
Abstract
This study developed and empirically tested a model to predict the factors affecting patients’ behavioral intentions to use a mobile health education website. It explored the behavioral intention to use a mobile health education website from the perspective of consumers by extending the Unified Theory of Acceptance and Use of Technology 2 model with the addition of mobile self-efficacy (M-SE), use motivation, and mobile literacy as moderators. For this purpose, variance-based structural equation modeling was used to analyze data collected from a sample of 1,649 patients at a hospital in Taoyuan, Taiwan. Partial least squares regression was used for model and hypothesis testing. The results revealed that (1) performance expectancy, effort expectancy, social influence, facilitating conditions, and habit were key predictors of the behavioral intentions of patients to use a mobile health education website; (2) M-SE had positive associations with effort expectancy; (3) use motivation was a significant determinant of both performance expectancy and effort expectancy; and (4) mobile literacy had a significantly negative moderating effect on the relationship between performance expectancy and behavioral intention. Our findings serve as a reference for the promotion of mobile health education in hospitals.
Introduction
Patient health education (HE) is a “purposeful,” systematic activity in which patients can acquire health care-related skills and knowledge. The aim of such HE is to improve the health care behavior of patients (Van Hoozer, 1987). Well-structured HE enhances a patient’s health care ability and self-efficacy (Loveman et al., 2003). The concept of HE comprises patients being involved in self-care and their care plans through participatory education and consequently achieving patient-centered improvement (Basak Cinar & Schou, 2014; Chakraborty et al., 2014). Many educators and clinicians are currently using electronic communication devices as a supplement to HE to convey health messages (Saffari et al., 2014). Such use of electronic communication provides a context that enables education to be provided anywhere, anytime, and on any topic. The focus of such HE is the development of skills rather than the mere acquisition of knowledge (Chakraborty et al., 2014; Saffari et al., 2014; Toyama et al., 2013).
Mobile devices have greatly improved our lives. More importantly, they have improved health care services (Balapour et al., 2019; Chakraborty et al., 2014, 2015). These improvements are underpinned by two developments. First, smartphones have become affordable, resulting in their widespread use. Second, smartphone performance has increased exponentially, allowing for the development of various health care applications (Balapour et al., 2019; Chakraborty et al., 2014, 2015; Petrovčič et al., 2018). As society becomes increasingly digitized and networked, health information and public HE are becoming widely available and accessible through the Internet and other media. Thus, digital medical care and mobile health (also known as “mHealth”) are rapidly growing fields that have attracted considerable attention from patients, clinicians, and researchers. Digital medical care and mobile health eliminate time and geographic constraints concerning access to health care services, thereby increasing the coverage and quality of medical services (Meng et al., 2019). Because most health care providers do not have sufficient time to provide patients with the continuing care required to control chronic conditions, a mobile health website can potentially compensate for this problem.
UTAUT 2
In recent decades, several theories have been proposed to explain and predict the acceptance and use of technology, the most prominent of which being the Technology Acceptance Model (TAM) (Davis, 1989) and the Unified Theory of Acceptance and Use of Technology (UTAUT) (Chao, 2019; Tan, 2013a, 2013b, 2019; Venkatesh et al., 2003). However, few studies have used these theories to investigate the general public’s use of HE websites. The UTAUT synthesizes the concepts and user experiences that provide the foundation for theories on the user acceptance process of an information system (Chao, 2019; Tan, 2013a, 2013b, 2019; Venkatesh et al., 2003). The following theories are derived from the UTAUT: the TAM (Davis, 1989), the Theory of Reasoned Action (TRA) (Fishbein & Ajzen, 1975), the Motivational Model (MM) (Davis et al., 1989), the Theory of Planned Behavior (TPB) (Ajzen, 1991), a Model Combining the TAM and the TPB, the Model of PC Utilization (MPCU) (Thompson et al., 1991), the Innovation Diffusion Theory (IDT) (Moore & Benbasat, 1991; Rogers, 2003), and the Social Cognitive Theory (SCT) (Bandura, 1986). In empirical tests, the UTAUT model could explain approximately 70% of the variance in a user’s behavioral intention of using a new system. By contrast, competing models only explained between 17% and 53% of variance. By integrating each model’s key moderating effects and capabilities for in-depth investigation, the structure of the UTAUT remains simple in spite of theoretical developments (Rondan-Cataluña et al., 2015).
To adapt the UTAUT to a consumer rather than a professional context, Venkatesh et al. (2012) proposed UTAUT 2. UTAUT 2 explains why individuals use the information technology they adopt. The original UTAUT model proposed by Venkatesh et al. (2003) includes three variables (performance expectancy, effort expectancy, and social influence), one variable (facilitating conditions), and four moderators (age, gender, experience, and voluntariness) that explain a person’s behavioral intention to use a particular technology. Venkatesh et al. (2012) expanded the original UTAUT model, naming it the “UTAUT 2,” and introduced three new constructs of hedonic motivation, price value, and habit. The UTAUT 2 model explains 74% of the variance in a consumer’s behavioral intention to use a technology and 52% of the variance in a consumer’s use of a technology (Venkatesh et al., 2016). The UTAUT 2 has been widely used to assess technological adoption in fields such as mobile health (Duarte & Pinho, 2019), mobile banking (Baabdullah et al., 2019; Merhi et al., 2019), information and communication technology (Macedo, 2017), and electronic health records (Badran, 2019), demonstrating excellent predictive ability. In addition, performance expectancy, effort expectancy, social influence, facilitating conditions, and habits are critical factors that influence behavioral intention (Baabdullah et al., 2019; Badran, 2019; Duarte & Pinho, 2019; Macedo, 2017; Merhi et al., 2019). Based on the above discussion, this study argues that performance expectancy, effort expectancy, social influence, facilitating conditions, and habit can significantly influence patients’ behavioral intentions to use a mobile health education website.
Mobile Self-efficacy (M-SE) and Mobile Literacy
According to SCT (Bandura, 1986), self-efficacy is an individual’s judgment of general behavioral competence (Agarwal & Karahanna, 2000) and personal belief that adequate skills are required for success in mobile technology-related tasks (Ozturk et al., 2016). Hsieh et al. (2016) suggested a proactive influence of self-efficacy on performance expectancy and effort expectancy. With the increasing prevalence of mobile devices, researchers have begun to discuss the effects of mobile self-efficacy (M-SE) (Chao, 2019). Nikou and Economides (2017) defined M-SE as an individual’s perception of his or her ability to complete specific tasks (e.g., browsing the Internet) by using a mobile device. Mobile learning research has suggested that information and communication technology literacy and skills can affect a student’s intention to use such technology (Nikou & Economides, 2017). Generally, the rapid development of mobile devices places increasing demand on user capabilities in the operation of mobile devices. Such capabilities are required to comprehend relevant health messages. To the best of our knowledge, most previous studies combined UTAUT 2 with self-efficacy. Few studies have explored the impact of M-SE on performance expectancy and effort expectancy in the UTAUT 2 model. Therefore, this study argues that patients’ M-SE will affect performance expectancy and effort expectancy in the UTAUT 2 model.
Goldman et al. (2010) argued that digital literacy encompasses not only device use but also the cognitive process; various cognitive and emotional skills are involved in the use of mobile technologies in the context of a digital environment (Martin & Madigan, 2006). Moreover, users who lack mobile literacy are often lost, misled, and confused when interacting with mobile interfaces (Greene et al., 2014). Most studies have incorporated digital and mobile literacy into their research models to investigate the use and acceptance of a technology (Mac Callum & Jeffrey, 2014; Mohammadyari & Singh, 2015). However, few studies have investigated whether mobile literacy can be a moderating factor in the UTAUT 2 model. Therefore, this study uses mobile literacy as moderators, and examine whether performance expectancy, effort expectancy, and mobile literacy moderate and predict behavioral intention to use a mobile HE website.
Motivation
According to cognitive valuation theory, motivation affects an individual’s behavior and behavioral intentions (Deci & Ryan, 1985; Deci et al., 2001). Scholars have distinguished motivation (Deci & Ryan, 1985; Senécal et al., 2001) by its intrinsic and extrinsic variants. Deci et al. (2001) and Deci and Ryan (1985) have argued that motivation is a key determinant of whether an individual will engage and continue to engage in a given behavior. Intrinsic motivation is derived from (internal) emotional factors such as interest, satisfaction, and perceptions of utility, whereas extrinsic motivation is derived from (external and often tangible) incentives and disincentives in the environment (Deci & Ryan, 1985; Deci et al., 1991; Pierce et al., 2003). Both motivation types spur individuals to improve their abilities (Pintrich & DeGroot, 1990; Wigfield, 1994). Motivation variables comprise and are linearly related to intrinsic and extrinsic motivation; the motivation viewpoint is a latent variable with multiple dimensions. Intrinsic and extrinsic motivations can be measured using assessment questions. In this study, motivation is set as a formative indicator rather than a reflective indicator, whereas intrinsic and extrinsic motivation are reflective indicators. Therefore, in this study, use motivation is regarded as an external variable in the UTAUT 2 model, and it is argued that use motivation will also affect performance expectancy and effort expectancy in the UTAUT 2 model.
This study investigated the use of HE websites by the general public as it relates to the suitability of these websites and the behavioral intention to use them, thus addressing a gap in the literature. The UTAUT was tested and modified (Venkatesh et al., 2012). The UTAUT 2 was selected because of its comprehensiveness, explanatory power, and applicability to a consumer context relative to other technology acceptance models (Pan & Jordan-Marsh, 2010; Verdegem & De Marez, 2011). Specifically, we used the UTAUT 2 to predict an individual’s use of HE websites and theoretically integrate behavioral self-efficacy, use motivation, and behavioral literacy. Our study also improved on the UTAUT 2 with respect to its predictive ability. This study further evaluated the correlation between the UTAUT 2 frameworks and their relationship with other variables. Our study provides a more comprehensive understanding of the use of mobile HE websites. Therefore, the four primary objectives of this study were as follows: (1) to investigate the factors influencing behavioral intention to use a mobile HE website; (2) develop an extended UTAUT 2 model incorporating use motivation, M-SE, and mobile literacy for a mobile HE website; (3) examine whether performance expectancy, effort expectancy, and mobile literacy moderate and predict behavioral intention to use a mobile HE website; and (4) assess the resultant model empirically. The following research questions were formulated to achieve the following objectives: (1) What factors determine patients’ behavioral intentions to use a mobile HE website for HE purposes? (2) Do use motivation and M-SE affect the UTAUT 2 model in relation to a mobile HE website?, and (3) How does mobile literacy moderate the effects of performance expectancy and effort expectancy on behavioral intention to use a mobile HE website? The major contributions of this study include extending the external variables (M-SE, use motivation, and mobile literacy) of the UTAUT2 model to assess the determinants of patients’ behavioral intentions using mobile HE websites. In addition, this study also uses mobile literacy as a moderator and uses motivation as the formation indicator. Moreover, because our study was conducted in Taiwan, it expands the limited geographical scope of the literature on this topic.
Methodology
Research Model
In this study, the UTAUT 2 model was selected as the basis for investigating patients’ perceptions of a mobile HE website. Figure 1 depicts the research model, which is constructed with the exogenous variables of M-SE, use motivation, social influence, facilitating conditions, and habit; the endogenous variables of performance expectancy, effort expectancy, and behavioral intention; and the moderating variable of mobile literacy. The hypotheses, discussed in subsequent sections, are numbered and illustrated in the proposed path model. Figure 1 presents the conceptual model.

Research model and hypotheses.
Research Hypotheses
The following hypotheses were proposed:
Hypothesis 1: Performance expectancy has a significant influence on the behavioral intention to use a mobile HE website.
Hypothesis 2: Effort expectancy has a significant influence on the behavioral intention to use a mobile HE website.
Hypothesis 3: Social influence has a significant influence on the behavioral intention to use a mobile HE website.
Hypothesis 4: Facilitating conditions have a significant influence on the behavioral intention to use a mobile HE website.
Hypothesis 5: Habit has a significant influence on the behavioral intention to use a mobile HE website.
Hypothesis 6: Performance expectancy has a significant influence on the effort expectancy of a mobile HE website.
Hypothesis 7: M-SE has a significant influence on performance expectancy.
Hypothesis 8: M-SE has a significant influence on effort expectancy.
Hypothesis 9: Use motivation has a significant influence on performance expectancy.
Hypothesis 10: Use motivation has a significant influence on effort expectancy.
Hypothesis 11: Intrinsic motivation has a significant influence on use motivation.
Hypothesis 12: Extrinsic motivation has a significant influence on use motivation.
M1: The relationship between performance expectancy and behavioral intention is moderated by mobile literacy.
M2: The relationship between effort expectancy and behavioral intention is moderated by mobile literacy.
Survey Questionnaire
We used a questionnaire to collect data. The research procedure was reviewed and approved by the institutional review boards of the Tri-Service General Hospital (2-108-05-032). The questionnaire design was based on a mental scale developed according to the procedures of DeVellis (2003) and MacKenzie et al. (2011). After we designed the questionnaire, five experts in the fields of hospital management, medical information management, HE, and questionnaire design were consulted to improve on the semantics of our questionnaire, thereby improving the questionnaire’s content validity. Following expert modification, we conducted a pretest and formal test of our questionnaire. All measurement items (mobile literacy, M-SE, and use motivation of the UTAUT 2) were close-ended and structured questions. Participants completed the questionnaire items in relation to subjective feelings and cognition. The items are rated on a 5-point Likert scale with anchors ranging from 5 (“strongly agree”) to 1 (“strongly disagree”).
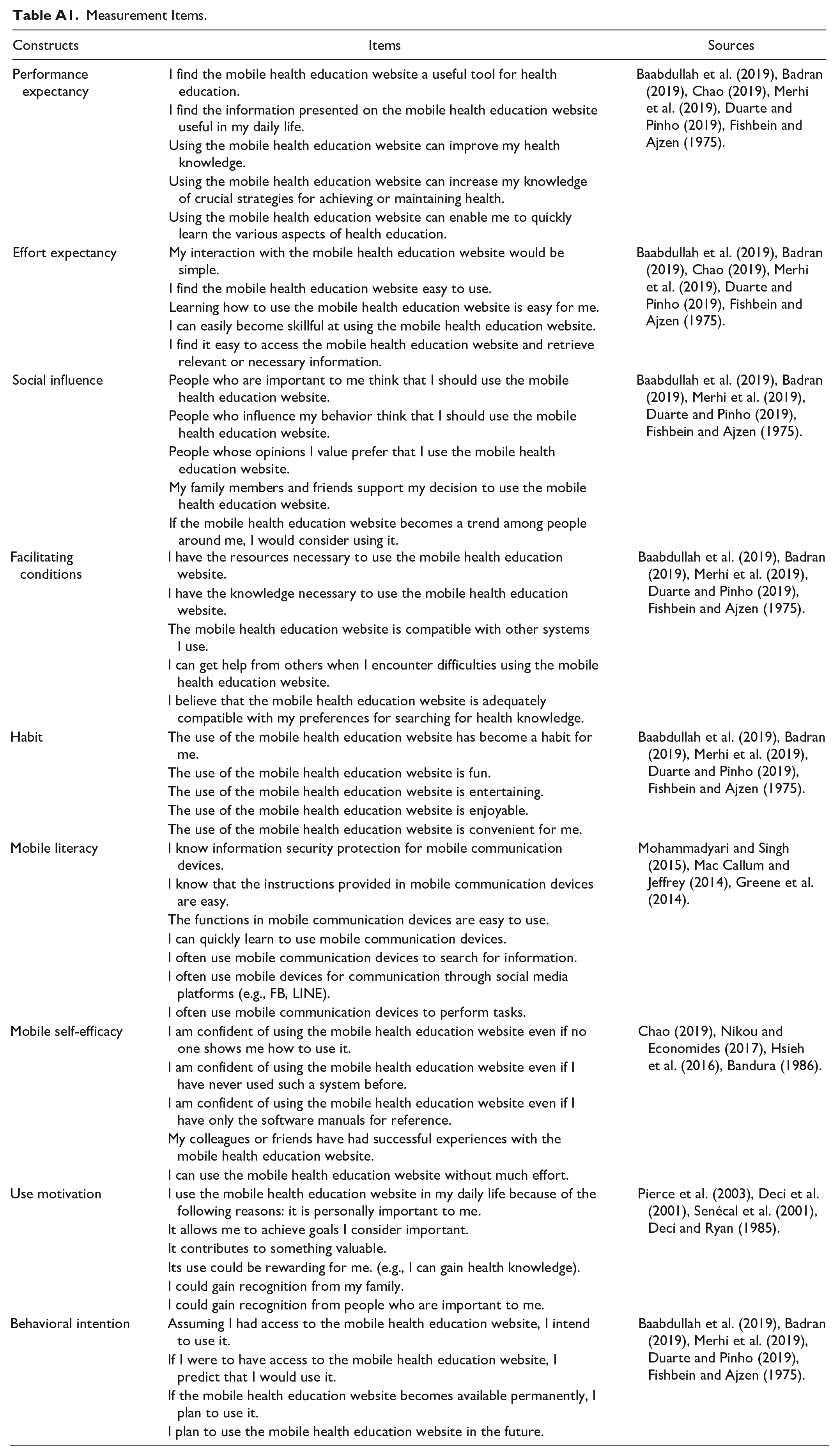
The main constructs of the UTAUT 2 model (i.e., performance expectancy, effort expectancy, social influence, facilitating conditions, habit, and behavioral intention) were adopted from measurement constructs developed in related studies (Baabdullah et al., 2019; Badran, 2019; Chao, 2019; Duarte & Pinho, 2019; Merhi et al., 2019; Venkatesh et al., 2012). The performance expectancy, effort expectancy, social influence, facilitating conditions, and habit measures had five items each, and the behavioral intention measure had four items. Patients’ M-SE in a mobile HE website was measured on the basis of five items from related studies (Bandura, 1986; Hsieh et al., 2016; Nikou & Economides, 2017); mobile literacy contained seven items (Chao, 2019; Greene et al., 2014; Mac Callum & Jeffrey, 2014; Mohammadyari & Singh, 2015). Items for the use motivation constructs were adapted from several related studies (Deci & Ryan, 1985; Deci et al., 2001; Pierce et al., 2003; Senécal et al., 2001) and included intrinsic motivation (three items) and extrinsic motivation (three items). In summary, the measurement instrument used in this study consisted of 47 items, and our research model consisted of nine constructs. In addition, basic information concerning respondent characteristics was included, such as age, gender, monthly income, formal education level, and health conditions. Details on the questionnaire are shown in Table A1 (Appendix).
In the pilot test, the study collected data from 121 questionnaires sent to mobile HE website users in Taoyuan, Taiwan. The focus of the pilot study was to examine the reliability and validity of the scales in the context of the UTAUT 2, mobile literacy, M-SE, and use motivation. The reliability scores, obtained using Cronbach’s α, ranged from .885 for social influence to .930 for performance expectancy. The results indicated that the α coefficients for all of the 47 items measured were higher than the minimum required value of .7 (Hair et al., 2010). This is considered an acceptable indication of reliability (Hair et al., 2010). These results imply that the scales used in this research could satisfactorily measure the constructs of interest.
Data Analysis
Participants
Most research participants of this study were patients in a hospital in Taoyuan, Taiwan who were recruited through convenience sampling. We conducted face-to-face interviews with them to collect data. Prior to data collection, we obtained informed consent from all participants and assured them that their responses would remain confidential and only be used for research purposes. The participants took 15 to 20 minutes to complete the questionnaire. In total, 1,770 questionnaires were distributed, and 1,720 questionnaires were returned to us. The investigation process excluded participants who (1) were younger than 30 years of age, (2) did not know of the mobile HE website, and (3) had not used the mobile HE website in the past. In addition, responses in which one-third or more of the items were unanswered or incompletely answered were discarded. The remaining 1,649 valid responses were statistically analyzed. The general characteristics of the participants are listed in Table 1. The proportions of female and male subjects were 65.3% and 34.7%, respectively, and most of the research participants were aged 39 years or younger (39.1%). In our sample, 51.2% of participants had attended college and university, and the monthly income of the majority (52.3%) was in the range of NT$20,001 to NT$40,000, with approximately half of the participants reporting that their health condition was ordinary (45.9%).
Profiles of Respondents (N = 1,649).

Measurement Model Analysis
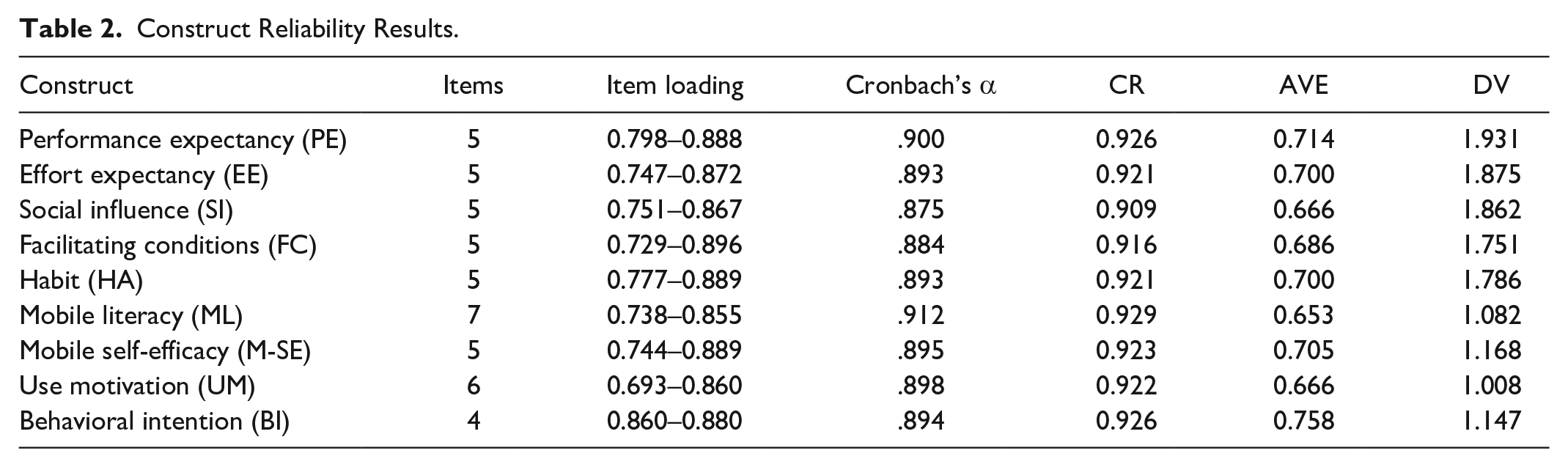
A measurement model assesses the internal reliability, convergent validity, discriminant validity (DV), Cronbach’s α, and composite reliability (CR) of a model’s structure, particularly its internal reliability. The average variance extracted (AVE) can be used to assess convergent validity. On the basis of the recommendation of Bagozzi and Yi (2012), we adopted the three most common model assessment indicators to assess our model: (1) item loading (λ) and reliability coefficient (i.e., Cronbach’s α), (2) CR value, and (3) AVE (Bagozzi & Yi, 2012; Chin, 1998; Fornell & Larcker, 1981; Hair et al., 2010; Jöreskog & Sörbom, 2005).
As shown in Table 2, Cronbach’s α coefficients ranged from .875 for social influence to .912 for mobile literacy. The CR coefficients for all constructs ranged from .909 for social influence to .929 for mobile literacy. Both of the Cronbach’s α and CR coefficients had values greater than .7 for all constructs, which suggests internal consistency (Hair et al., 2010). All constructs had AVE values between 0.653 for mobile literacy and 0.758 for behavioral intention. The AVE values for all constructs were found to be greater than 0.5, indicating strong convergent validity for the questionnaire (Fornell & Larcker, 1981). Table 2 also presents the DV. The DV values of all constructs were greater than 1.0, indicating an appropriate level (Fornell & Larcker, 1981; Hair et al., 2010, 2016). Overall, examination of the psychometric properties of the scale revealed unidimensionality and conceptual consistency.
Construct Reliability Results.
Hypothesis Testing
Structural model analysis verifies a study’s proposed research framework and explains a model’s overall explanatory power. To estimate the path of each variable, in this study, we conducted empirical analysis using SmartPLS 3.0 software (SmartPLS GmbH, Bönningstedt, Germany). The path coefficient values were normalized, and all research hypotheses in our research model were tested. To assess the goodness of fit (GoF) of our proposed research model, the GoF, standardized root mean square residual (SRMR), and explained variance (R2) were used as indicators (Alolah et al., 2014; Hair et al., 2010; Tenenhaus et al., 2005; Ziggers & Henseler, 2016).
First, the GoF indicator was calculated according to the formula proposed by Alolah et al. (2014):
To verify our research hypotheses and proposed moderating effects, we conducted the moderating analysis formulated by Baron and Kenny (1986). The empirical analysis was based mainly on the importance of interactions in model 3, thus testing for the moderating effects of ML. PLS regression was used to test the main effects of PE and EE and the moderating effects of ML on BI to use a mobile HE website. For example, to test the moderating effect, the PE (predictor) was multiplied by the ML (moderator) to create an interaction construct (PE × ML) for predicting BI to use a mobile HE website. The results show in Table 3.
Estimation Results.

p < .05.
Among the two hypothesized moderating effects, ML negatively moderated the relationship between PE and BI in relation to use of a mobile HE website (M1: β = −0.101; p < .05), indicating that M1 was significant. However, M2 was nonsignificant; that is, ML did not have a moderating effect on the relationship between EE and BI. These additional analyses provided support for the moderation pattern presented in our model. Figure 2 provides all results of the moderation analysis, including the structural path estimates and explained variances. Consistent with M1, PE, and ML had a negative effect on BI to use a mobile HE website. Specifically, we revealed that PE and BI related to use a mobile HE website increased with decrease in ML.

Path coefficients for the research model (including interaction effect).
As show in Table 3, the components of the UTAUT 2 model include five constructs (PE, EE, SI, FC, and HA). The PE, SI, FC, and HA constructs had significant positive effects on BI to use a mobile HE website (β = 0.193, 0.203, 0.190, and 0.165, respectively; p < .05). However, EE had significant negative effects on BI (β = −0.054; p < .05). Therefore, Hypotheses 1, 2, 3, 4, and 5 were supported. In addition, EE had significant positive effects on PE (β = 0.477; p < .05), thereby supporting Hypothesis 6. The construct of M-SE had a significant positive effect on EE (β = 0.307; p < .05) but a nonsignificant effect on PE, thereby supporting Hypothesis 8 and not supporting Hypothesis 7. The construct of UM was a significant determinant of both PE and EE (β = 0.279 and 0.343, respectively), thereby supporting Hypotheses 9 and 10. Finally, intrinsic motivation and extrinsic motivation were reported to be important antecedents of UM (standardized β coefficients = 0.347, 0.353, 0.318, and 0.343, respectively; p < .05). Therefore, Hypotheses 11 and 12 were supported.
Figure 2 presents the explanatory power. The model explained a substantial portion of the variance in all endogenous variables: PE (44.9%), EE (31.2%), and BI (44.4%). In summary, the model employed in this study explained a considerable number of variations in the endogenous variables. The endogenous variables exhibited strong explanatory power for these variations, thereby indicating the stability and robustness of the model. All estimated and standardized path coefficients (significant paths are indicated with asterisks) are illustrated in Figure 2.
Discussion
The purpose of this study was to develop and empirically test a model to predict the factors affecting patients’ behavioral intentions to use a mobile health education website. The major contributions of this study were to integrate M-SE, use motivation, and mobile literacy into the UTAUT 2 model to evaluate the determinants of patients’ behavioral intentions to use a mobile HE website. In addition, this study also uses mobile literacy as a moderator and uses motivation as the formation indicator. A cross-sectional online survey of 1,562 participants was conducted. This study expanded on and assessed UTAUT 2 in relation to the behavioral intentions of patients using mobile HE websites. An interpretation of the results based on the empirical findings is as follows:
In our empirical tests, 12 of 14 hypotheses were supported. Specifically, performance expectancy, effort expectancy, social influence, facilitating conditions, and habit were determined to be crucial predictors of a patient’s behavioral intention to use mobile HE websites. All variables except for effort expectancy had a positive effect on behavioral intention. When predicting behavioral intentions, the path coefficients of all variables differed in their weights. Social influence had the largest effect on behavioral intention, meaning that patients were most concerned with the opinions of others in their use of mobile HE websites. Thus, when promoting methods of using mobile HE websites among patients, the demographic background of many participants who exert substantial influence over others should be considered. Therefore, word of mouth is an effective tool for promoting mobile HE websites, and marketing strategies should assign greater weight to an individual’s opinion (Oh & Yoon, 2014).
The second largest factor affecting behavioral intention was performance expectancy, meaning that the cognitive advantage of mobile HE websites was influential in a patient’s decision to use these websites. This finding, in addition to findings of related studies, suggests that in the main structure of the UTAUT 2, performance expectancy is a variable with a relatively high coefficient path weight (Baabdullah et al., 2019; Badran, 2019; Macedo, 2017; Merhi et al., 2019; Venkatesh et al., 2012). Previous research on hospital patients corroborates our finding that performance expectancy predicts and is correlated with the behavioral intention of patients. The third largest factor affecting behavioral intention was facilitating conditions, meaning that familiarity with a website and its facility of use were influential in a patient’s behavioral intention to use the website. In contrast to these factors and inconsistent with previous findings, effort expectancy was observed to be negatively correlated with behavioral intention (Duarte & Pinho, 2019; Macedo, 2017; Venkatesh et al., 2012). HE is crucial for the general public, and mobile HE websites enable individuals to learn wherever they are. However, immediate feedback is not available when individuals have questions that require professional medical expertise. Moreover, the interactivity of mobile health can be inconvenient for the general public. This, in turn, dampens a person’s behavioral intention to use mobile HE websites.
With respect to the external variables added to the UTAUT 2, the hypothesized path coefficients testing the influence of M-SE and use motivation on performance expectancy and effort expectancy to use mobile HE websites also demonstrated significance. The first result revealed that when using mobile HE websites, the M-SE of patients (with respect to their use of mobile technology) had no effect on performance expectancy but a considerable effect on effort expectancy. In other words, patients considered mobile HE websites to be useful in addition to being an integrated part of their lives. Therefore, M-SE had no effect on performance expectancy.
Furthermore, consistent with Deci and Ryan (1985) and Deci et al. (2001), our findings suggest that intrinsic and extrinsic motivations are crucial factors from the perspective of motivation and motivation. Health consciousness has been increasing among the general public in recent years, and interest in the use of mobile HE websites has increased. Mobile HE websites aid learning better if they facilitate convenient knowledge transmission through media and technology, have an intuitive interface, and appeal to the user’s intrinsic motivation. When patients are motivated to use a mobile HE website and anticipate not having to spend considerable time familiarizing themselves with their operations, HE activities are completed more quickly. Consequently, use motivation has a negative effect on performance expectancy and effort expectancy.
Finally, this research model demonstrated the moderating relationships among performance expectancy, effort expectancy, and the behavioral intention to use a mobile HE website. Therefore, our research contributes to the understanding of how the use of mobile HE websites can be promoted among the general public. However, mobile literacy will have moderating effects on the relationship between performance expectancy and the behavioral intention to use a mobile HE website because there are nonsignificant moderating effects in effort expectancy and behavioral intentions. The moderator of mobile literacy can affect the path relationship of performance expectancy to behavior intention and lead to a significant relationship. Therefore, we conclude that mobile literacy is a crucial factor for enhancing the use of mobile HE websites. In particular, performance expectancy is crucial to enhancing an individual’s behavioral intention to use mobile HE websites.
Limitations and Suggestions for Further Studies
This study had some limitations. First, our data collection process was short, and only cross-sectional (and no longitudinal) data were collected. Therefore, data collected at a different time or for a longer period may produce different results. We recommend that future studies adopt a longitudinal research design and conduct surveys over a longer time period to yield more comprehensive results. Second, this study only targeted patients in a hospital in Taoyuan City, Taiwan. Given these limitations in geographical scope and sample size, our findings are insufficiently generalizable. Future studies should have a larger research scope and sample size, thus increasing the generalizability and comprehensiveness of their findings. Third, only the moderating variable of ML was considered, but other variables (e.g., perceived risk and “technostress”) can also moderate the relationship between BI and another factor. Future studies should include these other moderating variables. Finally, in this study’s questionnaire, a self-reported scale was used for data collection. Thus, respondents may not have expressed their true opinions, limiting the generalizability of our research findings.
Conclusions
This study improved on and assessed the predictive ability of the UTAUT 2 to understand the behavioral intention of patients in their use of mobile HE websites. Therefore, our research aims were to (1) investigate the factors influencing behavioral intention to use a mobile HE website; (2) develop an extended UTAUT 2 model incorporating use motivation, M-SE, and mobile literacy for a mobile HE website; (3) examine whether performance expectancy, effort expectancy, and mobile literacy moderate and predict behavioral intention to use a mobile HE website; and (4) empirically assess the resultant model. For this purpose, variance-based structural equation modeling was used to analyze data collected from a sample of 1,649 patients at a hospital in Taoyuan, Taiwan. The results revealed that social influence is an important factor that significantly influences patients’ behavioral intentions to use a mobile HE website. In addition, performance expectancy, effort expectancy, facilitating conditions, and habits had a significant effect on behavioral intentions. M-SE had a significantly positive effect on effort expectancy, but a non-significant effect on performance expectancy. Patient use motivation was a significant determinant of both performance expectancy and effort expectancy. In addition, motivation is set as a formative indicator, and intrinsic motivation is an important factor affecting motivation. Finally, mobile literacy had a significantly negative moderating effect on the relationship between performance expectancy and behavioral intention. The findings of this study can provide a reference for the promotion of mobile health education in hospitals.
Footnotes
Appendix
Measurement Items.
| Constructs | Items | Sources |
|---|---|---|
| Performance expectancy | I find the mobile health education website a useful tool for health education. | Baabdullah et al. (2019), Badran (2019), Chao (2019), Merhi et al. (2019), Duarte and Pinho (2019), Fishbein and Ajzen (1975). |
| I find the information presented on the mobile health education website useful in my daily life. | ||
| Using the mobile health education website can improve my health knowledge. | ||
| Using the mobile health education website can increase my knowledge of crucial strategies for achieving or maintaining health. | ||
| Using the mobile health education website can enable me to quickly learn the various aspects of health education. | ||
| Effort expectancy | My interaction with the mobile health education website would be simple. | Baabdullah et al. (2019), Badran (2019), Chao (2019), Merhi et al. (2019), Duarte and Pinho (2019), Fishbein and Ajzen (1975). |
| I find the mobile health education website easy to use. | ||
| Learning how to use the mobile health education website is easy for me. | ||
| I can easily become skillful at using the mobile health education website. | ||
| I find it easy to access the mobile health education website and retrieve relevant or necessary information. | ||
| Social influence | People who are important to me think that I should use the mobile health education website. | Baabdullah et al. (2019), Badran (2019), Merhi et al. (2019), Duarte and Pinho (2019), Fishbein and Ajzen (1975). |
| People who influence my behavior think that I should use the mobile health education website. | ||
| People whose opinions I value prefer that I use the mobile health education website. | ||
| My family members and friends support my decision to use the mobile health education website. | ||
| If the mobile health education website becomes a trend among people around me, I would consider using it. | ||
| Facilitating conditions | I have the resources necessary to use the mobile health education website. | Baabdullah et al. (2019), Badran (2019), Merhi et al. (2019), Duarte and Pinho (2019), Fishbein and Ajzen (1975). |
| I have the knowledge necessary to use the mobile health education website. | ||
| The mobile health education website is compatible with other systems I use. | ||
| I can get help from others when I encounter difficulties using the mobile health education website. | ||
| I believe that the mobile health education website is adequately compatible with my preferences for searching for health knowledge. | ||
| Habit | The use of the mobile health education website has become a habit for me. | Baabdullah et al. (2019), Badran (2019), Merhi et al. (2019), Duarte and Pinho (2019), Fishbein and Ajzen (1975). |
| The use of the mobile health education website is fun. | ||
| The use of the mobile health education website is entertaining. | ||
| The use of the mobile health education website is enjoyable. | ||
| The use of the mobile health education website is convenient for me. | ||
| Mobile literacy | I know information security protection for mobile communication devices. | Mohammadyari and Singh (2015), Mac Callum and Jeffrey (2014), Greene et al. (2014). |
| I know that the instructions provided in mobile communication devices are easy. | ||
| The functions in mobile communication devices are easy to use. | ||
| I can quickly learn to use mobile communication devices. | ||
| I often use mobile communication devices to search for information. | ||
| I often use mobile devices for communication through social media platforms (e.g., FB, LINE). | ||
| I often use mobile communication devices to perform tasks. | ||
| Mobile self-efficacy | I am confident of using the mobile health education website even if no one shows me how to use it. | Chao (2019), Nikou and Economides (2017), Hsieh et al. (2016), Bandura (1986). |
| I am confident of using the mobile health education website even if I have never used such a system before. | ||
| I am confident of using the mobile health education website even if I have only the software manuals for reference. | ||
| My colleagues or friends have had successful experiences with the mobile health education website. | ||
| I can use the mobile health education website without much effort. | ||
| Use motivation | I use the mobile health education website in my daily life because of the following reasons: it is personally important to me. | Pierce et al. (2003), Deci et al. (2001), Senécal et al. (2001), Deci and Ryan (1985). |
| It allows me to achieve goals I consider important. | ||
| It contributes to something valuable. | ||
| Its use could be rewarding for me. (e.g., I can gain health knowledge). | ||
| I could gain recognition from my family. | ||
| I could gain recognition from people who are important to me. | ||
| Behavioral intention | Assuming I had access to the mobile health education website, I intend to use it. | Baabdullah et al. (2019), Badran (2019), Merhi et al. (2019), Duarte and Pinho (2019), Fishbein and Ajzen (1975). |
| If I were to have access to the mobile health education website, I predict that I would use it. | ||
| If the mobile health education website becomes available permanently, I plan to use it. | ||
| I plan to use the mobile health education website in the future. |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author thanks the Taoyuan Armed Forces General Hospital of Taiwan for financially supporting this research under contract Taoyuan Armed Forces General Hospital: 10839.