
Abstract
The present study investigated how life stressors and sleep disturbances interactively affect depressive symptoms among university students. Based on a hypothesis that sleep disturbance can be a cause of depression, a statistical model is established which expects that life stressors impact depressive symptoms indirectly rather than directly by increasing sleep disturbances, while sleep disturbances directly work to increase depressive symptoms. Three groups of university students, Japanese (N = 784) and Chinese (N = 311) students in their native countries and Chinese students living in Japan (N = 82), were tested to reveal whether the model fits to all of them and whether there are cultural differences on life stressors and sleep disturbance. The participants responded to a set of questionnaires measuring the extent of depressive symptoms (BDI-II), sleep disturbance symptoms (insomnia, hypersomnia, and nightmare), and experience of life stressors. Japanese students reported more severe depressive symptoms than both groups of Chinese, but the Chinese have had experienced more life stressors than Japanese. Also, Japanese students reported severe hypersomnia symptoms than both groups of Chinese but the trend was reversed for nightmare. The statistical model of depression fitted well for all participant groups. Although experience of life stressors showed direct impact on depression, its indirect effect via sleep disturbance was stronger than its direct effect. This suggests that addressing sleep disturbance symptoms at earliest opportunity is an effective procedure to prevent onset of depression for university students. Implementing sleep education programs could be especially effective for this population.
Depression is one of the most widespread mental illness around the world (Murray & Lopez, 1996), signified by a persisting negative affect which manifests as a wide range of symptoms, including anxiety, loss of motivation and interests in life, low self-esteem, and sleep-related problems (World Health Organization, 2008). Established major risk factors of the illness are family history (Monroe et al., 2014), low socioeconomic position (Andersen et al., 2009), stressful life events (Kessler, 1997), and sleep disturbances (Breslau et al., 1996; Jaussent et al., 2011). The present research focuses on the last two factors, aiming to reveal their interactive influence on depression.
The association between stressful life events and depression is well established (see details in Hammen, 2005). Physiological responses to stress is a key factor for the development of depression (Burke et al., 2005), indicating that encountering stressful events is a major cause of the illness. The relationship between sleep disturbance and depressive symptoms is, on the contrary, less clear-cut. Whether the relationship is one-directional or bidirectional has been a frequent subject of debate (see Alvaro et al., 2013). While sleep distrubance is a common sypmtom of depression, some argue that it could be a cause. Indeed, there is some good evidence suggesting that sleep disturbance predicts depression much more consistently than depression predicts sleep disturbance (Buysse et al., 2008; Johnson et al., 2006). For example, childhood sleep problems can reliably predict future depression that occurs in few years’ time (Gregory et al., 2009). Among different sleep disorders, insomnia is reported to have a particularly strong relationship with depression (see reviews in Riemann et al., 2020), and many studies have shown that insomnia symptoms are independent predictors for depressive disorders (Baglioni et al., 2011; Li et al., 2016; Riemann, 2009; Riemann & Voderholzer, 2003). Also, individuals with pre-existing sleep disturbances have a significantly higher risk of developing the illness than those without sleep problems (Breslau et al., 1996; Ford & Kamerow, 1989; Okajima et al., 2012). Furthermore, increasing number of research has been establishing that the presence of sleep disturbances is an important predictor of relapse in major depressive disorder (Bao et al., 2017; Bromberger et al., 2016; Sakurai et al., 2017).
If sleep disturbance is a cause of depression, it is highly likely that there is an interactive relationship between life stress and sleep disturbances to influence depressive symptoms. Recently, Feldman et al. (2021) investigated predicting factors of psychopathology among emergency medical service providers using a prospective, longitudinal study. They reported that poor sleep quality at baseline predicted an increase in depression 3 months later. Interestingly, though, perceived levels of stress at baseline failed to predict the depression increase. The absence of relation between the stress and depression in this study is puzzling, but it is possible that the stress worked to increase sleep disturbance rather than increased depression directly. This account leads to a hypothesis that the relationship between life stress and depression is mediated by sleep disturbance. The present research investigated a theoretical model of depression based on this hypothesis, specifically, whether the primary influence of life stressor is to increase sleep disturbance rather than to increase depression symptoms directly, and sleep disturbances work to increase severity of depression. A cross-sectional survey was conducted, which measured participants’ severity of depressive symptoms, experience of sleep disturbances (insomnia, hypersomnia, and nightmare), and presence of life stressors.
The present research specifically examined university students. The prevalence of depression is influenced by a number of demographic factors such as age (Kessler et al., 2004), sex (Radloff & Rae, 1979), and socio-economic status (Steptoe et al., 2007), and there are increasing concern about the illness in particular groups, including children or young adults (Buysse et al., 2008). University students are one of those groups that might be specifically susceptive to depression and the prevalence rates among them appear to be higher than those reported in general populations (Ibrahim et al., 2013). The reason why university students are particularly vulnerable to depression is not yet clear, but one possibility is a sudden increase of life stressors. Stressful life events such as moving house and changing jobs or schools have direct influence on the onset of depression (Risch et al., 2009). Examples of life events experienced by university students are changes in lifestyle (e.g., living independently or moving to new locations), exposures to alcohol and other substances (Weitzman, 2004), pressure for academic success (Kessler et al., 1995), and concerns for future career (Kessler et al., 1998). Academic-related stress, such as exam anxiety, appears to have a specifically strong impact on students’ well-being (Bedewy & Gabriel, 2013). The source of the anxiety is likely to be an immense pressure cultivated by criticisms from teachers and parents as well as intense competitions with peers (Bedewy & Gabriel, 2015). Those unique stresses experienced by this population may relate to the high prevalence rate of sleep disturbance, which is reported to be 5% to 7% worldwide (see details in Schlarb et al., 2012). The present study investigated how these life stressors uniquely experienced by university students are related to sleep disturbance and depression.
In addition to test the theoretical model of depression, the present study aimed to examine cultural differences on sleep disturbance and depression between Chinese and Japanese individuals. Sleep patterns and academic-related stress experienced by university students must be strongly influenced by educational systems and living environment, which differ significantly across cultures. Therefore, it is meaningful to compare the stress and sleep disturbance situations in different countries and assess whether the hypothetical model of depression is applicable to multiple cultures.
The present research targeted three groups of university students who are Japanese and Chinese students studying in their native countries and Chinese students studying in Japan. These two countries were chosen based on sample availability for the authors as well as availability of established scales for depression, sleep disturbance, and life stress, written in the two languages. Also, targeting two East Asian countries enables the authors to highlight commonalities as well as differences, and the revealed commonalities may contribute to describe some general trends about depression and sleep disturbances among East Asians. It is important because large number of East Asians are reported to be suffering from depression and the prevalence rates in these regions are relatively high compared to other areas in the world (Steptoe et al., 2007). The appearance of sleep disturbances also looks high. Okawa (2012) reviewed that the prevalence of insomnia is 11.2% to 17.3% among Japanese and 12.9% to 17.5% among Chinese. Additionally, large proportion of Japanese are short sleepers (41%) while the number is much lower in China (less than 10%). Sleep disturbances among university students appear to be much higher than general population in both countries. Among Chinese students the prevalence of sleep disturbances was 25.7%, among which 20.3% had been suffering from poor sleep quality and 23.6% had insomnia symptoms (Li et al., 2018). For Japanese, a research targeting graduate students reports that approximately quarter of their sample (25.6% of 219 participants) were suffering from poor sleep quality (Pallos et al., 2007). Another research examined over 1,000 Japanese undergraduates’ sleep quality using Pittsburgh Sleep Quality Index, and found that their sleep is shorter, more disturbed, and more highly related to daytime dysfunctions than general population of Japan (Yamamoto & Nomura, 2009). In the present research, the extent of insomnia, hypersomnia, and nightmare symptoms were measured from the three groups of participants.
Along with insomnia, hypersomnia is suspected to have a strong relation with depression (Billiard et al., 1994), though the extent of its effect as a cause of depression is not yet well researched. Recently, Michaels et al. (2017) reported a relation between hypersomnia and suicidal behaviors. Murru et al. (2019) also found a positive relationship between hypersomnia and depressive episodes in bipolar disorder. Importantly, co-occurrence of hypersomnia and insomnia is surprisingly high (approximately 1 in 4) among patients of depression (Soehner et al., 2014). Nightmares also tend to cooccur with insomnia and increase the risk of severe mental illness (Sheaves et al., 2016). Nightmares are reported to enhance individuals’ suicide ideation, making people who are already suicidal even more prone to risks (Sjöström et al., 2007). Studies examined college students confirmed that nightmares increase suicide ideation by working with insomnia (Cukrowicz et al., 2006) and by working independently from it (Nadorff et al., 2011).
The inclusion of Chinese students studying in Japan in the current study is to examine how immigrants, who need to make cultural adjustment, are affected by the life stress and sleep disturbances. Living in a new culture is stressful enough but international students have many disadvantages in terms of academic achievement due to difficulties in managing non-native languages and unfamiliar studying styles. It is, therefore, important to examine whether the depression model applies to this population. The Chinese students in Japan also helps differentiating the effects of living environment and national culture (e.g., cultural values and beliefs) in the obtained results. The differences between the Chinese and Japanese in their native cultures are likely to be attributed to both their living environment and national culture. Whereas the differences between the Chinese in China and the Chines in Japan must be strongly related to their living environment. Finally, the differences between the Japanese and the Chinese in Japan can be attributed to their national culture more strongly than their living environment because the environment for both groups should have been similar, at least when the study was conducted.
In summary, the present research was conducted to investigate a model of depression supposes that relationship between life stressor and depression is mediated by sleep disturbance. Three groups of students, Chinese and Japanese who are studying in their native county as well as Chinese international students in Japan, took part in a survey measuring their severity of depressive symptoms, experience of sleep disturbances (insomnia, hypersomnia, and nightmare), and presence of life stressors. Beck Depression Inventory-II (BDI-II) was used to measure the extent of depressive symptoms. The reason behind using this inventory is that a positive correlation between this and the stressor scale mentioned below has already been established (Takahira, 1998). The sleep disturbance measure was created by combining relevant items from existing scales such as Athene Insomnia Scale (AIS: Soldatos et al., 2000) and ICD-10 (World Health Organization, 2004). To measure the level of life stress, the Scale of Life Events in Interpersonal and Achievement Domains for Undergraduate Students was used (Takahira, 1998). This scale was created specifically to measure university students’ stress, covering a wide range of events uniquely experienced in a student-life. The original was in Japanese, but a Chinese version also exists with its validity being confirmed (Matsuda & Liu, 2015). Thus, it was judged suitable to the present study.
If the mediation effect of sleep disturbance is robust in the result, this suggests that depression interventions focusing on sleep disturbances are very effective to reduce depressive symptoms, at least for university students. In fact, average psychological therapy for depression tend to focus on dealing with life stressors and treatments for sleep disturbances are not prioritized as much. It is, therefore, important to examine the relation among life stress, sleep disturbances, and depression, and to reveal how culture influences that relationship.
Methods
Participants
A total of 1,177 students participated in this study. This includes 784 Japanese students (326 males, 449 females, 9 unreported, mean age = 19.35 ± 2.35 years) from Edogawa University and Aoyama University, 311 Chinese students (110 males, 171 females, 30 unreported, mean age = 21.03 ± 1.43 years) from Shanghai Ocean University, University of Shanghai for Science and Technology, Changchun University, and Zhejiang Sci-Tech University, and 82 Chinese international students (49 males, 29 females, 4 unreported, mean age = 24.91 ± 3.27 years), who were studying at Edogawa University.
Materials and Procedure
A questionnaire distributed to participants consisted of four sections, which are a face sheet, Beck Depression Inventory-II (BDI-II), a sleep disturbance questionnaire, and a negative life-event scale. Chinese and Japanese students received the questionnaire written in their native language and Chinese international students in Japan received one written in both languages. The face sheets contained questions about participant’s demography (age, gender, and presence of pharmacological treatments for sleep disturbances). Chinese and Japanese versions of the face sheets were newly created for the present survey.
BDI-II (Steer et al., 2000) consists of 21 factors of self-report measures to assess severity of depression in the latest 1-month period. Each factor corresponds to depressive thoughts (e.g., pessimism, suicidal thoughts or wishes, and worthlessness), feelings (e.g., sadness, guilty feelings, and punishment feelings), behaviors (e.g., crying and indecisiveness), and physical conditions (e.g., changes in sleeping patterns and apatite, fatigue). Each factor consists of four choices representing varying degrees of severity (e.g., 0. I do not feel sad; 1. I feel sad; 2. I am sad all the time and I can’t snap out of it; 3. I am so sad or unhappy that I can’t stand it). The score of 0 to 3 are allocated to each choice, making the total score to range from 0 to 63. The severity is classified into four groups as follows: minimal, 0 to 13; mild, 14 to 19; moderate, 20 to 28; severe, 29 to 63. Existing Chinese (Chinese Behavioral Sciences Society, 2000) and Japanese (Kojima et al., 2002) versions of this scale were used. In terms of the reliability of this scale, several research has reported high internal consistency with Cronbach’s α being above .80 (García-Batista et al., 2018; Kojima et al., 2002; Kühner et al., 2007). The test-retest reliability correlation was also reported to be high (r = .07 in Kühner et al., 2007).
The sleep disturbance questionnaire, which contained 13 items, asked participants about the symptoms of insomnia, hypersomnia, and nightmare experienced in the latest 1-month period. Eight items measuring insomnia were taken from Athene Insomnia Scale (AIS: Soldatos et al., 2000). Established Chinese (Yen et al., 2010) and Japanese (Okajima et al., 2013) versions were used. The first five items of AIS assess quality of sleep as well as difficulties in getting asleep and maintaining sleep. The rest of the items assess the consequences of insomnia on the next day. Each question states a topic (e.g., Awakenings during the night) accompanied with four answer choices (e.g., 0. No problem; 1. Minor problem; 2. Considerable problem; 3. Serious problem or did not sleep at all). The score for each answer varies from 0 to 3 (0 always indicates no problem), thus maximum severity is indicated by the total score of 24 (3 times 8 questions). The total score exceeding 6 is regarded as clinical insomnia (Soldatos et al., 2003). In the original English version of AIS, the internal consistency among the eight items was high (Cronbach’s α = .90) and so was the test–retest reliability correlation coefficient (r = .90) at 1-week interval (Soldatos et al., 2000).
Two items related to hypersomnia and three items for nightmare were created based on the diagnostic criteria of ICD-10 (World Health Organization, 2004). The hypersomnia items asked participants whether they experienced prolonged main sleep episode caused by difficulty in waking, and whether such sleep disturbance had negative impact on their daily lives. The items of nightmare asked participants whether they experience the following: the recurrence of extremely distressful dreams, alertness after awakening from the nightmare, and significant distress or impairment in life caused by the nightmare. These questions were answered using 0 to 3 scales identical to the AIS, and therefore, the maximum score for hypersomnia was 6 and that for nightmare was 9. The Chinese and Japanese versions of the hypersomnia and nightmare items were created by referring to the wording used in the Chinese and Japanese editions of the ICD-10. Since these were newly created items in this study, validity of these items has not been tested.
The presence of stressors was measured using the Scale of Life Events in Interpersonal and Achievement Domains for Undergraduate Students (Takahira, 1998). The scale describes 30 positive and 30 negative life events, which are either related to interpersonal relationships or to life achievements (success or failure regarding to academic and work skills as well as personal interests). Participants answered whether they have experienced the described events or not in the last 3 months. Their experiences of the negative events (maximum of 30) were taken as an indication of the presence of stressors in their lives. Examples of negative events regarding interpersonal relationships are: (1) Being ignored by others. (2) Experienced a failed relationship with a friend or romantic partner. (3) Not getting along with family members. Examples of items indicating failure in achievement are: (1) Studies or research is not going well. (2) Not able to keep up with lectures. (3) Obtained bad results for exams or assignments. This scale is originally in Japanese, so it was translated into Chinese using a back-translation method. A native Chinese (a Chinese language teacher) who had lived in Japan for over 5 years translated the original questionnaire to Chinese, and another native Chinese bilingual (a postgraduate student) who had lived in Japan for more than 6 years back translated it to Japanese. A pilot study conducted by Matsuda and Liu (2015) confirmed that the factor structure for BDI-II, the sleep disturbance questionnaire and the life-event scale were identical for Chinese and Japanese versions and thus, the between language equivalence of all the questionnaires used in the present study has been validated. The reliability and validity indices of the life event scale has not been reported in previous research because the scale does not assume inter-item nor test-retest consistency (Takahira, 1998). In this scale, each event is unique and independent from each other. Therefore, it is not necessarily the case, for example, that the number of experienced positive and negative events are correlated, or that people who experience some negative events at one time consistently experience them in another time.
Ethical Considerations
Participants were asked to fill in the questionnaire voluntarily during university lectures. They were fully informed about the purpose of the study and told that they are allowed to quit anytime they want, and the responses will not be used unless the questionnaire is completed. Written informed consent was obtained from all participants. The survey was conducted anonymously, and it was impossible to identify individuals from the information on the face sheet. This research was approved by the ethics committee of Toyo University (No. P16015).
Data Sharing Statement
The current article includes the complete raw data-set collected in the study including the participants’ data set, syntax file, and log files for analysis, uploaded to the Figshare repository.
Results
Symptoms of Sleep Disorders and the Experience of Life Stressor Assessed by Severity of Depression
None of the assessed values taken in this study differed between males and females at statistically significant level. First, participants classified into four groups according to severity of depression regardless of their nationality. Participants’ experiences of negative life events and symptoms of the three sleep disturbances were aggregated for each depression severity group. The results are summarized in Table 1. The mean scores and standard deviation (in brackets) of BDI-II, the level of stressor, and the symptoms of the three sleep disturbances across all the participants were as follows: BDI-II = 12.72 (9.0); stressors = 13.29 (6.62); insomnia = 5.49 (3.47); hypersomnia = 1.09 (1.48); nightmare = 0.29 (0.1).
Means (SD) of the Stressor and Sleep Disturbances for Each Severity of Depression.

p < .05. **p < .01. ***p < .001.
When the sleep disturbance scores and life stressor scores are regressed on the BDI-II scores, significant relationships were observed, revealing that people with higher levels of stress and sleep disturbances reported severe extent of depression. The standardized regression coefficients and t-values for the analyses were also reported in Table 1. The asterisks next to the t values indicate the p values for the relevant analyses.
The Extent of Sleep Disturbance Symptoms in the Three Groups of Participants
The number of participants who reported the three types of sleep disturbance are summarized on Table 2. The severity of the sleep disturbance symptoms for each participant were categorized as “none,” “moderate,” or “serious,” in accordance with the cut-off value of the sleep disturbance questionnaire. The scores exceeding 6 for insomnia (AIS scale) were regarded as serious, and the scores of 4 and 5 were categorized as moderate. Participants whose total score of insomnia was 3 or lower were regarded as having no symptom. There are no standardized cutoff values for the hypersomnia scale (the score ranging from 0 to 6) and the nightmare scale (the score ranging from 0 to 9), so the authors determined criteria as follows. For hypersomnia, the score of 0 was regarded as no symptom, 1 to 2 was moderate, and above 3 was serious. For nightmare symptoms, 0 was none, 1 to 3 was moderate, and above 4 was serious. Table 2 also reports the number of participants for each severity of depression (minimal, mild, moderate, and severe) at each participant group. Number of people taking pharmacological treatments for the sleep disturbances were very low for all participant groups (3% for Japanese, 0.6% for Chinese, and 4% for Chinese students in Japan) so they remained to be included in the analyses.
Number of Participants (%) for Each Severity of Sleep Disturbance Symptoms and Depression.
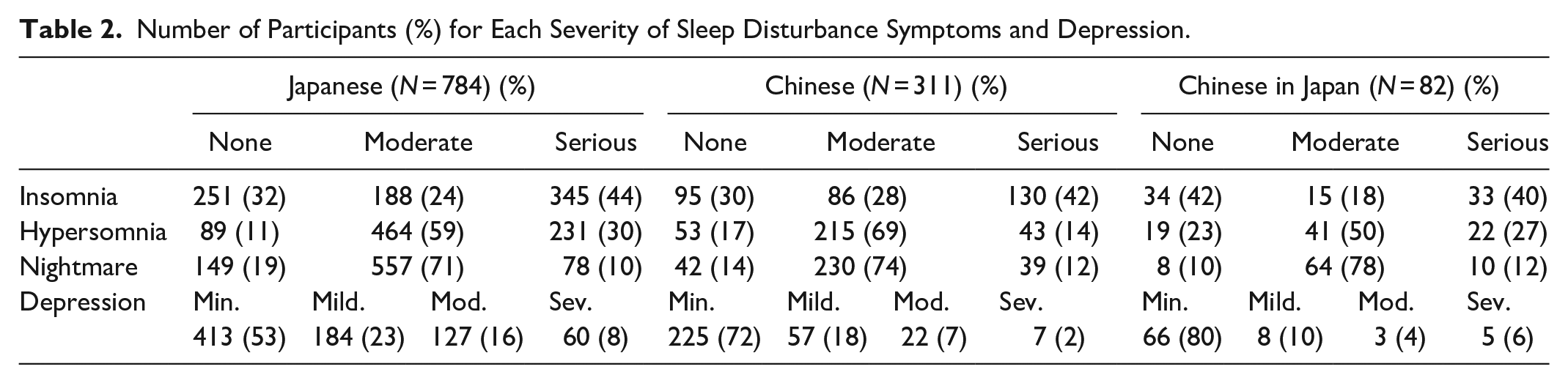
Serious symptoms were more frequently reported for insomnia than the other types of sleep disturbances for all groups of participants. A chi-square analysis on the distribution of the severity of insomnia symptoms among Chinese, Japanese, and Chinese international students revealed no cultural difference, χ2 (4) = 5.50, n.s. A similar analysis conducted for the distribution of hypersomnia symptoms reached statistical significance, χ2 (4) = 38.23, p < .001. The proportion of people with serious hypersomnia symptoms were higher for the Japanese than the Chinese students living in China. The analysis for nightmare was not significant, χ2 (4) = 8.86, p = .07.
Comparison Across Cultures for Depression, Life Stressors, and Sleep Disturbance Symptoms
Next, the mean scores for depression, stressors, and sleep disturbance symptoms were calculated for each group of participants. Each set of scores was submitted to a one-way ANOVA with a between subject factor of participant group (Chinese, Japanese, Chinese international students). The results are presented in Table 3. The asterisks on the F values and post hoc comparisons indicate p values of the relevant analyses.
Cross-Cultural Comparison of the Scores for Depression, Stressors, and Sleep Disturbances.

Note. Post-hoc comparison (Bonferroni) indicates C as Chinese in China, C in J as Chinese in Japan, and J as Japan.
p < .05. **p < .01. ***p < .001.
Substantial cultural differences were observed for severity of depression, experiences of life stressors, and symptoms of hypersomnia. The Japanese students reported significantly higher depressive tendency than the two groups of Chinese students. Those Japanese students have been, however, experiencing fewer life stressors than both groups of Chinese students.
Since the life stressor scale measured two types of events, interpersonal and achievement related, the mean scores for each event type were also submitted to the one-way ANOVAs (see Table 3). For the interpersonal items, the scores for the Chinese students exceeded that for the Japanese, but the scores for the Chinese international students did not differ from the other two groups. For the achievement related items, again the scores were higher for the Chinese students than the Japanese students, but the Chinese international students also reported the higher score than the Japanese. It should be noted that 8 items among the 15 achievement related items are about academic issues. Considering the great impact of academic-related stress on university students (Bedewy & Gabriel, 2013, 2015), it is possible that the participants had experienced more achievement related stress, which contained many academic stress items, than interpersonal stress. In order to investigate this, a paired-sample t-test was performed to compare the mean scores for the two types of events for each participant group. The results showed that the mean scores for the achievement related items were greater than the interpersonal items in all three groups [Japanese, t (783) = -7.21, p < .001; Chinese, t (310) = -6.94, p < .001; Chinese in Japan, t (81) = -5.35, p < .001], confirming that academic related stress is frequently experienced among university students.
In terms of sleep disturbances, the scores of insomnia symptoms are much higher than those for other two disorders regardless of the culture, and the magnitude of insomnia are equivalent across three participant groups. The reported symptoms of hypersomnia, though, differed significantly across groups, and showing that Japanese students scored higher than both groups of Chinese. The scores for nightmare symptoms also revealed a weak but a significant effect of participant group with higher scores for Chinese students in Japan than for the native Japanese.
Assessment of the Depression Model
The hypothesized model of depression contains “severity of depression” as a dependent variable and “stressor” and “sleep disturbance” as predictor variables. The model was tested using structural equation modeling (SEM) of IBM SPSS Amos 25. The maximum likelihood estimates were used. The sleep disturbance was a latent variable defined by the mean scores of all three sleep disorders. The stressor was an observable variable, which was the reported number of negative events on the Scale of Life Events in Interpersonal and Achievement Domains for Undergraduate Students. The number of experienced positive events were not included in the analysis because, as mentioned in the method section, each event in this scale is independent from each other, so it cannot be assumed that the number of positive and negative life events are negatively correlated. Reporting bias for positive events was also found for this scale (Takahira, 1998), and therefore, it was decided inappropriate to form a latent construct by combining the answers for the positive and negative events. In this model, the presence of life stressors is expected to increase sleep disturbances, which consequently causes depression. The stressor is expected to predict the extent of depressive symptoms but the regression path from stressor to sleep disturbance could be stronger than the path from stressor to depression.
The model was firstly assessed by nationality using a multi-group path analysis. The model was compared with its nested models, and the χ2 fit index of the hypothetical model was significantly larger than those of the nested models. The coefficient for the path running from sleep disturbance to insomnia was set to 1. The indices used to assess the model fitness were χ2, goodness of fit statistic (GFI), adjusted goodness of fit statistic (AGFI), comparative fit index (CFI), standardized root mean square residual (SRMR), and root mean square error of approximation (RMSEA). The present research employed the following cutoffs to judge the goodness of the model: GFI ≥ 0.90, AGFI ≥ 0.90, CFI ≥ 0.95, SRMR ≤ 0.05, RMSEA ≤ 0.06 (see Hooper et al., 2008, for the criteria). According to Hooper et al. (2008), there is no recognized cutoff for χ2 values, but the chi-square divided by the degrees of freedom (χ2/df) can be used as a measure of model fit, with values of 5 or less indicating an acceptable level.
The results reported on Figure 1 shows that this model fits the data adequately, χ2 = 27.12, df = 12, χ2/df = 2.26, p = .01, GFI = 0.99, AGFI = 0.97, CFI = 0.99, SRMR = 0.02, RMSEA = 0.03. The asterisks on each coefficient indicate the level of statistical significance of each path. Sleep disturbance scores are the better predictor of depression than the life stressor scores. Although the regression coefficient between depression and life stressor was significant for Japanese and Chinese in China, this path did not reach statistical significance for Chinese students in Japan. The path from stressor to sleep disturbance as well as the path from sleep disturbance to depression are highly significant. Importantly, indirect effect from stressor to depression via sleep disturbance was significant for all groups. The model, therefore, suggests that seriousness of sleep disturbance predicts depression more strongly than stressors do. Furthermore, stressors appear to have a strong influence on sleep disturbance, much more so than to depressive symptoms, which suggests that life stressors influence on depression through sleep disturbances in a major way. The analysis revealed that the direct path from stressors to depression was weaker for the Chinese in Japan compared to that for the Japanese.

The model of depression for the three groups of participants.
Next, the whole data were divided into four categories based on BDI-II cutoffs regardless of participants’ nationality (see Table 1) to examine whether the fitness level of the model differs by severity of depressive symptoms. The result is reported in Figure 2. The asterisks on each coefficient indicate the level of statistical significance of each path. The model fits adequately again in this analysis (χ2 = 19.56, df = 16, χ2/df = 1.22, p = .24, GFI = 0.99, AGFI = 0.98, CFI = 0.99, SRMR = 0.02, RMSEA = 0.01), generally showing that the direct influence of depression is stronger from sleep disturbance than from stressor. The direct effect from stressor to depression was not observed for participants having severe and mild level of depressive symptoms while these two groups yielded a significant path from sleep disturbance to depression. Interestingly, the impact of stressor to sleep disturbance was robust only for participants with minimal depressive symptoms. The indirect effect of stressor to depression via sleep disturbance was significant or marginally significant for participants with minimal, mild, and severe level of depressive symptoms.

The model of depression for the four groups by depression severity.
Discussion
The present research aimed to investigate a model of depression supposes that the relationship between life stressor and depressive symptoms is mediated by sleep disturbance. Three groups of students, Chinese and Japanese living in their native county as well as Chinese international students in Japan, responded to a survey measuring their severity of depressive symptoms, experience of sleep disturbances, and presence of life stressors. The model was generally supported by the results, showing that the primary impact of stressful life events on depression is indirect through sleep disturbance. In the present results, the impact of life stressor on depression was not as robust as the impact of sleep disturbance on depression. Stressors did not influence depression directly for Chinese students in Japan. Also, the life stressor scores could predict depression scores well only when the symptom was minimal. It has been argued that the role of life stress on depression is not straightforward because perception of stress interacts with other factors such as family history of depression (Monroe et al., 2014). The present results might have been affected by such factors. On the contrary to the life stress, the current model demonstrated that the causal effect of sleep disturbances to depression was robust. Therefore, the present model supports the account that sleep disturbances are independent predictors for depression (Baglioni et al., 2011; Buysse et al., 2008; Gregory et al., 2009; Johnson et al., 2006; Li et al., 2016; Riemann, 2009; Riemann & Voderholzer, 2003).
The mechanism of the interactive effect of life stress and sleep disturbances could be related to stress coping behaviors. It has been reported that sleep disturbances prevent people to use healthy stress coping behaviors, such as seeking for help and performing physical activities, and encourage them to use more unhealthy ones such as medication or overeating (Bergmans et al., 2021). Consequently, perceived stress level become greater for people with sleep disturbances than those without, making them more prone to mental illness. However, research findings on this issue are inconsistent; one study found that sleep disorders are associated with both smoking and drinking alcohol (Otsuka et al., 2017), while another study found no relation between insomnia and substance use for stress coping (Palagini et al., 2016). The present results cannot assess this mechanism since it did not measure perceived stress level, but it will be very informative to investigate the relationship among experience of stressful events, perceived level of stress, sleep disturbance symptoms, and coping strategies.
Regarding sleep disturbance, the present research revealed that it is frequently experienced among university students in China and Japan. More than half of the participants in the present study reported either moderate or serious sleep disturbance, consistent with a number of research demonstrating very high prevalence of sleep disturbance among university students (see details in, Lund et al., 2010). Cultural differences on sleep disturbance scores were present for hypersomnia and nightmare. For the former, Japanese students reported higher scores than Chinese living in China. Considering that there was no difference between the Japanese students and Chinese international students in Japan, hypersomnia symptoms are likely to be associated with difference in student lifestyles in China and Japan. One possibility of such difference is availability of student accommodation and how students’ daily schedules are controlled. In China, most students live in student accommodations and their daily schedule such as mealtime and bedtime tend to be monitored by the facility. In most accommodations, meals are provided, and lights are turned off at specific times. Compared to this, most university students in Japan live in rented apartments individually if they live away from their families. This freedom of deciding their own daily schedule likely to cause inconsistent bedtimes as well as sleeping hours for students in Japan. Indeed, it is reported that university students who live with their family have lesser degree of sleep disturbance than who don’t live with them (Galambos et al., 2013) and so, some external control on students’ daily schedule may reduce hypersomnia.
Contrasting to hypersomnia, both groups of Chinese students reported more serious nightmare problems than Japanese, consistent with a study revealing high level of nightmare experiences among Chinese university students (Wang et al., 2021). Interestingly, a very similar tendency to this was observed for experiences of negative life events. Chinese students experienced more stressful life events than Japanese, however, did not report severe depressive symptoms compared to the Japanese. This may suggest that recent experiences of negative life events are strongly connected to nightmares for the Chinese students while the link is not as strong for the Japanese. Nightmare occurrence is thought to be associated with state anxiety (Köthe & Pietrowsky, 2001) and thus, it is possible that negative life events measured in the present research triggered stronger anxiety for Chinese than for Japanese. Chinese students may strongly believe that their social and academic performance in university affects their future while Japanese students may not have such a strong belief. What employers look for in university graduates may differ across countries. Comparing the employment strategies of companies between China and Japan is out of scope of this research, but it is possible that Chinese students get anxious by experiencing negative life events because they connect those experiences and failures in the future.
The Chinese international students in the present study did not show noticeably severe symptoms for depression and sleep disturbance compared to the students studying in their native countries. While international students are likely to be exposed to difficulties during cultural adaptation, those who choose to study abroad may tend to have higher self-efficacy and adaptive capability than those who stay in their native countries. In fact, Matsuda and Liu (2015) reported that Chinese international students in Japan with high level of self-efficacy and adaptive ability (open to acculturation and integration) tend to show good mental health and sleeping patterns. Thus, investigation on mental illness specifically caused by cross-cultural experiences may needs to target people who are already suffering from some clinical problems.
Regarding stressful life events, most students in the present study have experienced almost half of the negative life events described in the questionnaire (approximately 15 out of 30 events). Thus, it is fair to say that university students are exposed to varieties of stress related to academic performance and interpersonal connection (Lund et al., 2010). Academic-related stress appear to be frequently experienced by all participant groups, supporting previous studies reporting that pressure caused by academic evaluations and competitions negatively influence students’ well-being (Bedewy & Gabriel, 2013, 2015). The present model demonstrated that those stressful events work to increase sleep disturbances. Other types of stresses which were not measured in the present study may also be experienced by the students and affected their sleep. Pressure for socialization including drinking and smoking, for example, is a unique type of stress introduced to people at late adolescent. Not only the intake of those substances directly triggers sleep disturbance (Pallos et al., 2007) but also pressure for socialization may increase students’ mobile phone and social media use, which consequently disturbs sleeping patterns (Adams & Kisler, 2013).
The findings of present research emphasize the importance of sleep disturbance treatment to reduce depressive symptoms. In Japan, cognitive therapy is most frequently used treatment for depression, and it tends to focus on altering cognition of stress rather than addressing sleep disturbance symptoms. Of course, working on stressors is important but the present study suggests that it is only the case for people with minimal or moderate depressive symptoms. For people with severe depressive symptoms, treating sleep disturbance may be a more effective and direct solution. Cognitive behavioral therapy (CBT) for sleep disturbance has been proved to be very effective especially for insomnia (Qaseem et al., 2016; Riemann et al., 2017; Riemann & Perlis, 2009), and its positive effect was also confirmed among university students (Freeman et al., 2015). However, CBT for sleep disturbance is not readily available in general, due to lack of professionals and inefficient service delivery systems. This has been preventing the treatment to achieve high volume of patient care in the last few decades (Espie, 2009). Also, university student may have insufficient awareness about the relationship between sleep problems and mental illness and so, they may not feel grate urgency in changing their sleeping habits. These situations have led researchers to try psychoeducational approaches to improve sleep quality among university students (see Kloss et al., 2011, for review).
University students tend to lack knowledge on good sleep hygiene (Suen et al., 2010) and thus, simply informing them using an educational program can improve their sleep quality and sleep hygiene behaviors (Brown et al., 2006). Importantly, research shows that sufficient knowledge alone does not improve sleep quality, and implementation of good sleep practices, such as maintaining regular sleep and wake times, and limiting caffeine and alcohol consumption, is essential (Brown et al., 2002). For example, Orzech et al. (2011) carried out a sleep media campaign for American college students by distributing posters, newspaper adverts, and newsletters featuring sleep related topics in student accommodations and observed that individuals who engaged in the campaign improved their sleep patterns as well as their mental health. Delivering the educational programs online is thought to be especially effective for the university student population, due to their high level of computer literacy (Kloss et al., 2011). Integrating such programs in the academic curriculum would also work to engage with large number of students.
The present research showed that the profile of sleep disturbance symptoms slightly differed across cultures, implying that culturally tailored educational program can be very effective. For instance, presence of nightmare was noticeable among Chinese students, and it might be related to their level of anxiety. Thus, it is ideal for the sleep educational programs to teach Chinese students how to reduce anxiety triggered by experiences of negative events. Including culturally specific exercises, food, and philosophy in the program is another way to make the training more familiar to students. For example, limiting alcohol and caffeine consumption contributes to good sleep and so, the educational program can recommend alternative favorable drinks that are readily available in the students’ culture.
The present research involves several limitations. One is the unbalanced sample sizes across groups. Especially, number of Chinese students in Japan were small and thus, it is difficult to draw strong conclusions about this group. Also, students’ living conditions (i.e., living in accommodation or living with family), which seem to have strong influence on sleep disturbance symptoms, were not considered in this research. The actual lifestyles of students in different cultures need to be thoroughly examined in order to assess how culture influences people’s sleep.
Another limitation is a potential response bias of the participants, which is caused by the study method. It is often referred as common method biases (CMBs) or common method variance (CMV), which is “any systematic, non-substantive influence on measures of substantive constructs that is due to the method of measurement used” (Baumgartner et al., 2021, p. 221). Measuring several variables using a common methodology (e.g., a questionnaire form as in the present study) can result in high amount of spurious covariance among them. The theme of the study can also cause response bias. For example, responses for sensitive personal issues tend to be heavily influenced by social desirability (Af Wåhlberg, 2010). It is possible that the present results are affected by those biases. CMB and CMV can be reduced by changing the response format across variables and giving participants short time lags between answering each variable (Podsakoff et al., 2012). Fortunately, the scales for depression (BDI-II), sleep disturbance, and life stress in the present study had slightly different answering formats. Although BDI-II and the sleep disturbance scale both required participants to choose their answers from 0 to 3, the choices of BDI-II were phrased differently in each question. Furthermore, the response for the life event scale, which selecting experienced events from a set of choices, was different from the other two. This variations in answering formats might have worked to reduce potential response bias in the present study, but still, all the measurements were organized as a single questionnaire and these measurements were about sensitive personal issues. Therefore, further research with improved methods is strongly desired. Important to note, however, that isolating the impact of CMB and CMV from observed results is very difficult because it is highly variable depending on the correlational direction (positive or negative) between the measurements and item reliability of each measurement (Baumgartner et al., 2021). Also, it is frequently argued whether CMB or CMV distorts empirical findings at all. Some says that the distortion is serios (e.g., Podsakoff et al., 2012), and others say the impact is minimal (Lance et al., 2010; Spector, 1987).
In conclusion, the present research denies that sleep disturbance is just a symptom of depression. Rather, it supports the account that it has a significant effect on the onset and severity of the illness. Furthermore, stressful life events are likely to increase depressive symptoms through worsening sleep problems. Therefore, addressing sleep disturbance is important for both preventing and treating depression. In case of university students, academic related stress and poor sleeping qualities, which are products of their student-lifestyle, interact with each other to affect their mental health. Educational institutions can find many ways to help their students, but it is important to remember that people’s lifestyles are partly determined by culture, thus effective solution can be culturally variable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All participants in this research submitted written informed consent. The research was approved by the ethics committee of the Department of Social Psychology, Toyo University (No. P16015).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI [Grant No. 22730552] awarded for the first author.