
Abstract
Medical education aims to train professionals who are capable of making extremely complex decisions. As part of the medical curriculum, bioethics education could have an important role in promoting moral development and decision-making in medical students. This study aims to determine if, after a Bioethics and Professional Deontology course, medical students would present a change of opinion on three ethical dilemmas. A quantitative and longitudinal study was developed by applying the MCTxt (Moral Competence Test extended), composed of three ethical dilemmas (Worker, doctor, and judge dilemmas), to a sample of 70, fourth year medical students, from a Portuguese medical school. The questionnaire was applied at the beginning and end of a bioethics course, with a 3 month time interval. For this study the opinion scores were analyzed and described using the mean and standard deviation. The comparison of these scores, at both times, were performed using t-tests for paired samples. A significance level of 5% was used. For students who were neutral in the first application, the majority went on to agree or disagree with the performance of the dilemma character, ultimately showing less indecision at the end of bioethics course. The results suggest that, after the bioethics course, students have lower indecision, however the changes were very tenuous. Bioethics education is important to promote more opportunities for reflection and discussion, to stimulate critical judgment, and the ability to make decisions by medical students. Further research could help to better understand this subject.
Introduction
With the development of new technologies in the field of medicine, numerous ethical dilemmas arise for which doctors must be prepared to respond. Doctors are expected to be professionals par excellence who make many decisions related to people’s health, and to have a focused preparation for the care they will provide. Therefore, the medical students’ education must promote their capacity for reflection as well as the ability to make judgments and decisions that focus not only on the decision-making act itself but also the capacity to justify those decisions (Caldicott & Danis, 2009; Ricou & Marina, 2020; Tsai et al., 2009).
In Portugal there are eight medical schools, the medical degree is structured into six academic years, with a total of 360 ECTS (European Credit Transfer System). One of the objectives of the course is to provide a fundamental knowledge of Bioethics and Ethics in Medicine (Conselho de Escolas Médicas Portuguesas, 2021). The main aim of the bioethics course is for students to gain an understanding of ethics in healthcare, particularly the relationship of the ethical dimension of health and disease with the medical profession. The bioethics course allows the student to develop critical thinking and decisions-making competencies expected of the medical profession. The students must also be taught the precepts of medical deontology so that their practice develops according to the principles that ethically guide medicine (FMUP, 2021; Nunes, 2002).
There is a lack of consistency in curriculum planning for bioethics education in Portuguese medical schools. Bioethics may be taught in different curricular years at each school (Conselho de Escolas Médicas Portuguesas, 2021). In the medical school where this study was developed, bioethics is taught in the fourth academic year with 30 hours of workload dedicated to it. This is composed of 18 hours of seminars and 12 hours of group work. The seminars involve guided discussion between teachers and students based on predefined topics. Whilst the group work combines analysis and problem solving skills coordinated by teachers with the active participation of students, followed by a presentation of a case scenario by the students. Some of the topics covered by this module include concepts and definitions of ethics, bioethics, and principles of biomedical ethics; the clinical relationship, privacy, and confidentiality in clinical practice and medical responsibility; ethical issues at the beginning and at the end of human life; other ethical issues such as transplantation, genetic diagnosis, genetic intervention in man, experimentation in humans, and the use of the human corpse in medicine; HIV infection; ethics committees for health; ethics and epidemiological research; ethical issues in evidence-based medicine; allocation of resources for health and distributive justice and drug policy; and Biolaw (FMUP, 2021).
In a recent study carried out in Portugal, it was found that students show a stagnation in moral competence after bioethics education (Martins et al., 2021), this is the ability to make a decision and act in accordance with that decision (Lind, 2016). This leads us to consider the role of bioethics education in decision-making and the change of opinion in medical students.
Some authors have proposed that the current ethics training is insufficient (Roberts et al., 2004, 2007) and that learning environments are not conducive for ethical reflection (García-Mangas et al., 2016), further arguing that bioethics education should be integrated throughout the whole duration of medical education (Asghari et al., 2009), and should be adjusted to each real caring situation (Abma et al., 2009).
Bioethics education should not be based solely on an approach to concepts and the use of expository methods, but it should promote the discussion of practical cases experienced in clinical practice, resorting to moral deliberation, the exchange of experiences, and the sharing of concerns and doubts (Abma et al., 2009; Asghari et al., 2009; Heidari & Ebrahimi, 2016; Roberts et al., 2007; Serodio et al., 2016; Zoboli, 2013).
Research shows that medical students consider bioethics education to be essential for the medical profession, and that training could lead to better ethical practice and decision-making (AlMahmoud et al., 2017; Greenberg et al., 2016; Liu et al., 2018; Savitha et al., 2018). However some students consider that bioethics education before clinical exposure makes it difficult to relate to the situations described in theory, and that bioethics should not only be formally taught but also imbibed by observing behavior (Savitha et al., 2018), endorsing the value of positive role models (AlMahmoud et al., 2017).
Theoretical Framework
Kohlberg (1964) developed his research in moral growth and presents moral judgment competence, as “the ability to make decisions and to judge morally, based on internal principles, and to act in accordance with such judgments.” According to the author, individuals, regardless of their origin or cultural influences, go through an evolutionary sequence of universal stages, although not all individuals reach the highest levels. Kohlberg argues that environments in which the individual takes responsibility for their actions, develops the ability to work in groups and share decision-making, can stimulate high levels of moral development (Kohlberg, 1958).
Lind (2016) based on Kohlberg’s definition, presents moral competence as “the ability to solve problems and conflicts based on a moral principle, through deliberation and discussion, rather than the use of force, power, or violence.” The author draws on Piaget’s Double-Aspect Theory toward a new approach to the cognitive and affective aspects of moral behavior. Lind argues that the relationship between moral orientation and moral competence are parallel in normal situations, however, when there is punishment or reward for certain actions, this can lead an individual to respond based on what is considered to be the appropriate response when making a certain assessment. Lind developed a questionnaire, the MCT (Moral Competence Test), which allows the determination of the C score and the opinions of individuals on three ethical dilemmas thus reflecting the individual’s ability to choose arguments in favor or against a moral option. According to the author, moral competence is not innate and does not develop on its own, it must be taught and reinforced, and the quality and quantity of education are important factors in the development of moral competence.
Studies considering the influence of bioethics education on moral competence of medical students are scarce. Serodio et al. (2016) developed a longitudinal study in which they accompanied two groups of students before and after teaching the discipline of bioethics. One group was subjected to the traditional teaching method and the other group had a complement with the Konstanz Method of Dilemma Discussion. The authors verified that both groups presented a stagnation on moral competence, although the group subjected to the Konstanz Method of Dilemma Discussion presented a slight increase in the moral competence scores, whilst the other group presented a decrease in those scores (Serodio et al., 2016). Given these results, the authors argue that the implementation of different teaching and learning methods may promote the moral development of medical students (Serodio et al., 2016). Martins et al. (2021) compared the moral competence of medical students at the beginning and end of the bioethics course, concluding that the students present a stagnation on moral competence scores, with lower scores of moral competence after the bioethics course. The same authors developed the present study as a more in-depth study of these results to verify whether, after being exposed to bioethics education, the students would change their opinion previously expressed about the three ethical dilemmas comprising the questionnaire.
Aim
This study aimed to determine if, after being taught a course of Bioethics and Professional Deontology, medical students would present changes in their opinion regarding three ethical dilemmas.
Method
Study Design
A quantitative and longitudinal study was developed by applying the MCTxt questionnaire (Moral Competence Test extended) to medical students at a Medical School in Northern Portugal. The bioethics course is taught to the fourth year students for 3 months. The questionnaire was applied to those students who attended this curricular year at the first and the last class of Bioethics. The questionnaire was administered at the beginning of the class, after the researcher explained the objectives of the study, and informed consent was collected. Attached to the questionnaire the participants were asked to provide demographic data, such as gender and age. On average, the students took 15 to 30 minutes to complete the questionnaire, with no time limitation to finish, as suggested by Lind (2016).
Data collection instrument: The questionnaire applied was the MCTxt (Moral Competence Test extended), composed of three moral dilemmas, developed by Lind (2000) and adapted to the Portuguese language by Bataglia et al. (2003). This instrument allows the simultaneous determination of the C score, concerning moral competence, and the individual’s opinion regarding the characters’ performance. For this study, the data regarding the students’ opinions about the three ethical dilemmas comprising the questionnaire was analyzed. In the first dilemma, the main characters are the workers who decide to break into the company where they work to find evidence on how the bosses illegally record workers’ conversations to fire them. In the second dilemma, at the request of a terminally ill cancer patient, a doctor administers a lethal dose of morphine to help the patient die faster. In the third dilemma, a judge authorizes the torture of a woman who is suspected to belong to a terrorist group in order to prevent an imminent attack that will lead to the deaths of 100s of people.
For each dilemma, the participant judges the main character’s behavior and on a scale of −3 (strong disagreement) to 3 (strong agreement) expresses how much he/she agrees or disagrees with the attitude of the main characters. For the application of the questionnaire in Portugal, authorization was granted by Professor Patrícia Bataglia, responsible for the validation of the questionnaire for the Portuguese language in Brazil, and the necessary adjustments were made in agreement with the author.
Data Analysis
Opinion scores were described using the mean and standard deviation, and the comparison of these scores at both times was performed using t-tests for paired samples. The variable of score differences between the first and second application follows a normal distribution. Changes in student opinion (disagree, neutral, and agree) between the first and second applications of the questionnaire were described as the frequencies and percentages of students who changed their opinion from the first to the second application and their 95% confidence intervals. A significance level of 5% was used.
Ethical Aspects
The authorization to apply the questionnaire was granted by the Ethics Committee of the School. The researcher informed the students about the objectives of the study and remained in the room to clarify possible doubts. Students participated in the study in a free and voluntary manner, expressing their consent to participate by completing an informed consent model. Each student placed a code of their choice on the questionnaire, to match the questionnaire at the second application, without the researcher having access to their identification. The informed consent form was held by the lecturer of the Bioethics and Medical Deontology course so that the researcher could not gain access to this data.
Results
A total of 125 students were enrolled in the Bioethics and Medical Deontology course. From these, 72 questionnaires were completed during both applications of the questionnaire. Of the questionnaires answered, two were rejected because they were not properly completed. The total sample, therefore, comprised of 70 (56%) medical students.
Regarding the characteristics of the sample, 63% of the students were female. The average age of students was 21 years, ranging from 20 to 39 years old.
Table 1 presents the opinions of medical students regarding the behavior of the characters in the three dilemmas.
Mean and Standard Deviation (SD) of Opinion Scores of the Medical Students.

The students mostly disagreed with the performance of the characters in the worker’s dilemma at both times and agreed with the behavior of the doctor and the judge in both applications of the questionnaire (Table 1). There are no significant differences in the opinions of students when comparing the two applications of the questionnaire, although there was a tendency toward a greater agreement in the second application.
Table 2 presents the number and percentage of students who maintained their opinion (had the same opinion in the first and in the second application) and the number and the percentage of students who changed their opinion from the first to the second application.
Number and Percentage of Students Who Maintained (Bold) or Changed Their Opinions From the First to the Second Application.
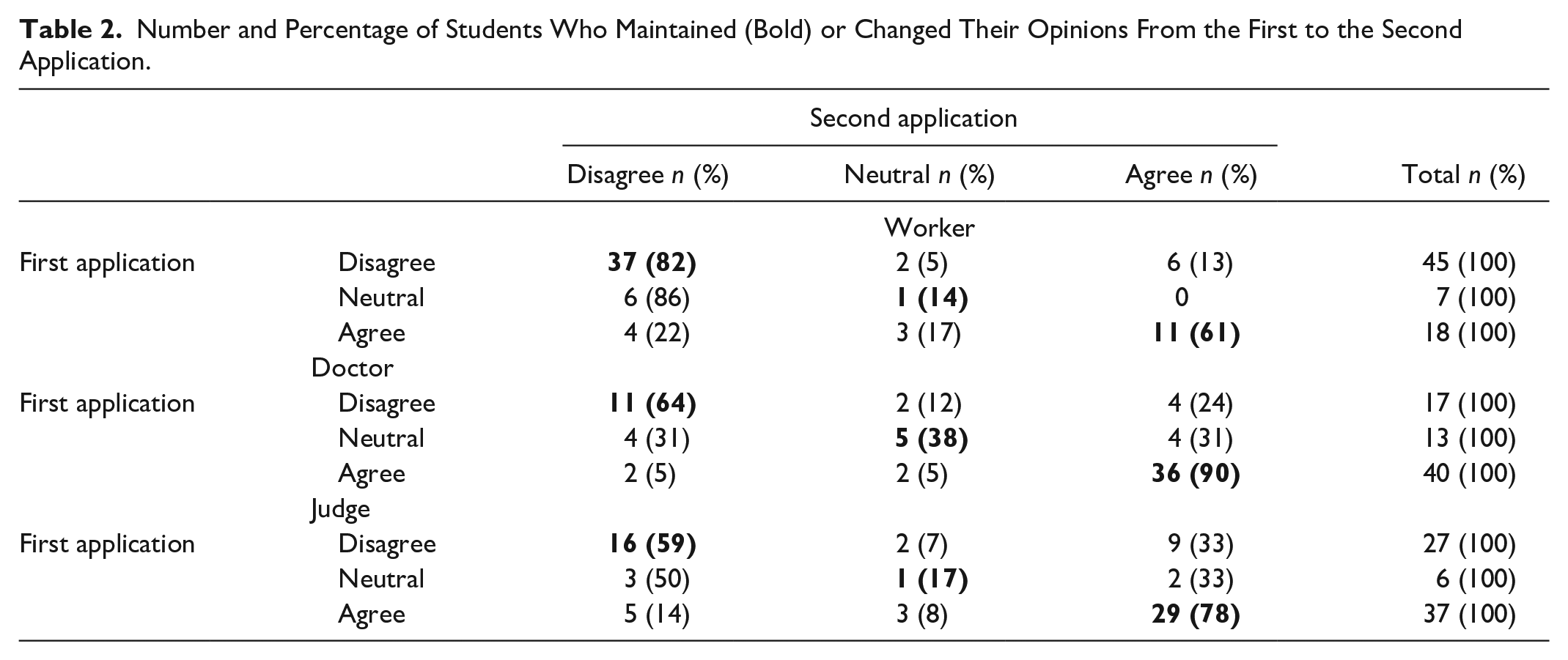
According to Table 2, whilst most students maintain their opinion in all dilemmas, some students even switched from disagreeing in the first application to agreeing in the second application (13%, 24%, and 33% in the worker, doctor, and judge dilemmas, respectively). Also, some students switch from agreeing in the first application to disagreeing in the second application (22%, 5%, and 14% in the worker, doctor, and judge dilemmas, respectively).
In the workers’ dilemma, of those who were neutral at first application, the majority changed their opinion in the second application (86% changed to “disagree”), with only 14% remaining neutral. Regarding the doctor’s dilemma, among those who were neutral at the first application, only 38% remained neutral at the second application, 31% changed their opinion to “disagree” and 31% changed their opinion to “agree.” In the judge’s dilemma, of those who were neutral at the first application, the majority changed their opinion (50% changed their opinion to “disagree” and 33% changed to “agree”), only 17% remained neutral.
Table 3 shows the number and proportion of students who maintain their opinion at the second application of the questionnaire.
Number and Proportion of Students Who Maintain Their Opinion at the Second Application of the Questionnaire in Each Dilemma (Bold) and by the Opinion in the First Application With Respective 95% Confidence Intervals.

Table 3 shows that students who at first have a neutral opinion keep that opinion at a low percentage (only 14%, 38%, and 17% of students in the worker, doctor, and judge dilemma, respectively). When students already have a definite opinion (agree or disagree) in the first application, the percentage of those who maintain their opinion in the second application is higher in all dilemmas.
Discussion
Medical students gave their opinion on three ethical dilemmas. Of the three dilemmas, only one, the doctor’s dilemma, was related to the doctor’s practice and a situation that medical students might face in the future: the patient’s uncontrollable suffering and patient’s request to anticipate the end of their life. Similarly, relating to the remaining dilemmas, although not directly related to the physician’s professional practice, it is clear that students present less indecision when faced with the dilemma in the second application of the questionnaire.
Bioethics education, as a discipline that aims to promote reflection and discussion within the most diverse areas, is expected to have an influence on the decision-making (Liu et al., 2018; Zoboli, 2013) and the moral competence of medical students (Serodio et al., 2016).
The bioethics course at the school where our study was developed, is taught over 30 hours. Teachers use seminar-based teaching methods to discuss specific current issues, group work on problem-solving and analysis, and the presentation and discussion of practical cases by students (FMUP, 2021). It appears, therefore, that emphasis is given to the discussion and analysis of practical cases with ethical dilemmas, as suggested by some authors (Abma et al., 2009; Asghari et al., 2009; Heidari & Ebrahimi, 2016; Roberts et al., 2007; Serodio et al., 2016; Zoboli, 2013). The medical students (future doctors) to whom relationships with others are constant, whether with colleagues, patients, relatives or other professionals, should develop good relationship skills, partly promoted through group work.
In the studied sample, we consider that bioethics education, by promoting reflection and critical judgment through the discussion of clinical cases and group work, could have some impact on the opinion of students who were neutral at first and start to have an agreement or disagreement at the end of bioethics course. These results are in line with the results obtained in previous studies related to bioethics education and moral competence in which, in the same way, there are tenuous differences between the two applications of the questionnaire (Martins et al., 2021; Serodio et al., 2016).
The bioethics course is taught in the year students begin their clinical teaching experience, so the practical cases discussed and analyzed in class, in many situations, have not yet been experienced in clinical practice. Several authors have proposed that bioethics education should occur not only before clinical practice but should be integrated to the whole duration of medical education (Asghari et al., 2009), highlighting the importance of positive role models in clinical practice (AlMahmoud et al., 2017; Savitha et al., 2018), and the positive influence that new educational approaches, such as the participant oriented intervention (Roberts et al., 2007), and decision-making training (Ricou & Marina, 2020) might have in the context of clinical ethics education. Throughout the medical students training, it is important that they develop several technical and cognitive skills necessary for decision-making, that are achieved not only through a theoretical recitation of ethical principles, guidelines, and regulation, but also in emotional and experiential education (Abma et al., 2009; Ricou & Marina, 2020; Roberts et al., 2007), highlighting the role that affective aspects of behavior, that result from situations experienced throughout life and in clinical experience, have on the students’ moral development (Lind, 2016).
The early promotion of reflection and critical judgment in adolescents through bioethics education will enable the formation of citizens with critical adaptability, able to respond to the constant challenges they will face within their professions (Nunes et al., 2015). Building on this knowledge and skills that are developed throughout secondary and higher education, medical students will be able to demonstrate more confidence in making decisions related to their professional practice.
Through our results bioethics education seems to promote students’ confidence in decision-making. In this sense, and considering that bioethics education is increasingly important, with greater individual diversity and technological complexity of medicine, it would be important to understand, in future studies, whether more hours dedicated to bioethics education and during clinical practice would allow a greater capacity for critical thinking by medical students. For this propose, further studies related to moral development in medical students would be of great importance, namely studies comparing the opinions and the moral competence among students before and after clinical education, and between medical students from different schools, one’s with bioethics education throughout the whole duration of medical education and others with bioethics education in a singular curricular year.
Above all, we believe that the debate about bioethics education can benefit the development of medical education and promote medical students moral competence and decision-making, being the art of making thoughtful decisions a moral virtue par excellence (UNESCO, 2015).
Limitations
Our study has some limitations. Firstly, the sample is small, so we cannot generalize the results obtained. Also, although bioethics course is a compulsory subject, the second application of the questionnaire coincided with moments of evaluation in several subjects, so the students could be more tired and less available to answer the questionnaire.
The same ethical dilemmas were presented at two different times, so the students might have remembered the answer presented in the first application and tended to repeat the answer in the second application. Regarding opinion, there is no right or wrong answer, so we consider it relevant that neutral students came to agree or disagree in the second application of the questionnaire. This study was part of a research study that aims to assess moral competence in medical students and although the questionnaire allows the measure of opinions and changes in opinion scores, we suggest that other studies should be developed in this area, with data collection instruments more focused on the evaluation of the opinion change. Also, it was not possible to have a control class without bioethics education, which would allow us to evaluate whether the results are associated with the course or might result from other factors.
Conclusions
The results suggest that, after the bioethics course, students have lower indecision, however the changes were very tenuous. We believe that bioethics education at this time might develop the student’s confidence in making a decision, but it will not have the expected impact on the decisions themselves, as many dilemmas arise, with clinical practice.
We propose as points of change: a greater number of hours available for the bioethics course, the integration of bioethics education throughout the whole duration of medical education, and the education of the students in clinical practice, by positive role models representing examples of good practice. It would be of great relevance to promote more opportunities for reflection and discussion during practical cases, stimulating critical judgment and the ability to make decisions. Similarly, students should be encouraged to develop ethical thinking and training in areas where they do not feel so confident throughout their academic and professional lives.
Footnotes
Acknowledgements
The authors are greateful to the students and teachers who collaborated in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by National Funds through FCT—Fundação para a Ciência e a Tecnologia, I.P., within CINTESIS, R&D Unit (reference UIDB/4255/2020).
Ethics Approval and Consent to Participate
This study was carried out in accordance with the Declaration of Helsinki, the anonymity of participants was guaranteed, and their informed consent was obtained in written form. The study project was submitted to the Faculty Ethics Committee of Faculty of Medicine of University of Porto for approval, and all the required authorizations were obtained. The approval number was 299/2017.