
Abstract
This study investigated a hospital online registration system using data derived from qualitative and quantitative research and analyzed through the means-end chain (MEC) approach and Kano model. Initial qualitative surveys with 34 interviewees set up the questionnaire items used in a subsequent survey with 376 valid respondents to construct a Kano–MEC hierarchical value map (HVM). HVM depicts the innermost thoughts and cognitive structure of hospital online registration users. Findings showed that offering the functions of right-clicking the registration by department tab or by symptom of a disease and providing outpatients with instant messaging to know the progress of clinic appointment number are the most important features to rapidly improve user satisfaction. Future research may consider following the procedure used in this study to understand the actual needs of users and develop an efficient e-system for them.
Keywords
Introduction
Birth, aging, sickness, and death are unavoidable stages of life and connected with medical and health care. People aim to live healthy, wealthy, and prosperous lives. Therefore, establishing good social security and healthcare systems is important for governments. In 1995, Taiwan established the National Health Insurance (NHI) system to ensure that its citizens have access to affordable medical treatment. The NHI system is well known globally for its quality medical services and equal treatment guarantees. The NHI system currently covers 99.9% of the population (approximately 23 million residents) and has contracts with 92.69% of the country’s hospitals and clinics (HWD (Health and Welfare Department of Taiwan), 2021). These hospitals and clinics are encouraged to join an e-health-record program to advance patient referral services and merge individual healthcare networks, thereby enabling doctors to access complete medical data of referred patients across different healthcare providers. With fast, accurate, and updated information in the e-system of hospitals and clinics, medical errors can be reduced and health care can be improved accordingly (HWD (Health and Welfare Department of Taiwan), 2020).
NHI cards issued by the NHI administration are beneficial to doctors and patients. Doctors can use patients’ cards to access the e-system and retrieve their records of medication usage and past examinations. By doing so, doctors will not duplicate prescriptions or tests, thereby helping protect patient safety and reduce waste of medical resources (HWD (Health and Welfare Department of Taiwan), 2020). Patients can use their NHI cards to obtain their medical history and also to make an appointment with their doctors via walk-in, telephone, or Internet registration. Through walk-in registration, people give their outpatient NHI cards to the registration counter, pay the fee (typically US$5, including registration, treatment, and 3-day prescription medicine), and wait in line for their registered number to be called. Through telephone registration, outpatients should go to the hospital on the appointment date, show their NHI cards, and pay the fee. Occasionally, telephone operators’ errors during registration may result in outpatients spending considerable time before they see a doctor. Internet (online) registration is the most convenient way to make an appointment with doctors. People simply access the hospital registration system website to register and receive registration numbers. At the time of their appointment, outpatients can go directly to the doctors and pay the fees after medical treatment. Whether using walk-in, telephone, or the Internet to make appointments with doctors, outpatients’ registration information is stored directly into the hospital e-system. Consequently, registration systems can be viewed as a key system that connects patients’ personal information with the hospital e-system.
Although people under NHI have access to good medical care, people continue to devote considerable time waiting for treatment (Wang, Lin et al., 2018). Liu and Wu (2001) indicated that the average waiting time for treatment is approximately 100, 72, 36, and 30 minutes in medical centers, regional hospitals, district hospitals, and clinics, respectively. Long waiting time for treatment implies an increase in infection probability in waiting rooms. The World Health Organization (WHO (World Health Organization), 2021) reported that virus spreads between people who are in close contact with each other or those who stay in poorly ventilated or crowded indoor settings. Therefore, outpatients who are unable to avoid contact with other waiting patients or who need to spend long periods in crowded rooms waiting for medical treatment are in danger. If Taiwan’s medical institutions can design an efficient e-system that enables outpatients to register online and informs them of the best time to go to hospitals and their turn for medical treatment, then reducing human interaction and shortening waiting time for treatment in crowded indoor settings become possible. Hence, how to offer user-friendly and efficient online registration systems to meet outpatients/users actual needs is a current critical issue for the academia and related hospital practitioners.
In the literature, means-end chain (MEC) theory originally proposed by Gutman (1982) has been widely used to understand users’ actual needs and wants (Bolzani, 2018; Kilwinger & van Dam, 2021; Lin & Fu, 2018; Patrick & Xu, 2018). This theory argues that when users determine to use a product or system, they would consider what they would acquire after using it. As a result, their preference for the product’s/system’s attributes becomes the focal point during their decision-making process. The underlying idea of MECs is that invisible chains exist in the innermost minds of users, linking a product’s/system’s attributes (As) preferred by users with consequences (Cs) and values (Vs) perceived by these users upon using these attributes (Gutman, 1982). Referring to Gutman (1982), this study adopted MEC theory to understand outpatients’/users’ innermost thoughts toward the online registration system provided by hospitals via A–C–V chain aggregation (namely, MECs). Although MEC theory can inform researchers and practitioners which attributes, consequences, and values are important to users, it is unable to explain which attributes are “attractive features,” “indifferent features,” and “must-have features.” Therefore, this study further adopted the Kano model to reveal which attributes of a hospital online registration system are highly prioritized by users by using Kano’s quality classification (i.e., attractive, indifferent, must-be, one-dimensional, and reverse quality). By integrating MEC theory and the Kano model, this study aims to (1) understand user preferences toward using a hospital online registration system and (2) construct a Kano–MEC hierarchical value map to deduce and formulate effective e-system planning and promotion strategies.
Literature Review
Means-end Chain (MEC) Theory
Gutman (1982) proposed the MEC model to depict the relationship between consumption behavior and personal value. Reynolds and Gutman (1988) adopted the laddering technique originally developed by Hinkle (1965) to uncover the implicit meanings in each MEC. The basic idea of MEC is that a product’s attributes are the means through which consumers obtain consequences/feelings after consuming such attributes to achieve consumers’ desired end state of being (Bolzani, 2018; Kilwinger & van Dam, 2021). Therefore, each MEC contains three major components: attribute (A), consequence (C), and value (V). Each MEC includes three levels of abstractness. At the lowest level are attributes, which can be abstract (e.g., atmosphere and style) or concrete (e.g., price and weight). At the next levels are functional and psychosocial consequences. Functional consequences are feelings directly derived from product usage (e.g., whitening and moisturizing of lotion), whereas psychosocial consequences are more subjective feelings from past experiences of using products (e.g., gaining face and time-saving). At the highest level are values, which could be instrumental (e.g., honesty and responsibility) or terminal (e.g., happiness and self-respect). Aggregating individual MECs enables researchers to form a tree diagram called hierarchical value map (HVM), which visualizes consumers’ innermost thinking toward a particular product or service.
To construct an HVM, all interview data should be tabulated into a summary implication matrix via laddering (Lin et al., 2021). Reynolds and Gutman (1988) indicated that if one consumer prefers a particular product attribute (Ai) that yields particular consequences (Cj) after consumption, then the researcher should record one (i.e., linkage frequency) in the column (Cj) related to the row (Ai) in the summary implication matrix. Consequently, if m consumers have similar views with regard to the Ai–Cj linkages, then the cell of row (Ai) and column (Cj) should be recorded m as the Ai–Cj linkage frequency. By following the same procedure, Cj–Vk linkage frequencies are recorded thereafter in the appropriate cells of the summary implication matrix. After completing the table of summary implication matrix, data are transformed into HVM (Lin & Fu, 2020; Lin et al., 2021). Such a map clearly depicts consumers’ product cognitions and is gradually increasing attention from the academia and practitioners with regard to their practical use. At present, MECs have become a representative theory to reveal consumers’ innermost cognitive structure of a particular product/service (Lin et al., 2020). In practice, MEC theory has been widely used to deal with issues in the retail, communication, tourism, and healthcare industries (Jeng et al., 2020; Lin & Fu, 2020; Lin et al., 2021; Pezeshki et al., 2019; Tey et al., 2020; Xiao et al., 2017).
Kano Model
Rooted in motivation-hygiene theory (Herzberg et al., 1959), a two-dimensional model that maps customer satisfaction and product development was proposed by Kano et al. (1984). The fundamental idea of the Kano model is that different quality attributes result in varying levels of customer satisfaction. Such quality attributes in the Kano model are classified into the following five categories.
Must-be quality
Attributes in the must-be category can be viewed as essential requirements that products or services must possess to meet customer demands. If such attributes are well done, then customers take this for granted and their satisfaction level will not increase at all. However, if such attributes are missing or not well done, then customers would view products or services as incomplete and will be dissatisfied. For example, product package in good condition is viewed as an essential attribute that products must have. Hence, customers will be extremely dissatisfied if product boxes were scratched, broken, or damaged.
One-dimensional quality
Customers will be satisfied if these attributes are fulfilled but will be dissatisfied if not fulfilled. The amount of free storage space provided in Google cloud is a good example of this quality (Lin & Fu, 2018).
Attractive quality
Attractive attributes are not typically expected by customers. That is, these attributes provide satisfaction if they are fulfilled, but do not cause dissatisfaction if they are not fulfilled. For example, providing free food in hotels is not expected by customers. Thus, customers’ satisfaction will increase substantially if hotels provide free food.
Indifferent quality
Attributes classified as indifferent quality will neither result in customer satisfaction or dissatisfaction nor influence customers’ quality evaluation of products or services.
Reverse quality
Products or services that have particular attributes in the reverse category may lead to customer dissatisfaction. Hence, designers designing products should avoid these attributes.
Matzler and Hinterhuber (1998) developed functional/dysfunctional questions for the Kano data collection and created a Kano evaluation table (Table 1) to identify each attribute’s classification. By integrating Kano’s classification questionnaire and 5-point Likert scale from 1 (dislike) to 5 (like), this integration enables researchers to analyze data using systematic and statistical methods for classifying each product attribute into its appropriate Kano category, as shown in Table 1 (Chen & Su, 2006). Witell and Löfgren (2007) empirically confirmed that the five-level Kano questionnaire is the most effective measurement for classifying quality attributes.
Kano’s Evaluation Matrix.
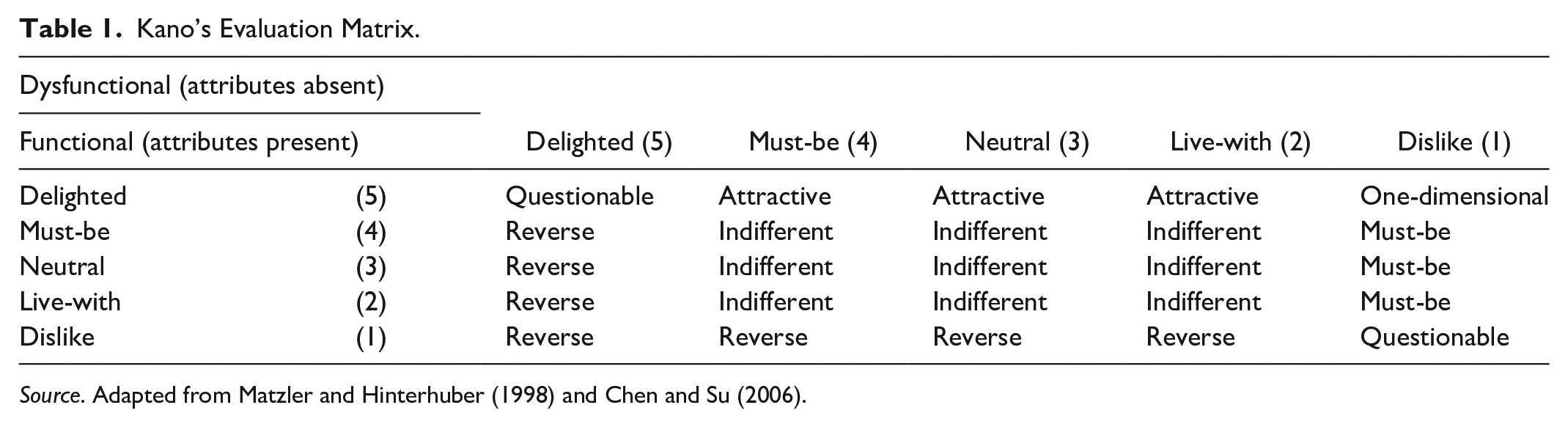
Source. Adapted from Matzler and Hinterhuber (1998) and Chen and Su (2006).
Witell et al. (2013) declared that the Kano model is an excellent tool to explain the roles of different quality attributes for customers. Plehn et al. (2016) further used the Kano model to analyze the medical tourism field and found that this model can efficiently depict key attributes to maintain satisfaction. Materla et al. (2019) assured that using the Kano model can transform the voice of the customer into inputs for the design of hospital service. In practice, the Kano model is applied in quality control and in the fields of product development, services, information, and health care (Barrios-Ipenza et al., 2021; Hussain & Mkpojiogu, 2016; Ma et al., 2019; Malinka et al., 2022; Materla et al., 2019; Yao et al., 2018).
Methods
Research Framework and Procedure
This study adopted MEC theory to examine the preferences and cognitive appraisals of users toward the hospital online registration system and then utilized the Kano model to classify the attributes or features of the online registration system into Kano’s five categories (i.e., one-dimensional, must-be, indifferent, attractive, and reverse quality). Through the use of the HVM derived from MEC theory and Kano’s quality appraisal, the findings of this study can provide hospital managers with insightful information to formulate effective strategies with regard to system planning, webpage copywriting and design, and function design. Figure 1 illustrates the research framework of this study.

Research framework.
Samples, Variables, Questionnaire Design, and Data Collection
This study used qualitative and quantitative approaches. The former was utilized to collect variables for the survey questionnaire design, whereas the latter was adopted for MEC and Kano analyses. Thus, data were collected in two stages. In stage 1, people with experiences using a hospital online registration system at least 10 times to register for themselves or family members are eligible to participate in this research. Hence, snowball sampling was used in this study. A total of 34 participants were recruited to participate in one-on-one in-depth interviews. Male and female participants were evenly divided. The majority of the participants were aged between 25 and 34 years. According to Datareportal (2021), people in this age group in Taiwan are heavy Internet users, and are also mainly familiar with hospital online registration systems. Three well-trained interviewers (i.e., two graduate students and one postdoctoral fellow familiar with MEC and the Kan model) followed the guidelines of MEC and the Kano model to collect variables for the questionnaire design. The following are the main questions asked in each interview:
Please recall the hospital online registration system that you have used before. What are the names of the hospitals? Please provide detailed information for the one that impressed you the most and why.
Which attributes/features of the online registration system do you prefer the most? Why are they important to you? Please provide more information.
What consequences or feelings do you have when the online registration system offers such attributes? What would you feel if such attributes are not provided and why?
Which values can you achieve after using this system?
Each interview took approximately 45 minutes. All interviews were audio recorded, transcribed, and conducted with permission from the participants. To ensure accuracy, interview transcripts were content analyzed using the terms identified in Table 2 and confirmed by each respondent. Thereafter, extracted phrases from the transcripts were coded into the appropriate categories of MEC as A, C, and V variables, as listed in Table 3. A total of 33 variables were gathered: 16 attribute, 13 consequence, and 4 value variables. The percentage and reliability coefficient agreements among the three coders are 94.7% and 98.2%, respectively, thereby indicating that the content analysis results are reliable (Krippendorff, 2004). The detailed procedure of the content analysis is provided in the Appendix.
Variable Definition.

Variable, codes, and definition.

With the use of the 33 variables from the 34 in-depth interviews, an MEC dot connection questionnaire was designed by arranging all the attribute, consequence, and value variables into three columns from the left to the right. All respondents were asked to choose which attributes in the first column were important to them and then draw a line to connect the dots from the attributes to the dots in the consequence and value columns to form their A–C–V chains for HVM construction. For Kano analysis, the functional/dysfunctional questions were designed by asking “How do you feel if this attribute (i.e., functional menu layout [A1], Q&A [A2], . . ., and App [A16]) is provided/not provided by the hospital online registration system?” All respondents were required to choose one of the following five levels: delighted, must-be, neutral, live with, and dislike. Therefore, the final questionnaire was designed to include one conditional question and four parts. The conditional question was used to validate that the respondent had used the online registration system before. The first part of the designed dot connection questionnaire was for the MEC analysis, and the second and third parts were the five-level Kano questionnaire, including functional and dysfunctional questions. The last part was designed to collect the respondents’ demographic information, such as gender, age, and monthly income.
In stage 2, convenient sampling was used to collect data via a paper-based questionnaire survey. With ineffective or missing data eliminated from 500 collected questionnaires, a total of 376 valid samples (effective recovery rate of 75.2%) were used for further analysis. The detailed analysis procedure of the MEC and Kano analyses is provided in the Appendix.
MEC and Kano Analyses
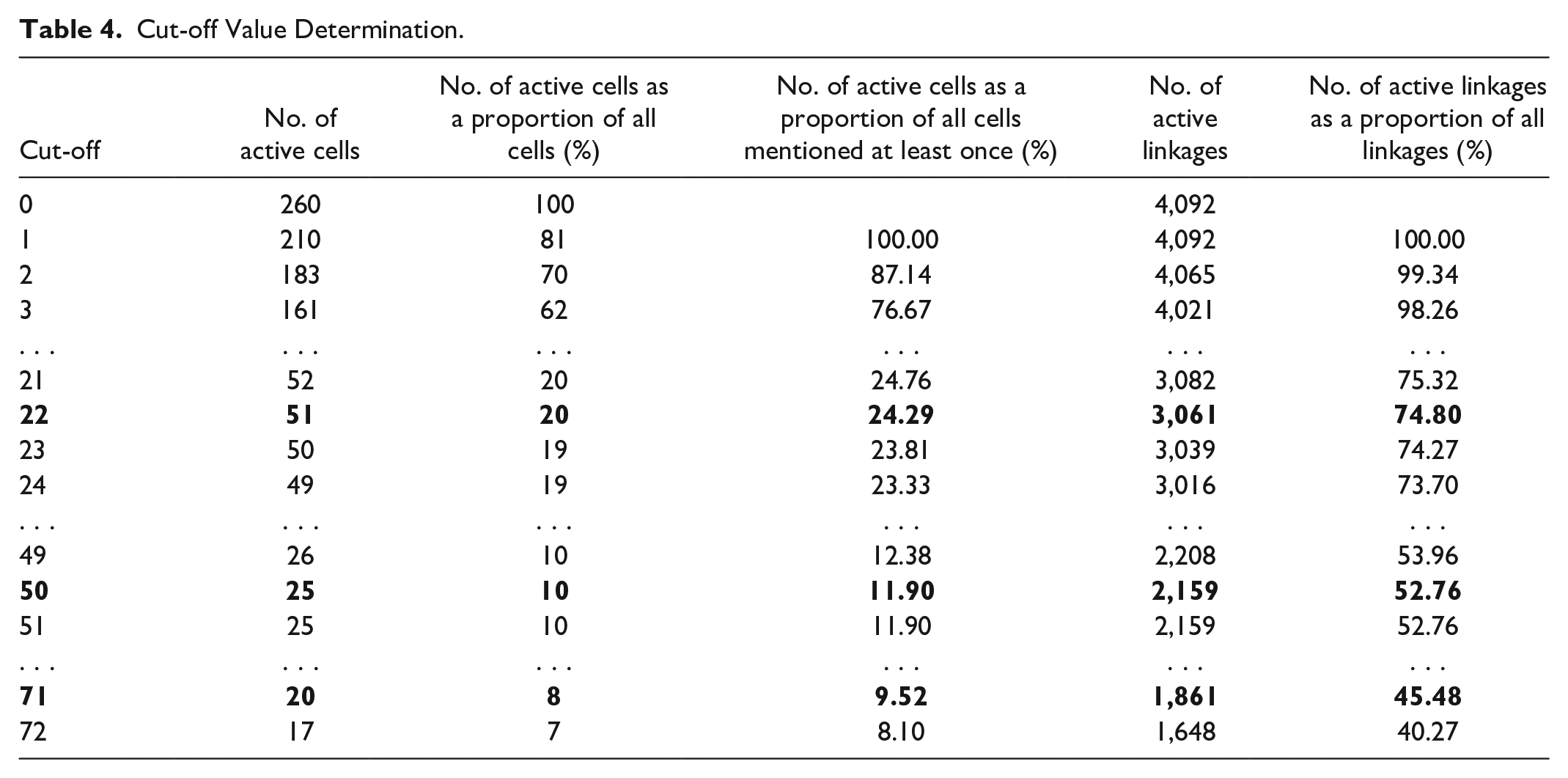
For MEC analysis, data collected from the dot connection-type questions that represent the A–C and C–V linkages and frequencies from 376 valid samples were tabulated into the summary implication matrix. In this work, 16 attribute, 13 consequence, and 4 value variables formed 260 (16 × 13 + 13 × 4) active cells in the summary implication matrix, and the total number of linkages was 4,092. Displaying 4,092 A–C and C–V linkages in a single HVM is impossible because doing so would make the HVM too complex to read. Consequently, setting a cut-off value is essential before constructing the HVM. The basic idea for the cut-off value determination is the use of a relatively small number of cells in the summary implication matrix to represent a large portion of the total number of linkages (Lin & Fu, 2018; Lin et al., 2020; Pieters et al., 1995; Wang & Yu, 2016). A detailed discussion of cut-off point determination and related criteria was provided in Pieters et al. (1995). High linkage frequencies correspond to high importance of these linkages (Lin et al., 2018, 2020). Therefore, for HVM construction, this study set the cut-off values at 22, 50, and 71 to represent weak, middle, and strong linkages, respectively. As shown in Table 4, the first cut-off value of 22 was set to construct the HVM because this level contained 74.8% of the 4,092 A–C–V linkages made by 376 respondents by using only 24.29% of all possible cells in the summary implication matrix. In other words, this HVM uncovered 74.8% of the overall information provided by the respondents but used only 24.29% of all possible cells in the matrix. A similar idea was applied to the second and third cut-off value determinations.
Cut-off Value Determination.
For the Kano analysis, this study adopted the five-level Kano questionnaire (i.e., delighted, must-be, neutral, live-with, and dislike) and used the Kano evaluation table (Table 1) proposed by Matzler and Hinterhuber (1998) to classify 16 attributes of the online registration system into one-dimensional, must-be, attractive, indifferent, and reverse quality. Furthermore, this study used customer satisfaction coefficient (see formulas 1 and 2) to evaluate which attributes can influence the satisfaction of online registration system users.


Acronyms: must-be quality (MQ), one-dimensional quality (OQ), attractive quality (AQ), indifferent quality (IQ), and attractive quality (AQ)
Results and Discussion
Sample Description
Among 376 valid samples (see Table 5), male and females occupied 39.36% and 60.64% of respondents, respectively. Approximately 36% of respondents were aged between 21 and 30 years old. A total of 67.29% respondents had a college or university degree. About 29% of them had a monthly income between NT$30,001 and NT$60,000 (US$:NT$ = 1:30) (Taiwan’s GDP per capita is US$33,433 in 2021), while the next income group (less than $30,000) accounted for 28.46%.
Sample Profile.

HVM of the Hospital Online Registration System
In Figure 2, the dotted line (weak linkage) indicates that a cut-off value of 22 was set for an HVM construction by using A–C and C–V linkage frequencies of 22 or higher in the summary implication matrix. For example, “app (A16)” provides users with “useful (C12)” feelings after using the online registration system, yielding “a sense of satisfaction (V3),” that is, hospital online registration system managers should promote that their app is useful and meets the satisfaction of users. Given that a high linkage frequency represents the high importance of the linkage, this study mainly focused on the discussion of those important (strong) linkages. The bold lines (see Figure 2) with a cut-off value of 71 represent that these A–C–V linkages are perceived as important by 376 respondents. “Functional menu layout (A1),” for instance, causes users to perceive that the system is “efficient (C1)” and leads to their “sense of security (V1).” In addition, users prefer “right-clicking the registration by department tab (A5)” and “modifying or canceling one’s appointment (A6)” provided by the hospital’s online system, because these attributes can produce a “convenience (C3)” benefit, achieving their psychological state of “security (V1),” “enjoyment (V2),” and “satisfaction (V3).” If a hospital’s registration system has the “downloading doctor’s schedule (A7)” attribute, then this attribute can make users perceive the “convenience (C3)” and “availability (C7)” of the system and thereby achieve “security (V1),” “enjoyment (V2),” and “satisfaction (V3).” Moreover, “doctor introduction (A8)” causes users to perceive that the system is “informative (C10)” and further leads to their “sense of satisfaction (V3).” “Right-clicking the registration by symptom of a disease (A13)” makes patients feel “not embarrassed (C8)” to register online and thus arouses the users’ “sense of satisfaction (V3).” Furthermore, the “instant messaging (A15)” attribute provided by the hospital online registration system not only provides users with “time-saving (C2)” and “easy-to-use (C13)” benefits but also gives users “a sense of security (V1)” and “a sense of enjoyment (V4).” Hospital managers should focus on “functional menu layout (A1),” “right-clicking the registration by department tab (A5),” “modifying or canceling one’s appointment (A6),” “downloading doctor’s schedule (A7),” “doctor introduction (A8),” “right-clicking the registration by symptom of a disease (A13),” and “instant messaging (A15)” in creating an online registration system, because these attributes are the most important features that encourage patients to make an appointment with doctors online.

The hierarchical value map of hospital online registration system.
Kano Classification of User’s Perceptions toward the Hospital Registration System
In this study, attribute data gathered from five-level Kano questionnaire were statistically analyzed and summarized in Table 6. The percentages of each row represent the results of the quality appraisals from 376 respondents. The highest percentage indicates the particular attribute belonging to that particular Kano classification, termed the first-priority attributes of Kano’s quality classification. The second highest percentage attribute is named the second-priority attributes of Kano’s quality classification.
Kano Classification.

Note. Figures in the shade of dark gray represent that the relative accumulated frequency is the highest in the row. AQ = attractive quality; IQ = indifferent quality; RQ = reverse quality; MQ = must-be quality; QQ = questionable quality; OQ = one-dimensional quality.
First-priority attributes of Kano’s quality classification
One-dimensional quality
For users, the attributes of an online registration system are classified as one-dimensional quality, which represents that user satisfaction will increase if the quality performance is good. By contrast, bad performance decreases satisfaction. As shown in the first-priority column with the symbol OQ, “right-clicking the registration by department tab (A5) (51.2%),” “modifying or canceling one’s appointment (A6) (45.6%),” “downloading doctor’s schedule (A7) (48.5%),” “doctor introduction (A8) (33.6%),” “right-clicking the registration by symptom of a disease (A13) (46.0%),” and “instant messaging (A15) (54.1%)” are classified as one-dimensional quality. Thus, the managers of hospital registration systems should pay more attention to the improvement of these attributes.
Must-be quality
None of the 16 attributes was classified as must-be quality in the first-priority Kano classification, which indicates that users believe the hospital online registration system must have these attributes. User satisfaction will not increase because the system provides these must-be attributes. However, user satisfaction will decrease dramatically if these attributes are not provided.
Attractive quality
None of the 16 attributes fell under attractive quality. If the system does not have such attributes, users will not feel dissatisfied or disappointed (Löfgren & Witell, 2005).
Indifferent quality
Whether the online registration system provides the attributes with indifferent quality will not result in user satisfaction or dissatisfaction. In this study, the following 10 attributes are classified as indifferent quality: “functional menu layout (A1) (33.1%),” “Q&A (A2) (49.3%),” “right-clicking the registration by symptom of a disease (A3) (48.5%),” “English interface (A4) (67.5%),” “schedule change notices (A9) (49.5%),” “department and clinic code (A10) (43.0%),” “hospital floor layout (A11) (36.6%),” “privacy notice of patients (A12) (50.5%),” “right-clicking the registration by doctor’s name (A14) (36.5%),” and “app (A16) (37.1%).”
Reverse quality
Attributes in the reverse category may lead to user dissatisfaction if the system provides such attributes. In this study, none of the 16 attributes was classified under reverse quality.
Second-priority attributes of Kano’s quality classification
In the first-priority Kano’s quality classification, 10 out of 16 attributes were in the indifferent category, showing that user satisfaction would not be influenced by these 10 attributes. Therefore, this study further examined the second highest percentage in each row to find the second-priority attribute quality classification of each attribute. As shown in the last column (second-priority quality classification) of Table 6, a total of 9, 2, and 5 items of attributes were grouped in the must-be, attractive, and one-dimensional categories, respectively.
Must-be quality
In the second-priority quality classification, “right-clicking the registration by department tab (A5) (30.7%),” “modifying or canceling one’s appointment (A6) (32.5%),” “downloading doctor’s schedule (A7) (35.2%),” “doctor introduction (A8) (27.5%),” “schedule change notices (A9) (19.5%),” “hospital floor layout (A11) (23.63%),” “right-clicking the registration by symptom of a disease (A13) (27.5%),” and “instant messaging (A15) (22.1%).”
Attractive quality
“Q&A (A2) (25.50%)” and “English interface (A4) (12.30%)” were grouped as attractive quality in the secondary quality classification.
One-dimensional quality
Five attributes were categorized as one-dimensional quality: “functional menu layout (A1) (28.0%),” “right-clicking the registration by symptom of a disease (A3) (20.3%),” “department and clinic code (A10) (24.9%),” “right-clicking the registration by symptom of a disease (A13) (25.9%),” and “app (A16) (29.9%).”
On the basis of the second-priority quality classification, improving attributes in the attractive and one-dimensional categories can increase user satisfaction, while attributes in the must-be category are essential features for an online registration system.
Kano’s Customer Satisfaction Coefficient
To understand the relation between online registration system users’ satisfaction/dissatisfaction if their requirements are met/unmet and the priority of these requirements in the Kano model, this study adopted Kano’s customer satisfaction coefficient to reveal the most important quality element for increasing satisfaction. As shown in Table 7, “instant messaging (A15) (0.678),” “right-clicking the registration by department tab (A5) (0.590),” and “right-clicking the registration by symptom of a disease (A3) (0.588)” are the top three most important quality attributes for increasing satisfaction. Notably, A15, A5, and A3 are classified as one-dimensional quality, thereby indicating that a high satisfaction index (SI) corresponds to the high influence of the satisfaction level. With regard to the extent of dissatisfaction indices (DSIs), the negative sign represents a negative impact on user satisfaction if these attributes are unmet. Table 7 shows that “downloading doctor’s schedule (A7) (−0.844),” “right-clicking the registration by department tab (A5) (−0.827),” and “modifying or canceling one’s appointment (A6) (−0.776)” are the top three quality attributes for decreasing the dissatisfaction level. Similarly, A7, A5, and A6 are also grouped under one-dimensional quality, thereby indicating that a high absolute value of the DSI corresponds to high dissatisfaction if the attribute does not meet the requirement of users. Interestingly, “right-clicking the registration by department tab (A5)” has high SI and DSI, thereby indicating that this attribute should be viewed as the core component that can effectively satisfy system users if its performance is met.
Customer Satisfaction Coefficient.
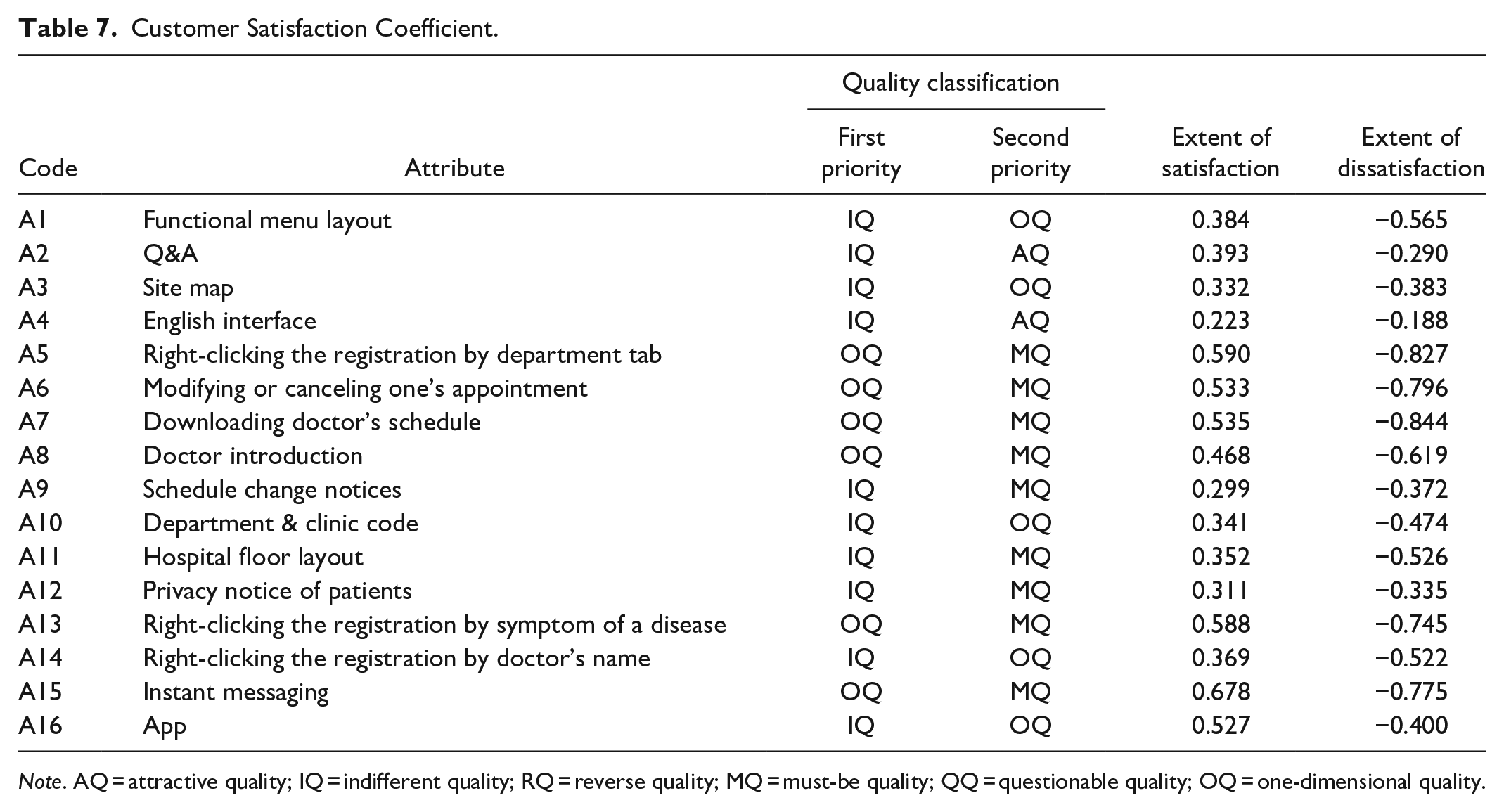
Note. AQ = attractive quality; IQ = indifferent quality; RQ = reverse quality; MQ = must-be quality; QQ = questionable quality; OQ = one-dimensional quality.
Figure 3 illustrates the impact on overall satisfaction with quality defined by the SI value on the x-axis and the absolute DSI value on the y-axis. Referring to Yao et al. (2018), when the attribute quality is far from the origin point (0, 0), such an attribute has a greater influence on satisfaction. As shown in Part I of Figure 3 (both SI and absolute DSI values greater than 0.5), “right-clicking the registration by department tab (A5),” “modifying or canceling one’s appointment (A6),” “downloading doctor’s schedule (A7),” “right-clicking the registration by symptom of a disease (A13),” and “instant messaging (A15)” are classified as one-dimensional attributes that can improve users’ satisfaction and reduce their dissatisfaction by increasing quality fulfillment. In Part II of Figure 3 (SI value greater than 0.5 but absolute DSI value less than 0.5), “app (A16)” is the only attribute located in this section. If the quality of “app (A16)” is met, then it would have a greater influence on user satisfaction improvement but less influence on dissatisfaction decrease. By contrast, “functional menu layout (A1),” “doctor introduction (A8),” “hospital floor layout (A11),” and “right-clicking the registration by doctor’s name (A14)” are attributes in Part III of Figure 3 (absolute DSI value greater than 0.5 but SI value less than 0.5) that would have greater impact on reducing user dissatisfaction but less impact on increasing user satisfaction if quality fulfillment increases. The rest of the attributes (A2, A3, A4, A9, A10, and A12) in Part IV of Figure 3 (SI and absolute DSI values less than 0.5) have little impact on user satisfaction and dissatisfaction. Thus, improving the quality of these attributes might not be necessary.

Satisfaction impact.
Conclusion and Suggestions
Conclusion
This study integrated the MEC and Kano models to reveal users’ preferences and perceptions toward the online registration system of hospitals. Through the integration of these two models, researchers can not only understand the implications of each A–C–V linkage of MEC but also further gain insight into the Kano’s quality classification of each attribute to provide hospital managers with insightful information for formulating effective e-system design and promotion strategies.
User preferences for hospital online registration system design
Figure 4 illustrates the results of integrating the MEC and Kano analyses. For MEC analysis, strong linkages correspond to increased importance of the linkages. Consequently, “functional menu layout (A1),” “right-clicking the registration by department tab (A5),” “modifying or canceling one’s appointment (A6),” “downloading doctor’s schedule (A7),” “doctor introduction (A8),” “right-clicking the registration by symptom of a disease (A13),” and “instant messaging (A15)” are the most important attributes perceived by the users of the hospital online registration system. Kano analysis indicates that users will have a high level of satisfaction if a product has more one-dimensional attributes or if such attributes have better performance. Through an integration of the strong linkages and one-dimensional classification, attributes highlighted with an orange box in Figure 4 (i.e., A5, A6, A7, A8, A13, and A15) should evidently be the focus of online registration system design. The use of attributes can yield “time-saving (C2),” “convenience (C3),” “availability (C7),” “not embarrassed (C8),” “informative (C10),” and “easy-to-use (C13)” feelings and lead to the achievement of “a sense of security (V1), “a sense of enjoyment (V4),” and “a sense of satisfaction (V3).”
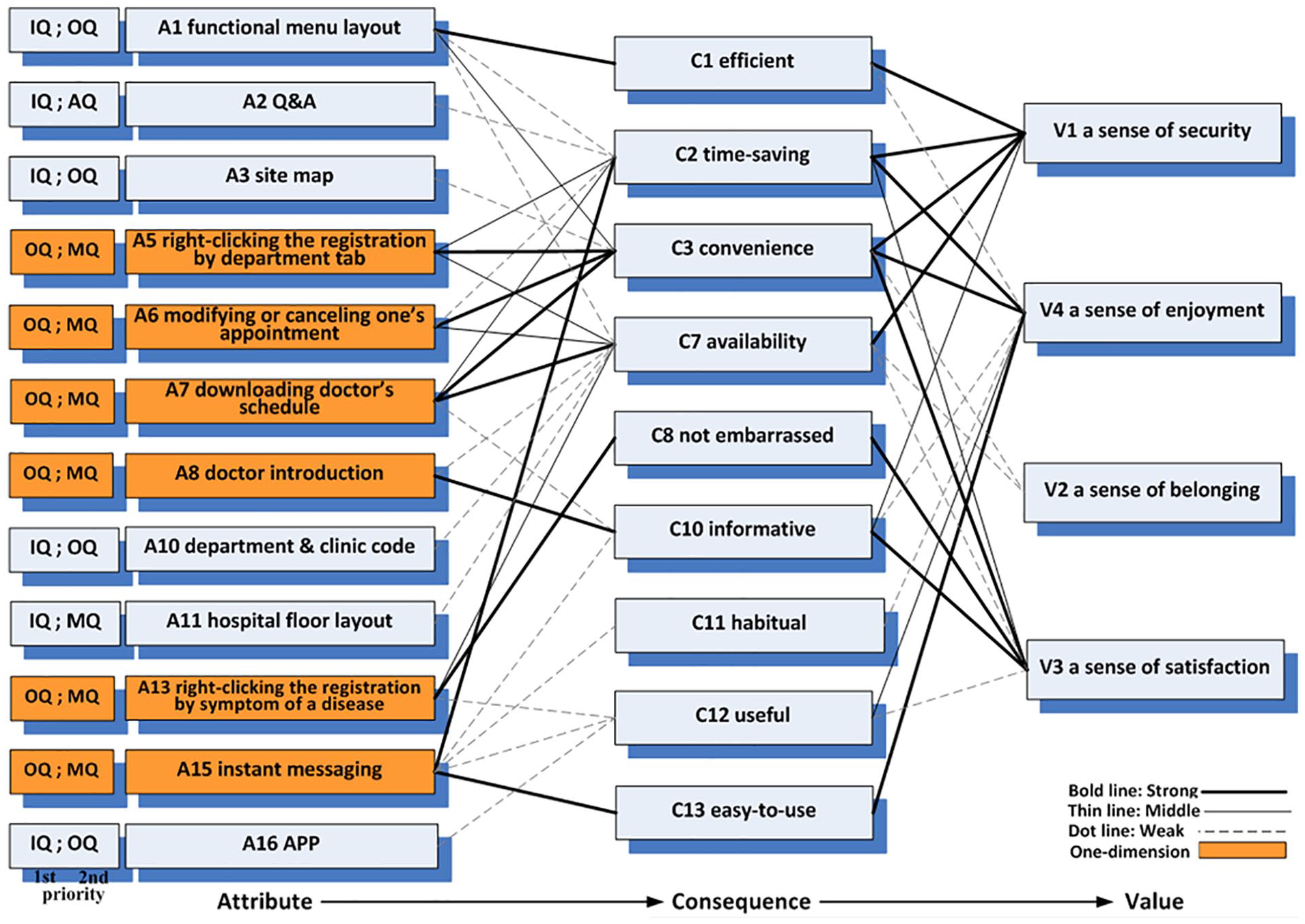
The Kano-MEC hierarchical map.
Attribute quality classification and user cognitive structure
On the left-hand side of Figure 4, each attribute is classified as indifferent, attractive, one-dimensional, or must-be quality by the respondents’ first or second priority order. First and second priorities represent that at least 33% and 12% of respondents have the same point of view and classified the attribute into its related Kano’s quality classification, respectively. In Figure 4, six attributes (A1, A2, A3, A10, A11, and A16) are listed as first priority and classified as indifferent quality, but four of them (A1, A3, A10, and A16) listed as second priority were classified as one-dimensional quality, that is, system designers still need to pay attention to “functional menu layout (A1),” site map (A3),” “department and clinic code (A10),” and “app (A16)” attributes, given that the performance of these attributes is highly related to customer satisfaction. Notably, “Q&A (A2)” in the second priority was grouped under attractive quality, representing that this attribute may produce additional satisfaction to users. “Hospital floor layout (A11)” in the second priority was classified as must-be quality, showing that at least 12% of respondents recognize this attribute as an essential feature of a registration system; without this attribute, they will feel the system is incomplete.
Suggestions
E-system planning
This study found that “right-clicking the registration by department tab (A5),” “modifying or canceling one’s appointment (A6),” “downloading doctor’s schedule (A7),” “doctor introduction (A8),” “right-clicking the registration by symptom of a disease (A13),” and “instant messaging (A15)” are classified as one-dimensional quality in the first priority and as must-be quality in the second priority, which means that they are important for online registration system design. Given that at least 33% of respondents viewed these attributes as one-dimensional quality, the high performance of these attributes corresponds to increased user satisfaction, and vice versa. These attributes were also classified under must-be quality, which means that if such attributes are missing, then users will be dissatisfied. Evidently, managers should focus on these attributes (A5, A6, A7, A8, A13, and A15) to formulate their e-system planning for enhancing the functions of their online registration system and increasing user satisfaction.
Promotion strategy
On the basis of the Kano–MEC hierarchical map (Figure 4), “efficient (C1),” “time-saving (C2),” “convenience (C3),” “availability (C7),” “not embarrassed (C8),” “informative (C10),” and “easy-to-use (C13)” are important consequences/benefits that users perceived upon utilizing the attributes of the registration system. Such consequences or benefits strongly link to “a sense of security (V1),” “a sense of enjoyment (V4),” and “a sense of satisfaction (V3),” showing that users’ values can be achieved via the consequences/benefits of using the attributes. As a result, hospitals can promote these benefits of using an online registration system to reduce the personal costs of hospital registration.
In summary, designing an e-system in hospitals that can meet users’ needs requires knowing their innermost perceptions toward hospital registration systems. Therefore, this study integrated MEC theory and the Kano model to construct a highly comprehensive user’s cognitive structure called MEC–Kano HVM (Figure 4). The use of this map enables e-system designers to understand which attributes they should significantly focus on, which feelings to arouse after using these attributes, and which values to achieve after using hospital e-systems. This study found that “right-clicking the registration by department tab (A5),” “modifying or canceling one’s appointment (A6),” “downloading doctor’s schedule (A7),” “doctor introduction (A8),” “right-clicking the registration by symptom of a disease (A13),” and “instant messaging (A15)” are must-have attributes for online registration systems. The reason is that these attributes can ultimately satisfy viewers’ desired states of “a sense of security (V1),” “a sense of enjoyment (V4),” and “a sense of satisfaction (V3).” Thus, these three value achievements should be emphasized in persuading people to use an online registration system. Given that this system connects directly to the e-system of hospitals, doctors, and health professionals can easily retrieve patients’ medical history and provide the best treatment to them. That is, an efficient hospital online registration system design can facilitate user willingness to register online and also help doctors and health professionals obtain complete and updated information of patients.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.