
Abstract
The study investigates the effects of multidisciplinary treatment for rheumatic treatment regarding (a) financial feasibility based on costs/remuneration in comparison to conventional treatment and (b) Patient reported outcome measures (Proms) to check for effectiveness. For (a), cost data and remuneration with and without multimodal rheumatologic complex treatment (MRCT) is analysed, including cost types. The database encompasses 18,794 treatment cases. For (b), a case study with retrospective patient data analysis (N = 375, all treated in a specialized German hospital) regarding self-reported quality of life and physical functions is carried out for subjects receiving MRCT. While conventional treatment is fully covered, MRCT is only incentivized for cases with long in-patient treatment, so financial feasibility for hospitals is limited. Patients with MRCT reported significant improvements in quality of life (p < .001; Nottingham Health Profile) as well as in physical functions (Functional Questionnaire Hannover [FFbH], p < .001) at discharge compared to admission. As short-term MRCT is not fully remunerated, less severe cases may not receive adequate care. Financial incentives should at least cover the costs incentivize the offer and thus ensure patient access to MRCT. Measuring the outcomes of the treatment process by means of Proms can contribute to the internal quality management. It also offers an inter-institutional benchmark to service providers, which can be used as a basis for performing comparative quality measurements and researching effectiveness.
Keywords
Introduction and Background
The World Health Organization (WHO, 1992) defined rheumatic disorders as diseases of the musculoskeletal system, which are almost always associated with pain, and often also with restricted mobility. Pain intensity and psychological comorbidities significantly affect the quality of life of patients with rheumatic disorders and thus should be considered during treatment (Katchamart et al., 2019). Effective, multidisciplinary methods (Borenstein et al., 2017) are advisable especially in more advanced stages of the illness.
Rheumatic diseases are partly age-dependent, so in view of demographic change the number of cases is increasing. This poses challenges to health systems worldwide (OECD, 2018) as care of these patients requires high investments of time and material resources (Tsiachristas, 2016) due to the complexity of their needs. Rheumatic diseases are associated with a variety of ailments and symptoms which are often disregarded in clinical settings (Ishida et al., 2018). This can reduce the effectiveness of the interventions. Thus, multidisciplinary treatment for rheumatic disorders for example combines physical/physiotherapeutic treatment with pain and behavioural therapy options (American College of Rheumatology Pain Management Task Force, 2010; Carbonell-Baeza et al., 2010; Dale & Stacey, 2016; Krause et al., 2006).
However, the costs incurred by multimodal rheumatologic complex treatment (MRCT) are partly unclear. In addition, research is needed to investigate how patients perceive a comprehensive treatment that tries to also cover comorbidities and improve general wellbeing and specific parameters. Moreover, the published evidence on the efficacy of care as specified by multimodal treatment for rheumatic diseases is still limited. In the past, particular emphasis was placed on the structural quality of the complex treatment (Lakomek et al., 2011), procedural aspects, for example connections to treatment pathways (Lakomek et al., 2007), and positive patient reported outcomes when following a defined protocol for specific illnesses or settings (Romeyke et al., 2018). Concerning the latter, a randomized study with 130 patients demonstrated that rheumatological complex treatment reduces pain and depression (Romeyke & Stummer, 2014). A recent study shows significant functional improvement and considerable reduction in disease activity. The characteristics of the course of the disease, such as the duration of the disease, the type and number of previous pharmacological treatments, and the current pharmacological treatment, did not significantly affect the response to MRCT (Klemm et al., 2019).
Nevertheless, the published evidence is still insufficient to answer the questions outlined above. This is because only a small number of subjects was investigated so far, and only limited consideration has been given to structural conditions. Furthermore, the remuneration of service providers, which is indispensable for ensuring adequate structures and processes, has not been adequately considered in scientific investigations so far. However, an adequate payment is indispensable for hospitals to first offer MRCT to patients
Thus, this paper analyses the case of rheumatic disorders and studies a specialised hospital in Germany (Waldhausklinik, Deuringen) that offers multimodal treatment. The focus of the investigation are the effects of integrating evidence-based multidisciplinary treatment approaches for rheumatic diseases on the hospital level regarding (a) financial feasibility based on costs/remuneration in comparison to conventional treatment and (b) Patient reported outcomes. The aims of the study can be summarized as follows: to Investigate a multimodal therapy program from the patient’s point of view as well as a health economic evaluation in comparison to a conventional therapy.
In combination, this will aid to determine the value of multimodal treatment for rheumatic disorders from a health system perspective.
Rheumatic Diseases: Treatment Options in Germany
In Germany, patients with advanced rheumatic diseases have access to multidisciplinary team care and treatment (MRCT) (Stoffer et al., 2014), but only in case outpatient therapy options are exhausted or immediate action is required due to the severity of the disease. Acutely exacerbated multilocular pain, progressive impairment of quality of life, long-term pain, and increasing drug consumption also support opting for a multimodal approach.
Multidisciplinary treatment for rheumatic disorders is officially classified as multimodal rheumatologic complex treatment (MRCT) in the German procedure classification (OPS) as OPS number 8-983 and provided by specialized hospitals. Hospitals offering MRCT must fulfil defined requirements for structures and processes, and quality measurement by means of patient-related outcomes is mandatory. The goal is to provide quality-oriented and efficient services that minimize risks and focus on patient needs as conventional or monomodal treatments are often not sufficient for chronic rheumatic diseases (Modic et al., 2005).
Interdisciplinary diagnostics is used to develop a treatment plan for an interdisciplinary team. Pharmacological and non-pharmacological interventions need to be carefully selected based on the individual patient profile, integrating psychological interventions, physical training, patient education, and complementary procedures (Cunningham & Kashikar-Zuck, 2013). At least three of the following therapeutic areas must be used: physiotherapy/physical therapy, occupational therapy, pain therapy, cognitive behavioural therapy, psychotherapy. The therapy must be patient-focused, start immediately, and therapy density must reach at least 11 hours per week. Disease activity, the functional impairment, and the extent of pain must be assessed at the beginning and end of hospitalization. Applicable scales are defined: The Disease activity score 28 (DAS 28), Functional Questionnaire Hannover, Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) or Bath Ankylosing Spondylitis Functional Index (BASFI) are used for possible diagnosing tools for disease severity. To assess pain intensity, the numeric rating scale/visual analogue scale (NRS/VAS) is used.
Patient Reported Outcomes Measures (Proms) as Quality Indicators
Patients typically have a more comprehensive view of their conditions than single professions treating them, and focus not only on disease activity, but also on physical functionality and quality of life (Taylor et al., 2016). Having patients monitor their condition and assess their symptoms not only empowers them, but also contributes to shared decision making and can help the treatment team develop a personalized therapy plan (Boyce et al., 2014). To assess the success of a therapy, factors such as pain intensity, quality of life, physical functionality, mental well-being, etc. can be assessed from the patient’s point of view (Donath et al., 2015). The results can be seen as outcomes that reflect patient satisfaction with the received treatment (Willke et al., 2004) and give valuable insight into quality improvement potentials as they can reflect service quality, effectiveness, adequacy, and quality of treatment (Appleby & Devlin, 2005). Collecting Proms using standardized questionnaires can therefore be used to control symptoms (Fautrel et al., 2018; Graupner et al., 2021) in the inpatient setting to improve patient outcomes when implementing multimodal programs. Standardized Proms are validated to ensure that changes in the results are identifiable and become more and more utilized in the field of rheumatology (Fautrel et al., 2018).
Despite the many benefits of using Proms, it is challenging to implement these tools in routine care (Jagpal et al., 2019). There may be, for example, patient-related problems, such as linguistic barriers, psychological stress, or issues with the use of modern information and communication tools (Hirsh, 2016) in case these are employed. Processing the results may also be difficult for physicians (Jagpal et al., 2019). A focus on overall quality is helpful (not only) in these cases, plus can have a positive effect on Proms. This is because especially structural conditions affect the process of service provision, which in turn may influence treatment outcomes (Donabedian, 1988b).
The processes and structures necessary to provide complex treatments and to integrate the collection of Proms can have a very positive effect on quality and outcomes but come at a price.
Incentivising Quality in Care
Figure 1a and b depict main elements of structural, procedural and outcome related quality (Donabedian, 1988a) that must be compensated for when remunerating hospitals for applying MRCT. Quality of structure covers all organizational framework conditions, such as structure and work-flow management, or professional. Process quality focuses on the core processes of service provision, diagnostics, and medical, nursing, and therapeutic procedures. This aspect can be assessed at the very beginning of treatment and when certain treatment intensity is achieved. Outcome quality is reflected by the results, for example, improvement in the quality of life or patient satisfaction.
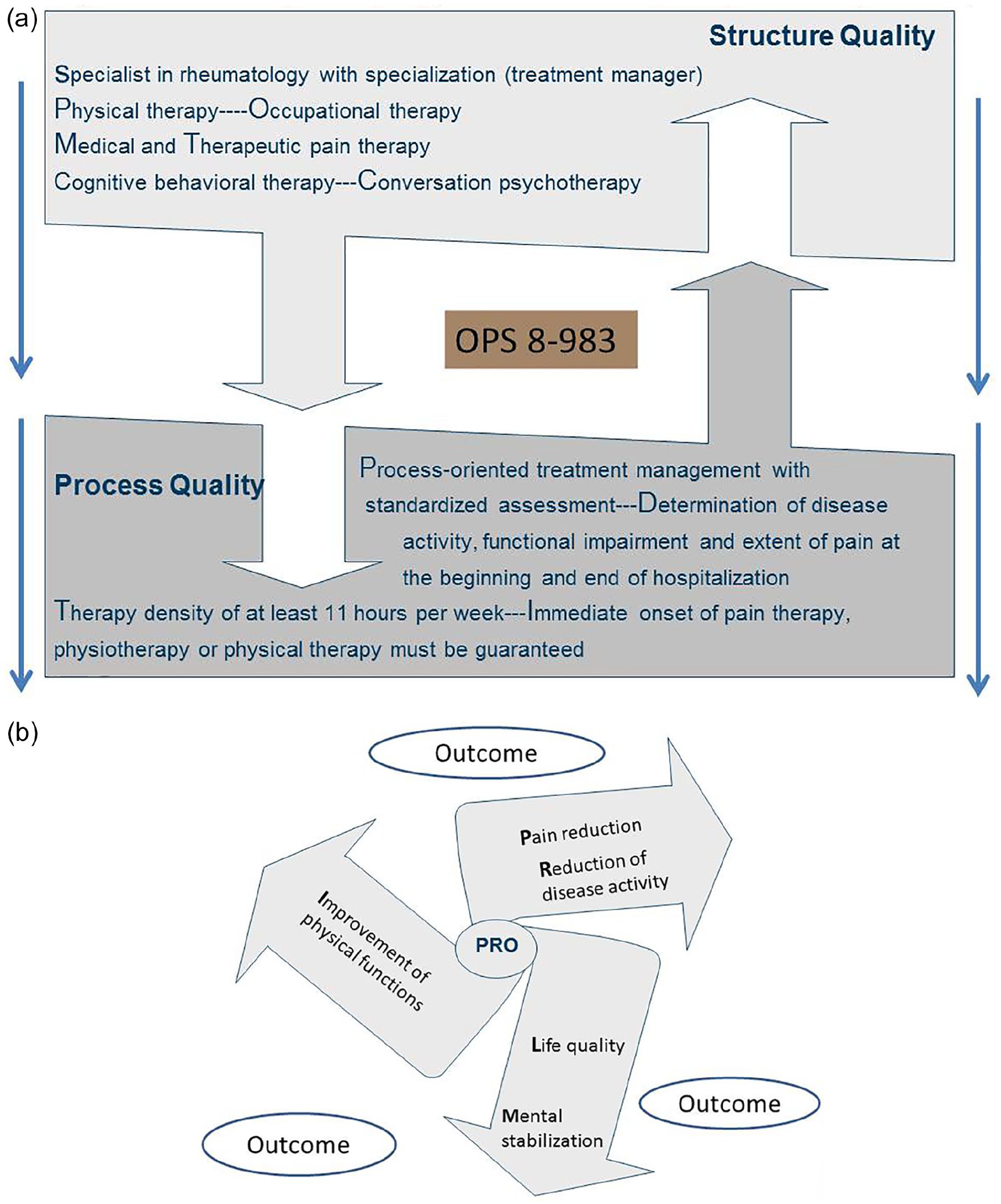
(a) Structure and process quality (Multimodal rheumatologic complex treatment, OPS 8-983) and (b) Patient reported outcome (Multimodal rheumatologic complex treatment, OPS 8-983).
Pre-defined quality indicators are needed to assess the (degree of) quality of provided healthcare services in order to implement a value-based compensation system. Indicators can be for example the six aims of the Institute of Medicine (IOM): patient-centeredness, safety, timeliness, efficiency, effectiveness and equity (Institute of Medicine (US) Committee on Quality of Health Care in America, 2001), but also improvement in pain management, assessment of communication with physicians and nurses, waiting times and workflows, building trust among the staff, or further patient-related outcomes, such as quality of life, mental health, or physical functionality. These can be reported by the patients themselves (Proms), closing the circle.
Due to scarce resources, both quality and efficiency of care are highly important in Europe’s mainly economical oriented Diagnosis Related Group (DRG) classification systems—and as a result, aspects of performance-related pay (Ryan & Blustein, 2012). This is especially true for complex treatments that result in higher costs. To compensate service providers for additional expenses and for the added value to the patient, financial incentives may be granted—an incentive instrument called Pay for Quality (P4Q) or Pay for Performance (P4P). Nevertheless, the impact of incentives on the improvement of care processes and treatment outcomes is not yet clear and investigated and discussed worldwide (Chou et al., 2019; Kiran et al., 2014).
Methods
This study aims at helping to close the research gaps outlined above by analysing the effects of MRCT (a) regarding financial feasibility based on costs/remuneration in comparison to conventional treatment and (b) Patient reported outcomes to check for effectiveness.
For (a), we investigated treatment costs and remunerations. The prices for DRGs are based on performance data of (1) all approved hospitals in Germany, as well as (2) actual cost data on MRCT collected from a random sample of specialised hospitals who participate in this data collection on a voluntary basis. Both datasets are publicly available (InEK, Reimbursement Institute). Cost data and incentives are analysed based on 18,794 treatment cases collected from the hospitals who send their data to InEK (over 100; specialized and non-specialized to cover treatment with/without MRCT) and differentiated according to the various types of costs. All costs (full costing) are considered in the cost-unit accounting. Remunerations are listed in the Institute for the Hospital Remuneration System (InEK-Data-Browser).The standardized steps for calculating the treatment costs can be seen in the additional accompanying document (further additional material; calculation steps).
For (b), a retrospective analysis of patient cases was done. All patients who were admitted to a specialized German hospital from 2013 to 2018 (Waldhausklinik Deuringen) and received MRCT were invited to participate based on the following criteria: All patients had the diagnoses: “rheumatoid arthritis,” “fibromyalgia syndrome,” “spondylitis ankylosing,” and “polymyalgia rheumatica.”
Of those who consented, (N = 375) completed the questionnaires on the Proms of interest here and are thus included in the study. The hospital is a specialized clinic with a patient-centred therapy approach that treats patients with pain and rheumatic diseases. The clinic location is in Stadtbergen, a town in Bavaria.
The diagnoses of the patients were confirmed by specialists in rheumatology, taking into account current medical guidelines, and encompassed rheumatoid arthritis, fibromyalgia syndrome, polymyalgia rheumatica, and ankylosing spondylitis. All these qualify for MRCT treatment, which all investigated patients received. The patients studied have a degree of chronicity of 2 and 3 according to Gerbershagen measure, that is, patients are homogeneous in terms of pain duration, medication, or previous outpatient or inpatient treatments. The discriminative validity was investigated using correlation and inference statistics by means of the Mainz Pain Staging System (MPSS) to determine how strongly various groups differ in the test (Gerbershagen et al., 2010).
As Proms, we used the assessment of quality of life (Nottingham Health Profile [NHP], 38 items) and the impact on physical functions (Hannover Functional Questionnaire [FFbH], 18 items). Both scales are presented below. Data was recorded at the beginning and end of hospitalization in the specialized hospital studied, as required by the guideline. Inpatient stay was typically 16 days. Data was anonymized completely, which is why we do not differentiate between socio-demographic criteria. Study participation was completely voluntary for the patients.
Nottingham Health Profile (NHP)
The NHP is a generic Prom tool that measures the subjective health status of the patient (Hunt et al., 1980). We chose the NHP because it is used in particular for patients with chronic diseases, such as rheumatic diseases (Teixeira-Salmela et al., 2004). It records the following six dimensions using 38 items: energy, pain, emotional reactions, sleep, social isolation, and physical mobility. Each dimension can receive a score from 0 to 100 by summing up the weighted items in the respective dimension. A total score is not calculated. The NHP is suitable to determine the effect of the disease on the quality of life (Wiklund, 1990) and is the current standard generic tool for recording self-assessed health related quality of life (Kohlmann, 1997). The questionnaire has been translated into German, and meets the quality criteria of practicability, reliability, validity, and sensitivity (Kohlmann, 1997).
Hannover Functional Questionnaire (FFbH)
FFbH records functional capacity of patients with rheumatic diseases. We chose the FFbH because scientific studies have validated its usefulness in diseases of the musculoskeletal system has been validated (Haase et al., 2001). It is sensitive to changes over time and mandatory for quality measurement according to OPS 8-983.
The questionnaire encompasses 18 questions on functional limitations in everyday life that are to be answered using points (0 = not at all or with external help, 1 = yes, but with difficulty, 2 = yes). Resultant values from 100% to 80% indicate “normal” functional capacity. Values close to 70% indicate moderate functional impairment, while values below 60% imply functional impairment that is clinically relevant.
Statistical Analysis
Descriptive and inductive evaluations are generated using the statistical software package SPSS Statistics 25.0 (IBM Corp, 2017). Depending on the instrument, we report N, Mean, Median, SD, Min/Max for Proms. Moreover, we compare the measurements at admission and discharge. All subjects received MRCT and thus report the Proms before and after treatment. We use the Wilcoxon signed-rank test in case necessary as nonparametric alternative to t-tests.
To analyse remunerations, the cost data for the treatments available from InEK is differentiated regarding cost types and treatment option. For the latter, we compare the remuneration for rheumatological complex treatment with the remuneration for the treatment of three disease/remuneration combinations of the rheumatologic spectrum without complex treatment. Thus, we can compare traditional and complex treatment regarding total remuneration, and remuneration for specific cost types.
In the next section, the results of the Proms as well as the incentivisation analysis are presented.
Results
After stating the results of Proms based on the investigation in Waldhausklinik, a specialized German hospital, the remuneration data (InEK) is reported. For both parts, please see Supplemental Materials A and B for more details.
Of the 375 included patients, 344 were female. The ages ranged from 24 to 82 years. All patients were advanced in chronification. More than 80% of the patients had a distinctive patient career. At the time of admission to the hospital, the patient’s condition was acutely exacerbated.
Patient Reported Outcomes Measures (Proms)
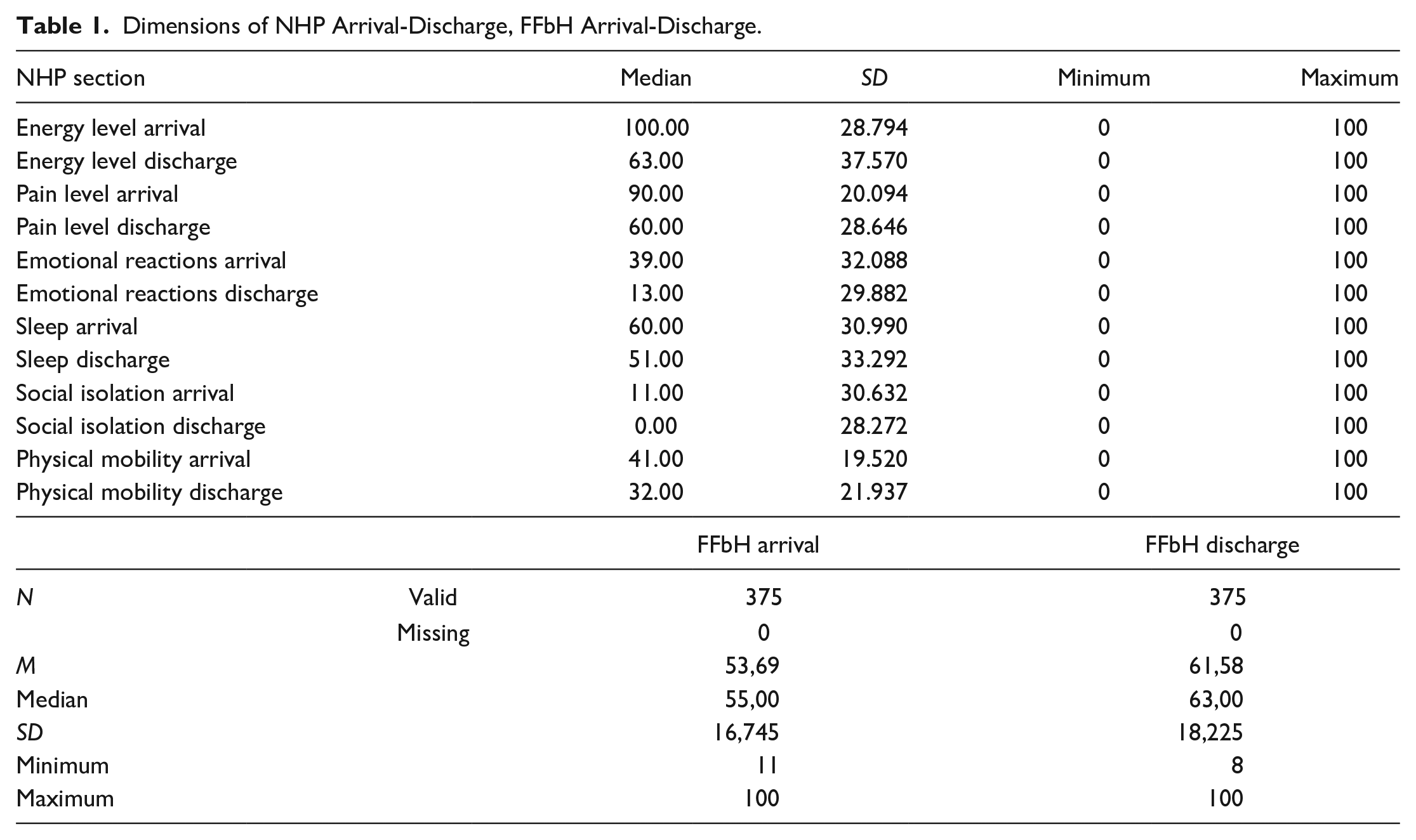
The results of the descriptive statistics of NHP and Hannover Functional Questionnaire (FFbH) are presented in Table 1. In all dimensions of the Nottingham Health Profile (NHP) the values are on average higher on admission than on discharge from the hospital (Figure 2). The plots of the NHP dimensions show several deviations from the normal distribution, as well as some outliers in various measurements. A large number of moderate and extreme outliers are present in the pain dimension at admission. The situation is similar for social isolation at discharge (Figure 3).
Dimensions of NHP Arrival-Discharge, FFbH Arrival-Discharge.

Mean NHP scores at hospital arrival and discharge.

Boxplots—dimensions NHP.
In all six dimensions of the NHP, there are significantly more negative ranks at discharge, indicating a significant improvement of the patients receiving MRCT in the specific dimensions investigated. The results are described in Table 2.
Summary of the Evaluation of the Dimensions of Nottingham Health Profile.

Incentivisation of Hospitals
For treatment without MRCT, we evaluate cost data from over 100 hospitals in Germany, on the basis of InEK costing data, in order to obtain benchmark figures. Average total costs incurred are shown for chronic polyarthritis, polymyalgia rheumatica, ankylosing spondylitis, and fibromyalgia, and compared to their remuneration. In addition, we present the average costs for the respective conditions with MRCT and their remuneration.
The Supplemental Material part B gives further details regarding the costs of the cases with diseases covered in this study under regular treatment conditions—without MRC—and also depicts the costs valid for all of those diseases with MRCT. Without multimodal treatment, hospital costs per case are decidedly lower than those with MRCT in the period studied (2017). In summary, the analysis yields the following results:
Chronic polyarthritis: N = 5,713; Mean cost = 2,255€;
Polmyalgia rheumatica und ankylosing spondylitis: N = 2,010; Mean cost 2,129€;
Fibromyalgia: N = 1,568; Mean cost = 2,907€;
MRCT: N = 878; Mean cost = 4,666€.
It is important to note here that regular treatment costs are covered by regular remuneration. Below, we go into details of remunerations for MRCT.
Figure 1 not only depicts quality aspects, but also the OPS codification for the duration of the stay in MRCT conditions (8-983.-0–8-983.2). Figure 4 shows an overview of the results regarding the remuneration system for MRCT for 2018 and 2019. MRCT ensured hospital compensation of € 5,275.81 in 2018 and € 5,364.16 in 2019 (Figure 4) for a duration of treatment of at least 14 days. The amount is independent of the rheumatic indication and is on average € 2,912 higher than without multimodal therapy. For cases with stays of more than 18 days, a daily rate of € 332.17 is added to the amount.

Incentive for multimodal rheumatologic complex treatment in 2018 and 2019.
From an economic point of view, offering MRCT only makes sense under conditions of OPS 8-983.1 and OPS 8-983.2. For OPS 8-983.0, losses are incurred. Though prices are adjusted every year and the remuneration for MRCT increased, the sum for this is not high (under € 100) and is not changing the underfunded situation of OPS 8-983.0.
Discussion
Rheumatic diseases are chronic conditions on the rise globally. In Germany, the multimodal rheumatologic complex treatment offers an option to ensure a holistic, interdisciplinary approach to the treatment of acutely exacerbated rheumatic diseases. This study aimed at analysing the effects of integrating MRCT on the hospital level (a) regarding financial feasibility based on costs/remuneration in comparison to conventional treatment and (b) Patient reported outcomes to check for effectiveness.
International health policy emphasizes the necessity of care optimization through improved outcomes, greater effectiveness, reduced costs, and integrated care (Kumar et al., 2011; Shortell et al., 2014). OECD requirements call for improved quality of care with the focus on teamwork among service providers and on treating patients as partners in the delivery of care. In this context, ore attention should be given to the needs of patients with complex conditions who need multimodal treatments (Lovell et al., 2012). This requires stakeholders to work inter- and crossdisciplinary, which is associated with improved quality and efficiency, and a positive impact on patients (Nancarrow et al., 2013). International studies demonstrate that multimodal therapeutic approaches can trigger positive stimuli and quality improvements and lead to positive outcomes for patient care (Benditz et al., 2017; Borys et al., 2015; Romeyke & Stummer, 2014). Also, the results of the Proms reported here show improvements in patient’s conditions when receiving MRCTs.
Complex treatment prescribes a standardized collection of validated Proms (Fitzpatrick et al., 1998). Due to the mandatory use of assessment parameters when the patient is admitted to the hospital, the treatment team receives the necessary information about the state of health directly from the patient. This allows creating patient-related individual treatment plans and setting individual treatment goals. As could be shown in our study, patients report improvements in terms of the six dimensions of subjective health assessment. Results of NHP show that the values are lower on discharge. Overall, physical functions also improve significantly until the discharge.
As complex treatments require specified structural and procedural conditions, providing the necessary financial resources is important. When comparing the remuneration for different types of MRCTs, we found the remuneration only equals an incentive for cases treated according to OPS 8-983.1 or OPS 8-983.2, covering patients with longer, but not stays of less than 14 days. This might be a problem for milder cases. Thought these would profit from a complex treatment that could have preventive effects, hospitals would opt for traditional treatment due to economic reasons. In the long run, this might not even affect health related, but also financial consequences negatively. The conditions of these patients might worsen and require more costly interventions and treatments. Nevertheless, for inpatient treatment of at least 14 days with high treatment intensity, the hospital has more money at its disposal to cover the added value of the treatment. This can be considered an improvement in the context of reduced options of inpatient multimodal treatments (Tompkins et al., 2017) due to rising costs and scarce resources in health systems. The German system of adjusting prices yearly and closely working together with participating hospitals in combination with strict setting of standards is an innovative approach, but not yet sufficient for all OPS. Our study demonstrated this for OPS 8-983.0. Further research is required to check which of the complex treatments stated in the OPS are financially covered, and which are not.
Limitations
Our study has several limitations. First, we report only on complex treatments for rheumatic issues in one specific geographical location. Second, there is no cost and remuneration data on MRCT before 2018 for comparison, though standard treatment cost data is available for analysis for 2016 to 2019.
In addition, the hospital investigated for the Proms related case study is specialized in complex treatments, so only cases receiving the latter could be analysed as all others are referred to regular hospitals. This means comparisons regarding Proms between patients with and without complex treatments are not possible using our data. Nevertheless, the effectiveness of MRCT could be demonstrated. However, being a specialized clinic, the impacts might have been higher due to learning effects of staff and may be lower in hospitals just starting with the offer.
We achieved an excellent response rate when collecting Proms. Only the dimension “emotional reactions” is missing 13 values. Therefore, missing data does not represent a sufficient risk of bias (Sloan et al., 2007). However, Proms are by nature self-reported, which makes them hard to objectivize. Proms can also highlight aspects of the patient experience that would otherwise be less visible to care providers, improving the basis for optimizing care. This can help to control symptoms, improve patients’ quality of life, and save resources (Noonan et al., 2017).
Comparative Analysis
Performance and quality do incur costs which have to be covered. Though contested (Woolhandler et al., 2012) and still leaving questions regarding impact on treatment outcomes and processes open (Chou et al., 2019; Kiran et al., 2014) P4P and P4Q thus are instruments for quality improvements in the clinical setting. The results of studies on financial incentives show mixed potential for P4P, but many initiatives were designed in a suboptimal way (Milstein & Schreyoegg, 2016). Mendelson et al. (2017) report divergent effects of P4P depending on the setting and the indicator. Unützer et al. (2012) highlight the relevance of choosing the most central quality indicators. For the German context, remuneration for complex treatments can be linked to incentives in the clinical setting (Romeyke et al., 2020). In our study, and in contrast to Mendelson et al. (2017), patient health seems improved based on Proms, which adds to the importance of including these measures in studies.
Stokes et al. (2018) provide an overview of types of incentive payments and lament that current uses are highly specific for sectors and illnesses, plus there is not yet much knowledge available regarding effectiveness. Cattel and Eijkenaar (2020) reviewed (value based) initiatives for quality incentives and found many for primary care, a focus on risk aspects, and generally good signs for effectiveness and efficiency. de Vries et al. (2019) highlight the role of governmental rules for implementing value-based payments. Petersen et al. (2006) underline the importance of close monitoring of incentive programs.
Though there is a focus on investigations in primary care, evidence there is discussed, as well. Glazier et al. (2019) report the need for better targeting and aligning (treatment) goals and incentives in primary care. As Lavergne et al. (2016) demonstrated, incentives do not necessarily lead to better outcomes. However, Proms were not included there, and cost reductions for treating chronic conditions are not very likely—especially not when complex treatments are administered. In addition, comparisons with other groups and preventive effects are difficult to calculate. Bazemore et al. (2018) thus argue—amongst other indicators—for including utilization and satisfaction data. Proms therefore seem promising in this sector, as well.
In sum, the alignment of goals and incentives must be carefully managed and monitored to ensure the remuneration system works properly. For this, fitting quality indicators must be chosen. Proms seem an important aspect to include. In our study, the first is not yet granted as not all types of treatments are financially covered. As for the second, we suggest Proms to become integral part of quality measurement in health care.
Implications of Research
Investing in providing and/or improving extended structural and procedural quality requires adequate remuneration. Since these quality aspects are related to outcomes, investments make sense from a public health perspective. This emphasizes that complex treatments should be offered and financially covered, which is not always the case. The difficulty of reaching good outcomes in chronic complex care underlines the importance of ensuring that they can be reached. Proms aid in this process both as indicators for outcomes as well as indirect evidence for procedural and structural quality.
Measuring the outcomes of the treatment process by means of Proms can contribute to the internal quality management and also offers an inter-institutional benchmark to service providers, which can be used as a basis for performing comparative quality measurements and researching effectiveness (Basch, 2014).
Conclusion
The study combines a financial and patient perspective on MRCT plus analyses cost types. These data can be used by other service providers to compare effectiveness and efficiency measures plus in remuneration negotiation. For health systems, healthcare providers, and patients, maintaining minimum structural requirements and emphasizing outcomes measurement will continue to be of central importance in the future (Suter et al., 2016). However, it is important that the (additional) expenses and added value are reimbursed to service providers. Financial incentives should at least cover the costs to ensure quality improvements in the long term and to keep service providers motivated in their demanding role. As could be shown, incentivisation is not yet fully implemented. This endangers the offer of MRCT, as costs incurred are or may not be fully covered.
As we analysed MRCT in the German DRG context, the financial results will be mainly comparable in highly developed health care systems. However, the methodological approach we used to analyse cost data is generalizable. In addition, our study shows that it is feasible to include Proms for chronic conditions in the context of MRCT. Both the quality of life and the physical functionality have improved in the patients. Including Proms more broadly in treatment effect measurements can create benefits in all treatment areas. So far, Proms have hardly been implemented in routine clinical care (Baumhauer, 2017).
Future research is required regarding the financial coverage of complex treatments as well as Proms. The latter should be studied in more detail in clinical care in general, and their potential in the treatment of other chronic conditions should be investigated. Moreover, comparative analysis for treatment of rheumatic diseases in other (geographical) settings is encouraged. Future research avenues also include (1) comparing remunerations for similar diseases across health systems and (2) developing effectiveness benchmarks including Proms. Moreover, (3) effects of not adequately reimbursing certain treatments could be analysed regarding costs for the health system and individual consequences. This will require interdisciplinary approaches, for example combining financial analysis with behavioural economics and outcomes research.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440221126620 – Supplemental material for Incentives for Combining Structure and Process Quality to Improve Outcome in Rheumatic Treatment
Supplemental material, sj-docx-1-sgo-10.1177_21582440221126620 for Incentives for Combining Structure and Process Quality to Improve Outcome in Rheumatic Treatment by Tobias Romeyke, Elisabeth Noehammer and Harald Stummer in SAGE Open
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All patients were informed about the study and participated voluntarily. Informed consent was obtained. For the analysis, data was completely anonymized.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.