
Abstract
Targeting and reducing health inequities is a requisite for public health. The Maltese Islands are divided into six geographical districts with a total area of 316 km2. It is anticipated that the close geographical proximity and social integration would result in similar population health status. This study aims to identify whether geographical health inequities exist despite the small country area. A cross-sectional health examination survey was conducted. Participants with type 2 diabetes (T2DM) and impaired fasting blood glucose (IFG) were identified, depending on their medical and drug history and fasting blood glucose levels. Those with body mass index ≥30 kg/m2 were labeled as obese. Different health status was compared between the residents in the different districts according to demographic, socioeconomic, lifestyle, and medical history. Regression analysis was carried out to identify links between the different districts, BMI, IFG, and T2DM diagnosis, while adjusting for confounders. Geographical inequities were evident despite the close proximity. The Gozo district exhibited distinctive metabolic inequities compared to the other districts. An independent relationship was present between IFG diagnosis and residence in Gozo and Northern districts. Obesity was linked to residing in Gozo. Health inequities were evident between the close districts of the Maltese Islands despite similar socioeconomic, lifestyle, and healthcare provision. Psychosocial factors might be the underlying causes for these inequities. Public health officials and government should work to enhance public education and set up local policies and interventions to target these inequities.
Introduction
Health inequities are defined as systematic, unfair, and avoidable difference among populations, both at a regional and national level, affecting their health outcomes (McCartney et al., 2019). A number of determinants have been attributed to the development of health inequities, including demographic change, geographical variations, economic conditions, social protection and security, education, lifestyle and health behaviors, physical environment, built environment, road safety, healthcare resources, and expenditure and healthcare performance (Marmot, 2016; Santana et al., 2017). The presence of health inequities within European countries have long been reported for the past decades (Mackenbach et al., 2018). No country, large or small, is immune to the presence of health inequities. Even the Nordic countries, known for their advanced welfare states, are subject to large health inequities, equivalent to those of other European countries (Mackenbach, 2020). Targeting health inequities is a priority for Europe, both at a national and European Union level (The Lancet Public Health, 2019; van Den Broucke et al., 2013). Indeed, the EURO-HEALTHY project was an initiative set up to evaluate and compare the determinants of the health inequities as well as monitor the health outcomes across the different regions of the European member states (Nomenclature of Territorial Units for Statistics (NUTS) classification). It also developed the “Population Health Index (PHI)” as a metric to measure and compare health inequities determinants and outcomes between European countries (Santana et al., 2017). Of note, the NUTS levels in small geographical countries, such as Malta, are the same, therefore the PHI does not allow to identify inequities.
Spatial inequities are defined as the unequal distribution of services and resources across different areas or locations. These inequities are linked with health and social inequities that affect the population (Kanbur & Venables, 2005). In Europe, spatial inequities have been reported to originate from various health determinants and evident between the Northern, Southern, and Eastern regions, with the Northern countries exhibiting a better general population health (Santana et al., 2017). Additionally, regional inequities have been reported within large islands including the United Kingdom (McCann, 2020) and New Zealand (Pearce & Dorling, 2006), as well as within aggregation of islands including the Pacific (Matheson et al., 2017) and Comoros Islands (Kassim et al., 2017). Small countries and islands may also be subject to spatial health inequities. To our knowledge, spatial health inequities have never been investigated in the smaller geographical area islands of Malta. This study aimed to investigate the health status (through common non-communicable diseases) across the different districts making up the Islands of Malta and to assess whether geographical health inequities exist despite the short distances and population homogeneity.
Characterization of the Population and Regions of Malta
The Maltese islands, situated in the middle of the Mediterranean Sea, constitute an archipelago covering a total surface area of 316 km2, making it one of the smallest European nations with a total population of 493,559 (National Statistics Office [NSO], 2020). There are two main inhabited islands, Malta and Gozo, separated only by a 20-minute ferry ride. The Maltese Islands are divided into 6 geographical districts. Malta is divided into five districts while Gozo constitutes one other district. Figure 1 illustrates the different districts and their total population while Supplemental Table 1 provides the districts demographic characteristics (NSO, 2020). The Northern Harbor district is the most densely populated district and has a higher proportion of elderly population than the other districts. The Northern Harbor district also houses one of the most deprived residential areas in Malta (Satariano, 2019). In 2018, the population residing in the Northern Harbor, South Eastern, and Northern districts had the highest number of persons-at-risk of poverty (NSO, 2020). Indeed, a town situated within the Northern district was also established to be a deprived residential area (Satariano, 2019).
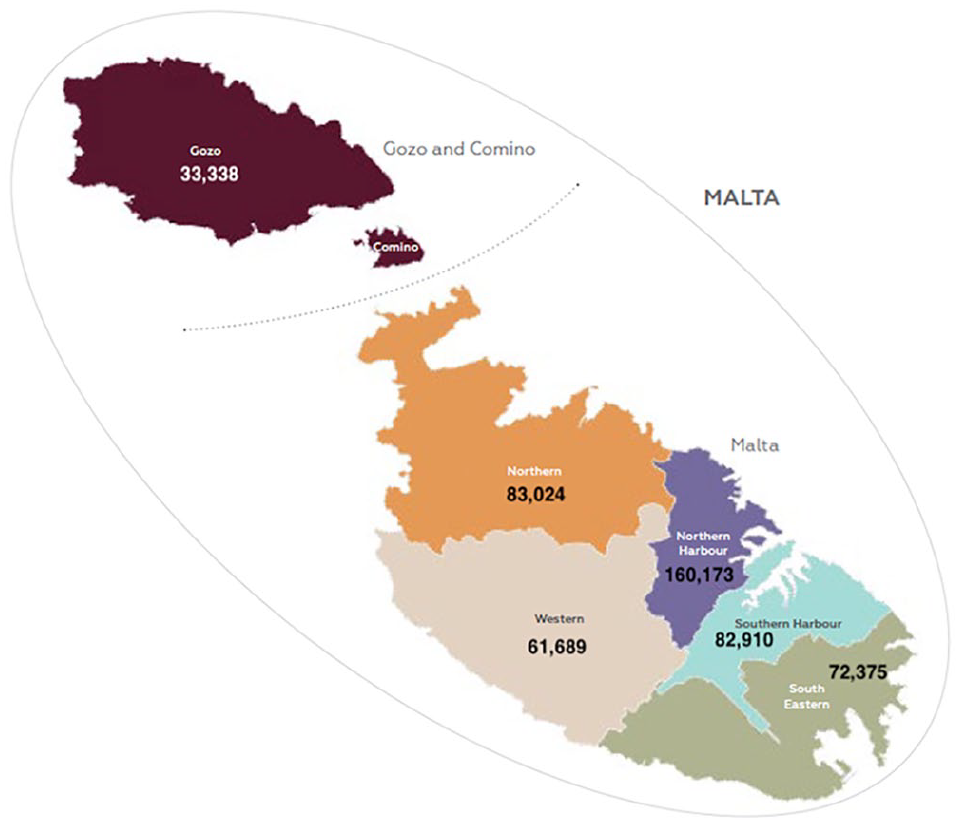
The different districts making up the Maltese Islands and their respective total population (NSO, 2020).
The six districts have designated areas for factories and industrial zones. Although they provide a substantial proportion of employment, these zones inevitably, are a source of air pollution (Alshuwaikhat, 2005). It is important to note that most of these industrial zones are located within a 1 or 2 km of the urban residential areas. Conversely, the power plants for energy generation supplying the whole Maltese Islands and the International trade port (Freeport) are situated in an isolated area in the South Eastern district.
Healthcare Access Across the Maltese Islands
The healthcare system of Malta is government dependent and plays an important role in the health and wellbeing of an individual, community, and country level. The Maltese healthcare system is easily accessible to all residents as the state offers free primary healthcare through 10 health centers distributed across the islands (nine in Malta and one in Gozo). These centers offer a variety of services to the community varying from specialist consultation clinics to radiography, physiotherapy and performance of minor operations. Furthermore, an acute hospital with an adjoining accident and emergency department is situated on each inhabited island. Mater Dei Hospital, found within the Northern Harbor district, caters for all the inhabitants of Malta and is situated within 13 km of the furthest town (situated in the Northern district). Gozo General Hospital caters for the inhabitants of Gozo and is situated under 6.5 km away from the furthest town on the island. All state health services are free of charge to permanent and employed residents. The private sector also offers all types of services (accident and emergency services, primary care and tertiary care) on a fee-for-service basis (Azzopardi-Muscat et al., 2017). The accessibility to outpatient clinic services and surgeries is perceived as good with the waiting lists been substantially reduced as a general trend across specialties from years to couple of months (World Health Organization [WHO], 2019). Hence, one can postulate that health care access, which is a determinant of health, is well provided within the Maltese Islands, should the individual seek medical help (De Vogli et al., 2007). In fact, the 2014–2015 Maltese European Health Interview Survey (HIS) reported that a substantial proportion of the population visited both primary care and secondary care within a period of year (Directorate for Health Information and Research, 2018).
Health Status in Malta
The average population health index (PHI) for various determinants in Malta was reported to be 61 out of 100, with obesity as the leading contributing determinant. This index is a comparable score to the nearby islands of Sicily (PHI 59) and Sardinia (PHI 65) (Santana et al., 2017). A nationally representative cross-sectional study (2014–2016) conducted among the Maltese adult population (18–70 years) reported that 30.12% suffered from hypertension, 10.31% had type 2 diabetes, 69.75% had an overweight-obese status, 26.30% had the metabolic syndrome while 19.26% had dyslipidemia (Cuschieri, 2020; Cuschieri, Vassallo, Calleja, Camilleri, et al., 2016; Cuschieri et al., 2017a, 2017b, 2018). Evidence is lacking in Malta on the different determinants contributing to the development of these non-communicable diseases (NCDs) among the population. Indeed, recently the Ministry of Health of Malta established a “Social Determinants of Health Unit” with the aim to tackle health inequities (Gauci, 2018). Concurrently, a nationally representative survey conducted by the University of Malta, targeting NCDs among the adult population of Malta has been recently concluded and can provide evidence on potential spatial health inequities associated with common NCDs in Malta.
Methods
Data Sampling and Recruitment
A nationally representative health examination survey was conducted (2014–16) using the European Health Examination Survey (EHES) guidelines (Finnish Institute for Health and Welfare, 2019) in order to assess the noncommunicable disease situation in Malta. Using PiFace software® with a maximum allowed confidence interval of ±5% while considering achieving a 50% response rate, a total sample size of 4,000 people was required. This represents 1% of the total Maltese population. A single staged random process was performed to obtain a stratified sample population (by age 18–70 years, sex and district) from the national passport registry. The participants that were randomly selected were invited to participate in this survey through a postal letter sent to their home address. Those that accepted the invitation were asked to attend examination hubs that were set up in their hometown. This enabled the accessibility to the examination hub and enhanced the response rate. Participants were asked to complete a socio-demographic, medical history (self-reporting the presence/occurrence of coronary heart disease, myocardial infarction, hypertension, hypothyroidism, dyslipidemia) and medication validated questionnaire with a trained interviewer, followed by blood pressure, weight, height, and waist circumference measurements. Blood samples for fasting blood glucose (FBG) and lipid profile were also taken at the end of the examination. A detailed description of the protocol can be found elsewhere (Cuschieri, Vassallo, Calleja, Pace, et al., 2016).
The response rate was 47.15%. A weighting factor was applied to the responding population (n = 1,861) to maintain national representation, using the IBM SPSS® version 21 software. The method used considered the respondents and non-respondents for each town by age and sex. Weights were derived by multiplying each participant (by age and sex) by the ratio of the total sample size to the total population size within each town. Ultimately, each participant was representative of approximately 1% of the population of each Maltese town by age and sex. The weighed data (total adjusted/weighted study population of 3,947) was used for national representative population descriptions.
The Research Ethics Committee of the Faculty of Medicine and Surgery at the University of Malta together with the Information and Data protection commissioner gave their permission for this study. All participants gave their informed written consent prior to participating in the survey. Each participant was given a unique code so no identifying data was available during and after the data collection. Only the principal researcher had access to the personal identifiable information of each participant.
Definitions
Our independent variables were the presence of obesity, impaired fasting glucose and type 2 diabetes. Body mass index (BMI) was calculated from the measured weight and height. An overweight status was considered as BMI between 24 and 29.99 kg/m2 while an obese status as a BMI above or equal to 30 kg/m2. Participants with an examined FBG between 5.60 and 6.99 mmol/L with no self-reported history of T2DM or on medication were labeled as impaired fasting glucose (IFG). Participants with a self-reported history of type 2 diabetes (T2DM), on oral hypoglycemic agents (self-reported) or scoring an FBG above 7 mmol/L during the examination were labeled as T2DM. An elevated LDL-C level was considered as ≥3 mmol/L, while the total cholesterol lower limit cut off point was of ≥5 mmol/L (Hockley & Gemmill, 2006).
As socio-economic variables, we used educational levels and employment status. The survey used did not include parameters for income therefore educational and employment status were used as a proxy for socio-economic status. The categorical definition for education followed the ISCED-1999 criteria (OECD, 1999). Hence, education was categorized into levels as follows: no formal education, primary education level, unfinished secondary level, finished secondary level, tertiary level, university level and postgraduate level. Employment status was categorized into employed, unemployed, retired, student, and domestic task.
As lifestyle variables, we used alcohol consumption and smoking habits. Considering that the majority of the study population reported to consume one to two glasses of alcohol per week, for the purpose of this study, alcohol consumption was defined as an average consumption of at least one glass of an alcohol beverage per week over a period of 12 months. Participants reporting smoking more than one cigarette per day were considered as “smokers” while those that stopped smoking for more than a year were considered as “non smokers.” Smokers reporting to have stopped smoking for less than a year were still considered as “smokers.” This definition of the subgroups was based on the WHO report that stated that up to 1-year post cessation, smoking related symptoms are still evident (WHO, 2013).
Statistical Analysis
First, we compared the six districts of Malta by (1) socio-economic status (self-reported education level and employment status); (2) diagnosed medical conditions (Obesity, IFG and T2DM); (3) self-reported lifestyle behaviors (smoking and alcohol habits); and (4) history of medical comorbidities.
This was followed by univariant analyses (Model 1) through generalized linear modeling. Model 1 measured the association between each dependent variable (obesity, IFG, T2DM) and districts (independent variable).
Multivariant analyses (Model 2) through a backward stepwise logistic regression was performed in order to establish associations between the significant univariant independent factors and the different districts while adjusted for potential effects from demographic, socio-economic and lifestyle variables (age as continuous variable, gender, education level, employment status, smoking, alcohol and BMI status) (Hocking, 1976). Model two was performed twice; (i) considering the Southern Harbor district as the reference category and (ii) considering all districts of Malta as the reference category. The Southern Harbor district was observed to have generally normal biochemical and anthropometric parameters and hence this district was considered as an appropriate reference category for modeling purposes. The second modeling set was performed to assess the association between the Gozo district as opposed to the Malta districts.
Quantitative data analyses and modeling were performed using IBM SPSS (IBM Corp. Release 2012 Version 21). A p-value of <.05 was considered significant. Where applicable a 95% confidence interval (CI) was provided.
Results
Study Population Characteristics
The study population was stratified according to their residing district and homogeneity was observed by gender (p = .98), ethnicity (p = .88), and employment status, with the majority being employed (p = .18). The majority of the study population was younger than 50 years of age across all the districts. Although the commonest reported education level across all the six districts was education up till secondary school, differences in population proportions across each education level were noted (p ≤ .01). Indeed, the Gozo district exhibited the highest population proportion reporting to have finished an undergraduate and a postgraduate degree (34% of the Gozo district) when compared to the rest of the five districts (Southern Harbor 17%; Northern Harbor 28%; South-eastern 21%; Western 26%; and Northern 30%). The socioeconomical characteristics of the study population stratified by districts can be found in Supplemental Table 2.
Similar trends in lifestyle behaviors were observed across the six districts. A predominant “no smoking” habit was present across the six districts. Conversely, alcohol consumption was more prevalent across these districts (p ≤ .01). A distinctive prevalent gap was observed for the Gozo and Western districts, where the majority living in these districts reported to consume alcohol as illustrated in Figure 2.
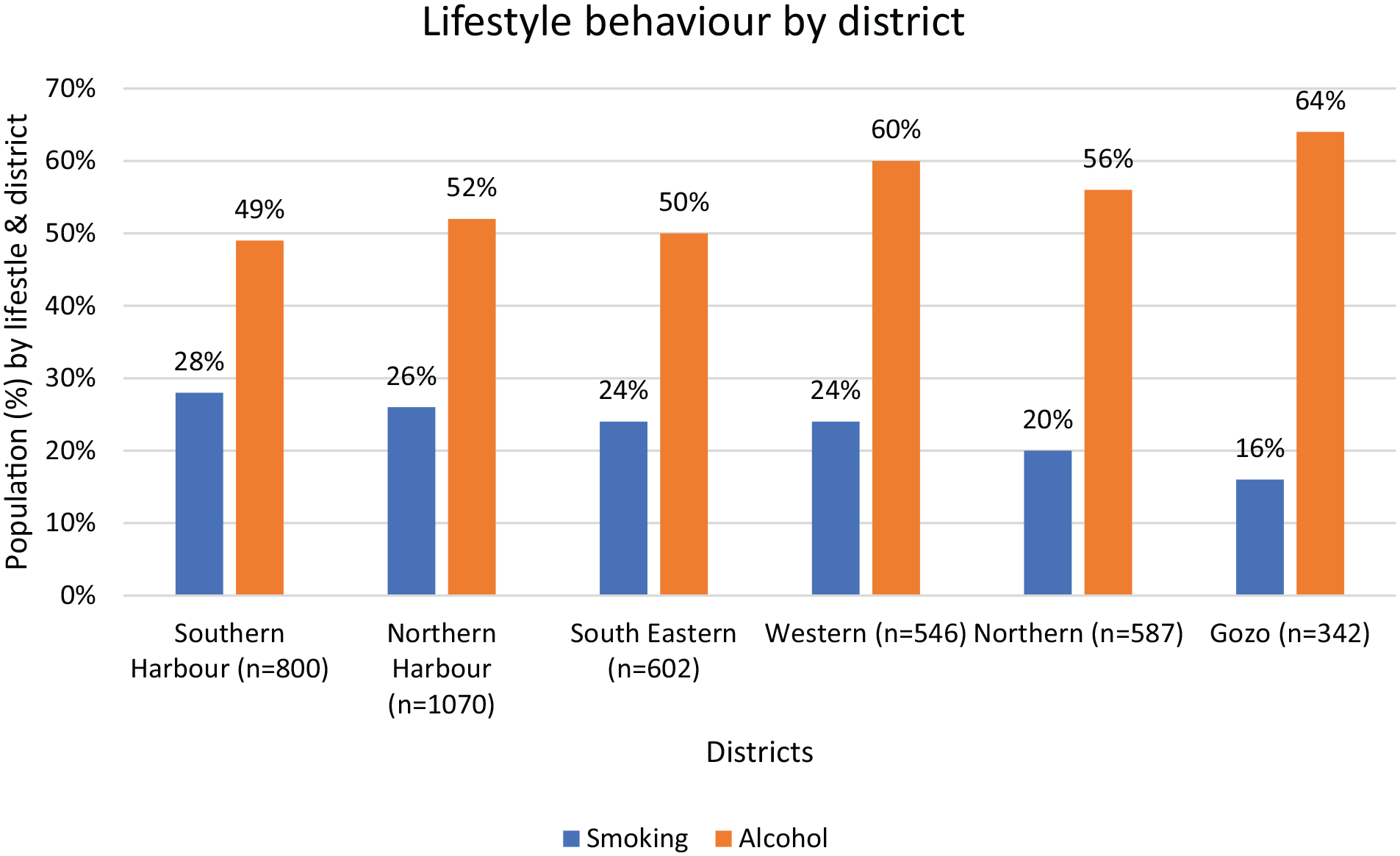
Distribution of lifestyle behavior by districts.
Metabolic Inequities
The residents of the district of Gozo self-reported the highest cardiovascular (11.12%) and dyslipidemia (29.82%) comorbidities. Meanwhile the Western district had the highest self-reported diabetes (8.79%) prevalence (Table 1). It is important to note that Table 1 only illustrates the self-reported medical history and does not take in consideration the results from the health examination. This survey’s biochemical testing revealed that the district of Gozo had the highest population proportion with high LDL-C levels (p ≤ .01), high total cholesterol levels (p ≤ .01) and fasting blood glucose (FBG) within the impaired fasting blood glucose range (5.60–6.99 mmol/L) (p ≤ .01), as seen in Figure 3. This coincided with the self-reported histories provided by the Gozo district population. On considering the dysglycemic (IFG and T2DM) examined results along with the self-reported histories (as per definition in the methods section) the total prevalence for each district of dysglycemic profiles can be seen in Figure 4. It is noted that the Gozo district had the highest IFG prevalence (p ≤ .01) and the second highest T2DM prevalence (p ≤ .01) when compared to the rest of the districts. A stronger obesity occurrence was observed in the Southeast, Western and Gozo districts, as seen in Figure 5.
Distribution of Self-Reported Medical Comorbidities, by Districts.

Chi square value indicate the differences between the different districts and each self-reported medical history.
The bold values indicate the significant comparisons.

Distribution of the prevalence of the measured abnormal biochemical parameters, by district.

Distribution of the prevalence of the different dysglycemic profiles, by districts.
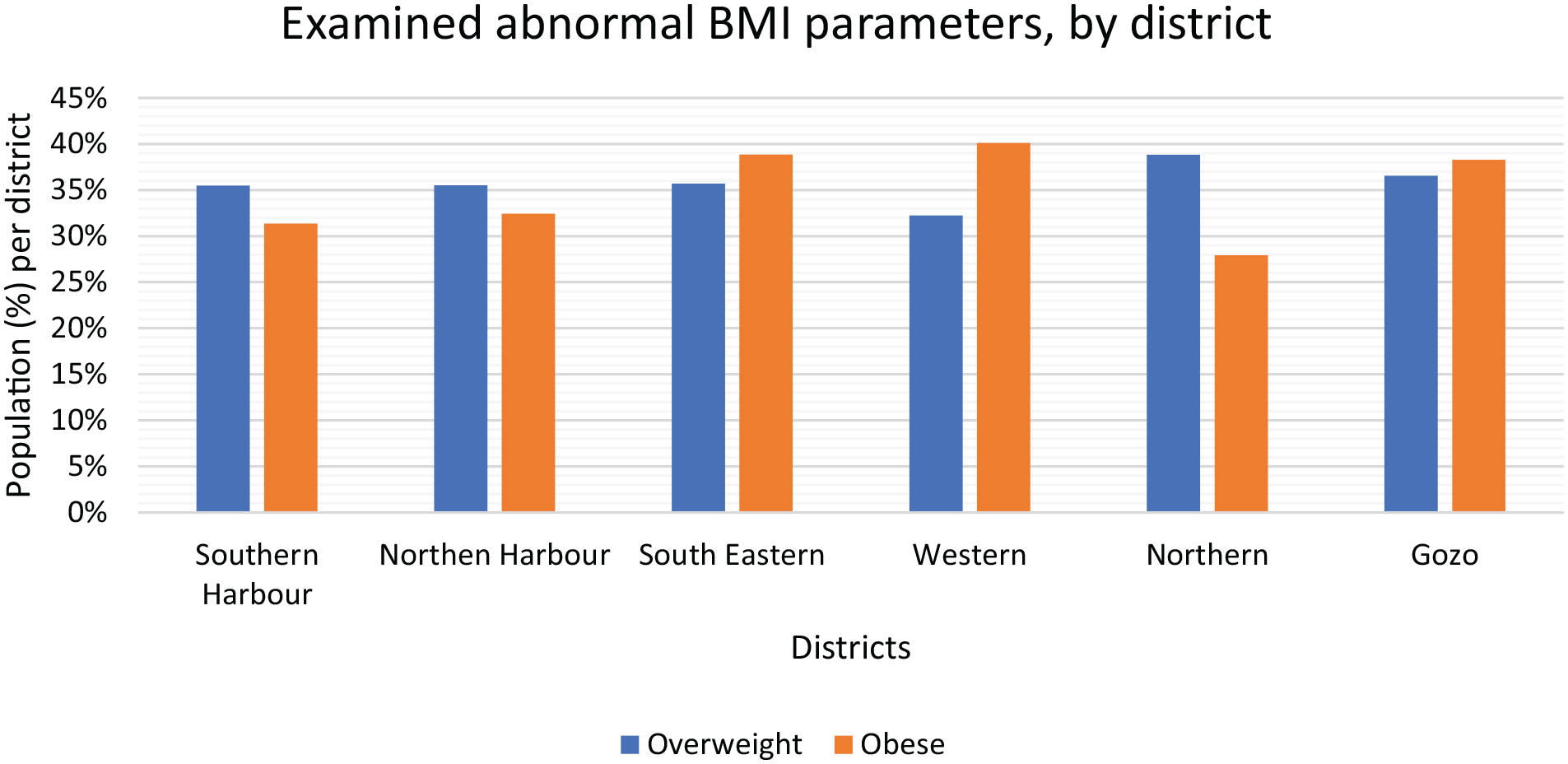
Distribution of abnormal body mass index (BMI) proportions, by districts.
Modeling
On performing univariate logistic regression modeling, the residents of Gozo had a 44% increased likelihood of being obese, when compared to the Southern Harbor (reference category). This association was enhanced on adjustment for potential confounding factors after performing backward stepwise multivariate logistic regression modeling (OR: 1.64; 95% CI: [1.25–2.16]), as seen in Table 2. A similar association was present for both the Western (OR: 1.65; 95% CI: [1.30–2.10]) and South Eastern (OR: 1.55; 95% CI: [1.23–1.95]) districts (Table 2). The link between the district of Gozo and obesity was still present when compared to all of the other Malta districts after adjustment (OR: 1.38; 95% CI: [1.09–1.75]) (Table 2).
Multiple Regression Models Between Districts and Different Medical Conditions.

Note. Obesity Model 2: adjusted for age, gender, education level, employment status, smoking, and alcohol habits. IFG & T2DM Model 2: adjusted for age, gender, BMI, education level, employment status, smoking, and alcohol habits.
p ≤ .01. **p < .01. ***p < .05.
The population of Gozo also exhibited an independent association with having an IFG diagnosis when compared to the Southern Harbor (OR: 4.00; 95% CI: [2.99–5.37]) as well as when compared to the combination of all the Malta districts (OR: 3.45; 95% CI: [2.39–4.99]) (Table 2). Similarly, the Northern district had an independent association (OR: 1.31; 95% CI: [1.00–1.71]) with having an IFG diagnosis when compared to the Southern Harbor (Table 2).
Of note, none of the districts exhibited any marked association with having a diagnosis of T2DM (Table 2).
Discussion
This study set out to explore spatial health inequities between the six districts of the Maltese Islands and common non-communicable diseases (NCDs) despite the short geographical distances. Indeed, a number of non-communicable diseases leading to health inequities were evident within the close districts of the Maltese Islands, especially for the district of Gozo. The Maltese Islands, like the rest of the world, are in a constant struggle to control the growing non-communicable diseases epidemic. Hence, establishing such discrepancies across short geographical distances raise concerns. It needs to be appreciated that the demographic area of this country (316 km2) is smaller than most European cities such as Greater London (1,572 km2), Rome (1,285 km2) and Berlin (1,347 km2) among others.
A number of different factors and determinants of health can contribute to health inequities, including socioeconomic factors, physical and social environments, health behaviors, and access to healthcare (De Vogli et al., 2007; WHO, 2008). Hence, in this study we tried to assess for the various reported determinants (demographic, socioeconomic, health behaviors). Additionally, “environmental” factors including the effect of pollution, physical risks as well as lack of resources might influence health and its outcomes (Arcaya et al., 2015).
Health Inequities in the Gozo District
The district comprising the island of Gozo is separated from the other five districts by a short ferry ride and is known for its more rural environment and tranquility compared to the Malta’s districts (Visit Malta, 2020). Even though health inequities were evident across the Maltese Islands districts, the Gozo district exhibited a predominance for such inequities. There is a lack of local evidence pertaining to the differences in health and wellbeing between both islands, so assumptions based on international literature are being presented here.
Socioeconomical Factors
The population social gradient, measured in this study through the socioeconomic indicators of education and employment, has also been linked with health outcome. There is a positive correlation between educational level and health, with the higher the education level the better is the level of health (Marmot & McDowall, 1986; Marmot et al., 1991). The adult population residing in the Gozo district reported the highest university and post-graduate education levels when compared to the other districts. However, on conducting association studies, health inequities in Gozo were still apparent even after adjusting for education levels, suggesting that other underlying determinants are contributing to these inequities.
Behavioral and Psychosocial Factors
Behavioral differences are known to contribute to health inequities (Arcaya et al., 2015). It was assumed that homogenous behavioral characteristics would be present within the Maltese Islands considering the short distances and social integrations across the districts. However, again the Gozo district reported the lowest tobacco smoking rates but the highest population proportion with an alcohol consumption habit. Although in the association studies, on adjusting for alcohol consumption, health inequities were still significantly evident. Other determinants such as psychosocial factors and stress may be the contributing factors for the health inequities in Gozo. Indeed, as discussed below, the Gozo population is faced with a higher level of psychosocial problems than the other Maltese districts residents (Marmot & Bell, 2019). In fact, health inequities are also explained through psychosocial factors where stress, depression, hostility, low social support among others, play a role in the health outcome with a particular association with heart diseases (Cassel, 1976; Hemingway & Marmot, 1999; Marmot, 1998).
The physical separation of both islands (Malta and Gozo) could be resulting in a negative psychosocial impact on the Gozo population. The main island is Malta, where higher educational institutes (such as the University of Malta) and the highest employment opportunities are situated. Hence, a substantial proportion of the Gozitan population need to commute daily or weekly between Gozo and Malta for work and schooling. This internal migration brings with it a number of hardships to the involved Gozitans, unlike the Maltese, including but not limited to; very early rising, fatigue, costs of traveling, wasted time in traveling, separation from family and accommodation costs when compared to the Malta residents (Mizzi, 1988). In fact, a Gozitan commuter requires an estimated additional 3 hours commuting time on top of the normal Maltese commuter time to go to work and return back home on a daily basis. Such a lifestyle “stressor” may lead to a disturbed biological stress response leading to increased inflammation as well as blood pressure (McEwen, 2006; Rozanski & Kubzansky, 2005). Altered circadian rhythms may also occur, which are associated with an increase in blood pressure, in heart rates as well as in an increased predisposition to cardiovascular disease, diabetes and obesity (Farhud & Aryan, 2018; Muller et al., 1989). In fact, this coincides with the Gozo population metabolic abnormalities observed in this study.
It must be noted that during the same timeline of this national study, the Maltese version of the European Health Interview Survey (EHIS) was being conducted. The EHIS involves dissemination of an interview questionnaire among representative population without undergoing a health examination. Both EHIS and this national study (combination of a health examination and interview questionnaire) followed the same sampling process and represented 1% of the population. The EHIS survey reported the district of Gozo had the highest “very good self-perceived health” when compared to the other districts (Directorate for Health Information and Research, 2018). However, when considering that this national study was conducted during the same period as the EHIS, the examination results obtained (this study) showed an opposite picture to the perceived health status (EHIS). This is a public health concern since these health inequities might be originating from the fact that the Gozo population might be perceiving their health as being good and residents do not undergo regular check-ups. These metabolic inequities were observed by means of self-reported comorbidities as well as through measured parameters (lipid profile, impaired fasting glucose, type 2 diabetes, and body mass index). Another explanation could be that unless the Gozo population are provided with a clear disease diagnosis, such as having type 2 diabetes, just having risk factors for NCDs such as an impaired fasting blood state or an obese state, they still perceive their heath as good. Hence, they may opt to follow an unhealthy dietary and/or behavioral lifestyle. In fact, residing in Gozo appeared to have an independent association with an obese status and an impaired fasting blood glucose (IFG) diagnosis, although no associations were present with T2DM. This raises the question as to whether a psychosocial and geographical health inequality might be the predisposing factors to such findings.
Environmental Factors
It has been reported that an inverse relationship exists between the level of health and sources of air pollution (Arcaya et al., 2015). Within the Maltese Islands, all major sources of pollution including both electrical power stations, waste collection and recycling areas are situated on the island of Malta in close proximity to the urban zones. The district of Gozo has one main industrial estate, which is relatively smaller in size when compared to the other districts’ industrial zones. Thus, considering the effect of air pollution as a source of health inequities as previously established (Yang & Liu, 2018), the Gozo district is expected to exhibit less health inequities and a better health outcome than the rest of the districts, which is the contrary to this study’s findings.
Spatial Health Inequities
It is difficult to determine the exact reason/s for the findings of our study, but this has very important implications for public health since it supports the presence of health inequities between short geographical distances. This evidence is not only essential for other small countries but also for larger countries inter-regional policies and strategies planning.
Public health education in Malta for both public health trainees and general practitioners especially those planning to work in Gozo, should focus on geographical and environmental differences and the evident health inequities. This is even more important for the medical students training in the Gozo General Hospital, as now it has its own separate medical school. Medical graduates from this university may henceforth be more likely to spend their internship and possibly enter family medicine specialist training in Gozo. Therefore, these shall be assumed to be taking care of Gozitan patients during their training. Furthermore, it is important that a national effort to close the gap in health inequities is set up, to improve population health and inevitably reduce the healthcare costs, budgets as well as improve the conditions in which people are born, live, work and age (Donkin et al., 2018; WHO, 2008). A whole-of-government and whole-of-society approach to address health inequities is suggested. As observed in this study, local policies are recommended to aid in closing the health inequities gap. One recommendation is to decrease commute times (by building bridges, better roads, railways, public transportation), which in this study’s setting, may be a pinnacle policy to decrease health inequities. Another initiative may be the provision of subsidiaries for Gozitans to rent property in Malta for residential purposes. Local health screening programs may be considered to target metabolic abnormalities from an early age among the adult population of the Gozo district. Also, setting up of specific interventions such as focusing on promoting physical activity by improving public spaces, may be another initiative worth considering. Further research is recommended focusing on potential health inequities differences between Gozo residents that work in Malta and Malta residents that work in Gozo, with special consideration on the different occupations that may lead to different degrees of health inequities.
Some strengths and limitations regarding the data being presented here include the response rate of 47.15%, which was considered as an adequate one considering the invasive measurements performed. When compared to other European Health Examination surveys such as the Czech edition of the European Health Examination Survey (EHES) and the better-established SHeS in Scotland, the Malta response rate was similar or higher than these (Čapková et al., 2017; Scottish Government, 2016). The sociodemographic, behavioral characteristics and comorbidities data were self-reported. Recall bias may have been present when reporting medical comorbidities. The definition used for alcohol consumption in this study follows a broad definition due to data constrains. Such definition could have had an effect on the analyses and outcomes of the study. Some variable categories had a small sample size and could have affected the study’s results and interpretations, with potential type 2 errors. Temporal relationships could not be accessed due to the nature of this cross-sectional study. Data on household income, total income, and income per family member was not available, therefore unable to explore whether income was the potential contributing factor in this study’s findings. This is the first study to attempt investigating geographical health inequities in Malta, hence potential reasons for their existence are based on international literature rather than on local studies. In this respect, other potential causes for health inequities could have been present but may not have been recorded or considered. Although the EHIS and the current study were conducted in the same time period, it is highly unlikely that the persons from the same sample were under study. It is recommended that a longitudinal cohort study be conducted to clarify which conditions may be challenging the health outcome of those less privileged within the Maltese Islands and leading to the established health inequities.
Conclusion
To our knowledge this is the first study to attempt to address the determinants of health in Malta through geographical health inequities. This study established that despite the short geographical distances, similar social and environment factors, health inequities are still evident. Associations were confirmed between geographical districts and health conditions, namely with obesity and impaired fasting glucose. Hence, there are no geographical boundaries to health inequities, and it is essential to understand the effects of subnational social and environmental modifiers. Public health training should give consideration to such demographic differences during educational programs to public health and general practitioners. This is especially paramount for the district of Gozo, where metabolic abnormalities predominated. Public health officials should work to enhance public education, local administration and schools to set up policies and interventions that are locality specific, such as promoting physical activity by improving public spaces.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440221082123 – Supplemental material for Health Inequities Exist in Europe: Are Spatial Health Inequities Present in the Small State of Malta?
Supplemental material, sj-docx-1-sgo-10.1177_21582440221082123 for Health Inequities Exist in Europe: Are Spatial Health Inequities Present in the Small State of Malta? by Sarah Cuschieri, Neville Calleja and Julian Mamo in SAGE Open
Footnotes
Acknowledgements
The authors are extremely grateful for the strong support forthcoming from the University of Malta (through the Medical School and Research Innovative Development Trust department) and from the Alfred Mizzi Foundation as major sponsors, as well as that of a host of others, including Atlas Health Insurance (Malta). The in-kind support and encouragement of the Parliamentary Secretariat for Health of the Government of Malta is also gratefully acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was obtained from the University of Malta, Alfred Mizzi Foundation and Atlas Insurance (Malta). Funding had no role in the design of the study, analysis, and interpretation of data and in writing the manuscript.
Permissions
The Research Ethics Committee of the Faculty of Medicine and Surgery at the University of Malta together with the Information and Data protection commissioner gave their consent for this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.