
Abstract
Competent delivery of interventions in child and youth social care is important, due to the direct effect on client outcomes. This is acknowledged in evidence-based interventions (EBI) when, post-training, continued support is available to ensure competent delivery of the intervention. In addition to EBI, practice-based interventions (PBI) are used in the Netherlands. The current paper discusses to what extent competent delivery of PBI can be influenced by introducing supervision for professionals. This study used a mixed-method design: (1) A small-n study consisting of six participants in a non-concurrent multiple baseline design (MBL). Professionals were asked to record conversations with clients during a baseline period (without supervision) and an intervention period (with supervision). Visual inspection, the non-overlap of all pairs (NAP), and the Combinatorial Inference Technique (CIT) scores were calculated. (2) Qualitative interviews with the six participants, two supervisors, and one lead supervisor focused on the feasibility of the supervision. Four of six professionals showed improvement in treatment fidelity or one of its sub-scales. Had all participants shown progress, this could have been interpreted as an indication that targeted support of professionals contributes to increasing treatment integrity. Interviews have shown that supervision increased the professionals’ enthusiasm, self-confidence, and awareness of working with the core components of the intervention. The study has shown that supervision can be created for PBI and that this stimulates professionals to work with the core components of the intervention. The heterogeneous findings on intervention fidelity can be the result of supervision being newly introduced.
Keywords
Introduction
Competent delivery of interventions is related to positive outcomes for children and families (Goense et al., 2016; Lyon et al., 2018; Schoenwald et al., 2009). Evidence-based interventions (EBI) work with continued consultation and support following (initial) training to enable competent delivery of interventions on a long-term basis and to sustain the effectiveness of the intervention (Dorsey et al., 2017; Lyon et al., 2018; Ogden et al., 2005). Supervision (Dorsey et al., 2013; Cunningham et al., 2006; Schoenwald, 2016), also referred to as (expert) coaching (Akin, 2016; Kretlow & Bartholomew, 2010; Lyon et al., 2011), is recognized as a key strategy for building and sustaining competencies among professionals for a proper implementation of interventions (Fixen et al., 2019; Kretlow & Bartholomew, 2010; Wandersman et al., 2012). Attention to qualitative execution of interventions and, thereby, the positive implementation of interventions is key in EBI.
Much less attention is paid to these factors in community practice contexts (i.e., “usual care”—see definition below) (Lyon et al., 2018). Likewise, research attention for the support of professionals working in usual care is limited (Dorsey et al., 2018). This is surprising as both interventions (1) have the same aim—attaining positive outcomes for clients, (2) are known to include many components of evidence-based interventions (Garland et al., 2010; Lyon et al., 2018), and (3) organizations and professionals in children’s services are under high (financial) pressure to deliver effective care (Connell et al., 2009; Friele et al., 2018).
The current paper will discuss to what extent competent delivery of interventions in usual care in The Netherlands can be influenced by introducing supervision to support professionals in this sector.
Usual Care
We begin by clarifying our definition of “usual care” as it exists in the Netherlands where three separate systems are in place: (1) Child and youth health care (infant health system, school health system), (2) Child and youth social care, based on (a) easily accessible, preventive neighborhood teams and (b) indicated specialized help by local and regional organizations for youth and parenting assistance, as well as organizations for child protection and youth probation, and (3) Child and youth mental health care. Since the introduction of the Youth Act in 2015 Dutch municipalities are responsible for providing appropriate services and care for children, young people and families in need of assistance, including mental health provisions (Netherlands Youth Institute, 2019). Due to this development, greater collaboration amongst the three systems is taking place. This research project addresses child and youth social care and, more specifically, indicated, specialized help for youth and parenting assistance.
Evidence-Based and Practice-Based Interventions
In Dutch child and youth social care, organizations roughly provide two types of interventions: evidence-based interventions (EBI) and practice-based interventions (PBI). EBI is typically imported from abroad and is applied to the main internalizing and externalizing problem groups. Examples are Parent Management Training Oregon (PMTO) (Forgatch & Patterson, 2010), Triple P (Sanders et al., 2003), Aggression Replacement Training (ART) (Goldstein et al., 1998) or Multi System Therapy (MST) (Henggeler et al., 2009). These EBIs are theoretically based, well documented, protocoled or structured, contain a manual and have gained empirical support in at least two randomized controlled trials (Veerman & van Yperen, 2007). PBIs, on the other hand, are developed within organizations for child and youth social care, usually for client populations with combinations of complex internalizing and externalizing problems. These PBIs make use of a combination of known, effective components of EBI and parts of recognized EBIs which overlap (Leijten et al., 2015; Visscher et al., 2018)
A national program for effective youth care was introduced around the turn of the last century. It was aimed at the bottom-up development of PBI toward EBI, following distinct evidence levels (Veerman & van Yperen, 2007): (1) descriptive and theoretical evidence; (2) indicative evidence; and (3) causal evidence. Each level stems from different types of research (see Brady et al., 2016, for an example of this developmental process). These are well-known steps in the development of interventions (Bartholomew et al., 2006) which were logically the basis of the currently well-known and worldwide implemented EBI (Schoenwald & Hoagwood, 2001).
Linked to the bottom-up development of interventions, a national accreditation panel was initiated along with a national database of effective interventions, whereby only interventions that are at least accredited on the level of descriptive and theoretical evidence are included. The database supports organizations and local governments in their choices on investments in intervention and care.
Inclusion in the database stimulates organizations to engage in research concerning the interventions they carry out. Admission is valid for 5 years, after which time reassessment is necessary to remain in the databank. Deliverance of research is required to acquire the next evidence level during reassessment. The performance of implementation research combined with research on intervention outcomes is a minimum requirement (Netherlands Youth Institute, n.d.).
Performance of Intervention
During research addressing the implementation of interventions, focus on the quality of the performance of the intervention is crucial. This is indicated by the terms “treatment integrity” or “treatment fidelity,” meaning the degree to which intervention is carried out as intended (McLeod et al., 2013; Perepletchikova, 2011; Schoenwald, Garland, Chapman, et al., 2011). To determine treatment integrity it is necessary to know the components contained in an intervention. Additionally, a distinction is made between common and specific factors of an intervention. Common factors of interventions apply to all target groups regardless of presenting issue. Examples are a good relationship between caregiver and client or, creating positive expectancies (Andrews et al., 1996; McLeod et al., 2013). Specific factors are components of interventions which are effective by specific target groups (i.e., with specific presenting issues). This concerns both therapeutic and conversational therapy techniques as well as intervention format (i.e., group or individual sessions) (Blase & Fixsen, 2013; Van Yperen et al., 2015).
The application of the different intervention components is central in determining treatment integrity or treatment fidelity. This refers not only to the application of the intervention components (therapist adherence), but also competent application (therapist competence) (Perepletchikova, 2011). Therapist competence refers to the technical skills and clinical acumen (timing and appropriateness) in delivering the intervention components (Barber et al., 2006; Barber, Sharpless et al., 2007; Barber, Triffleman et al., 2007). Finally, treatment differentiation in interventions is considered: the degree to which components other than those in the original intervention are applied (often to meet individual client needs) (McLeod et al., 2013; Perepletchikova, 2007). Here we will refer to the term “fidelity” to indicate professionals’ adherence and competence concerning common as well as specific ingredients of intervention.
Supervision
Supervision (Milne, 2009, p. 15) is “the formal provision, by approved supervisors, of a relationship-based education and training that is work-focused and which manages, develops, and evaluates the work of colleagues.” Supervision has different functions: foremost, it is directed at the progress of the client, reflection on previous sessions, and anticipation of upcoming sessions (Cunningham et al., 2006; Goense et al., 2015). Milne (2009) defines this as the normative function of supervision (oversight of quality control and client safety issues). The other two functions are a restorative function (fostering emotional support for professionals) and a formative function (supervising skill development) (Bearman et al., 2017; Milne, 2009).
Active learning methods, such as role play and other forms of rehearsal are essential for competency building in supervision (Bearman et al., 2013, 2017; Goense, Boendermaker, & Van Yperen, 2016; Nadeem et al., 2013). Additionally, working with video feedback (VF) is considered a powerful (Murray & Leadbetter, 2018; Topor et al., 2017) and effective active learning method, especially in combination with an observation form of the skills to be learned (Fukkink et al., 2011). Despite the fact that reviewing actual practice by using audio or video recordings is considered one of the “gold standard techniques” in supervision (next to symptom monitoring, fidelity assessment, clinical behavioral rehearsal in supervision, and supervisor modeling) (Milne, 2009), only few interventions regularly work with VF as an active learning method in supervision (Dorsey et al., 2018). Only PMTO is known for incorporating VF on a regular basis (Akin, 2016; Ogden et al., 2005; Thijssen & De Ruiter, 2010).
Monitoring Fidelity
In efficacy studies, the measurement of fidelity is vital for linking the studied intervention with the outcomes. In EBI for young people with behavioral problems—and their families—different instruments to assess therapist or trainer fidelity are in use (Goense et al., 2018; Schoenwald, Garland, SouthamGerow, et al., 2011). Instruments for research purposes typically focus on intervention adherence (Goense et al., 2014; Perepletchikova et al., 2007), whereas in supervision, competence assessment will likely be considered more important (McLeod et al., 2016). In EBI for behavioral problems (Goense et al., 2018) and in cognitive behavioral therapy for youth anxiety (McLeod et al., 2016) observational instruments are used to assess fidelity. An example of such an instrument, which is used in regular supervision with VF, is the fidelity of implementation rating system (FIMP) by the Parent Management Training Oregon (Forgatch & Patterson, 2010). To our knowledge, this is the only example of an instrument that is integrated in an online system and used on a regular basis in video-based supervision (Goense et al., 2018).
Identifying and operationalizing the core components of the intervention is a crucial step in developing such an instrument (Feely et al., 2018; Kirk, 2020). It is important to not only describe the practice elements that must be applied, but also to describe how to implement them (McLeod et al., 2016), allowing an intervention to be “teachable, learnable, doable and assessable in practice” (Fixen et al., 2019, p. 71). Input from professionals working with the intervention should be organized and used to describe the implementation of the core components (Feely et al., 2018; Goense, 2018). The core components of an intervention are those elements that are expected (based on theory) or known (based on empirical research) to contribute to client outcomes. These can be seen as the cause of the intervention’s effect.
The Study
This study describes a small-scale project where supervision with a focus on fidelity was introduced to support professionals of two PBIs in the Netherlands. The central question of this study was: to what extent does supervision—based on a combination of video feedback, role play and a fidelity monitoring instrument as active learning methods—influence the level of fidelity with which professionals conduct the intervention?
The study aims to deliver support in the charting and influence of intervention fidelity of PBI in the Netherlands, as part of the bottom-up development of PBI to EBI.
Method
Design
This 2-year study (2016–2018) used a mixed-method design and consisted of two parts. (1) A small-n study consisting of six participants in a non-concurring multiple baseline design (MBL) was used to explore the effect of newly introduced supervision using video feedback, role play, and a fidelity monitoring instrument. Participants filmed a selection of sessions with clients during a 6-month baseline period (without supervision) and an 8-month intervention period (with supervision). These recordings were used in the supervision sessions and were coded by the research team to score fidelity. (2) Qualitative interviews with the six participants, two supervisors, and one lead supervisor on the supervision process were conducted, examining the learning experiences and the feasibility of the supervision. Data were gathered simultaneously, with the qualitative data having a complementary function (Palinkas et al., 2011).
The small-n design was chosen in consultation with both participating organizations. As Dutch municipalities have been responsible for providing services and care since the introduction of the Youth Act in 2015, both financial pressure and workload have increased. No margin exists for a study with the contribution of large groups of professionals.
Context
Two organizations for child and youth social care participated in the supervision project. Both are large organizations that offer a variety of interventions and special education. Both were invited to select a practice-based intervention that (1) was accredited as “theoretically well-grounded” by the Dutch national accreditation committee for youth interventions and formally included in the national database of effective interventions and (2) worked regularly with individual meetings/coaching sessions with young people focused on behavior change that would serve as the point of reference of the supervision.
Professionals in both PBIs are expected to use a mixture of techniques in the individual coaching sessions to address (1) non-specific intervention ingredients (Blase & Fixsen, 2013), such as establishing contact, stimulating motivation, and establishing clear goals with clients; and (2) specific therapeutic solution-focused (Gingerich & Peterson, 2013) techniques (such as exception-, scaling, or wonder-questions) and cognitive behavioral (Andrews & Bonta, 2003; Goldstein et al., 1998) techniques (such as cognitive restructuring) in non-protocoled individual sessions with young people.
Intervention
The supervision included video feedback, role play, and application of an instrument to monitor fidelity. Supervision was organized as group supervision and developed by the research team based on previous projects (Boendermaker et al., 2012; Goense et al., 2015) and inspired by the organization of supervision in PMTO. An expert of the license holder organization of PMTO in the Netherlands functioned as lead supervisor and trained both supervisors in two 1-day training sessions. Substantiation of the content was outlined in a manual (Goense & Ruitenberg, 2018).
Supervision sessions followed a fixed structure: specific topics discussed at the start of the session, transition to the discussion of a video fragment, transition to rehearsal in role play, and the closing of the meeting (see Table 1). During the 8 month intervention period, seven 2.5-hour group supervision meetings took place for site 1 and five for site 2. Both supervisors used an intervention log to report on the supervision content applied. Both used the topics of the start of the session, although it took the supervisor of site 2 two sessions to work with reference to the agreements of the former sessions (see Table 1). Both applied all parts of the discussion of a fragment. Only the supervisor of site 1 worked with rehearsal in role play and both worked with the topics of the closure of the meeting (see Table 1). Supervisors had no disciplinary duties.
Content of the Group Supervision With Video Feedback, Role-Play, and Monitoring Instrument.

As for professionals, supervisor support is necessary to achieve an effective implementation of supervision (Cunningham et al., 2006; Goense et al., 2015; Milne & Reiser, 2016). Likewise, as in supervision content, supervisor training was developed based on previous projects and in close collaboration with the licensed expert, and outlined in a manual (Goense & Ruitenberg, 2018). The training for supervisors focused on agenda setting, providing feedback, working with action planning, role play, use of the fidelity monitoring instrument, and working with a fixed schedule in the supervision sessions (see Table 1). Following, five support meetings for the supervisors took place between late 2016 and late 2017. One supervisor participated in all meetings, the second supervisor (due to practical circumstances) in three. Supervisor support was concluded with an evaluation meeting (end 2017).
At both sites professionals focus on stimulating the strengths of young people. In the same way, supervision is focused on stimulating the professionals’ strengths (Murray & Leadbetter, 2018). Also at both sites, the supervisor applied the same techniques in supervision sessions as professionals were expected to use with their clients. For example, professionals are supposed to use role play with their clients. Likewise, professionals were engaged in role play to experience how this helps in applying new behavior.
Participants
Supervisors
Two (female) supervisors (one from each site) participated in the pilot. One is a supervisor/trainer with a bachelor-level degree and more than 10 years of experience in supervision and the other is a master-level psychologist with about 2 years of experience in supervision. Mean age was 35.
Professionals
Six professionals (three male, three female) participated in the pilot (site 1: n = 4; site 2: n = 2). All completed a bachelor-level social work education. Their ages varied between 27 and 38 years, and excepting one participant they all had more than 10 years’ work experience in youth care.
Selection
Both organizations had two teams working with the selected intervention. Teams were approached by a researcher of their own organization who, together with the authors and a third researcher, formed the research team in this project. All aspects of the pilot were discussed during a team meeting (including the recording of sessions with clients, the use of the recordings in group supervision sessions, the coding of the recordings by the research team, the need for written informed consent of all clients to record sessions, as well as consent of the parents with clients under 16). Teams were free to decline on participation in the pilot. In both organizations one team volunteered to participate in the supervision and provided informed consent for participation in interviews. The other teams (one in each organization) were facing a period of instability due to staff turnover and sick leave and decided not to participate. Both teams have experience with non-protocoled support sessions, concerning personal dilemmas in cases or with implementing the intervention.
Video Recordings
The six professionals participated in a short training on recording client conversations using an instruction film (Meerhoek et al., 2015), and received instructions on informed consent to record conversations with young people.
Participating professionals were asked to record four conversations with clients during the baseline period and four during the intervention period (6 professionals × 4 recordings × 2 periods) in different phases of their work with clients. In multiple baseline designs, the recommended measurement standard is to include at least five data points in each baseline and intervention phase in at least three participants (Kratochwill et al., 2013). In this study the number of participants (six) is more than sufficient. Since acquiring consent and making the videos in daily practice is demanding, four recordings during each phase were planned. When multiple baseline designs include at least three data points in each phase this is considered to meet standards with reservations.
Fidelity Rating
Development fidelity instrument
At both sites the fidelity instrument was developed based on previous work (Goense & Ruitenberg, 2015). In line with the steps for identifying core components of intervention as described in Feely et al. (2018) and Kirk (2020) the core components were based on the intervention descriptions available in the Dutch national database of effective interventions (Cleef, 2015; Pronk, 2016). According to the steps of developing a practice profile (Metz, 2016) work sessions with professionals and their supervisor were used at each site to define core components and competent delivery (Boendermaker & Goense, 2017). This process is described in a manual (Goense, 2018).
The core components defined were: contact, application of techniques, and goal orientation. Contact consisted of seven (site 1) and six (site 2) elements respectively, such as: “being a good listener,” “being patient,” “being reliable,” “connecting with the youth,” and “being a positive role model.” At both sites five elements were distinguished for application of techniques: “giving feedback,” “providing insight into emotions, thoughts, and behavior,” “utilizing motivational conversation techniques,” “stimulating and practicing alternative behavior,” and “working in a solution-oriented manner.” In both interventions one element was distinguished for goal orientation. Because of the small difference in the description of contact in both interventions, the total number of elements was 13 at site 1 and 12 at site 2. This small difference is acceptable from the viewpoint of implementation; in this way the fidelity instrument is applicable and fitting for the specific situation in practice (Damschroder et al., 2009; Fixen et al., 2019). Also, due to the fact that by consideration of fidelity we assume the total score of the three core components.
Each element was further defined as to what constituted a competent execution. “Being a good listener,” for example, means that the professional “takes their time and gives the conversation their full attention,” “is an active listener (makes eye contact, uses friendly intonation and facial expressions, nods, and/or agrees),” “speaks in a calm and clear manner, knows how to incorporate silence,” “summarizes what has been discussed,” and “is flexible when encountering resistance (sees youth’s point of view, repeats arguments).” In this manner, the three core components were operationalized in professionals’ behavior on the 13 (site 1) and 12 (site 2) elements (Appendix).
The operationalized elements were combined into an observational questionnaire, to be employed to monitor the execution of the intervention. In the project, this instrument was used in two ways: as a supervision instrument to reflect on the execution and as an instrument for the researchers to measure the quality of the execution (Goense et al., 2015).
Fidelity Rating
The observational questionnaire was completed for each video recording by a researcher of the research team, all of whom were familiar with the interventions and helped develop the instruments. Each recording was viewed in its entirety, with researchers checking for the three core components (operationalized in 12/13 elements) regarding they were applied, and if so, how competently. Each item was assigned a rating between 1 and 9, where a score of 7 to 9 means “good work,” a score of 4 to 6 means “acceptable,” and a score of 1 to 3 suggests that more work is needed on the specific component. Scores were combined to determine the total score.
Inter-rater Reliability
At the start of both coding processes agreements were made on the interpretation and rating of the recordings. Subsequently, two researchers coded the same recording. The inter-rater reliability of this was satisfactory (site 1: ICC .62) to good (site 2: ICC .80). Subsequently, two randomly selected recordings were coded by two researchers as well. These tests also yielded satisfactory and good inter-rater reliability scores respectively (site 1: resp. ICC .64 and .88; site 2: ICC .80 twice).
Qualitative Interviews
To gather qualitative information on the supervision process, professionals (6) as well as supervisors (2) and the lead supervisor (1) were approached for an interview near the end of the intervention period. Interviews were between 30 and 45 minutes. All respondents received a transcript of their interview for validation. Interviews focused on the content of the supervisionary sessions and (learning) experiences during the supervision (as participant, supervisor, or lead).
Analyses
Fidelity measures
In this project each of the six professionals was treated as a single case. Single-subject experimental design data analysis started with a visual inspection of the alliance, application of techniques, goal orientation, and total fidelity score (Barlow et al., 2009). After visual inspection the non-overlap of all pairs (NAP) and the Combinatorial Inference Technique (CIT) scores were calculated. Both scores compare the scores between the baseline and the intervention period. A so-called NAP score is used in single-subject studies to calculate the differences in scores between the baseline and the intervention period. The NAP score expresses the likelihood that a random score from the intervention period is higher than a random score from the baseline period (in this case, the period with and without coaching). The NAP score is a value between 0 and 1 in which .50 means no difference between both time periods. As a rule of thumb, in this pilot we interpreted .65 as “meaningful” (Parker & Vannest, 2009).
The so-called CIT score was used to establish the level of change relative to the maximum change achievable based on the baseline score. This method was derived from the Combinatorial Inference Technique, which compares all possible changes with the maximum change (Rouanet et al., 2000)
Interview data
Data were analyzed using Maxqda 11 by a master level, junior researcher in collaboration with the first author; working from a directed content analyses approach the focus was on identifying themes or patterns in the data (Hsieh & Shannon, 2005). Basic codes were (learning) experiences with the distinct parts of the supervision protocol (VF, role play and the fidelity instrument). Due to the limited number of interviews analysis consisted of one round of coding.
Results are per site, combined with the results of the quantitative analysis, discussed with participants for validation.
Results
Fidelity Ratings
Mean fidelity scores
Producing video recordings proved challenging, especially during the baseline period. Professionals were not always successful in attaining permission to record sessions, therefore the number of recordings in the baseline and the intervention period varied. In total, 20 baseline recordings were made and 25 recordings during the intervention phase (a total of 45 available recordings out of the requested 48). The desired distribution of recordings over the different phases of treatment was, with some exceptions, maintained.
Sessions with clients were sometimes difficult, especially those with young people entering a program, where the focus is on engagement and motivation. Therefore some recordings were very short; recordings varied in length between 5 and 96 minutes (three recordings were 5 minutes in length, the duration of most were around 25–30 minutes). All recordings were accepted as the goal was competency building and learning and with the consideration that a 5-minute session with an unmotivated young person may offer significant learning possibilities.
As the focus of the sessions differed, so did the number of items in the core element contact. It was decided to present the outcomes as averages of the three core components of both interventions: contact, application of techniques, and goal orientation (Table 2). The column “number of recordings” shows that not all three components were applied in all conversations. According to the professionals, these did not always fit the purpose of the individual session.
Mean Scores on the Monitoring Instrument of Each Professional (Range 1–9).

Fidelity change
Visual inspection in single case research consists of evaluating the graphs with respect to six elements: level, variability, trend, overlap, intercept gap, and consistency (Vannest & Ninci, 2015). Assessing the level change means evaluating whether treatment fidelity increased from baseline to intervention. Variability is evaluated by judging whether fidelity was stable between measurement moments within phases. Trend occurs when increasing or decreasing patterns are visible within phases. For example, increasing fidelity within the baseline phase would indicate trend and thus complicate assigning change to the intervention. Overlap is assessed by evaluating the difference in range of fidelity in both phases. It indicates to what degree data points in the baseline phase fall in the range of the data seen in the intervention. Intercept gap evaluates whether change occurs immediately when intervention is started, or is delayed and cumulative. Lastly, consistency is evaluated by examining whether patterns across cases are the same. Desirable change would mean consistent increasing level with a clear intercept gap and no overlap between phases, without signs of high variability or problematic trend in one of the phases.
The visual inspection of the development of treatment fidelity over time for the six professionals (Figure 1) consistently shows no desirable change in each of the six cases (Table 3). Professional 2 and 5 seems to have higher levels of fidelity in the intervention phase, but trend in the baseline is problematic. In the other professionals there is no evident level-change between the two phases. Neither immediate or cumulative change occurs between phases and much overlap between data from baseline and intervention phase exists.
Visual Inspection of the Fidelity Score by Assessing the Development of Six Professionals With Respect to Six Elements (Vannest & Ninci, 2015).

No more than 3 points difference between two subsequent data points within the phases is coded as stable.
More than 1 point difference between last data point in baseline and start of intervention phase denotes an intercept gap.
Development within the professional that would support the effectiveness of the intervention are marked.
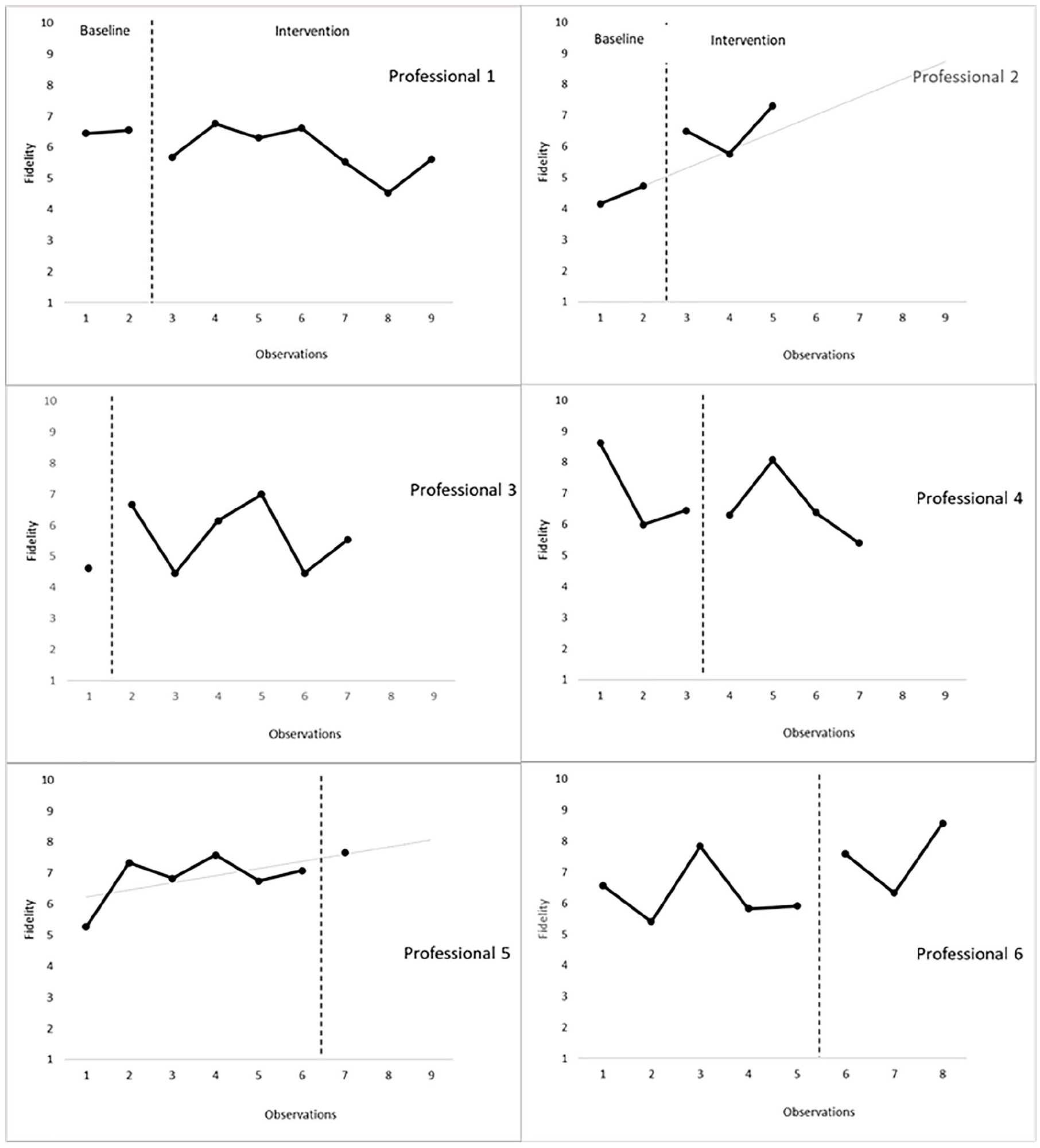
Development of the treatment fidelity during baseline and intervention phases in six professionals.
The subscales follow a similar pattern (Figure 2). Participants 1, 2, 3, 5, and 6 show improvement over time in some or all of the subscales. Due to positive trend during baseline, lack of consistency between the professionals and phases with few data points, the patterns render no evidence of an effect in subscales of treatment fidelity. With respect to contact, professionals 2, 3, 5, and 6 show improvement, however, there is only one data point in one of the phases in two of the cases (p3 and p5). The implementation of techniques grows only in professional 2, but there a positive trend during baseline already existed. Lastly, with respect to goal orientation, professional 1, 2, 3, and 5 show improvement. However, lack of data in one of the phases (p3 and p5) and positive trend in the baseline (p1 and p2) are present.

Development of the three core elements contact, application of techniques and goal orientation during baseline and intervention phases in six professionals.
Evaluation of changes in fidelity
As the NAP scores (Table 4) show, professional 2 shows meaningful change in application of techniques, goal orientation, and total score. Professional 3 shows meaningful change in the elements contact and goal orientation. Professional 5 makes meaningful progress in all elements and professional 6 makes meaningful progress on those items that fall under contact and application of techniques and on total score. Professionals 1 and 4 show no meaningful change. Based on CIT changes that were found were moderate to strong: The professionals that show meaningful change make between 44% and 96% progress on the different parts of the fidelity measure (Table 4). These findings do not determine that a functional relation exists between video feedback and treatment fidelity since not all replications show the same pattern. Some desirable changes occur, but whether these changes are due to the video feedback is doubtful at least.
NAP and CIT Scores of the Six Pilot Professionals (≥0.65 bold).

Interview Supervision
Participants responded enthusiastically and saw advantages in working with the organized supervision. It ensures that supervision is goal-oriented and helps to formulate [and practice?] concrete (learning) questions during discussion of the video fragments. The fixed closure of a discussion of the fragment creates a focus for the professional for the next session with the client. “You see that what has been previously said continues to play a role in the following sessions and that video recordings are made of this” (supervisor).
Recording and viewing of videos
The professionals had to accustom themselves to producing videos. Requesting permission (also from parents) was discussed and practiced in the first supervisory session. Watching the recordings was very positive for all participants. They felt that the recordings clearly showed how the professional performed and how the youth responded. Performance was more evident than by the oral description of a situation during peer supervision. Through observation by others and through the questions and suggestions by colleagues and the supervisor, professionals learn alternative working methods. They become more aware of their techniques and the intervention in which they work. The strength-based approach used in the coaching sessions was considered a welcome change from standard case discussions, thereby creating more enthusiasm and energy and increasing the professionals’ confidence. This allowed for the manifestation of a safe atmosphere and a learning culture. As one professional commented, “This is educational for the entire organization.”
Fidelity instrument
The fidelity instrument helps to view the recordings in a focused way and to provide concrete and specific feedback. It contributes to “speaking the same language” regarding the invention being used.
Professionals stated that using the fidelity instrument led to an increased awareness of the core components of the intervention which changed their approach to the work. One professional said: “Normally I just try to have a good conversation, but now I give much more thought to what I want to achieve with the conversation.” Another professional: “I would start a conversation, certain topics would present themselves along the way, we would discuss these and that would be it. Now I have been able to structure that. I am more aware of it, and I am working on incorporating this.”
Several professionals shared their realization that when a coaching session did not go as envisioned, it was not always because of the client: “(. . .) Professionals tend to adopt a certain style and then claim afterwards that they can’t work with a certain youth, because they feel no connection. You cannot really say that (. . .) You can look at yourself: What exactly am I doing (. . .) You can better yourself and adjust your approach.”
Role play
After discussing the contributed fragment rehearsal (in role play) was also seen as a positive learning experience, because tips could be immediately applied. The professional who had contributed the fragment chose which tips to practice. One example: “For example, we practised using solution-focused questions . . . you really have to formulate your questions differently. If you’ve done it once, then you’ll try it again the next time” (professional).
Supervisors
Providing feedback required a great deal of creativity from both supervisors. Incorporating different methods for providing feedback (flipchart, oral feedback, post-its) helped to keep it fun and varied. Both supervisors learned a great deal from the supervisory sessions where they discussed their own recordings of the supervision sessions with the professionals.
They recognized the value of working with a strength-based approach in their own supervision and that of the professionals as a parallel process of working with the clients of both interventions. The suggestion was made in the interviews to create reminders to help professionals incorporate the tips and core components in daily practice. Busy work schedules cause these elements to quickly fade into the background as professionals cannot find the time to apply the agreed-upon core elements.
Preconditions
For this type of supervision to stand a chance of success, several organizational preconditions must be met. Quality equipment must be readily available to record sessions. Professionals should be able to view recordings anywhere (making a secure online environment for uploading and downloading a prerequisite). As acquiring clients’ permission to record conversations proved challenging, a well-formulated text or pamphlet appropriate for the target group could be helpful. Finally, adequate time must be made available for the lengthy nature of supervision, addressing recording sessions, viewing of the recordings, and preparing the supervision. It is expected that recording enough videos will not be an issue. For the purpose of the project, eight recordings were needed per professional, which was considered a burden.
Discussion
The goal of this project was to develop supervision for practice-based interventions and to test the effect on intervention fidelity. Applied to a small-scale project of professionals working with young people “in unprotocolled” coaching sessions in two interventions, group supervision occurred using video feedback, role play, a fidelity monitoring instrument and supervision of the supervisors.
Although it took some time for the professionals to become comfortable in asking youths’ (and sometimes their parents’) permission to record conversations, as well as making the actual recordings, ultimately working with video feedback in group supervision has increased the professionals’ enthusiasm, self-confidence, and awareness of working with the core components of the intervention.
Unfortunately, this positive picture from the interviews is not reflected in the quantitative data. Four out of six professionals showed improvement in treatment fidelity or one of its subscales. Had all participants shown progress, this could have been interpreted as an indication that targeted support of professionals contributes to increasing treatment integrity. However, not all project participants showed meaningful progress and progress did not take place in all core components. Moreover, other aspects of the data such as trend, overlap, and short phases, complicate assigning the improvement to the supervision. Two professionals showed a decline in quality in one component. As this was not a meaningful change it can be concluded that these professionals’ fidelity scores remained more or less the same; these professionals showed no development. All in all, some desirable changes occurred, but whether these changes were due to the video feedback is doubtful at least.
Influence of Age and Experience
There are several possible explanations for the heterogeneous results. First, other research shows that age and experience might play a part. For example, interviews with supervisors have shown that professionals with less experience benefit more from support (Goense et al., 2015), whereas experimental research by Bearman et al. (2013) shows that practice and modeling (in the pilot: modeling using video recordings) mostly impact older employees. However, differences in age and experience were not that substantial in this pilot, making attribution difficult. Moreover, one could argue that all professionals started the pilot with relatively high fidelity, making progress in the short time of the pilot difficult and perhaps not equally necessary in all cases.
Supervision Frequency
Monthly supervision occurred during this study. Over a limited period of time (estimate around 20 hours per person, based on 12.5–17.5 hours of group supervision over 8 months, plus time for producing recordings and preparing supervision) a great deal was accomplished.
In other EBIs there is a higher frequency of supervision. In PMTO, for example, twice monthly supervision is employed (Akin, 2016). In Multisystem Therapy (Henggeler et al., 1993) weekly supervision is the norm. Research in the application of supervision in evidence-based intervention shows that in practice supervision occurs less frequently than prescribed in the intervention. A high workload, which was also seen in our project, plays a role in this (Dorsey et al., 2017). It is possible that a higher frequency of supervision in our project would have led to other results.
Implementation of Supervision
This project has shown that supervision can be created for practice-based intervention. Interviews show that supervision based on a strength-oriented approach and learning culture stimulates professionals, resulting in active learning and skill building. These are important core functions of supervision in the implementation of interventions (Akin, 2016). As stated, the participants were previously unfamiliar with group supervision with a focus on fidelity. This form of support is to be seen as an implementation strategy, geared toward the competent delivery of practice-based interventions. It should not be underestimated that the adaption of a new work method such as this is in itself an implementation process. It is for good reason that several organizational aspects, which are known barriers in implementation processes, are mentioned in the interviews (Damschroder et al., 2009; Fixen et al., 2019).
In a next phase of supervision at both sites it is important to: (1) pay greater attention during group supervision to those core elements not yet fully applied, such as the application of techniques; (2) to pay attention to the use of rehearsal in role play during supervision; and (3) ascertain what consequences the development in treatment integrity has for client outcomes.
Limitations and Future Directions
The intervention period of this project was 8 months. During this time, each participant could only ask a learning question twice, and these (basic) learning questions mostly focused on the core component “contact.” Outcomes show that in a next phase supervisors could focus more on the application of specific core components (such as “techniques” or “goal orientation”) which now show (too) little progress or show a decline in quality.
Secondly, recording sessions with clients was experienced as challenging, especially during the baseline period. It took professionals some time to acclimate to asking client permission. In one organization, supervision did not start at the agreed upon moment, even though one of the professionals had already made arrangements with her clients to record sessions. Because of these practicalities, the number of recordings made during the baseline and during the intervention period differed. One professional only made one recording during the intervention period. This may have influenced the outcomes. In addition, recording situations were not randomly assigned, as getting permission and recording were novel aspects and professionals and clients had to get used to these. In a next phase of the supervision and research, random assignment of sessions to be recorded would be a possible solution to getting too many recordings during baseline or intervention phase.
Thirdly, the baseline as well as the intervention period were relatively short in the non-concurrent multiple baseline design. The design would have benefited from a longer baseline and intervention period, during which a larger number of measures could have been taken and the design could have been brought into greater alignment with the standards of multiple-baseline designs. In practice, it was challenging to acquire four measurements in each phase, resulting in phases consisting of less than three observations in four cases. Also, in a non-concurrent multiple baseline design, ideally the start of the baseline is simultaneous. When conditions change in one case only the data pattern in that case should change. If the data patterns in other cases change as well at the same time, there might be an external cause. This could not be controlled in the project as observations were executed in different timeframes. If this project is replicated, obtaining phase lengths of at least five data points within at least three cases that receive supervision in the same timeframe is recommended. Additionally, the fact that participation in the pilot was voluntary could influence outcome. It is possible that these professionals were already eager to learn. However, as two professionals showed no development this might not be the case. Also the fact that the intervention at site 2 only works with girls, compared to boys and girls in site 1, might be influencing the results.
Finally, evaluation of fidelity was done using an instrument developed for use in the supervision sessions. This instrument has not yet been validated and may pay insufficient attention to certain components. The appraisal in general was quite “crude.” Every recording was viewed in its entirety, regardless of length. It is probable that a 5-minute recording will be scored differently than a recording lasting 55 minutes.
Footnotes
Appendix
Operationalization of Three Core Components at Two Sites in Elements and Example Behavior.

| Core component | Element | Example behavior |
|---|---|---|
| Contact | 1. The professional is a good listener | Takes adequate time for the session and gives full attention Has an active listening attitude (friendly intonation/facial expression, nodding) Speaks calmly and clearly, is comfortable with silences Summarizes what was discussed |
| 2. The professional is involved and empathetic | Asks about the young person’s different areas of life Inquires about experiences, thoughts, and feelings Empathizes with the young person’s perspective Responds to and empathizes with what the young person is saying Gives compliments and magnifies success Names emotions and behaviors |
|
| 3. The professionals is predictable and consistent | Is clear about expectations within the conversation Is consistent in statements Is transparent about what information is shared with whom Is open regarding consequences and uses them consistently |
|
| 4. The professional connects with the young person | Adjusts attitude, tone, and language to the young person Begins at a low-threshold/is light-hearted and uses humor Considers the (im)possibilities of the young person Checks if the young person and professional understand each other |
|
| 5. The professional has an open and accepting attitude | Doesn’t judge or accuse Doesn’t show disappointment in the young person Relates, uses humor |
|
| 6. The professional acts as a positive role model | Is optimistic and shows confidence Demonstrates pro-social values (arrives on time, looks neat, does not smoke in view of the student) |
|
| 7. The professional is direct (extra element site 1) | Holds the young person accountable for his/her own responsibility where necessary Is realistic about the young person’s capabilities Repeatedly inquires about wishes and ideas |
|
| Application of techniques | 1. The professional uses feedback | Lists the pros and cons of behavior and its consequences Gives feedback on the behavior, not on the person Gives sincere compliments |
| 2. The professional provides insight into feelings, thoughts, and behavior | Investigates patterns in thoughts, feelings, and behavior with the 5G method Names helpful and disruptive thoughts Works with the top-10 cognitive distortions Explores with the young person the consequences of his/her behavior and alternatives |
|
| 3. The professional stimulates the young person to show alternative behavior | Practice alternative behavior with the student (role play) Make concrete agreements about how the student will self-practice Provides feedback on student behavior Explains, draws or makes behavior visual |
|
| 4. The professional applies solution-focused questions | Asks expectation questions Asks scaling questions Asks wonder-questions Focuses on solutions and strengths (re)Formulates plans in small steps |
|
| 5. The professional uses modeling (site 1) | Names experiences or examples from his/her own life or work Shows alternative behavior, for example, being able to receive feedback |
|
| 5. The professional uses motivational interviewing techniques (site 2) | Uses open questions Summarizes Reacts to resistance by taking the young person’s position and repeats arguments Provokes change language |
|
| Goal orientation | The professional works in a goal-oriented fashion | Determines the goal together at the start of a sessions Returns to previously set goals Asks targeted questions Guides the young person back to target when he/she strays Draws up concrete actions and plans together |
Acknowledgements
The authors would like to thank the staff working with interventions for young people at site 1 and 2, and the researchers and supervisors working at both organizations for their contribution to the practical implementation of the project. We thank (former) collegues Pauline Goense, Inge Ruitenberg, Claire Bernaards, Peter Kemper and Marinus Spreen for their constribution to the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by ZonMW under grant number 729102005 (2015).