
Abstract
Physical inactivity is common during periods of self-isolation, but for children with special needs, there are crucial benefits to be gained from maintaining moderate to vigorous physical activity throughout the COVID-19 pandemic. This study aimed to compare the physical activity levels of children with cochlear implants and their typically developed peers before and during the COVID-19 pandemic. The sample included 135 children with cochlear implants and 105 typically developed peers. We compared the daily activity levels of the two groups, measured by a 10-item questionnaire and the triangulation method. Results of this study showed that the girls were less active than the boys. Most items had adequate variance, and their means were close to the center of the range of values. The PAQ-C scores for the children with cochlear implants were distributed across a wider range than the scores for the typically developed children. Children with cochlear implants were physically active during school hours but were less active outside school, spending 3 to 6 hours per day using digital media during the COVID-19 pandemic. Children with cochlear implants need to increase their physical activity in and out of school by increasing their level of independence and their ability to adapt to social life. Giving information about physical activity opportunities to parents of children with cochlear implants is an important issue. School presents an opportunity for children to engage in regular physical activity, which is beneficial for their health status.
Introduction
Physical activity (PA) is essential for health, and it is especially associated with psychological benefits in children (e.g., improving their ability to control symptoms of anxiety and depression). It also supports social development by providing opportunities for self-expression, the development of self-confidence, social interaction, and integration (WHO, 2018). PA for children includes play, games, sport, chores, recreation, physical education, and planned exercise with family, in school, and in community activities (WHO, 2011). One of the primary aims of the Turkish education system is to promote physical education and sport activities for children at all levels of schooling by structured PA to instill lifelong PA habits in children. However, children in Turkey are now experiencing an extraordinary change in lifestyle because of the COVID-19 pandemic, during which schools have been closed and are not expected to reopen this academic year. Prior to the COVID-19 pandemic, PA adjustments were made by the Turkish Ministry of National Education (2006) as follows:
- Unstructured PA twice a week in primary and secondary schools (40 minutes per lesson)
- Structured PA twice a week in high school (40 minutes per lesson)
A curfew for children in Turkey under the age of 20 was implemented on April 4, 2020. Behavioral strategies for social distancing and hygiene are other valuable methods to limit the spread of COVID-19 and reduce morbidity and mortality in children. However, the public health restrictions (i.e., stay at-home orders, and closures of parks, pools, and sport schools) have the potential to reduce unstructured PA, which is unfortunate because daily PA may help combat the disease by boosting children’s immune systems and helping children maintain a healthy weight (Woods et al., 2020). Although the effects of the COVID-19 pandemic on children are still being studied, it will have long-term effects on children’s health status because of social isolation and reduced PA. It is well known that the development of self-esteem, body image, and mental performance is facilitated by PA, and the frequency of cigarette, alcohol, and drug use is lower in children who engage in regular PA. Children who do regular PA are also less likely to have behavioral disorders and to have a higher academic performance than children who do not do regular PA (Kayıran, 2016). Participation in PA is associated with strong social integration among children, including building friendships and enhancing social skills. These benefits are especially important for children with hearing impairment.
The health status of children with a hearing impairment has recently been assessed in terms of their delayed motor development or poor motor proficiency traits (Engel-Yeger & Weissman, 2009). PA has a positive effect on development, which is partly because of the physiological changes in the body in children with a hearing impairment. It is also reported that the motor skills of children with a hearing impairment may influence their cognitive development. In fact, the literature consistently reports that increased PA time in school has a positive effect on academic performance, executive functions, and on-task behaviors of children with a hearing impairment (Zeng et al., 2017). Therefore, both structured and unstructured PA are essential for children with a hearing impairment. In PA studies of children with a hearing impairment, we identified gender was a relatively consistent determinant of PA, and boys were significantly more physically active than girls.
No previous study has examined PA in children with cochlear implants even though the physical activity is the most valid rehabilitation option for children with hearing impairment. Cochlear implants play an essential role in the quality of life and overall health of children with a hearing impairment (Lenarz et al., 2017). However, the avoidance of structured or unstructured PA by children with cochlear implant increases the risk of inactivity and its side effects. Therefore, children with cochlear implants are at risk for severe health problems both before and during the COVID-19 pandemic. PA among children with cochlear implants is one of the significant determinants for protecting and enhancing their health status, and their PA levels have decreased markedly because of the COVID-19 pandemic. Therefore, this study focused on children with cochlear implants. Previous studies showed that school-age children with hearing impairment were more active and more likely to take part in sport and leisure activities than other children with sensory deficits (Lieberman et al., 2000; Longmuir & Bar-Or, 2000; Williams et al., 2018). Results from a nutrition and health survey showed that adolescent obesity is associated with a higher prevalence of sensorineural hearing loss in adolescents (Kohlberg et al., 2018). We expect that the COVID-19 pandemic is likely to double out-of-school time this year for many children with cochlear implants in Turkey, and this will exacerbate the risk factors for inactivity associated with the summer recess. As a result, it is important to assessing PA in children with cochlear implants. The Physical Activity Questionnaire for Older Children (PAQ-C) provides a general measure of PA for youth from grades 4 to 12 (approximately ages 8–13). The purpose of the PAQ-C is to ensure that we can easily administer the PAQ-C measures before COVID-19 pandemic and during COVID-19 pandemic.
The present study aimed to investigate cochlear implantation as a risk factor for children’s inactivity through a PAQ-C questionnaire before and during the COVID-19 pandemic. We also aimed to identify COVID-19’s long-term risk factors in children with cochlear implants. Our research questions were the following: (1) what is the physical activity (PA) level of children with cochlear implants? and (2) what are factors that impact their PA levels? The findings of this study are important for health professionals, teachers, and policy makers in developing interventions to increase the PA participation of children with cochlear implants.
Materials and Methods
Data for this study came from a cross-sectional pilot study of parents of hearing-impaired children between the ages of 7 and 15, conducted from May 2018 to the present. No participants reported a pre-existing diagnosis of metabolic syndrome. The study was approved by the local ethics committee (project no. 10848, May 2018) and, during COVID-19, Turkish by the Ministry of Health (project no. Senkal-2020-06-18T11_08_02). The study was conducted in accordance with the Helsinki Declaration of 1975. Parents gave verbal and written consent prior to the COVID-19 pandemic after listening to a research assistant read aloud an approved script describing the study in easy-to-understand language. The script explained the study procedures and expectations (i.e., how to complete the questionnaire), and parents were also encouraged to ask questions.
Turkish Health Promotion Context
One of the primary goals of health promotion and health policy in Turkey is to encourage healthy lifestyle habits and to develop the knowledge, attitudes, and behaviors of individuals in society. The Ministry of Health of Turkey supports these goals by emphasizing the importance of health promotion as a process of empowerment where citizens increase attention to their own health, promote their own health conditions, and raise awareness regarding health issues. The main organization that ensures the participation of individuals with a disability in sports and physical activity in Turkey is the Ministry of Youth and Sports, and all the Federations of Sport for Individuals with a Disability. School-based health promotion is a legal requirement in Turkey (Turkish Law Enforcement About National Health Services Guideline; Number 154). However, in Turkey, where 12.29% of the population has a disability, there is a significant need for sports trainers and physical education teachers for individuals with a disability. As of the 2011 to 12 academic year in Turkey, there were 303 special education primary schools, 102 special education secondary schools, 110 special education schools, 1,134 schools with special education classes, and 6,060 special education classes in public schools. Apart from public and private special education schools, there are 1,591 special education and rehabilitation centers throughout Turkey. At the end of the third year of the “Education Overcomes All Obstacles” Campaign, which was initiated in 2009 under the auspices of the President of the Republic of Turkey, the Ministry of National Education, the Ministry of State responsible for the Disabled, and the Turkish White Moon Association, the number of students with disabilities in special education settings had increased by 144%. Today, parents make health decisions for their children with cochlear implants, and parents can provide their children with cochlear implants positive health promotion information to assist them adopt physically active lifestyle behaviors.
Participants
The participants in the study group were children with cochlear implants from two cities in Turkey (Adana and Istanbul). A total of 135 children who attended special education and rehabilitation centers and public elementary schools were invited to take part in the study (all of whom had profound congenital hearing loss, ranging from 75 to 100 dB). They had all been fitted with a cochlear implant unilaterally before the age of three: 43 children had received a Nucleus 22 or Nucleus 24 (Cochlear, Australia); 55 children had received a Maestro (Med-el, Austria); and 37 children had received an Oticon Medical Digisonic SP (William Demant Holding A/S, Denmark). One hundred and five typically developed children from public elementary schools from two cities in Turkey (Adana and Istanbul) were also invited to take part in this study as controls (Figure 1).

Distribution of participants of this study.
The Physical Activity Questionnaire for Older Children (PAQ-C)
The PAQ-C was used in this study to obtain data about children’s PA levels. The PAQ-C is a valid and reliable, self-reported, 7-day recall measure of PA in children (Kowalski et al., 2004), adapted for the Turkish context by Erdim et al. (2019). We asked children with cochlear implants and their typically developed peers to report the types and intensity of PA they had experienced within a particular seven-day period prior to and during the COVID-19 pandemic. The PAQ-C consists of ten questions, nine of which focus on the child’s PA and are scored using a five-point Likert scale. Each question has a maximum score of five, where 1 = a low level of activity and 5 = a high level of activity, for a maximum total score of 45 (Erdim et al., 2019; Kowalski et al., 2004). The 10th item in the questionnaire asks whether the child was sick, injured, or had experienced any other events that prevented him or her from engaging in regular PA the week prior to completing the questionnaire.
Measures
We used methodological triangulation to determine the effect of cochlear implantation on the participants’ levels of physical and recreational activities (Figure 2). Before the COVID-19 pandemic, PAQ-C questionnaire with children and exploratory interviews with the mothers of children fitted with cochlear implants were carried out. The PAQ-C questionnaire was administered again during the COVID-19 outbreak, and interviewed with mothers again by telephone.

Methodological triangulation method of obtaining data about the PA of children with cochlear implants (Denzin, 2012).
Phase one: PAQ-C Questionnaire
All the children in the study completed the PAQ-C in a special education and rehabilitation center during their formal education time. Children who needed help completing the PAQ-C were assisted by a parent. The average time taken to complete the questionnaire was 15 minutes. At the time of the COVID-19 pandemic, the PAQ-C was implemented as an online survey (Google forms) on June 5, 2020 and shared with respondents (via their parents) by sending a link to a mobile phone and emailing a message to the children. Data gathered using Google forms are typically stored in a spreadsheet.
Phase two: Interviews with mothers
The second phase of our study involved interviews with 68 normally-hearing mothers between the ages of 22 and 46 regarding the PA of their child. They were interviewed by the two authors of the study face-to-face once before the COVID-19 pandemic and by telephone once during the pandemic. We asked the mothers eleven questions in a semi-structured format (see Appendix A). Each interview lasted about 45 minutes and was tape-recorded and transcribed verbatim by the first two authors. Ary et al. (2010) stated that interviewing is one of the most widely used methods for obtaining qualitative data. During the interviews, the mothers were asked to elaborate on the PCR-Q questionnaire completed by their child. The questions aimed to reveal the level of activity of children with cochlear implants by, for example, assessing the child’s screen time (TV or video) (e.g., “Over the past 30 days, on average, how many hours per day did your child watch TV or videos?”); based on the recommendation of the American Academy of Paediatrics (AAP), the variable was categorized as 1 ≤ 2 hour per day and 2 > 2 hour per day (Calvert, 2015). The first two authors independently read each transcript to identify emerging themes.
Phase three: Documentary analysis
Two of the 135 mother of cochlear-implanted children shared photographs they took during their quarantine. The photographs provided another way for the children with cochlear implants to symbolically express their thoughts and feelings about their quarantine experiences (Johnson & Weller, 2002).
Sample Size Calculation and Statistical Analysis
The Kolmogorov–Smirnov test was used to test the normality and outlier. The values of skewness and kurtosis were applied to determine whether data transformation should be performed. Means and standard deviations (SD) were calculated for boys, girls, and combined samples for individual items and total PAQ-C scores. Descriptive statistics were used to characterize the data. Based on the type and distribution of the data, non-parametric (Mann–Whitney U) tests were used to assess the differences between girls and boys and between the study and the control groups before and during the COVID-19 pandemic. All statistical analyses were performed using SPSS version 22.0 (SPSS 22.0, IBM Inc., USA), and a two-tailed p value of <.05 was considered statistically significant.
Results
Children with incomplete data and those who reported sickness or other events that prevented them from participating in their usual activities during the previous 7 days were excluded. The study group comprised 135 children (60 females and 75 males) with a mean age of 10.26 (SD: 1.02) years (range: 9–13 years old); the control group included and 105 children (60 females and 45 males) with a mean age of 10.59 (SD: 1.04) years (range: 9–12 years old). The Kolmogorov–Smirnov test revealed that the PAQ-C scores were not normally distributed for both groups before the COVID-19 pandemic (study group = 0.017; control group p = .00) and during the pandemic (study group = 0.00; control group p = .00) (Table 1).
PAQ-C Responses by Question.

Note. SD = standard deviation.
Most items had adequate variance, and their means were close to the center of the range of values. The PAQ-C scores for the children with cochlear implants were distributed across a wider range than the scores for the typically developed children. The typically developed children (the control group) had higher mean PAQ-C scores (Q 2, 3, and 4) than the children with cochlear implants (the study group) during school hours before the COVID-19 pandemic. The mean PAQ-C summary score was 2.98 (SD: 0.49) for the children with cochlear implants (the study group) and 3.71 (SD: 0.63) for the typically developed children (the control group) before the COVID-19 pandemic (Figure 3). The PAQ-C results showed that the typically developed children’s mean PAQ-C scores (control group mean PAQ-C score = 3.71) were higher than those of the children with cochlear implants (study group mean PAQ-C score = 2.98) before the COVID-19 pandemic, and the difference was statistically significant (p = .00) (Table 2). The mean PAQ-C scores of all the children (both study group and control group) decreased during the COVID-19 pandemic (Figure 3). However, the difference between the study group and control group was not found to be statistically significant during the COVID-19 pandemic (p = .68) (Table 2).

The PAQ-C scores comparison study and control groups of the children before and during the COVID-19 pandemic.
Statistical results before and during COVID-19 pandemic of study and control groups.

Figure 4 shows the PAQ-C scores of the children separated by gender before and during the COVID-19 pandemic. Figure 4 shows that the girls were less active than the boys (Figure 4). The mean PAQ-C score for females in the study group before the COVID-19 pandemic was 2.83 (SD: 0.59), and it was 3.41 (SD: 0.51) for males. The mean PAQ-C score for females in the control group before the COVID-19 pandemic was 3.60 (SD: 0.67), and it was 3.85 (SD: 0.7) for males. The mean PAQ-C scores and each item score before the COVID-19 pandemic (p = .00) shows that boys were significantly more active than the girls. The mean PAQ-C scores decreased during the COVID-19 pandemic, and statistically significant differences were found among boys and girls (p = .003) (Table 3).
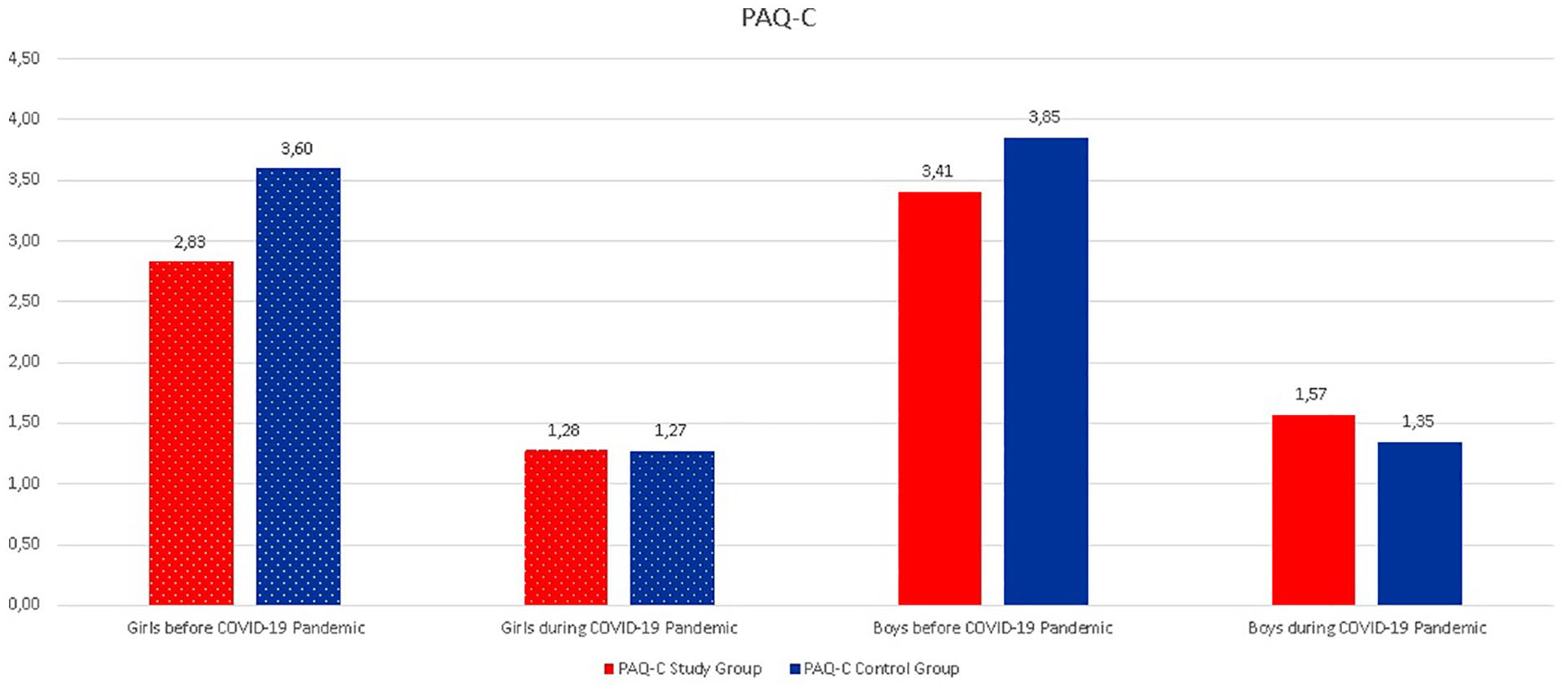
PAQ-C scores comparison of the children separated by gender before and during the COVID-19 pandemic.
Statistical results before and during COVID-19 pandemic of boys and girls.

“Daily Life”
For the mothers taking part in this study, taking care of their child with cochlear implants is an activity that takes most of their time: “. . .. you have to feed him, dress him, and watch over him because, just like that, if he falls, he throws himself down. Or if he drops his cochlear implant device. . . So, you have to stay with him 24 hours a day” (M62).
The mothers’ adjusted their daily routines and time organization to those of their child with cochlear implants: school, home, transport to the rehabilitation center, return home, home tasks, cleaning, etc. One of the mothers stated: “My child, for example, on weekdays he does not have time for PA. He can’t go to the park, he can’t play with other children; he can’t, because he doesn’t have time in the afternoon” (M5).
“. . ..I know, that many water sports do not present any risks for cochlear implant users as long as the sound processor is removed. My daughter removes her speech processor before swimming. Our audiologist told us that there will no risk when not wearing the speech processor during swimming. However, she swims only in summer holidays” (M22) (Figure 5).
Swim pool activities of a girl with cochlear implants.
“Physical Education Class”
During the time their children spend in school, the mothers stayed next to the school building. The mothers who took part in the interviews before the COVID-19 pandemic tried to keep their child with cochlear implants away from physical education class, as they thought their child could damage their cochlear implant devices. It was found that they lacked knowledge about which physical activities they could safely encourage their child to take part in. A mother (M3) stated: “. . . I don’t not know how to train my child to protect their cochlear implant devices from being damaged,” while another mother stated that she lacked knowledge about the physical education class at school and, therefore, did not encourage her child to take part in it.
“Reduced Physical Activity”
The mothers indicated that taking care of their child with cochlear implants was an activity that took most of their time as illustrated by the following quotations: “. . .she was going to the rehabilitation centre and also to the speech therapy. She had to quit several things because we don’t have time” (M5) (Figure 6). “. . ..My child stayed away from streets, playgrounds, and schools, so I am glad that this was reducing the chances of the cochlear implant devices getting damaged” (M19). “. . .I am worried that my child would suffer due to damage to their cochlear implant devices” (M12) “. . Children with cochlear implants aren’t getting enough PA. My child has a hard time using some playground equipment. He has trouble with climbing ladders, using the monkey bars, swinging and even sliding require being able to coordinate many different body movements.” (M47).

Playground activities of a boy with cochlear implants and his sister.
During interviews to validate data during the COVID-19 pandemic (conducted by telephone), all mothers reported that their children stayed away from streets, playgrounds, and the mothers were glad that this was reducing the chances of the cochlear implant devices getting damaged. Mothers were particularly worried that their children would suffer due to damage to their cochlear implant devices.
“Screen Time”
Mothers of children with cochlear implants also reported in their interviews that their child spent more time on screens during the COVID-19 pandemic than before the pandemic: “. . .My child would spend three to six hours per day on screens before the COVID-19 pandemic and that the time has increased during the COVID-19 pandemic to between five and seven hours per day” (M11).
It was noted that the mothers played a more active role than fathers in caring for and educating their children with special needs.
Discussion
Cochlear implantation is the best rehabilitation modality to restore hearing in severe to profound hearing impairment. Recently, studies on children with cochlear implants have typically focused on children’s speech and language development and their association with quality of life. However, the younger age at cochlear implantation and the application of bilateral cochlear implantation create the risk of cochlear implantation–induced motor developmental problems (Gheysen et al., 2008). Engel-Yeger and Weissman (2009) reported delayed motor development or poor motor proficiency traits in children and adolescents with hearing impairment. The literature suggests that children with hearing impairment tend to score lower than their typically developed peers on motor test items that require good control of balance (Engel-Yeger et al., 2004; Livingstone & McPhillips, 2011), and studies have linked poor kinesthetic integration and balance abilities in children to hearing impairment (Dair et al., 2006; Ellis et al., 2005; Jernice & Nonis, 2017). Environmental constraints on PA for children with hearing impairment include an unstructured physical education curriculum, inadequate instruction time, and limited physical activity opportunities (Gheysen et al., 2008). Environmental factors like early inclusive education and parental involvement in physical activity seem to influence motor development in children with cochlear implants. Therefore, it is important to compare the physical activity levels of children with cochlear implantation with the PA levels of their typically developed peers.
PA has many health benefits for all children (Burns et al., 2015). The children with cochlear implants in our study had a mean PAQ-C score of 2.98 (SD: 0.49), which was lower than that of their typically developed peers. Consistent with previous PA level assessment studies, the finding from the current study revealed that the Turkish children showed higher levels of PA (Erdim et al., 2019). Erdim et al. (2019) found that the PAQ-C total scores of Turkish students (3.16, SD: 0.73) were similar to those of children of similar age in different countries. However, in our study, the mean PAQ-C total scores for the control group (3.71, SD: 0.63) were higher than Erdim et al.’s findings. Environmental factors can affect the physical activity rates of children. However, this finding calls for action to improve PA among Turkish children with cochlear implants. The effects of environmental factors on children’s activity levels need to be studied further.
The impact of COVID-19 and the related physical inactivity on the health of cochlear-implanted children has not been studied so far. It has been shown that daily exercise may help development of a child, which is partly because of the physiological changes in the body in child with a hearing impairment. Moreover, children with cochlear implants have delayed motor development or poor motor proficiency traits, which worsened during COVID-19 pandemic. Thus, this study aimed to examine PA levels in children with cochlear implants (aged between 9 and 13 years old) before and during the COVID-19 pandemic. In our study, all of the children’s scores decreased dramatically during the COVID-19 pandemic. The mean of the second item on the questionnaire (Q2) (relating to PA carried out during physical education classes) was high in typically developed children (3.61, SD: 0.26) and very low in children with cochlear implants (2.59, SD: 1.1). This was below other reports of Turkish (4.52, SD: 0.99) (Erdim et al., 2019), British (4.14, SD: 0.80) (Thomas & Upton, 2014), Chinese (4.04, SD: 0.98) (Wang et al., 2016), and Italian (3.96, SD: 1.13) (Gobbi et al., 2016) samples. Parents of children with cochlear implants pay extremely close attention to their children and their children’s experiences and problems (particularly at educational institutions), and they reported keeping them away from physical education classes. This could be the reason why children with cochlear implants reported not being active in these lessons. The children’s scores on the second item also decreased dramatically during the COVID-19 pandemic. As noted by the authors of previous studies, the lasting effects of the COVID-19 pandemic will not be fully realized for some time. Because of the COVID-19 pandemic, we showed that this health crisis has the potential to increase physical inactivity among children with cochlear implants as well as among typically developed peers. Children with cochlear implants were physically active in their daily activities in terms of daily mobility (Q8 and Q9) before the COVID-19 pandemic, but school-based PA is in question.
In Turkey, physical education lessons are not different from lessons in other subjects in terms of teacher-student communication and interaction. Essentially, physical education and sports activities are part of general education and can be carried out at every day. Usually, physical education consists of 40 minutes of activities per week. However, parents of children with cochlear implants often apply to the school authorities to have their child excused from physical education and sports lessons to avoid potential damage to their child’s cochlear implant device.
Most means for items in the questionnaire were close to the center of the range of values for typically developed children. However, the mean PAQ-C item values for children with cochlear implants were lower than those for typically developed children. In particular, the PA levels of children with cochlear implants were lower outside of school (after school, evenings, and weekends), although physical activity outside of school is vital for children’s health. Children who engage in activity outside of school and during school hours have higher daily physical activity levels (Howie et al., 2010). This finding was a key contributor to overall PA levels among children with cochlear implants, reinforcing the need for interventions targeting families, the community, and schools. Engel-Yeger and Hamed-Daher (2013) stated that children with hearing or visual impairments might have limited participation in physical activities. Children with sensory loss who take part in social activities within and outside school experience a better quality of life (Engel-Yeger & Hamed-Daher, 2013; Howie et al., 2010; WHO, 2018). However, children with cochlear implants have been found to engage in fewer activities outside of school.
The mean of the PAQ-C checklist, which is the first item of the questionnaire (Q1), was found to be a little lower than that of the other items for boys with cochlear implants (1.92; SD: 0.66) and even lower for girls with cochlear implants (1.33; SD: 0.67). Typically developed children had slightly higher scores than children with cochlear implants. Typically developed boys had a mean score of 2.08 (SD: 0.67), and girls had a mean score of 1.76 (SD: 0.73). This outcome is lower than the results reported in another study (2.11; SD: 0.59) conducted with typically developed Turkish children (Erdim et al., 2019). This is interpreted as being a consequence of the many activities covered by the checklist and because the children did not perform most of them. In this study, we observed differences between boys and girls in terms of the PA levels of children with cochlear implants and that of their typically developed peers, and our findings are consistent with previous studies (Lieberman et al., 2000; Longmuir & Bar-Or, 2000; Williams et al., 2018). The mean score for the Turkish version of the PAQ-C was significantly higher in males than in females in the study group. Sallis et al. (1992) investigated the epidemiology of PA among children and found that males were more active than females. The results of our study are in line with those of Sallis et al. (1992) for children with cochlear implants. Descriptive epidemiological studies of PA levels in children have consistently reported that males were more active than females (Sallis et al., 1992; Trost et al., 2002). In our study, more boys with cochlear implants took part in school-oriented physical activities than did girls with cochlear implants. Globally, girls are less physically active overall than boys. Differences in cultural norms and potential differences in the role of males and females in the social life of Turkey, combined with parents’ knowledge and awareness levels, may explain this result.
Besides the PAQ-C data, interviews were conducted with the children’s mothers in our study. Creswell and Plano Clark (2007) stated that data should be collected through several sources (e.g., interviews, observations, and document analysis) as this triangulation in data collection ensures internal validity. Therefore, to strengthen the validity of the PAQ-C, it is advisable to use two different data collection methods so that the validity and reliability of the questionnaire can be proved. In interviews with the mothers of children with cochlear implants, the mothers stated that they worried about their children’s cochlear implant devices, so they had decreased the amount of PA that their children engaged in before the COVID-19 pandemic. Results of this study shows that children with cochlear implants are not denied access to PA, but their mothers impose restraints. Therefore, increasing PA levels among children with cochlear implants depends on parents’ knowledge and awareness. Parental education is a crucial component of clinical services after diagnosis of a child’s hearing loss to help parents prepare for the challenges that they may encounter daily. A disproportionate number of children with a hearing impairment come from low-income family backgrounds and use medical services less frequently (Rajendran & Roy, 2010). Social inequalities and relative poverty among families with children with hearing impairment can lead to stress and social exclusion, which has been found to worsen the PA levels of children with hearing impairment (Jernice & Nonis, 2017) .
The importance of parents’ participation in their children’s education program, especially parents of children with special needs, was first highlighted with the “Education for All” law implemented in the United States in 1975. The laws in Turkey (Turkish Ministry of National Education, 2006) state that the participation of families who have children with disabilities is a necessity at every stage of a child’s education. In Turkey, based on the Decree Law No. 573, which came into force in 2000, as well as on the “Special Education Services Regulation,” which came into effect on May 31, 2006, families are encouraged to actively take part in the assessment of their child, the preparation of an individualized education program, the child’s education process, and the assessment of the education process. Schools with a commitment to parent involvement take an active role in helping parents learn a variety of ways to be involved.
Parents, especially mothers, are likely to influence the access to and participation in sports experiences of their children with disabilities. Nixon stated that parents of children who were blind or visually impaired tended not to be strong encouragers of their children’s involvement in sports, which resulted in relatively few of these children participating in sport (Nixon, 2007). Although children with cochlear implants are a relatively small population, the current study provides some valuable insights about PA and the approach of parents. Parents of children with cochlear implants may be most comfortable with sports that are structured to pose a low risk and over which they have some control. The inclusion of children with cochlear implants in sports clubs may be the best option (Geidne & Jerlinder, 2016).
Limits
This study has several limitations. The PAQ-C was designed for children aged 8 to 14. However, although the age range of children who participated in the current study was 9 to 13 years, the number of participants was small, and the sample was drawn only from Turkish children, which may limit the generalizability of the results. Additional studies are needed to examine the PA of the children with cochlear implants during the COVID-19 pandemic worldwide.
Conclusion
Children with cochlear implants were physically less active before COVID-19 pandemic in their daily activities than were their typically developed peers. However, we want to call attention to the pandemic’s longer-term effect on the health of children with cochlear implants. School closures during the pandemic may exacerbate the coordination and balance problems of children with cochlear implants and increase the disparities in obesity risk. Sedentary activities and screen time are expected to increase during the pandemic and may negatively influence speech and language development of children with cochlear implants.
During periods of isolation, children with cochlear implants should maintain good health by following the WHO PA recommendations for 60 minutes of moderate-intensity PA per week. Cochlear implant users are strongly advised against sports in which physical injury or blows to the head are likely or inevitable. It is possible to take part in sports for which helmet is recommended (cycling, horseback riding, sailing, skiing, etc.). It is important that no pressure be directly applied to the cochlear implant area or the scar. Many water sports do not present any risks for children with cochlear implants as long as the sound processor is removed, including swimming, diving in shallow water down to 3 m deep, and sailing. Examples of home exercises not requiring a large space or special equipment and easily practised at all times of the day include walking, stair climbing, lifting and carrying groceries, chair squats, push ups, sit-ups, rope jumping, yoga.
In conclusion, using a cochlear implant should not affect children’s activity levels if proper parental information given by audiologist, sport coaches, and teachers. However, the COVID-19 pandemic has increased the risk of inactivity. Children with cochlear implants need to increase their PA levels in order to increase their independence and become better able to adapt to social life. Providing parents with knowledge and awareness about the importance of PA for their cochlear-implanted child is essential as parental engagement crucially impacts the health status of children with cochlear implants.
Footnotes
Appendix A
Interview Protocol for Parents
Acknowledgements
The authors are thankful to the parents of cochlear-implanted children who participated in this study and to our families for their support during the COVID-19 pandemic.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.