

The statistical test also showed that occupation significantly affects personal stigma, H(6) = 29.655, p = .000. The occupation with the highest personal stigma level was from the retired respondents (Mdn = 17), and the lowest was from a health service provider (Mdn = 8.50). However, there was no significant effect of occupation on perceived stigma, H(6) = 4.272, p = .640.
Education level
Spearman’s correlation shows a significant relationship between education level and depression literacy (rs = .117, p = .00). However, the result did not indicate significant relationship between the level of education and stigma scores (rs = −.001 and rs = −.004, p > .05). A Kruskal Wallis test was conducted for the effect of education on the factors. It indicated a significant effect of education level on depression literacy, H(7) = 25.116, p = .001). However, there was no significant effect of education level on personal and perceived stigma levels.
Religion
A Kruskal Wallis test was conducted for the effect of religion and the variables and the results showed a significant effect of religion on all the variables. For depression literacy, there was a significant difference among different religions, H(4) = 18.625, p = .001. The highest score for depression literacy was from atheist respondents (Mdn = 17), and the lowest was from Buddhist and Muslim respondents (Mdn = 14) (Table 10).
The Median Scores for Different Religions and the Factors (New Table).

For the effect of religion on personal stigma score, the test result was H(4) = 16.652, p = .002. The highest personal stigma score was from Buddhist respondents (Mdn = 15), and the lowest was from atheist respondents (Mdn = 10).
The test also suggested a significant effect of religion on perceived stigma. The result was H(4) = 11.837, p = .019. The highest score was from atheist respondents (Mdn = 25.5), and the lowest was from Christian respondents (Mdn = 20).
Experiences with people with depression
A Kruskal Wallis test indicated a significant effect on having an experience with people with depression on the level of depression literacy, personal stigma, and perceived stigma (Table 11).
The Median Scores for Prior Experience With People With Depression and the Factors.

The test result for the effect of experience with people with depression and depression literacy score was H(2) = 74.611, p = .000. The highest score was from people who answered “yes” (Mdn = 15), and the lowest was from people who said “no” (Mdn = 13).
The effect of experience with people with depression on the level of personal stigma was H(2) = 89.823, p = .000. The respondents with no experience scored personal stigma the highest (Mdn = 18), and the lowest score was from people who said: “yes” (Mdn = 13).
The effect of the prior experience on perceived stigma was H(2) = 10.998, p = .004. The highest score was from people who answered “yes” (Mdn = 23), and the lowest was from people who said “not sure” (Mdn = 20).
Qualitative data
Out of 914 responses, there were 117 comments at the end of the survey (excluding the ones that said they had nothing to add) or 12.80%. Comments from the survey were categorized into six themes. The themes were as follows;
Identifying symptoms of depression and depression literacy
Thirty-six responses were categorized into this theme. Most people commented that depression could be treated, but some suggested it cannot be treated entirely. Most respondents suggested that the depressed should be brought to a psychiatrist or psychologist. Some respondents suggested the use of medication and professional treatment. Some acknowledge the risk of suicide. One respondent who talked about rTMS treatment said:
Nowadays, rTMS(repetitive transcranial magnetic stimulation) can be used to treat depression by stimulating the parts of the brain that have problems which are quite effective. It can also reduce side effects from drugs and have a higher chance of recovery than medication. It also allows the patients to live normally without using an anesthetic like electrotherapy.
This may suggest that knowledge of treatment of depression is quite good, and formal help-seeking is also deemed necessary. However, some respondents also demonstrated an inaccurate understanding of depression by including symptoms such as delusions. Moreover, some suggested that consuming vitamins and exercising were valid methods to treat or prevent depression.
Identifying with depression or suspecting that they have depression
Nineteeen participants claimed that they had depression or thought they might have depression. One of the respondents said:
I am diagnosed [with depression] and with bipolar disorder, so I truly know how it feels like to go through all the inevitable symptoms during a depression episode. I’ve been dealing with depression [for] more than two and a half years now, so these questions are most of what I personally experience.
Some people expressed their feelings and how they coped with depression or their depression-like symptoms:
I had depression, but I was lucky to have someone to help me out of it. The reason I had it was because I lost my self-worth, internalized others’ words about myself, and thought that no one understood me.
How should we treat or act toward people with depression
Thirty-two comments were categorized into how people should treat those with depression. Most said that people with depression should be closely taken care of and should not be left alone. Social support and activities should be provided to help them recover from depression:
If there is a patient with depression, they should not be left alone. They should be brought out to hang out, like traveling, eating out, going to the temple to make merit and convince them to talk to their friends. Importantly, they should see a psychiatrist.
Six comments expressed sympathy or empathy for people with depression. These people suggested that those close with people with depression should try to understand and listen to them. One comment said,
People with depression are not dangerous. Do not tell them to fight it; just listening to them is enough. Sometimes they have already been fighting for a long time.
Attitudes toward depression
Sixteen comments show different attitudes toward depression. Some of the comments express negative attitudes. For example, a male participant described people with depression as unpredictable and delusional:
People with depression are hard to predict. Sometimes they look happy, sometimes they look sad. Also, they have the symptom of delusion. Especially women with depression. They will have over-obsessive-like symptoms when they are close to the opposite sex. And when things don’t go their way, they will behave negatively to men.
Some of the comments mentioned self-help, personal responsibility to overcome depression, or changing oneself to cope with depression. Three out of six male participants who identify with depression referred to self-help methods to recover and did not mention professional treatment. One respondent who identified as having depression mentioned self-training and self-acceptance to cope with depression:
I have depression. I feel better when I try training myself by not listening to other people’s insults. But those symptoms are like a cycle, getting better, then feeling down again. But by training ourselves is a way to deal with it, like it is our friend and we have to accept ourselves. Believing in and encouraging ourselves is the most important.
Four responses mentioned religious beliefs and practices in treating depression, referring to Buddhism. All of the respondents are female. One thoroughly explained how to integrate Buddhism into one’s life in order to treat depression:
We already have the wisest teacher in the world, which is the Lord Buddha. […] To train our mindfulness is very important because it will calm us and help us in finding ways to solve life problems. When we face a crisis, it will help us to find the way out, and continue our lives, and rely on ourselves. […] The foreigner’s psychological theories on counseling […] have both advantages and disadvantages. But the Lord Buddha’s theory only has advantages, no disadvantages. […] For people with depression, just seeing a psychiatrist and taking drugs is not enough. They have to exercise, have friends and take care of themselves in a Buddhist way. Like this, they can become friends with themselves, and they can solve the problem sustainably. In the age of information, if we do not meditate and contemplate our lives, we cannot differentiate what is appropriate because we lack the wisdom to do this and cannot catch up with the flood of information. Praying, practicing the dhamma, meditation, and making merit is very important. Thai people should integrate these practices into their daily lives so it can reduce their inner greed, anger, and obsession. So they can understand self-efficiency and self-help for themselves, their family, and the country.
Other comments also recognized both religious and psychological approaches to treating depression:
I used to work as a volunteer on self-development with Buddhist methods. I have met with children who were likely to have depression. Most of them are affected by their family background, parental care, environment, and their own mindset. Although depression is medically diagnosed as an abnormality of the chemicals in the brain and the patients have to be treated medically, Buddhism can also treat this disorder by using dhamma to heal their minds to reduce the symptoms or recover. I would like to suggest this as an alternative for future study that in what way Buddhism can cure depression.
Interest in knowing more about depression knowledge
Fourteen comments expressed a personal interest in knowing more about depression and calling for more publications about depression knowledge, such as how to deal with people with depression within the Thai context:
There should be serious studies on this disorder in order to find treatment guidelines and proper future interventions. I believe that in the future, there will be a lot more patients with this disorder, caused by factors like livelihood, society and the change in the environment, or even changing lifestyles. All these can lead to depression.
Others
Thirty comments were categorized as miscellaneous. Some mentioned their acknowledgment of the prevalence of depression. Fourteen comments gave suggestions regarding the direction of the research. A few of these questioned the items on dangerousness, whether it was directed to people around them or the patients themselves. One of the comments said:
In the dangerousness question, it should be specified or defined whether it is dangerous to other people or people who have depression. I answered it in the way that it is dangerous for the patient themselves.
Some of them suggested that the questions in the depression literacy questionnaire are too specific and need specialized knowledge to answer. Some suggested it would be helpful to include the answers to the depression literacy questionnaire.
Discussion and Recommendations
The survey implemented in this study indicates that depression literacy in Thailand is at a moderate to a higher level. The personal stigma was lower to moderate, while the perceived stigma was high to moderate. The individual items on the Depression Literacy Scale showed some areas in identifying depression (questions 1–10) that many people still ?misunderstand, particularly regarding the presence of hallucinations and several distinct personalities. Given that these are symptoms of schizophrenia and dissociative identity disorder, respectively, this may indicate that some Thais may find distinguishing various method health conditions difficult, as reflected in Prukkanon et al. (2013) when they reported that 72% of participants still associate mental health with mentally ill persons (literal translation as “crazy person” in Thai). This may help to understand that although Thais may be better at identifying mental health and mental illness, they may still merge different illnesses. This is exemplified by the work of Namdej et al. (2018) on Thai high school students, which found that 65% of the students could identify depression correctly. 87.90% could identify anxiety disorders. They suggested that anxiety disorders have more evident signs and symptoms and are easier to identify than depression. This may explain why the respondents scored lower for depression. The participants attributed these depressive symptoms to normal stress and avoided seeing a psychiatrist due to personal shame and potential social stigma (Namdej et al., 2018). This is further reflected by one of the comments in this study which expressed confusion between depression and stress.
The other half of the questionnaire regarding knowledge of treatments for depression revealed that two areas scored lower than the other questions. Almost half of the population perceived that other types of treatment are more effective than anti-depressants. However, there is no specification on which treatment they referred to. Moreover, most respondents think that counseling is as effective as cognitive-behavioral therapy. Although many people acknowledge the need to bring those who exhibit signs and symptoms to seek professional treatment, some with depression tend to refer to self-help or counseling from friends as a way to treat their symptoms. This may be the result of the stigma common to formal help-seeking. This aligns with Prukkanon et al. (2013), who found that mental health is associated with hospital visitation. The study by Barney et al. (2009) also found that some participants fear the stigma attached to seeking formal help from other people and are reluctant to receive treatment. However, this requires further research as this survey does not directly measure the stigmatization of treatment.
The stigma of dangerousness is in line with Jansongsang (2007), which suggests that people see patients with depression as dangerous. Another study in Australia also found the notion of dangerousness when depression is associated with mental illness (Barney et al., 2009). This result contradicts studies outside of Thailand, whereby depression is not seen as dangerous as other mental disorders such as schizophrenia (Seidman, 2014). This may be linked to a lack of knowledge and confusion in identifying different disorders, especially stress-related disorders and schizophrenia.
In terms of the weak-not-sick stigma, this research has confirmed the results of a previous study by Pumpayung and Taifapoon (2018), which indicated that Thai people perceived problems with health as due to neurological dysfunction, trauma, and the environment. A moderate correlation between personal control, personal weakness, and perception as a medical illness indicate relationships between these stigmas and how these stigmas may influence one another. However, it may be possible that Thais recognize depression as a disorder while also expecting the people with depression to overcome it. A study by Barney et al. (2009) also found a similar association between depression and personal responsibility in Australia. The study also found that the people with depression also fear being stigmatized as weak if they disclose their condition to other people adding that they will be treated differently or “being seen in a lesser way” (p. 11). Furthermore, this study’s frequent reference to self-help may also reflect expectations of personal control over depression. This specific stigma may be related to obstacles in terms of help-seeking behavior and self-help behaviors.
In terms of discrimination, there is a slightly elevated negative stigma that people with depression may not be capable as a leader, while discrimination as an employee is lower. This may be linked to a stigma of weakness that is expected to be absent from a leader. The result from the current study indicated a correlation between weakness, unpredictability, and discrimination items. This may imply that some of these harmful stigmas, such as weakness and unpredictability, affect discrimination against people with depression as it may not fulfill the image of an ideal employee or leader. A study by Chongpanish et al. (2014) on postpartum depression and stigmas in Thailand suggests that women who have postpartum depression are deemed to have less ability to make decisions and lower competence than normal people.
A study by Dietrich et al. (2014), which used the same stigma scale in Germany, also found that all groups scored higher in perceived stigma than personal stigma. This propensity for a perceived stigma confirms the study results on the stigmatization of mental illness in Thai university students by Pitakchinnapong and Rhein (2019), which found that the participants had a higher perceived stigma of mental illness while claiming that they did not stigmatize mental illness. The study also suggests that the participants may be exhibiting a bias blind spot in which they think they are less biased than others (Scopelliti et al., 2015). This may explain why the discrepancy for the disclosure of depression was the widest among the item pairs, exemplifying the idea that they are more open and accepting of depression when they have it than other people in society.
However, another explanation is also offered in a comparative study between Australia and Japan by Griffiths et al. (2006), which suggested that the differences between the two stigmas may partly be due to social desirability bias. The participants avoid expressing their true feelings. The study found that the Australians had a wider score discrepancy between personal and perceived stigma when compared to the Japanese. The author suggested that the sense of social desirability may differ between the two countries. As a result, it may be more socially acceptable to stigmatize mental disorders in Japan, or the Australians were more commonly exposed to de-stigmatization campaigns and were more sensitive to stigmatization. However, this explanation was not conclusive.
Regarding the current study, it may be possible that more exposure to de-stigmatization campaigns may have impacted the level of perceived stigma. According to Pumpayung and Taifapoon (2018), the content surrounding mental health in Thailand received by the netizens was centered on self-development psychology and positive psychology, while the anecdotes and academic literature about people with mental illness and psychiatrists were less commonly consumed. This may suggest that the attempt to de-stigmatize mental illness did not receive enough attention from the public.
Correlation Subquestions
A strong correlation between depression literacy and personal stigma follows previous studies (Busby Grant et al., 2015; Griffiths et al., 2008). This may suggest that de-stigmatizing depression at a personal level may be done by raising awareness and developing a correct understanding of depression. This result is similar to findings outside Thailand (Mannarini & Boffo, 2014; Ozmen et al., 2005), as well as the local findings by Pumpayung and Taifapoon (2018), which concluded that the participants who are more informed about mental health are more likely to have more positive attitudes about mental health. Another study from Thailand by Mingkwanjai et al. (2015) also found that improvement in depression literacy can improve acceptance, attitudes, and positive stigma toward depression.
The perceived stigma is associated with the willingness to accept treatment and the continuation of treatment (Barney et al., 2009; Griffiths et al., 2014; Sirey et al., 2001). Therefore, there is a need to find a strategy to de-stigmatize perceived stigma to create an effective intervention for depression (Griffiths et al., 2014). The current study examines whether depression literacy is related to reducing perceived stigma. However, this study found no relationship between depression literacy and perceived stigma. This may suggest that even if depression literacy has increased, the perceptions of the public stigma may not be influenced, as reported by Griffiths et al. (2014).
In addition, the current study found that age has little relationship with depression literacy and perceived stigma. The results suggest that Thais have a fairly distributed understanding of depression throughout the age groups. This differs from research outside Thailand which concluded that adolescents held a higher level of negative personal stigma (Calear et al., 2011; Dietrich et al., 2014; Eisenberg et al., 2009).
Although most of the perceived stigma items scored higher than personal stigma items in all age groups, there are some items that the older generation scored higher in the perceived stigma. Moreover, the gaps between personal and perceived stigma were more likely to be narrower in the older generations and decreased with age. This may have two possible explanations. One is that bias blind spots may occur in the younger generation, and the older generation tends to internalize the perceived stigma or see the world more realistically. The other possibility is that this may be how the younger generation interacts with the older generation, such as their family, and perceives the personal stigma of the older generation as the perceived stigma. According to Pitakchinnapong and Rhein (2019), most university students are reluctant to discuss mental illness with their family members or older generations in Thailand. The participants claimed that the older generation viewed mental illness negatively and was less informed about the matter. Although the current study indicates that the older generation tends to have a higher level of stigma, misperception of a lower level of depression literacy was not true as depression literacy level was fairly distributed throughout all the age groups. This may indicate a misperception about depression across generations, and this differing perception creates obstacles to open discussions among different age groups. It is essential to acknowledge this information to design an effective depression intervention.
The current study further indicates that men tend to have lower levels of depression literacy when compared to women and the other group. Moreover, the men in this study tend to have greater personal stigmas and perceived stigmas. This is similar to the findings by Jorm and Wright (2008) in Australia. Other studies in Thailand indicate similar results in terms of sex, depression literacy, and personal stigma (Namdej et al., 2018; Pumpayung, 2016). Other studies also received the same result regarding sex and personal stigma (Dietrich et al., 2014; Eisenberg et al., 2009; Griffiths et al., 2008). The study also found that depression is attributed negatively to females, as expressed in the comments. This suggests that some men misunderstand depression.
For example, unpredictability was indicated as a symptom of depression, which, according to Pluempitichaikul (2019), women are commonly stereotyped as weak, emotional, and unpredictable in the media. According to Rungreangkulkij (2017), men tend to associate depression with helplessness and weakness, both characteristics which do not conform to traditional masculine gender norms. Instead of identifying it as depression, they avoid using the term and use “feeling stressed” to explain symptoms (p. 159). The results from the current study also indicated that, on average, male personal and perceived stigma is higher than in other groups. This may imply that men tend to have a stigma that depression is associated with weakness, both in personal and perceived stigma. As a result, if they feel depressed, they may internalize these feelings. According to a study by Seidler et al. (2016), most of the research found that depressive symptoms went against masculine norms such as success, feelings of control, strength, and stoicism. Conforming to these masculine norms may hinder help-seeking and result in maladaptive coping strategies. The qualitative data from the current study also indicate that males are more likely to employ self-help than females who identified with depression. A study in Canada by Johnson et al. (2011) found that although many had attempted to seek professional help, most men who were not formally diagnosed with depression relied on informal support and self-help. The study also suggested that one of the patterns employed by their participants was “manly self-reliance,” which involved perceptions that depression could be handled by themselves as it was a minor personal problem (p. 350). Combined with the results from the current study, it may indicate a certain pattern among men with depression that these symptoms can be dealt with independently.
Regarding education level, the current study found that depression literacy increases with the level of education. Negative personal stigma also decreases with the level of education, then increases again after a master’s degree. Prukkanon et al. (2013) found that people who did not have a higher education or never completed the undergraduate level tended to have lower mental health literacy. According to Ozmen et al. (2005), higher education is associated with more positive opinions about the treatment of depression. On the other hand, another study in Thailand by Pumpayung (2016) found that undergraduates had more exposure to mental health issues through social media. This may explain the fall and rise of the level of personal stigma in accordance with educational level.
Lastly, the results from the current study indicate that people who have experience with the depressed tend to have a better understanding of depression and have fewer negative personal stigmas. This is evident in sections that compare occupations that interact with people with depression, such as education and healthcare. This aligns with contact theory, as exemplified by a study by Busby Grant et al. (2015), which found that contact with people with depression resulted in lower personal stigma. However, it may not play a significant role in perceived stigma. Similar findings were found in 2008 in a study by Griffiths et al.
Limitations and Future Research Necessary
It should be recognized that this research is the result of a survey that was translated from English to Thai, and there may be some cultural elements that were not mentioned or included in the questionnaires. For example, the influence of religion, especially Buddhism, emphasizes self-help as a coping strategy. In addition, although this study implemented mix-methods, there is a propensity for quantitative data. Therefore, further exploration of Thai depression literacy and stigma toward depression using qualitative methods is called for. Furthermore, future research may also look at depression-related discrimination in Thailand. Additional research is needed in order to understand this aspect of stigmatization. Moreover, future research may further explore the stigmas of various treatments and other factors that influence the decision to seek professional treatment within the Thai context. Finally, qualitative research on perceived stigma toward depression and other mental disorders is needed to fill the gap and help improve the interventions and policies.
Conclusion
This study explored the Thai stigma toward depression and its relationship with depression literacy. The research found that Thai people have moderate levels of depression literacy; however, some cannot identify different disorders. The research also found that the stigma toward depression was a moderate one. Nevertheless, the personal stigma of dangerousness, unpredictability, and discrimination as a leader is higher than others. Perceived stigma was found to be higher than personal stigma. The relationship between higher depression literacy and lower personal stigma was confirmed. On the other hand, depression literacy did not relate to perceived stigma. The research also explores other factors which may be related to these factors. It found that being older, male, identified with faith, having a lower level of education, and having lower contact with people with depression tend to have lower depression literacy and higher negative personal stigma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.