
Abstract
Patients with Ehlers-Danlos Syndrome, hypermobile type (hEDS) often report a decrease of health-related quality of life (HRQoL), symptoms of anxiety and depression, and show a prevalent incidence of psychiatric disorders. Still, there seems to be a lack of a more thorough analysis addressing the relations between these entities. We studied the HRQoL and its relations with depressive symptoms and subgroups of anxiety in a group of patients with hEDS (n = 81) compared to a comparison group (n = 90) of healthy controls (HC). HRQoL was assessed with the RAND 36-item health survey, depressive symptoms were measured with the 21-item Beck Depression Inventory (BDI-II) and State/trait anxiety inventory (STAI) was used to estimate levels of state and trait anxiety. The hEDS group showed significantly lower scores on total HRQoL, on all subscales as well on calculated subgroups of physical and mental HRQoL than the HC group. Depression, state, and trait anxiety scores were significantly higher in hEDS group than in the HC group. However, both state and trait anxiety showed a lower degree of negative associations with social functioning in the hEDS group when compared to the HC group. Patients with hEDS present with a lower HRQoL and greater psychological distress than healthy individuals. These factors play a significant role in the patients’ overall functional capacity and should be noticed when examining and treating patients with hEDS.
Keywords
Introduction
Ehlers-Danlos Syndrome (EDS) is the name given to a group of different inherited disorders, all involving a genetic defect in collagen and connective tissue synthesis and structure (Beighton et al., 1998). EDS is a relatively uncommon chronic illness with a variety of physical presentations. According to the National Organization for Rare Disorders (NORD, 2017) reported estimates for the incidence of all EDS types range from 1/2,500 to 1/5,000 births. The hypermobility type (hEDS) is the most common form of EDS and may affect 1/10,000 to 15,000 (Beighton et al., 2012). There seems to be no epidemiological study specifically reporting gender distribution in hEDS, but according to study samples of patients participating in studies, the sex ratio has been estimated to be approximately 4/5 in favor of women (Hermanns-Lê et al., 2016), which is in concordance with an earlier study by Castori et al. (2010), in which hEDS was more prevalent in women, with a sex ratio of 84% females and 16% males.
The genetic basis of hEDS remains unexplained and the diagnosis of hEDS is based on clinical symptoms: generalized joint hypermobility, absence of unusual skin fragility, exclusion of other heritable and acquired connective tissue disorders, and exclusion of alternative diagnoses that may also include joint hypermobility by means of hypotonia and/or connective tissue laxity (Malfait et al., 2017). The hEDS is defined as a multi-systemic disorder and the clinical description in the medical literature has expanded considerably to include more features, such as chronic pain, chronic fatigue, dysautonomia, and anxiety among other associated symptoms (Tinkle et al., 2017). The new set of clinical diagnostic guidelines and criteria for hEDS provide a framework for the diagnosis but are more stringent than the previous Villefranche Criteria (McGillis et al., 2020). The main purpose of these is to differentiate hEDS from other JH conditions as well as other EDS subtypes (Riley, 2020).
Pain symptoms are common and can be severe in hEDS. Joint pain has been reported as the most frequent and most severe symptom (Rombaut et al., 2010). Pain has shown associations with moderate to severe impairment in daily functioning (Voermans et al., 2010) as well as a high frequency of psychiatric disorders (Hershenfeld et al., 2016) in patients with hEDS.
More than three-quarters of patients with hEDS suffer from severe fatigue and those who are severely fatigued are more impaired than non-severely fatigued patients, and report a higher level of psychological distress (Voermans et al., 2010). A strong relation between severity of fatigue and fear/avoidance of movement (i.e., kinesiophobia) has been found in patients with hEDS, suggesting a direct link between musculoskeletal pain and fatigue (Celletti et al., 2013). The study by Rombaut et al. (2010) revealed that both physical and emotional health-related quality of life (HRQoL) were significantly impaired in patients with hEDS. This is further supported by more recent studies in which a significantly lower HRQoL was found in the hEDS group in comparison with a group representing the general population (Berglund et al., 2015; Bovet et al., 2016).
Patients with hEDS frequently report psychological distress, commonly exhibit a range of mental symptoms, and they have an increased incidence of psychiatric disorders. Anxiety and depression (Berglund et al., 2015; Smith et al., 2013), somatosensory amplification (Baeza-Velasco et al., 2011), and panic disorder/agoraphobia (Garcia-Campayo et al., 2011) are prevalent in hEDS. A 15-year follow-up cohort study showed a higher risk for developing anxiety disorders (Bulbena et al., 2011). In a psychiatric assessment of patients with hEDS, Pasquini et al. (2014) found an overrepresentation (21%) of personality disorders when compared to matched controls. Therefore, it appears that psychiatric symptoms are not just reactive, but some predisposition might also be present. Bulbena et al. (2015) have suggested a new neuro-connective phenotype model in hEDS that presents an anxiety–collagen hyperlaxity core with five dimensions: behavioral, psychopathological, somatic symptoms, somatosensory symptoms, and somatic illnesses.
Despite a cumulative increase of knowledge about health- and disease-related factors in patients with hEDS, the overall picture is still incomplete. Although psychological distress and decreased HRQoL are both prevalent in hEDS, there are no published studies addressing state and trait subtypes of anxiety in patients with hEDS. Consequently, we aimed to investigate HRQoL in relation to depressive symptoms and levels of state and trait anxiety in a sample of patients with hEDS, compared to healthy controls.
Methods
Participants
The study group comprised of patients (n = 81) with diagnosed hEDS, aged 18 to 65 years. A total of 46 patients (56.8%) were diagnosed according to the criteria by Malfait et al. (2017) at the Department of Clinical Genetics at a University Hospital, Finland, another 34 (42%) were diagnosed elsewhere, and data were missing for one patient. They were recruited through a private clinic and the Finnish national EDS patient association.
The comparison group of healthy controls (HC, n = 90) comprised adult nursing students (bachelor’s degree), aged 20 to 55 years, studying at a University of Applied Sciences (UAS). For the HC group the inclusion criterion was that the subject defined himself or herself as healthy. Exclusion criteria were any diagnosed medical condition, long-term pain condition, or regular medication of any kind. The participants’ socio-demographics are presented in Table 1.
Socio-Demographics of the Groups of hEDS and HC, Including p-Values for Group Differences.
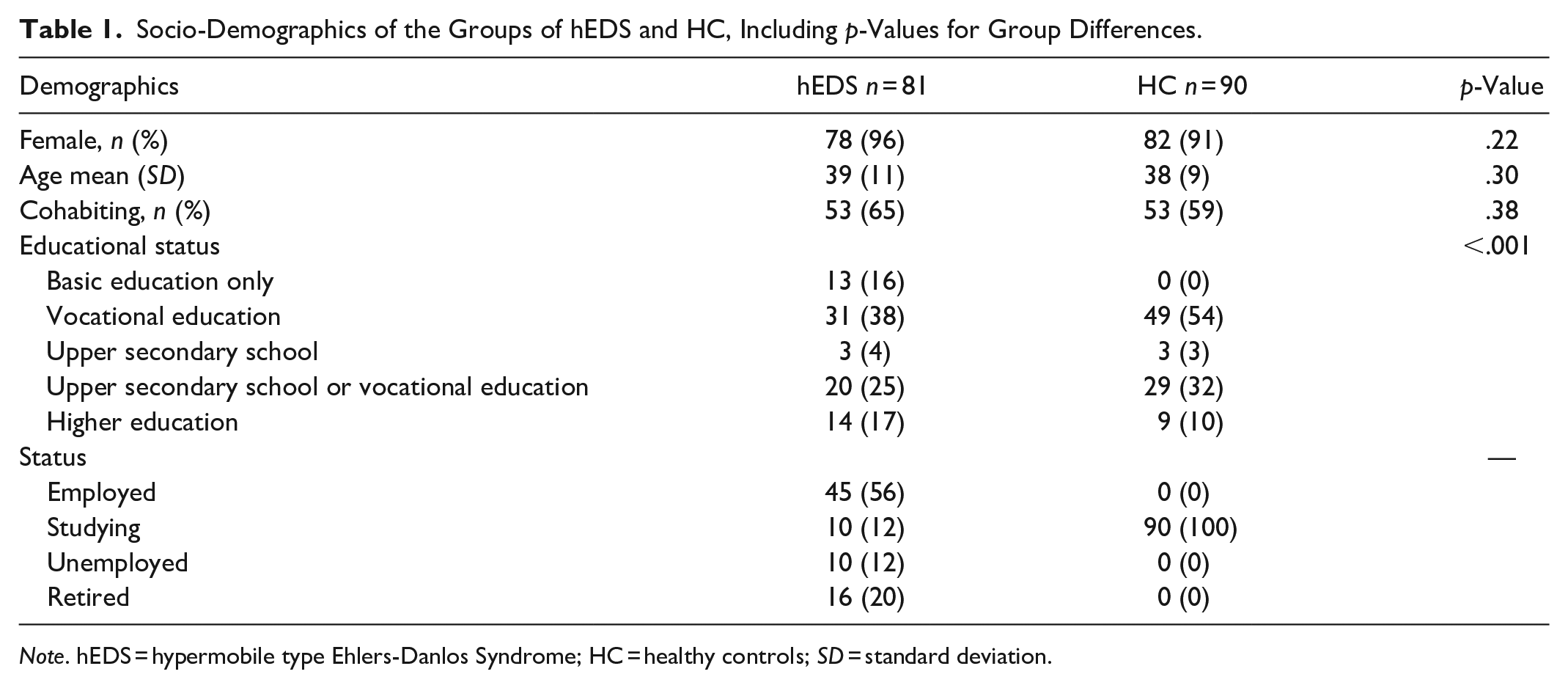
Note. hEDS = hypermobile type Ehlers-Danlos Syndrome; HC = healthy controls; SD = standard deviation.
Procedures
Questionnaires were given to 111 patients in the hEDS group: 17 were given during a rehabilitation course at a private clinic and 94 were sent by mail. A total of 89 questionnaires were returned, yielding a response rate of 80%. Eight questionnaires were discarded due to insufficient data, uncertainty of diagnosis, or wrong diagnosis.
In the HC group, questionnaires were delivered to 110 participants, 90 of which were returned, yielding a response rate of 82%. The contact person from UAS delivered the questionnaires to the participants in the HC group during one course; the questionnaires were completed after a lecture. All participants were provided with both oral and written information about the study.
Materials and Measures
Basic demographic information (gender, age, marital status, educational status, and employment status) was collected via a questionnaire.
HRQoL was assessed using the RAND-36 health survey, which consists of 36 items on eight domains of qualitative living: physical functioning, role functioning limitation due to physical health problems, emotional matters, vitality, emotional well-being, social functioning, bodily pain, and general health. The subject is instructed to answer regarding feelings during the past 4 weeks. Each item is scored on a range of 0 to 100, with higher scores indicating higher HRQoL (Aalto et al., 1999). In this study, distinct physical and mental summary components were aggregated from the eight domains by using a reference population for standardization of the eight domains and for factor score coefficients. The physical and mental component scores were standardized using a mean of 50 and a standard deviation of 10 (Korhonen et al., 2014; Ware et al., 2001). The profile-based RAND-36 is the most widely used instrument to measure HRQoL (Hays & Morales, 2001). The RAND-36 has been proven effective in differentiating levels of mobility, self-care, and poor outcome (Kaarlola et al., 2004). The Finnish version of RAND-36 has satisfactory psychometrical features (Aalto et al., 1999).
Depressive symptoms were measured with the 21-item Beck Depression Inventory, version II, (BDI-II) (Beck et al., 1996). The 21 items are scored from 0 to 3, with a total score ranging from 0 to 63. The subject is instructed to answer regarding feelings during the past 2 weeks, including the current day. According to the reference levels given in the BDI manual, 0 to 13 equals minor depression, 14 to 19 equals mild depression, 20 to 28 equals moderate depression, and 29 to 63 equals severe depression. The Finnish version has shown acceptable levels of reliability and validity (Beck et al., 2004). A good agreement between the BDI score and a diagnosis of depression has been found in patients with musculoskeletal pain (Olaya-Contreras et al., 2010).
The state–trait anxiety inventory (STAI) was used to estimate levels of anxiety subtypes (Spielberger, 1983). The STAI includes two sub-scales. The state anxiety scale (S-Anxiety) measures the presence and severity of current anxiety symptoms. The trait anxiety scale (T-Anxiety) evaluates relatively stable aspects of proneness to anxiety. The STAI has 40 items: 20 items allocated to each of the S-Anxiety and T-Anxiety sub-scales. The range of scores for each sub-test is 20 to 80, with higher scores indicating greater anxiety. A cut-off point of 39 to 40 has been suggested to detect clinically significant symptoms on the S-Anxiety scale (Addolorato et al., 1999). Responses for the S-Anxiety scale assess the intensity of the respondent’s current feelings “at this moment”: (1) not at all, (2) somewhat, (3) moderately so, and (4) very much so. Responses for the T-Anxiety scale assess the frequency of the respondent’s feelings “in general”: (1) almost never, (2) sometimes, (3) often, and (4) almost always. The STAI is reliable, valid, and sensitive to clinical change (Quek et al., 2004). Responsiveness to change has been proven good, especially in the S-Anxiety scale (Julian, 2011).
Statistical Analysis
The main physical and mental factors were calculated from the RAND-36 sub-components. Independent sample t-tests and an age- and gender-adjusted non-linear quadratic model were used in the analyses. Data are presented as the means (M) with standard deviations (SD) or as counts with percentages. The 95% confidence intervals (CI) are given for the most important outcomes. Comparisons between groups were performed using the t-test, chi-square test, or Fisher–Freeman–Halton test, when appropriate. In the case of violation of the assumptions (e.g., non-normality), a bootstrap-type t-test was used. Correlation coefficients were calculated with the Pearson’s method. Partial correlations, adjusted for age and sex, were calculated regarding BDI and STAI subscales. Differences between independent correlations were tested using the Fisher r-to-z transformation. The normality of variables was evaluated graphically, and using the Shapiro–Wilk W test. No adjustment was made for multiple testing, but this information can be obtained by multiplying the actual p-value by the number of comparisons made. All reported p-values are two-sided and were not adjusted for multiple testing. Stata 15.1 (Stata Corp LP, College Station, TX, USA) was used for the analysis.
Results
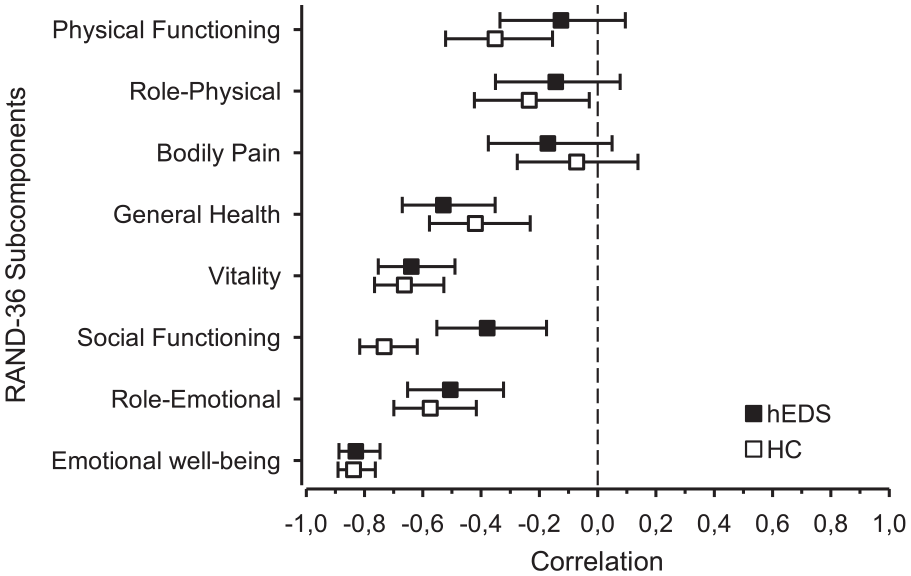
There was no significant difference regarding demographic variables between groups, but there was a significant difference between groups regarding education status, showing higher scores in the hEDS. Analyses showed that hEDS scored significantly (p < .001) lower on all eight RAND-36 sub-scales. HRQoL scores of the sub-scales of hEDS and HC are presented in Figure 1.

Age- and gender-controlled differences in eight HRQoL subcomponents between the hEDS and HC groups according to the RAND-36. The dotted line shows age- and gender controlled RAND-36 subcomponents of the general population.
After calculating separate physical and mental RAND-36 subfactors, the HRQoL–physical component score was significantly lower in the hEDS group (M = 34.69, SD = 20.32) compared to the HC group (M = 95.83, SD = 7.32); t(169) = −26.70, p < .001. The HRQoL–mental component was significantly lower in the hEDS group (M = 61.63, SD = 23.05) compared to the HC group (M = 80.58, SD = 17.73); t(169) = −6.06, p < .001.
The BDI scores were significantly higher in the hEDS group (M = 18.07, SD = 11.26) than in the HC group (M = 5.09, SD = 6.32), p < .001. In the hEDS group, 49 individuals (60%) exceeded the cut-off score for mild depression according to the clinical reference limits (Beck et al., 1996). Of these, 13 (16%) scored as having a severe degree of depression. In the HC group, the cases were 9 (10%) and 2 (2%), respectively. Group differences of BDI individual items are presented in Supplemental Appendix 1. The relationships between BDI scores and HRQoL sub-components are presented in Figure 2.

Age- and gender-controlled relations between components of HRQoL and depressive symptoms as measured by the BDI in the hEDS and HC groups.
S-Anxiety scores were significantly higher in the hEDS group (M = 45.51, SD = 14.43) than in the HC group (M = 31.90, SD = 9.81); t(168) = 7.25, p < .001. When using a cut-off value of ≥40 on S-Anxiety scores, 52 (64%) people in the hEDS group and 15 (17%) in the HC group met the criteria for clinically relevant state anxiety. The relationships between S-Anxiety scores and HRQoL sub-components are presented in Figure 3.
Age- and gender-controlled relations between components of HRQoL and state anxiety in groups of hEDS patients and HC.
T-Anxiety scores were significantly higher in the hEDS group (M = 43.86, SD = 13.96) when compared to the HC group (M = 31.59, SD = 9.58); t(169) = 6.76, p < .001. The relationships between T-Anxiety scores and HRQoL sub-components are presented in Figure 4.

Age- and gender-controlled relations between components of HRQoL and trait anxiety in groups of hEDS patients and HC.
There was a significant difference between the groups regarding associations between anxiety and the social functioning scores of HRQoL. The hEDS group showed significantly weaker negative correlation between HRQoL–social functioning scores and S-Anxiety (r = −.38, 95% CI [−0.55, −0.18]), as well as T-Anxiety (r = −.38, 95% CI [−0.55, −0.17]) than the HC group (r = −.73, CI [−0.82, −0.62]) and (r = −.63 CI [−0.74, −0.48]), respectively (Figures 3 and 4). No significant differences between the groups in relationships between HRQoL components and psychological measures were found.
A partial correlation (controlling for sex and age) between BDI and S-Anxiety and BDI and T-Anxiety scores revealed significant and similar results for both groups. In the hEDS group, the correlation between BDI and S-Anxiety was r = .83, p < .001; between BDI and T-Anxiety r = .84, p < .001. Respectively, in the HC group, the correlation between BDI and S-Anxiety was r = .85 and p < .001, and between BDI and T-Anxiety, it was r = .86, p < .001.
Discussion
In this cross-sectional comparison study, we investigated relationships between HRQoL and psychological distress, including anxiety subtypes, in a group of patients with hEDS, compared to a HC group. The results showed that the HRQoL was significantly lower on all subscales in patients with hEDS than in the HC group. Further, depression scores as well as state and trait anxiety scores were significantly higher in the hEDS group. Similar negative associations between state and trait anxiety, depressive symptoms, and HRQoL were found in both groups. However, in the hEDS group, both state and trait anxiety showed significantly weaker negative associations with social functioning group than in the HC group.
The low HRQoL levels found in this study resemble results of an earlier study by Rombaut et al. (2010) in which HRQoL was significantly impaired in patients with hEDS on all eight dimensions of the RAND-36 as well as on calculated physical and mental subfactors. These results seem intelligible, given that hEDS represents a multifaceted syndrome with extensive disease burden (Castori et al., 2013). An inverse relationship between multimorbidity or comorbidy and HRQoL has been demonstrated (Fortin et al., 2006). In chronic physical conditions, a negative association between multi-morbidity and HRQoL has been found in adult primary-care patients, even when confounding variables were controlled for Fortin et al. (2004). People with three or more chronic conditions have expressed the highest risk of reporting moderate to poor health compared with respondents with no chronic conditions (Chen et al., 2011). A study on a large (n = 21,133) population revealed that the impact of chronic conditions, particularly when experienced with comorbid disease, was associated with decrements in HRQoL. In addition, more disabling chronic conditions related to poorer HRQoL (Rothrock et al., 2010). In a follow-up study of patients undergoing total hip arthroplasty due to chronic osteoarthritis, anxiety showed a statistically significant negative correlation with HRQoL both before and after operation, indicating that a chronic illness may intrinsically maintain anxiety despite positive clinical outcomes (Montin et al., 2007). So, HRQoL is a complex factor that seems to be related to chronic conditions in general as well as multimorbidity. Given that hEDS is a multi-systemic disorder, our results are in concordance with results found in studies on other chronic conditions.
Our findings of high psychological distress in the hEDS group compared to the HC group are highly relevant and have clinical implications. Over half of the patients with hEDS expressed some degree of depressive symptoms, and almost every sixth patient presented scores for severe depression, according to reference values. In addition, nearly two-thirds of the hEDS group manifested clinically-relevant state anxiety according to criteria mentioned in the literature (Addolorato et al., 1999). The influence of anxiety on HRQoL could even exceed that of depression, as revealed in a longitudinal study by Orenius et al. (2013), in which anxiety, compared to depression, predicted decreased HRQoL in patients with diagnosed chronic musculoskeletal pain. Further, Baeza-Velasco et al. (2018) found that hEDS patients belonging to the high-anxious group had increased somatosensory amplification, pain catastrophizing, and poorer social functioning. Therefore, it seems appropriate and necessary to assess depressive and especially anxiety symptoms in every patient with hEDS and to provide treatment for cases with clinical psychological issues.
The results of this study support earlier findings showing that patients with hEDS present substantial psychological distress (Berglund et al., 2015; Smith et al., 2013) and have an increased incidence of psychiatric disorders (Bulbena et al., 2011). The plausible anxiety-proneness in patients with hEDS could reflect an elevated autonomic symptom burden. In a study by De Wandele et al. (2014), the total autonomic symptom burden (i.e., hypermobility, fatigue, pain, affective distress, and physical inactivity) was higher in hEDS than in controls (classical and vascular EDS subtypes). The same study revealed that the autonomic symptoms in hEDS correlated with lowered HRQoL, fatigue, and pain severity (De Wandele et al., 2014).
Although not analyzed in this study, pain symptoms probably relate to an impaired HRQoL in the patients in this study. Associations between pain severity and avoidance of physical activity (Koho et al., 2011; Leeuw et al., 2007; Vlaeyen & Linton, 2000) as well as positive association between self-reported physical activity and HRQoL (Bize et al., 2007) have been presented. Presumably, avoidance behavior could mediate relationships between hEDS symptoms and physical activity and thus contribute to the low levels of HRQoL found in this study. Psychosocial factors such as fear-avoidance behaviors, activity limitation, catastrophizing, and fear of movement may substantially contribute to increased levels of disability in this patient group as pointed out by Bennett et al. (2019). This subject has not yet been appropriately addressed in patients with hEDS and needs to be investigated more thoroughly in future studies, preferably using longitudinal study designs to indicate causalities.
Variation in the symptom complex in patients with hEDS could influence parameters in this study. In a study on hEDS by Castori (2012), the state of fatigue resulted from multiple factors, including muscle weakness, respiratory insufficiency, unrefreshing sleep, dysautonomia, intestinal malabsorption, reactive depression, and anxiety, as well as excessive use of analgesics. Postural Orthostatic Tachycardia Syndrome (POTS) has been indicated as a common accompanying condition in hEDS. POTS comprise symptoms that may potentially influence parameters, particularly measures that focus on symptoms of anxiety (Anderson et al., 2014). Therefore, in patients with hEDS future work should address this topic and assess the possible overlap between symptoms of POTS and the symptoms assessed using anxiety measures. Further, fatigue and enervation have been found to cause daily variability in function in patients with hEDS (Hämäläinen & Hirvonen, 2015). Therefore, these factors need to be controlled for in future studies.
An entirely novel finding in this study was that the hEDS group showed significantly weaker associations between HRQoL social functioning and levels of state and trait anxiety than did the HC group. Anxiety, defined as an emotion characterized by feelings of tension, worried thoughts, and physical changes like increased blood pressure (Kazdin, 2000), compromises quality of life and significantly impair psychosocial functioning even in individuals with sub-threshold forms of anxiety disorders (Mendlowicz & Stein, 2000). Further, the quality of life domains of mental health and social functioning have shown associations with the highest levels of impairment among patients with diagnosed anxiety disorders (Olatunji et al., 2007). It seems intuitively obvious that anxiety disrupts social interaction; further, poor social functioning generates anxiety, possibly resulting in a vicious circle. But, according to the present results, this conclusion is not that obvious in patients with hEDS. Anxiety and social functioning seem more independent features in patients with hEDS compared to individuals in the HC group. Since the weaker association in the hEDS group was found between both state and trait anxiety and HRQoL social functioning, the relation cannot be explained by the nature of trait anxiety either. Possible explanatory models need to be thoroughly studied in patients with hEDS.
There are some limitations in this study. One main issue is the suitability of the HC group as a comparison group against the hEDS group, or whether it represents the general population. Regarding the gender distribution, the comparison group matches the hEDS group, which, in turn, corresponds to sex ratios in study samples (Castori et al., 2010; Hermanns-Lê et al., 2016). Due to the high representation of females in hEDS, we chose nursing students as HC. It is known that most adult nursing students are females, with around 88% females and 12% males at the UAS (Official Statistics of Finland [OSF], 2020). In addition, in HC, BDI scores that exceed the thresholds for mild depression and major depression correspond to scores of the general population (Aasen, 2001), which further justifies the use of nursing students as HC group in this study.
Nevertheless, the inclusion of nursing students as comparison group can be criticized for differences in education. The requirements of having either a vocational or a high school degree before attending the UAS probably explains the differences in the educational status between the groups. The differences in HRQoL scores between the HC and the general population, as reported by Aalto et al. (1999), might indicate some degree of source of error, and the HC possibly presents slightly deviant scores on anxiety and depression measures as well. So, the group differences regarding educational status can impact the results and should be assessed in future studies, especially since patients with hEDS experience limited possibilities of self-actualization in daily living and social life (Berglund et al., 2015).
Another possible limitation in this study is the lack of information of the impact of pain severity on the behavioral measures. Further, there was a lack of psychiatric diagnosis since information was only obtained through questionnaires. Considering the cut-off points of the measures, more than half of the hEDS subjects have a high likelihood of suffering from anxiety disorders and/or depressive disorders. Future studies on hEDS patients would benefit from a thorough psychiatric examination. Finally, our data is cross-sectional. In future studies, a longitudinal design seems warranted in order to make causality inferences.
Even the use of self-assessment tools comprises information bias that affects the validity of health research (Althubaiti, 2016). Patients with hEDS may over- or underreport their symptoms as well as experience confusion regarding their diagnosis. Therefore, in future clinical and scientific work with this hEDS patient population the incorporation of a screening questionnaire to independently test and identify clinically significant hypermobility could be beneficial.
Strengths of this study are the good quality of the measurement methods as well as novel findings of clinical relevance. The inclusion of a comparison group for comparison can be considered a major strength. Given that hEDS is a relatively rare condition, the data from 80 patients can be considered extensive. Even the high response rates (i.e., 80% in the hEDS group and 82% in the HC group) can be considered strengths. The clinical relevance of the manuscript is the high degree of psychological distress in patients with hEDS, and importantly, that this distress relates less strongly to social functioning than in basic healthy individuals. The Supplemental Appendix 1 presenting group differences of hEDS and HC of BDI individual items can benefit clinicians who are working with patients with hEDS.
Conclusions
Patients with hEDS show a decreased HRQoL and express high levels of depression and anxiety. Therefore, it is important to pay attention to psychosocial factors in these patients in clinical practice. The biopsychosocial approach seems appropriate because of the multifaceted syndrome. Targeting psychological and psychiatric conditions could be important in managing the range of symptoms reported in these patients. Particularly the role of pain severity and fatigue in the manifestation of psychological symptoms should be thoroughly addressed in future studies.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440221091237 – Supplemental material for Health-Related Quality of Life and Psychological Distress in Patients With Hypermobility Type Ehlers-Danlos Syndrome
Supplemental material, sj-docx-1-sgo-10.1177_21582440221091237 for Health-Related Quality of Life and Psychological Distress in Patients With Hypermobility Type Ehlers-Danlos Syndrome by Tage Orenius, Hannu Kautiainen, Marja Louhi, Liisa Montin, Antonio Bulbena and Karl-August Lindgren in SAGE Open
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was obtained through Orton Evo grants by the Ministry of Social Affairs and Health, Finland. Project number 9310/462.
Compliance With Ethical Standards
The study obtained research permission by the Research Institute at Orton Ltd. All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards
Ethical Approval
The research project has the approval (312/13/03/2014) provided by an ethical committee at the Helsinki University Hospital.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.