
Abstract
Nightmares influence the mental health of university students, but the prevalence of nightmare and nightmare disorder requires additional documentation. The data of detailed nightmare experience of nightmare disorder and related depressive mood in this population are also scarce. First, a total of 1,451 students in a comprehensive Chinese university were invited to report their nightmare frequency. Sixty-eight patients with nightmare disorder were diagnosed using a semi-structured clinical interview according to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013). Second, 60 patients with nightmare disorder (8 of 68 patients were dismissed due to data incompletion) and 124 gender-matched, healthy students were invited to answer the Nightmare Experience Questionnaire (NEQ) and the Plutchik-van Praag Depression Inventory (PVP). Of 1,451 students, 923 reported nightmares (its annual prevalence was 63.61%), and 68 were diagnosed with nightmare disorder (its prevalence was 4.69%), with a female preponderance. The mean PVP and four NEQ scale scores in patients were higher than those in healthy students. The PVP scores were correlated with NEQ Physical Effect in patients, and with Negative Emotion in healthy students. This is the first report regarding nightmare disorder prevalence and detailed nightmare experience in university students. The findings of a high prevalence of nightmare disorder in women and elevated scores of nightmare experience among patients in the university population might help address the mechanisms and the management of patients with nightmare disorder.
Introduction
At some stages in their life, people may experience nightmares, especially female adolescents or young adults (Schredl & Reinhard, 2011). Approximately 2% to 6% of normal adults report nightmares once a week or more (Sandman et al., 2013), although there are limited nightmare reports available for health care providers with underutilized nightmare treatments in general (Nadorff et al., 2015). The etiology of nightmares is not yet fully known, but the psychological processes related to worry, depersonalization, paranoia, and hallucinatory experiences might cause nightmares (Rek et al., 2017). Job stress (Kalimo et al., 2000), and work experiences of typical jobs like the cumulation of critical incident–exposure among police officers (Vila, 2006) or death-related experience among nurses (Mealer et al., 2009) were found to be associated with individual nightmare experience. Recently, both neurocognitive model of nightmares supported by neuroimaging results (Marquis et al., 2019) and stress acceleration hypothesis of nightmares supported by neurodevelopmental results (Nielsen, 2017) have been proposed.
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; American Psychiatric Association, 2013), repeated nightmares associated with significant clinical distress or impairment regarding social/ occupational/other important areas of functioning were symptoms of nightmare disorder. Frequent nightmares are considered as one of the disturbing sleeping problems in clinics, related to impaired concentration, bad daytime functioning, anxiety, and suicidal behaviors (Cukrowicz et al., 2006; Nadorff et al., 2014; Petrov et al., 2014). Studies also showed that nightmares had a positive correlation with depression (Bernert et al., 2005; Cukrowicz et al., 2006) and that patients with major depression reported more negative nightmare experiences and suicidal tendencies (Aǧargün et al., 1998). Patients with bipolar disorder reported more willingness to interpret the meaning of nightmares (i.e., meaning interpretation), and patients with bipolar I disorder in addition reported more terrifying activity, adventure, and violence (i.e., horrible stimulation) in their nightmares (Ma et al., 2018). Interestingly, there was an emotional continuity between dreaming and waking life; for instance, nightmare sufferers reported negative emotions during sleep as well as after sleep (Antunes-Alves & De Koninck, 2012). Consistent results showed that nightmares were related to negative physical effects (Köthe & Pietrowsky, 2001; Shen et al., 2016), and daily physical activities influenced individuals’ emotions (Netz et al., 2005). In addition, physical inactivity was a risk factor for depressive symptoms (Teychenne et al., 2008).
Interestingly, gender differences in emotional and sleep-related aspects have been documented. For instance, more increased depressive emotions were reported in women than in men (Salk et al., 2017). Both laboratory studies (Blatter et al., 2006) and population-based surveys (de Souza et al., 2018; Vallat et al., 2018) have shown worse vigilance performance in women. The dream recall frequency and nightmare frequency were consistently higher in women (Schredl & Reinhard, 2011). Moreover, the sleep duration of adult women was shorter, according to a Japanese study (Park et al., 2001).
There is an abundance of investigations focusing on mental health among the university student population, who experienced a critical period of change and a transition to adulthood, related to both future career decision and social role position (Liu & Tein, 2005). Nearly 50% of university students suffered from different types of mental problems, which might affect their educational attainments (reviewed in Hunt & Eisenberg, 2010). The major problem involved sleep-related issues, which influenced over 27% of students according to an epidemiological study (Gaultney, 2010), and over 60% of students according to an online survey (Lund et al., 2010). Scholars have reported 2.4% to 5.8% prevalence of frequent nightmares (Kelly, 2016; Schlarb et al., 2015) and 10.2% prevalence of clinical-defined nightmares with a cutoff criterion (Nadorff et al., 2011) in university students. Investigators have found an association between nightmares and psychological disturbance in university students (Levin & Fireman, 2002; Sheaves et al., 2016). In addition, in Chinese students, frequent nightmares were reported to contribute toward increased suicidal attempts (Li et al., 2010; Liu, 2004) and non-suicidal self-injury (Liu et al., 2017) and were associated with attention-deficit hyperactivity disorder (Chiang et al., 2010). In the general Chinese population, frequent nightmares were also related to the severity of depression symptoms (Li, 2014). Nevertheless, to date, to the best of our knowledge, there has been no study indicating the prevalence of nightmare disorder and the detailed nightmare experience in Chinese university students.
Based on these results, we hypothesized the following within a sample of university students: (1) women have a higher prevalence of nightmare disorder than men and (2) the more pronounced nightmare experiences, such as negative emotion and physical effect, are related to depressive mood in patients. Thus, we invited 1,451 students from a comprehensive university to complete the Nightmare Experience Questionnaire (NEQ) (Chen et al., 2014), which comprises both nightmare frequency and detailed descriptions of Physical Effect, Negative Emotion, Meaning Interpretation, Horrible Stimulation, and the Plutchik-van Praag Depression Inventory (PVP) (Plutchik & Van Praag, 1987), which measures individuals’ depressive tendencies.
Methods
Participants and Procedure
In three successful school terms, we had randomly chosen three classrooms on every floor of five teaching buildings at Zhejiang University, a typical comprehensive Chinese university with a large student population majoring in engineering, science, agronomy, medicine, humanities, social sciences, and so on. We persuaded the students in these classrooms to participate in the current study regarding their nightmares and concurrent emotional (depressive) state. We explained that our study focused on the novelty of the current design, and that our request was based on mobilizing their devotion to this type of scientific research. The participants voluntarily entered the study, and they were allowed to quit at any time.
First, we recruited a total of 1,451 students (661 men and 790 women; mean age, 20.36 ± 2.06 [SD] years; age range, 17–28 years), and we asked them to report whether they had nontraumatic nightmare(s) during their lifetime, and if yes, they were further interviewed about the nightmare frequency and its content narrations. In addition, all of the participants had to abstain from using drug or alcohol and from viewing horror videos or movies for at least 72 hr before the test. The participants reporting frequent nightmares were invited to a semi-structured clinical interview conducted by an experienced psychiatrist (W.W.). The nightmare frequency criterion for patients with nightmare disorder was at least four times per month. Of 1,451 students, 68 were diagnosed as patients with nightmare disorder according to the criteria of the DSM-5 (American Psychiatric Association, 2013).
Second, to compare the detailed nightmare experience and depressive emotions between patients and normal people, we enrolled a group of gender-matched, healthy volunteers, who were randomly selected from the participants who reported experiencing nightmares at least once or twice annually. Finally, 60 subjects with nightmare disorder (18 men and 42 women; mean age, 20.40 ± 1.82 years; age range, 18–25 years; the other eight patients failed to complete the questionnaires and, thus, were not enrolled in this group; see Results), and 124 healthy volunteers (40 men and 84 women; mean age, 20.41 ± 2.02 years; age range, 17–25 years) were included in this group. The two groups had no significant differences regarding either gender (χ2 = .10, p = .76) or age (t = .04, p = .97) distribution. The participants (patients and healthy volunteers) who had experienced traumatic events or who had alcohol or tobacco abuse, central nervous system inflammation, prior history of head injury, psychoactive substance abuse, schizoaffective disorder, schizophrenia, posttraumatic stress disorder, or other types of neurocognitive disorders were excluded. The local ethics committee had approved the study protocol (ZGL201404-2-3), and all of the participants had provided their written informed consent (guardians signed the informed consent forms for the adolescents).
Questionnaires
The participants were asked to complete the following two questionnaires in a quiet room (classroom).
1. The Nightmare Experience Questionnaire (NEQ)
The NEQ measures nightmare frequency and four factors of nightmare experience (five items each), which had been validated by procedures, including translation-back translation between Chinese and English languages (Chen et al., 2014). The scale of Horrible Stimulation portrays scenes of terrifying activity or adventure and violence in nightmares. Meaning Interpretation illustrates an effort of the dreamer to interpret the meaning of nightmares. Negative Emotion exemplifies the frightened, scared, and helpless emotions during nightmares. Physical Effect reveals a deficit of physical health, appetite, and other daily activities after nightmares. We used a 5-point Likert-type rating scale (1 = very unlike me; 2 = moderately unlike me; 3 = somewhat like and unlike me; 4 = moderately like me; and 5 = very like me) to measure the four factors. Using the four scales, internal reliabilities were previously demonstrated as .85, .80, .65, and .69, respectively, in a Chinese sample (Chen et al., 2014), and as .77, .81, .60, and .66, respectively, in the current study.
2. The Plutchik-van Praag Depression Inventory (PVP)
The PVP (Plutchik & Van Praag, 1987) consists of 34 items. Each item is rated using 3-scale points (0, 1, and 2) corresponding to increasing depressive tendencies. If the participants score between 20 and 25, they have “possible depression”; if they score above 25, they have “depression.” In a previous study (Wang et al., 2002), internal reliability was .94, and in the current study, internal reliability was .88.
Statistical Analyses
The chi-square test was applied to detect the prevalence of nightmares and nightmare disorder in different genders of the total sample. The mean NEQ scale scores in groups of those with nightmare disorder and healthy students were assessed using the two-way analysis of variance (ANOVA) (Group × Scale). If a significant main effect was found, the post hoc independent Student’s t test would be applied to evaluate between-group differences. The independent Student’s t test was also applied to the mean PVP scores and the annual nightmare frequencies in the two groups. The Pearson correlation test was used to analyze the correlation between the PVP and NEQ scales (including the annual nightmare frequency). A p < .05 was considered to be statistically significant.
Results
Among 1,451 students, 923 (prevalence, 63.61%) reported one or more nightmares annually, including 405 (61.27%) men and 518 (65.57%) women (gender effect: χ2 = 2.87, p = .09). Of 1,451 students, there were 68 (4.69%) students who were diagnosed with nightmare disorder. The prevalence of nightmare disorder in men (20 participants, 3.02%) was significantly lower (χ2 = 6.84, p < .01) than that in women (48 participants, 6.08%).
The PVP scores in the nightmare disorder group were significantly higher than those in healthy volunteers (t = 2.74, p < .01). The mean annual nightmare frequency in patients was also significantly higher (t = 9.86, p < .001) than that in healthy volunteers. The NEQ scale scores of patients were significantly higher, group effect: F(1, 182) = 43.78, p < .001, mean square effect (MSE) = 1001.11; scale effect: F(3, 546) = 273.78, p < .001, MSE = 3267.65; and Group × Scale interaction effect: F(3, 546) = 1.96, p = .12, MSE = 23.36. The post hoc analyses showed that the nightmare disorder group had significantly higher scores than the healthy volunteers on Physical Effect (t = 5.70, p < .001), Negative Emotion (t = 2.26, p < .05), Meaning Interpretation (t = 5.30, p < .001), and Horrible Stimulation (t = 4.09, p < .001) (Table 1).
Scale Scores (M ± SD) of the Nightmare Experience Questionnaire and the Plutchik—van Praag Depression Inventory in Patients With Nightmare Disorder (n = 60), and Healthy Volunteers (Controls, n = 124).

p < .05 vs. controls.
Regarding the relationships between nightmares and depression (Table 2), PVP was significantly correlated with Physical Effect in patients (n = 60, r = .26, p < .05), and with Negative Emotion in healthy volunteers (n = 124, r = .26, p < .01). For instance, when scrutinizing individual data, we found one patient with a PVP score of 26, who had a Physical Effect score of 13, a Negative Emotion score of 24, a Meaning Interpretation score of 17, and a Horrible Stimulation score of 18; and one healthy volunteer with a PVP score of 25, who had scores of 6, 21, 24, and 8, respectively, of the four NEQ scales.
Relationships (r Values, and p Values in Brackets) Between Scales of the Plutchik—van Praag Depression Inventory and the Nightmare Experience Questionnaire in Nightmare Disorder Patients (n = 60) and Healthy Volunteers (Controls, n = 124).
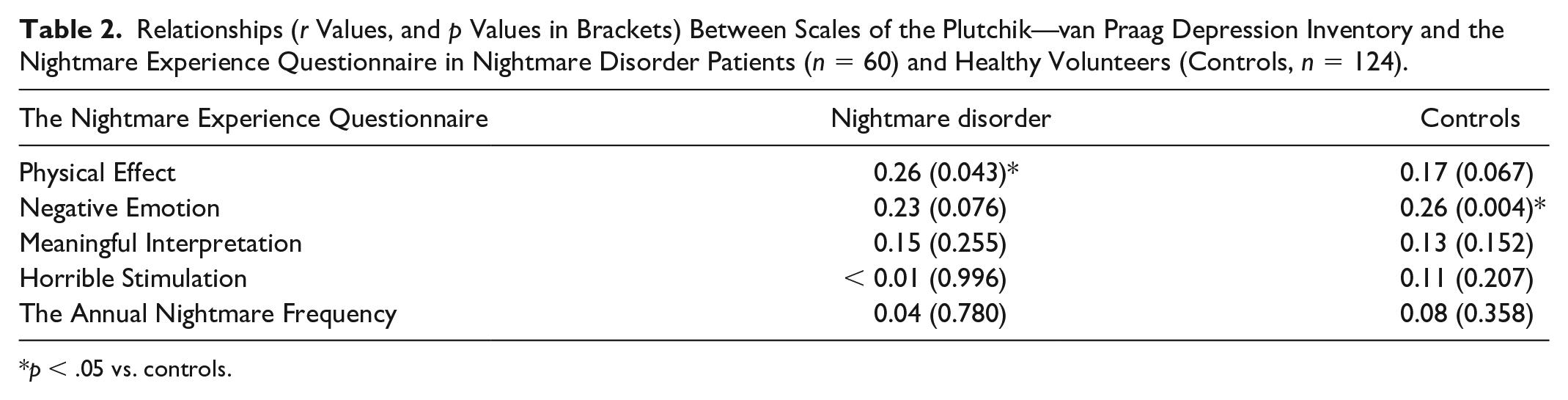
p < .05 vs. controls.
Discussion
In our study, we found a 63.61% prevalence of annual nightmare and a 4.69% prevalence of nightmare disorder in Chinese university students, which was consistent with previous findings of a 5.8% prevalence in university students with frequent nightmares (Schlarb et al., 2015). The study among the Hong Kong population reported 5.1% and 5.2% prevalence of frequent nightmares in adults and children, respectively (Li, 2014). In the Chinese population, female students experienced more nightmares than males, which was consistent with an earlier report by Schredl and Reinhard (2011). The patients with nightmare disorder had higher nightmare frequency and four scale scores of nightmare experience than healthy volunteers. The Physical Effect in patients and the Negative Emotion in healthy volunteers correlated with the depressive mood. This study is the first to report the prevalence of nightmare disorder and detailed nightmare experience in a sample of university students.
Our first hypothesis confirmed that a higher prevalence of nightmare disorder was found in women than in men. Indeed, besides poorer sleep quality (de Souza et al., 2018; Schredl & Reinhard, 2011), women reported more depressive or anxiety emotions (Salk et al., 2017), and these emotions were associated with nightmare occurrence (Bernert et al., 2005; Cukrowicz et al., 2006). In addition, women were more susceptible to childhood sexual abuse or traumatic events, which were considered as nightmare-related risk factors (Levin & Nielsen, 2007).
Our patients with nightmare disorder had higher scores than healthy volunteers on all four NEQ and PVP scales, which were consistent with previous results of more negative emotions and terror experience during bad dreams in frequent nightmare sufferers (Antunes-Alves & De Koninck, 2012). Some results also demonstrated that dreams stimulated individuals’ spirituality and creative insight (Schredl & Erlacher, 2007; Schredl et al., 2016), which might motivate such patients to engage in spiritual activities, such as interpreting the meaning of nightmares. Indeed, frequent nightmare sufferers were more sensitive to their dreams (Levin, 1994). In addition, previous studies have shown that nightmare sufferers reported more physical complaints and changes in their daily lives (Köthe & Pietrowsky, 2001; Shen et al., 2016). Furthermore, depressive moods and suicidal tendencies (Aǧargün et al., 2003; Cukrowicz et al., 2006) were reported in patients with nightmare disorder, which helps explain our patients’ higher Negative Emotion and PVP scores.
A portion of our second hypothesis has been confirmed, since our correlation results were specifically displayed in the two groups. Depression was associated with Physical Effect in patients, which was consistent with prior reports that the nightmare disorder sufferers presented more physical complaints (Shen et al., 2016) and more depressive emotion (Cukrowicz et al., 2006). Meanwhile, depression was observed to correlate with Negative Emotion in our healthy volunteers, which was consistent with previous results that occasional nightmares were related to negative mood (Köthe & Pietrowsky, 2001) or depression (Blagrove et al., 2004). Moreover, the association between depression and nightmare distress documented in college students (Nadorff et al., 2011, 2013) was also found both in our healthy volunteers and patients with nightmare disorder.
Our current study design suffered from several limitations. First, we did not enroll a comparison group of other occupations. Second, our participants were only from a comprehensive university, with relatively small sample sizes of different specialties. Third, the measurements of nightmare experience and depressive mood were influenced by recall bias. Nevertheless, we reported the prevalence of nightmare disorder and its female preponderance, and the detailed nightmare experience in a sample of Chinese university students. We believe that our findings enhance the epidemiological literature and might help to shape both basic and clinical designs to address the mechanisms of treatment and the management of patients with nightmare disorder.
Footnotes
Author Contributions
C. W., J. X., M. W., and X. S. conducted the tests, W. W. conceived the study and participated in the design and coordination of the study, and C. W., J. X., and W. W. drafted the manuscript. CW and JX contributed equally to the work described in the present paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a grant from the National Natural Science Foundation of China (No. 81771475) to the correspondent author (Dr W Wang).