
Abstract
Public education campaigns are recommended to increase awareness for stroke. The effect of a public advertising and education campaign in an urban region in Germany was assessed and compared with a control region. We hypothesized that such a campaign would increase the number of patients being admitted by emergency medical services (EMS). A multimedia campaign and targeted education of health care professionals and the public was employed in Berlin during six consecutive months to disseminate knowledge about stroke symptoms and appropriate actions to take. Data on time to hospital admission and details on transport were retrieved from registries for the episode before, during, and after the campaign. To test the effect of the campaign, it was compared with another urban region in Germany (Ruhr-Area), where no campaign had been conducted. Between January 2010 and February 2011, 9,166 patients with stroke or transient ischemic attack (TIA) were documented in Berlin and 9,994 in the Ruhr-Area. In both regions, following the campaign period, patients were more often admitted to hospital within the first 2 hr after onset (Berlin: odds ratio [OR] = 1.16, 95% confidence interval [CI] = [1.02, 1.32]; Ruhr-Area: OR = 1.18, 95% CI = [1.05, 1.34]). Patients were more likely being admitted via EMS after the campaign (Berlin: OR = 1.71, 95% CI = [1.50, 1.94]; Ruhr-Area: OR = 1.34, 95% CI = [1.17, 1.53]). The results suggest that an increased uptake of EMS triggered shorter time to hospital admission. A reduction in delay to hospitalization and an increased uptake of EMS were observed over the study period for both regions. No effect of the campaign was identified.
Introduction
Stroke is a medical emergency requiring immediate hospitalization for initiating appropriate diagnosis and treatment (Jauch et al., 2013). Despite increasing knowledge about effective but time-critical stroke therapies within the general population (Minnerup et al., 2011), most studies did not observe substantial improvement in time from symptom onset to hospital arrival within recent years (Heuschmann et al., 2010; Tong et al., 2012). In addition, previous reviews showed poor knowledge of stroke symptoms in low- as well as high-risk populations (Jones et al., 2010; Stroebele et al., 2011). There is evidence that mass media campaigns (MMCs) are able to increase knowledge of stroke signs in the population (Lecouturier et al., 2010). Thus, several guidelines recommend regular educational programs targeting the general public as well as health care professionals to improve stroke knowledge. These programs aim at shortening time from stroke onset to hospital arrival (Jauch et al., 2013). However, previous studies evaluating the effectiveness of MMCs showed mixed results (Advani et al., 2016; Denti et al., 2017; Folyovich et al., 2018; Hodgson et al., 2007; Morgenstern et al., 2002), indicating further need to test effects of MMCs on pre-hospital delay (Lecouturier et al., 2010).
This analysis aimed to investigate the effects of a comprehensive MMC dedicated at informing the general public as well as health care professionals on stroke signs, symptoms, and actions in a defined urban region in Germany. We hypothesized that such a campaign would increase the number of patients being admitted by emergency medical services (EMS) and would also increase the number of patients arriving early (i.e., within 2 hr after onset) in the hospital. Hence, effects on time from onset to hospitalization and the means of transportation to hospital were compared with another German region of similar size without a dedicated MMC.
Patients and Methods
Study Regions
Intervention region Berlin
A comprehensive multimedia campaign named “Berlin gegen den Schlaganfall” (free translation: “Berlin fighting stroke”) was employed in Berlin (source population 3.4 million inhabitants) with an estimated number of 12,300 patients with first or recurrent stroke or transient ischemic attack [TIA] per year (based on epidemiological study estimates; Kolominsky-Rabas et al., 1998). Data of acute stroke or TIA patients were collected within the Berlin Stroke Register (BSR), a network of 15 acute stroke units in the city of Berlin (Grube et al., 2012). All BSR hospitals treat stroke patients independent of age, sex, comorbidities, and stroke severity. Data from consecutively admitted patients with acute stroke or TIA within the last 7 days prior to admission were collected prospectively as part of a regional program for quality assurance. The BSR is part of the German Stroke Registers Study Group (ADSR), a network of regional hospital-based stroke registers for quality assurance in Germany with standardized methods and definitions (Heuschmann et al., 2006).
Effects of the campaign were investigated by analyzing time from symptom onset to hospitalization and pre-hospital management before, during, and after the campaign, and comparing the results with a control region of similar size where no dedicated campaign took place.
Control region Ruhr-Area
The control region was the North-East of the Ruhr-Area (source population about 3.0 million inhabitants) comprising an estimated number of 12,200 patients with first or recurrent stroke or TIA per year (based on epidemiological study estimates; Kolominsky-Rabas et al., 1998). Within the North-East Ruhr-Area, 19 hospitals provide acute stroke care, including 15 stroke units. Data were collected according to the methods and definitions of the Stroke Register North West Germany (NWSR), being also member of the joint working group of german-speaking countries (Arbeitsgemeinschaft Deutschsprachiger Schlaganfall-Register [ADSR]). Thus, identical data definitions and data collection methods were used.
Multimedia Campaign
The media campaign “Berlin fighting stroke” covered a 6-month period from May 10 (National Stroke Day) to October 29, 2010 (International Stroke Day). The campaign aimed to inform the general public as well as health care professionals on stroke signs and symptoms and correct action by various approaches, including, for example, print media, local broadcast, internet and poster presentation, scientific lectures open to the general public or targeted at health care professionals, cultural events, and presentations in public events. Details of the comprehensive multimedia campaign are shown in the online supplement.
Within the control region, no dedicated MMC took place during the study period. As in previous years, local, mainly 1-day activities were performed sporadically. Examples are lectures for the general public and a skater night during the annual national and European stroke awareness days in May and October, respectively. In May 2011 (after the end of the MMC evaluation), a network structure (Neurovascular Net Ruhr) among 27 neurology departments in the whole Ruhr-Area was formally established and a 4-week information campaign started in the region.
Data Definition
In the present analyses, the following variables were used: age, gender, pre-stroke living condition, stroke subtype, comorbidities (hypertension, diabetes mellitus, atrial fibrillation, and previous stroke), National Institutes of Health Stroke Scale (NIHSS), time from stroke onset to hospitalization, and means of transport to hospital. Details of data definitions are shown in the online supplement.
Statistical Analysis
Time from onset to admission as well as means of transportation to hospital were compared before, during, and after the intervention took place, categorized into a 4-month pre-intervention period (January 2010–April 2010), a 6-month intervention period (May 2010–October 2010), and a 4-month post-intervention period (November 2010–February 2011). Four months pre- and post-intervention periods were assessed, as no information on the means of transportation to hospital was available before 2010. Time from stroke onset to hospitalization was categorized based on an a priori decision into admission within 2 hr after stroke onset, more than 2 hr, or unknown time period. Transport to hospital was categorized into EMS versus private or other. Odds ratios (ORs) for estimating the probability of being admitted early or admitted via EMS were calculated from multivariable logistic regression analyses adjusted for potential confounders with variable selection using backward elimination procedure (variables were removed from the model when the p value was above 10%). All multivariable analyses were stratified by intervention and control regions. Potential interactions between region and time periods (pre-intervention, intervention, post-intervention) were assessed by combined data sets from both regions. They were accounted for by adding terms of interaction to the regression models for assessing predictors on time to hospitalization as well as means of transportation. The statistical significance of the resulting coefficient was tested by the likelihood ratio test. Transport to hospital was included separately in the multivariable model on factors associated with time to admission to evaluate whether transport to hospital was an intermediary variable. Sensitivity analyses were performed using month of onset as continuous variable and restricting analyses to patients with ischemic stroke only. Patients with missing values were excluded from analyses. All tests were two-tailed, and statistical significance was determined at an alpha level of .05. Statistical analyses were performed using the IBM SPSS Statistics 21.0 Software Package.
Standard Protocol Approvals, Registrations, and Patient Consents
The identity of an individual patient is anonymous in our data sets; thus, no specific informed consent was obtained from patients. The data were collected routinely within quality assurance registers. Therefore, no specific ethics board approval was needed according to local regulations confirmed by the ethics committee at the University of Würzburg. Hospital identities were only known to the coordination office and the data analyzing center of the respective register.
Results
Study Population
Between January 2010 and February 2011, 10,321 patients with stroke or TIA were documented in the BSR and 11,351 in the NWSR. Of those, 2,278 patients (BSR: 1,117; NWSR: 1,161) suffered an in-hospital stroke or it was unknown whether they were treated in hospital before; of the remaining patients, 234 (BSR: 38; NWSR: 196) suffered from subarachnoid hemorrhage (SAH) or undefined stroke. Demographic and clinical characteristics of the remaining 19,160 patients (BSR: 9,166, NWSR: 9,994) by region are shown in Table 1.
Sociodemographic and Clinical Characteristics of the Patients Included in Both Study Regions Between January 2010 and February 2011.

Note. NIHSS = National Institutes of Health Stroke Scale; IQR = interquartile range.
Time From Onset to Hospitalization
Time from onset to hospitalization by study episode and region is shown in detail in Supplemental Table I. Briefly, proportion of patients being admitted within 2 hr of stroke onset pre-intervention, during the intervention, and post-intervention was 23.0%, 22.6%, and 25.4% in BSR and 25.6%, 26.6%, and 29.0% in NWSR, respectively. In multivariable analyses, age, sex, pre-stroke living conditions, stroke subtype, diabetes, previous stroke (NWSR only), and stroke severity were independent predictors for admission within 2 hr after stroke onset (Table 2). In both regions, a similarly increased probability of early hospital admission was observed after the intervention period compared with the time period before the intervention. Including month of onset as continuous variable in the multivariable model showed similar results (BSR: OR = 1.014, 95% confidence interval [CI] = [1.002, 1.322], p = .024; NWSR: OR = 1.015, 95% CI = [1.003, 1.027], p = .009). Restricting analyses to patients with ischemic stroke only did not change results substantially (data not shown). When pre-hospital management was included into the multivariable model, means of transportation to hospital was an independent factor associated with early hospital arrival in both regions (admission via EMS—BSR: OR = 2.89, 95% CI = [2.06, 4.06]; NWSR: OR = 2.58, 95% CI = [1.25, 5.32]; via other ways—BSR: OR = 0.84, 95% CI = [0.59, 1.20]; NWSR: OR = 0.75, 95% CI = [0.36, 1.56] compared with private transportation). Time of intervention was no longer statistically significant in both data sets when adjusting for pre-hospital management (p values—BSR: .64; NWSR: .15). The term of interaction between region and intervention period was statistically not significant when combining both data sets (p = .88).
Multivariable Analyses: Predictors for Being Admitted Within 2 hr of Stroke Onset.
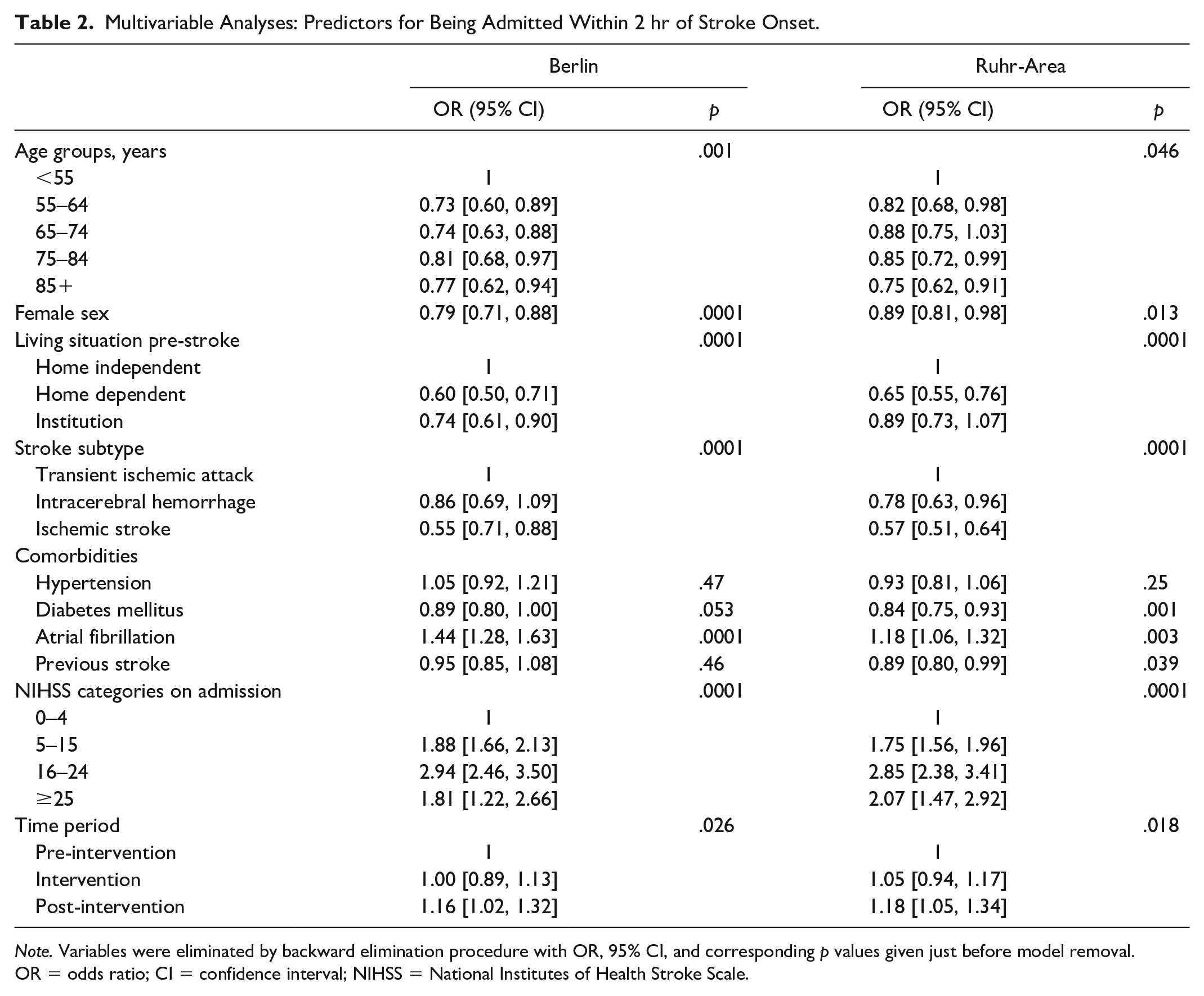
Note. Variables were eliminated by backward elimination procedure with OR, 95% CI, and corresponding p values given just before model removal. OR = odds ratio; CI = confidence interval; NIHSS = National Institutes of Health Stroke Scale.
Pre-Hospital Management
Means of transportation to hospital by time period and region is shown in detail in Supplemental Table II. Briefly, proportion of patients being admitted via EMS pre-intervention, intervention, and post-intervention was 63.2%, 63.4%, and 72.9% in BSR and 67.3%, 64.5%, and 71.4% in NWSR, respectively. In the multivariable analysis, probability of being admitted via EMS was significantly associated with age, sex (BSR only), pre-stroke living condition, stroke subtype, diabetes (BSR only), and stroke severity (Table 3). Patients were more likely to be admitted via EMS after the intervention compared with the study episode before the intervention in both regions. Including month of onset as continuous variable in the multivariable model yielded similar results (BSR: OR = 1.056, 95% CI = [1.044, 1.069], p = .0001; NWSR: OR = 1.026, 95% CI = [1.013, 1.039], p = .0001). Restricting analyses to patients with ischemic stroke only did not change results substantially (data not shown). The term of interaction between region and study episode was statistically significant when combining both data sets (p = .004).
Multivariable Analyses: Predictors for Being Admitted by EMS.

Note. Variables were eliminated by backward elimination procedure with OR, 95% CI, and corresponding p values given just before model removal. EMS = emergency medical services; OR = odds ratio; CI = confidence interval; NIHSS = National Institutes of Health Stroke Scale.
Discussion
“Berlin fighting stroke” aimed at raising awareness about stroke and its time-critical therapies by launching a highly intense campaign lasting for 6 months. It targeted the general public as well as health care professionals in the Berlin urban area. It informed about stroke symptoms and promoted the immediate referral to dedicated stroke centers by EMS in case of stroke signs. As per our initial hypothesis, we observed an increase in the percentage of patients admitted within 2 hr of onset and of patients admitted via EMS was observed in the intervention region after the campaign compared with the episode before. However, a similar increase in proportion of patients being admitted early was seen in the control region where no comprehensive public campaign took place. Therefore, observed increase in early admission in both regions is best explained by a more intense utilization of EMS and might not be attributed to the campaign.
A major determinant of early admission is the appropriate action in case of a suspected stroke event. Several studies found that public campaigns using television, newspapers, or radio-broadcasting increase awareness of stroke signs in the general population (Fogle et al., 2008; Lecouturier et al., 2010). There is also some evidence that women show better stroke knowledge compared with men (Miyamatsu et al., 2012; Stroebele et al., 2011). However, results are inconsistent regarding a potential association between knowledge of stroke symptoms within the population and correct action in case of stroke with some studies suggesting a positive correlation (Fogle et al., 2010; Gordon et al., 2019; Hickey et al., 2018) and others finding no association (Fussman et al., 2010; Marx et al., 2008). Two review articles concluded that the impact of public campaigns on people’s awareness did not translate into changes in behavior and rather identified an improvement of stroke management when health care professionals were targeted (Lecouturier et al., 2010; Rasura et al., 2014). A third systematic review acknowledged that most interventional studies identified a partial effect of interventions. However the authors stressed flaws in study designs that limit the generalizability of the effect or hinder the attribution of the effect to a specific part of the intervention (Mellon et al., 2015). As an answer, Caminiti and colleagues (2017) published a guideline how to plan an educational campaign.
Nonetheless, even recent assessment of awareness for stroke symptoms and actions to take shows limited knowledge, especially for persons with low socioeconomic status, poor education, and persons with risk factors (elderly, patients with comorbidities). Thorough evaluation on how to specifically reach these persons should anticipate future campaigns (Khalil & Lahoud, 2020; Krishnamurthi et al., 2020; Soto-Camara et al., 2019).
Only few observational studies investigated the effect of MMCs on time to hospitalization or on means of transport to hospital within the general population. A campaign in Western Norway prompted faster admissions and higher thrombolysis rates for 6 months and dropped to usual numbers afterward (Advani et al., 2016). This unsustainable and short-lasting effect of a campaign was also reported from a national campaign in Ireland with three televised campaigns within 1 year, lasting 3 weeks each (Mellon et al., 2014). One study from the region of Ontario, Canada, showed an increase in public awareness of stroke signs during a television advertising campaign being associated with an increase of the number of emergency department visits for stroke, including presentation within 2.5 hr of onset (Hodgson et al., 2007). Similar results were reported from Australia (Bray et al., 2011) and Japan (Nishijima et al., 2016). However, there was no control group for comparing potential general time trends. A nationwide, intermittent campaign in the United Kingdom showed a sustained improvement of thrombolysis rates and emergency call numbers for patients with major stroke (Wolters et al., 2018), also after 4 years (Wolters et al., 2015). Importantly, the effect of an MMC was not found for transient stroke symptoms or minor stroke (Wolters et al., 2018). The evaluation of the number of thrombolysis rates during a time interval with repetitive campaigns in Hungary showed no significant change in treatment rate (Folyovich et al., 2018). Similar to our results, the Temple Foundation Stroke Project in Texas (USA) failed to demonstrate that a comprehensive intervention targeting the general population and health care professionals significantly increases the proportion of stroke patients being admitted within 2 hr of stroke symptoms compared with a control region (Morgenstern et al., 2002). A previous cluster randomized trial within selected areas in Berlin in 2004/2005 suggested a reduction in pre-hospital delay in women but not in men by a population-based intervention through individualized educational letters with stroke signs and symptoms (Muller-Nordhorn et al., 2009). For increasing stroke awareness in the population, MMCs were perceived to have a wider population impact compared with other alternatives such as screening events or patient education programs (Lecouturier et al., 2010). The growing importance and the wide reach of new media—for example, E-tools—is recognized, and its integration in campaigns is recommended (Lecouturier et al., 2010). Furthermore, search engines allowing public access (e.g., Google Trends) represent an additional tool to evaluate effects of public health campaigns. Increased queries were documented following a campaign informing about cardiovascular disease in women (Morgenstern et al., 2002). Interestingly, some argue that in up to 90% of patients, help is sought by bystanders and not by affected patients themselves (Wolters et al., 2015). However, the answer to the question whether improved stroke awareness directly translates to human action and admission behavior remains inconclusive (Mellon et al., 2015). In addition, the use of social media was not so common when our study took place.
In our study, more patients were admitted earlier to hospital after the campaign in both regions. However, this significant effect disappeared in the intervention and the control regions when the means of transportation was included in the multivariable model. This finding indicates that the higher proportion of patients being admitted early in Berlin and the Ruhr-Area after the campaign might be caused by an increased proportion of patients being admitted via EMS in both regions. The increase in EMS uptake observed in Berlin after the end of the intervention period might be caused by the MMC addressing the need for immediate EMS involvement. However, the reasons for the observed increase in EMS use in the control region remain unclear and could also be mediated by more frequent deployment of EMS in possible stroke patients by the dispatch center. To the best of our knowledge, no major events (e.g., national awareness campaign) or organizational changes (e.g., restructuring of EMS) took place in either regions. However, the recent establishment of a stroke-specific network of hospitals serving for acute stroke patients within the Ruhr-Area also affects the organization of acute stroke services for the population, including pre-hospital management procedures within this region (Eyding et al., 2012). Therefore, anticipated changes in means of transportation within the Ruhr-Area as major determinant of delay to hospital might be causative for the increase in patients admitted within 2 hr in this area.
Limitations
The study has limitations. In both registers, no specific measures were undertaken to estimate completeness of data collection within respective hospitals. Therefore, some findings might be caused by variations in patient’s selection across the study periods. However, the number of patients documented in the hospitals before, within, and after the intervention remained stable in both regions and it is unlikely that the campaign had any major impact on completeness of case ascertainment. Using data from quality registries might miss relevant information that was not assessed or later categorized, to reduce variables for the statistical analyses (e.g., time from onset to hospital in case of unknown onset or wake-up symptoms, socioeconomic data, knowledge of stroke). To maximize the possible effect of an MMC, it is recommended to organize focus group interviews, which was not the case in our study. We are aware of relevant information that was not taken into account during preparation of the MMC (e.g., socioeconomic status). Within the intervention region, a number of additional research projects were conducted during the study period such as the theoretical development of a dispatcher algorithm for correct identification of stroke patients in emergency calls, which might increase stroke awareness among dispatchers of the intervention region (Krebes et al., 2012). However, the potential implications of this project on the population level might be limited as similar time trends were seen in the control region. The introduction of a stroke-specific ambulance in the Berlin area was after the end of the study period (Weber et al., 2013). Although the campaign was supported by Boehringer Ingelheim, the larger portion of the campaign was carried out pro bono by the medical staff and participants of the 15 contributing stroke units of the BSR. Therefore, we were unable to provide any detailed cost estimates. No indicator of exposure to intervention among stroke patients and relatives in both regions was documented. Therefore, although the MMC is based on local media in Berlin, a region of over 400 km airline distance from the Ruhr-Area, we cannot exclude that there might be some exposure to the intervention also in the control region. The MMC in our study did target the public as well as health care professionals, hampering dissolution of a potential impact of the campaign on defined endpoints (Lecouturier et al., 2010). It is important to note that our results might be confounded by unmeasured confounders and effects caused by interaction between variables. Last, it has to be acknowledged that publication of the results of our study has taken more time than originally intended.
Conclusion
Although a reduction in delay to hospital arrival mediated by an increased uptake of EMS was observed over the study period in an urban area, there was no major improvement by a comprehensive MMC compared with a control region with state of the art public information but no dedicated MMC.
Supplemental Material
sj-docx-1-sgo-10.1177_2158244021989275 – Supplemental material for Effects of a Public Awareness Campaign on Time to and Way of Hospital Admission After Stroke
Supplemental material, sj-docx-1-sgo-10.1177_2158244021989275 for Effects of a Public Awareness Campaign on Time to and Way of Hospital Admission After Stroke by Peter U. Heuschmann, Sarah Zweynert, Jan Sobesky, Christian H. Nolte, Heinrich J. Audebert, Christiane Hantke, Hans-Christian Koennecke, Marianne Kalic, Klaus Berger and Matthias Endres in SAGE Open
Footnotes
Acknowledgements
We wish to thank Dr. Hoffmann as representatives of the Ärztekammer Berlin (Berlin Chambers of Physicians) as well as Prof. Hermanek from the Bavarian Working Party for Quality Assurance, Munich, for its support of the Berlin Stroke Register. In addition, we wish to thank Dr. Pelz and Ms. Sieveking from the Center for Stroke Research Berlin and Dr. Härtle from Boehringer Ingelheim for supporting the conduct of the mass media campaign (MMC) in Berlin. We also wish to thank all hospitals participating in the study (see Supplemental Material), all health care professionals involved in the contributing hospitals, as well as all patients and their families.
Author Contributions
P.U.H. and M.E. conceived the study and were responsible for the protocol development and supervision. M.E. acquired the funding of the study. J.S. contributed to the protocol development and organized the campaign. C.H.N., C.H., H.J.A., and H.-C.K. contributed to the campaign. Data analysis was performed by M.K., K.B., and P.U.H. P.U.H. wrote the first draft of the manuscript. S.Z. contributed to the manuscript, and all authors were involved in the critical discussion and editing of the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.U.H. reports grants from Berlin Chambers of Physicians, during the conduct of the study; grants from German Ministry of Research and Education, German Research Foundation, European Union, Federal Joint Committee (Gemeinsamer Bundesausschuss [G-BA]) within the Innovationsfond, Charité–Universitätsmedizin Berlin, German Parkinson Society, University Hospital Würzburg, Robert Koch Institute, German Heart Foundation, University Göttingen (within FIND-AF randomized (Finding Atrial Fibrillation in Stroke Patients), supported by an unrestricted research grant to the University Göttingen from Boehringer Ingelheim), University Hospital Heidelberg (within RASUNOA-prime [Registry of Acute Stroke under Novel Oral Anticoagulants], supported by an unrestricted research grant to the University Hospital Heidelberg from Bayer, BMS, Boehringer Ingelheim, Daiichi Sankyo), Charité–Universitätsmedizin Berlin (within Mondafis, supported by an unrestricted research grant to the Charité from Bayer), outside the submitted work. J.S. reports grants from Boehringer Ingelheim, during the conduct of the study; personal fees from Boehringer Ingelheim, personal fees from Pfizer, personal fees from Bayer, personal fees from Sanofi, personal fees from Maquet, personal fees from Takeda, outside the submitted work. H.J.A. reports grants from Boehringer Ingelheim, during the conduct of the study; personal fees from Lundbeck Pharma, personal fees from Bristol-Myers Squibb (BMS), personal fees from EVER Neuropharma, personal fees from Pfizer, personal fees from Sanofi, personal fees from Boehringer Ingelheim Pharma, personal fees from Bayer Pharma, personal fees from Roche Diagnostics, grants from German Federal Ministry for Education and Research, grants from Technology Foundation Berlin, outside the submitted work. C.H.N. reports grants from Boehringer Ingelheim, during the conduct of the study; other from Boehringer Ingelheim, outside the submitted work. H.-C.K. is auditor in the certification process of stroke units for the German Stroke Society. M.E. reports grants to the Charité from Boehringer Ingelheim, during the conduct of the study; M.E. reports grants from Bayer, German Federal Ministry for Education and Research (BMBF), Corona Foundation, Deutsche Forschungsgemeinschaft (DFG), Deutsches Zentrum für Herz-Kreislauf-Forschung (DZHK), Deutsches Zentrum für Neurodegenerative Erkrankungen (DZNE), European Union (EU), and Foundation Leducq and fees paid to the Charité from Bayer, Boehringer Ingelheim, BMS/Pfizer, Daiichi Sankyo, Amgen, GlaxoSmithKline (GSK), Sanofi, Covidien, Novartis, all outside the submitted work. S.Z., C.H., M.K., and K.B. have nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The mass media campaign (MMC) in Berlin was supported partly by Boehringer Ingelheim. Boehringer Ingelheim had no influence in the design of the study, the data analysis, the draft of the manuscript, or the decision to submit the manuscript.
Ethical Approval
The data were collected routinely within quality assurance registers. Therefore, no specific ethics board approval was needed according to local regulations confirmed by the ethics committee at the University of Würzburg.
Guarantor
M.E. is the guarantor of the article.
Informed consent
The identity of an individual patient is anonymous in our data sets; thus, no specific informed consent was obtained from patients.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.