
Abstract
The impact of the Great Recession on health stands out due to its implications for the wellbeing of the population. The available empirical evidence suggests that macrosocial inequalities can be a central element in explaining differences in the impact of the crisis on the health of the population during its early years (2008–2011). Specifically, it is necessary to analyze the role played by the processes constituting a model of inequalities based on social exclusion. This study addresses the topic by using longitudinal data taken from the European Union statistics on income and living conditions (EU-SILC) survey (n = 5.924), with a hierarchical structure of four measurement moments nested in 5,924 individuals nested in 17 regions. Variables from two levels of analysis are considered: individual and ecological (regional) variables. The findings show that personal socioeconomic status (income and education) are significantly associated with changes in self-rated health during the onset of the crisis. The findings for ecological variables show that the variables measuring exclusion (material deprivation and low work intensity) play a significant role in the explanation of inequalities in health and how they changed during the crisis. Both indicators are negatively associated with self-rated health, while the Gini index and the proportion of the population in long-term unemployment do not have a consistent significant effect. These findings support the hypothesis that there are higher risks to wellbeing in more unequal societies compared with more equal societies.
Background
The impact of economic crisis on health is a highly significant topic in contemporary discussions regarding the determinants of wellbeing. The debate between studies that report a positive impact on population health (Ruhm, 2016; van Den Berg et al., 2020) and those finding a negative impact (Davalos & French, 2011) shows the complexity of the relationship between economic recession and health in contemporary societies. The Great Recession of 2008 has given rise to a striking increase in studies that contribute to this debate. In this regard, it is possible to identify two major threads in the studies addressing the role played by the 2008 financial crisis in terms of health.
One group of studies has used individual variables to evaluate the impact of the crisis on alcohol consumption (Harhay et al., 2014), health and mental illness (Bartoll et al., 2014; Gili et al., 2013) and self-rated health (Reile et al., 2014). This line of research generally points to the Great Recession having a negative impact on individual health indicators, with few exceptions (Latif, 2020). A second group of papers is characterized by the use of ecological, group, and/or aggregated data and indicators in order to analyze the relationship between health and the Great Recession. These studies analyzed the impact of the crisis on general and cause-specific mortality rates. Their findings have been heterogeneous. Studies that analyzed suicides (Huikari et al., 2019; Reeves et al., 2015) and mental and behavioral disorders (De Vogli et al., 2014) identified an increase in mortality due to both causes during the onset of the crisis. Studies that considered other causes of mortality report that the reduction in general and cause-specific mortality rates characteristic of European societies continued during the onset of the Great Recession (Baumbach & Gulis, 2014; Regidor et al., 2014), although a slowing in the reduction of mortality rates has been recorded (Laliotis et al., 2016).
The main limitation of the literature, whether in the case of the first or the second group, is that the evidence produced does not facilitate an understanding of the complexity of the impact of economic crisis on population health. The studies mentioned had the aim of identifying a potential impact of the crisis on health and the meaning of that impact (Parmar et al., 2016). While this is a highly important research topic, there is also a need to examine the processes that mediate the complex relationship between crises and health, and an understanding of these processes would make it possible to grasp some of its complexity. The proposal of this study is that social inequalities are a central and constitutive element of said complexity. The argument is underpinned by the existence of a social gradient in health, such that socioeconomic status has an impact on the prevalence and incidence of numerous diseases (Dugravot et al., 2020; Lewer et al., 2020), including mental disorders and those affecting psychological wellbeing (Lorant et al., 2003), quality of life (Watson et al., 2017), and self-rated health (Warren & Hernandez, 2007). Moreover, the available studies have shown that macrosocial inequalities, examined using ecological data, are as important as interindividual inequalities, or even more so, in explaining health differences (Subramanian et al., 2001). This statement forms part of a general argument, according to which individual health is related not only to interindividual and intergroup inequalities, but also to the existence of macrosocial processes such as corruption or cultural characteristics (Achim et al., 2020). In this vein, the extent of inequality in a society is expected to be a determinant of population health, meaning that more unequal societies would be related to worse health indicators than more equal societies. The available empirical evidence focuses on the role played by inequality of income and wealth distribution in terms of mortality and life expectancy, and it appears to offer reasonable support for this hypothesis (Hiilamo, 2014; Messias et al., 2011; Wilkinson, 1992; Wilkinson & Pickett, 2006, 2008). The structure of unequal societies negatively affects population health, particularly among groups in disadvantaged areas as regards distribution of resources.
These studies, conducted in stable economic times, underpin the hypothesis that the social gradient in health will be particularly significant in explaining the impact of economic crises on population health, particularly in the case of the 2008 crisis. However, the literature that is specific to the Great Recession did not address the complexity of inequalities and their central role in the social gradient in health. In the case of studies using ecological data, the indicator of inequality (change in GDP, increase in unemployment rate) has typically been used more as a marker for the onset of crisis. In the case of population studies, the most commonly used inequality indicators are unemployment and/or belonging to disadvantaged ethnic groups. In all cases, these are measures that do not capture the complexity of inequality in contemporary societies or the impact of the crisis on the consolidation of a model of inequality based on social exclusion processes (Dagdeviren et al., 2017; Mercille & Murphy, 2016).
This type of analysis offers notable potential benefits. It is necessary to emphasize that the effects of the Great Recession on the health of the population have been described in various countries and social contexts and taking into account various dimensions of health. As stated by Birgisdóttir et al. (2020) in their study on the impact of the crisis on cardiovascular problems in Iceland, the 2008 collapse was an extreme and sudden event that patently compromised the health of the population. Along these lines, the results obtained by Beletsioti and Niakas (2019) in Greece suggest that during the onset of the crisis, the predictive capacity of socioeconomic indicators (including income and education) for quality of life rose significantly, with an increase in the social gradient compared to immediately before the crisis. In the area of mental health, several studies suggest the potential utility of incorporating a multilevel analysis such as those used to examine social inequality. In Italy, an increase has been reported in admissions due to affective disorders among the general population, with a causal relationship established between increased unemployment and admissions for severe mental disorders during the crisis (Wang & Fattore, 2020). These results appear to be replicated in Spain (Oliva et al., 2020). A study by Kronenberg and Boehnke (2019) suggests that the impact of the crisis on the population’s mental health is mediated by the changes occurring in the socio-employment context. Their study, carried out in Great Britain, found that even employees who remained in employment during the crisis faced an increased likelihood of deterioration in mental health as a result of changes in the conditions and characteristics of employment arising out of the 2008 crisis, particularly as regards increased workload, restricted training opportunity and reduced labor mobility. In summary, the available empirical evidence shows the global impact of the Great Recession on population wellbeing and health, as well as the need to identify the socio-structural elements that make it possible to understand the processes involved.
Within this context, the aim of this research was to analyze the role played by socioeconomic inequalities in the effect of the 2008 economic crisis on population health in Spain. Specifically, the aim was to analyze the relationship between individual health level score variations and (a) interindividual socioeconomic inequalities and (b) macrosocial (ecological) inequalities, as well as to evaluate any interaction between these levels. Various circumstances invite the view that the Spanish case is particularly significant in this regard: the intensity of the economic recession, the marked increase in the inequality gap after 2008, and Spain’s administrative territorial organization into autonomous communities (regions) with notable differences in terms of social inequalities. Specifically, longitudinal data were used from the European Union statistics on income and living conditions (EU-SILC) survey conducted during the onset of the Great Recession. In order to achieve the proposed aims, a multilevel dataset was created including ecological variables measured at a regional level, as described later.
Territorial and Administrative Organization in Spain
The Spanish State is organized based on the existence of 17 autonomous communities (“regions”) and two autonomous cities (Ceuta and Melilla). Each region constitutes an administrative entity that affects a territory and a population, within which framework political representatives are elected via universal suffrage and whose government and/or institutions have exclusive powers to design, approve and implement policies in the education, healthcare, budgetary, judicial, and social areas. The high level of regional autonomy as to the implementation of these policies is accompanied by significant differences in population and territory size, levels of wealth and wellbeing, social stratification characteristics, size of internal inequalities, demographic dynamics, cultural characteristics, and other factors. The region is also a fundamental element in the construction of its population’s identity. It is therefore a fundamental system for economic, social, cultural, and institutional differentiation in Spain.
Methods
Data and Measures
The data used were taken from the European Union statistics on income and living conditions (EU-SILC) survey. Data were accessed through the project “RPP 141/2015-EU-SILC-EHIS: The impact of the Great Recession on health inequalities in Europe.” Data also came from the Life Conditions Survey (ECV, due to its initials in Spanish) conducted by the Spanish National Statistical Institute (INE, again due to its initials in Spanish). The ECV has a longitudinal design with a 4-year rotating panel, which permitted an analysis of the evolution of the various indicators during the four waves that comprise each panel. Specifically, longitudinal data from the survey conducted in the 2008 to 2011 period were used. This period was selected so that the data would adequately reflect the role played by social inequalities in health differences during the Great Recession. Data were used corresponding to participants aged 18 or over, for whom there was complete information on the study variables (n = 5.924). The subsample for Ceuta and Melilla was excluded due to its low n and the extreme scores in the different measures of social inequality. The average age of the sample in 2008 was 46.44 years (SD = 17.78), with 51.8% women (n = 3.071), 30.9% having completed compulsory education (n = 1.829), 45.8% having completed secondary studies (n = 2.714), and 23.3% having completed higher education degrees (n = 1.381). Ethical approval was obtained for the national survey according to the national guidance and regulation at the time of data collection.
The health indicator (outcome variable) was a five-point measure of self-rated health (SRH), ranging from “very bad” (1) to “very good” (5). Self-rated measures are among the commonest means of evaluating health status in a summarized manner, their usefulness having been demonstrated in a large number of studies (see Schnittker, 2004), mainly because of their well-known validity as a predictor of mortality (Idler & Benyamini, 1997; Idler et al., 1999). The variables used to predict health scores were organized in hierarchical/nested form in three levels: four moment measures (waves) nested in individuals nested in regions. The first level was defined by the four moments at which participants were interviewed (2008, 2009, 2010, 2011). The second level included the individual socioeconomic inequality measures most commonly used in the literature (income and educational level) and demographic control variables (sex and age). The third level included inequality-related social and contextual ecological variables corresponding to the regions in which participants were resident. The study variables are described in Table 1.
Information About the Variables Included in the Study.

Statistical Methods
Given the nested structure of the data, a multilevel regression analysis was performed with maximum likelihood (ML) estimation. Multilevel regression analysis provides an analytical framework when the processes that affect the outcome variable are hypothesized to operate at more than one level. Its use offers two fundamental advantages (West et al., 2015). First, multilevel analysis permits analysis in the same model of the impact of variables corresponding to different levels, including multilevel interaction. Second, it facilitates the incorporation of fixed and random effects into the specification of the model.
Multilevel techniques provide estimates of relationships between individual variables and the variations between regions that cannot be explained by such variables. Moreover, it is possible to estimate the variation in selected individual associations between regions (random-slope parameters) and, at the same time, the interaction between individual-level variables and contextual-level measures. As multilevel linear models are an extension of the linear model, the assumptions include linear relationships, homoscedasticity, and normal distribution of the residuals. The assumption of independence of observations and errors is not applied, since the correlations between cases caused by higher-level variables tend to be included. In our case, the lack of independence in the observations caused by level-3 variables (region) is included in the analysis model. In addition, in repeated-measures designs it is not necessary to restrict the covariance structure to being spherical. The unstructured covariance structure model was used to fit the data. This model is the most parsimonious and requires no assumption in the error structure (Shek & Ma, 2011). An unstructured covariance matrix permits estimation of the intercept and slope variances when the latter is included in the random part of the model, as is the covariance between the intercept and slope.
ML properties include asymptotic consistency (approaches the parameter value with increasing sample size), efficiency (lower variance than other estimators), and parameterization invariance (estimates do not change when measurements or parameters are transformed in allowable ways). As a result, ML estimation is generally robust, producing estimates that are asymptotically efficient and consistent. In fact, with large samples as in the case of this study, ML estimates are robust against mild violations of the assumptions (Hox, 2010). Specifically, non-normal distributed residual errors on the group level of a multilevel regression model appear to have little or no effect on the estimates of the fixed effects (Maas & Hox, 2004). As such, the estimate of the regression coefficients is unbiased (Elff et al., 2021). This characteristic is particularly significant for the present study, given that the coefficient estimations mainly correspond to fixed effects. It is important to bear in mind that the ML estimators of the variance components do not correct for the degrees of freedom lost due to the estimation of the fixed effects, and the estimates of the variance components are generally small. In this vein, ML produces random effects estimates that could be biased (underestimated). However, more substantial biases occur with smaller samples (fewer groups). Sample size is hence a highly significant element for the proposed analysis. Moreover, the necessity to detect both fixed and random effects coefficients increases the complexity in terms of power and sample size issues in multilevel linear models. Recommendations made by Kreft and de Leeuw (1998) suggest that if the model incorporates cross-level interactions (as in the case at hand), then the number of clusters must be around 20 in the higher level-variables, in addition to having adequate group sizes. The multilevel structure for the data used in the present work comprises four measures/moments (level 1) nested within 5924 individuals (level 2) nested within 17 regions (level 3). The minimum n corresponds to the Balearic Islands (153) and the maximum to Andalusia (626). In general, our dataset is reasonably aligned with the aforementioned recommendations. Table 2 shows the sample size in each region.
Sample Size in Each Region.

In order to determine the significance of the different groups of variables, they were introduced in successive steps based on the following theoretical models: (1) “household income”, including only the income distribution variable; (2) “time and income”, adding the interaction between income and the four waves; (3) “social exclusion”, including the level-3 (macro) variables that define social exclusion, together with GDP and sanitary expenditure per capita as control variables; (4) “social inequalities”, adding two traditional variables for the measurement of social inequalities, namely the Gini coefficient and the long-term unemployment rate; and (5) “full model”, including the interactions between the income variable (level 2) and the variables measuring social inequality (level 3). The models were nested and developed by adding variables to the previous model.
The general design for the models tested in our work is the following:

Where SRH of individual i in region j and wave t is a function of p level 2 variables (

For level-2 variables (first line in the model),

Concerns could be raised about using regression analysis to fit ordered categorical variables (self-rated health). In this vein, Liu and Agresti (2005) have shown that OLS regression is a frequent choice for the analysis of ordered categorical outcomes in social sciences. Moreover, recent research suggests that inferences in these cases can be considered robust to violation of model assumptions in terms of Type I error and statistical power (Larrabee et al., 2014). Recent studies have adopted this strategy by using the same outcome variable (Sánchez-Moreno et al., 2016), including studies with a longitudinal design (Latif, 2020). Quantitative variables were introduced after obtaining Z-scores.
Results
The effects of the crisis on average SRH scores (Table 3) were non-linear, with the 2011 wave recovering the levels recorded in 2008 after 2 years of falls in the SRH average. The results set out in Table 2 suggest a social gradient in health for both income and (particularly) education. The percentage prevalence of ill health was 8% in 2008, 9% in 2009, 8.8% in 2010, and 8.2% in 2011. Information about data distribution of the level-3 variables by region can be found in the additional material.
Mean (and Standard Deviation) for Self-Rated Health by Income Quintile, Sex, and Education.

Individual socioeconomic status showed a significant association with variations in health during the initial phase of the crisis. A social gradient in SRH was found for both linear distribution of income and education (Table 4, model 1). The interaction between income and the “time” variable (model 2) suggested that the association of the former with health increased over the course of the three waves. Both linear and quadratic rates of change for individuals were significant. In both models, it was found that the estimation of variance of a random intercept and the variance of a random slope for the “time” variable resulted in statistically significant values, though not the covariance between them. When the level-3 social exclusion dimensions were added (model 3), a negative relationship appeared between SRH and percentages of the population in situations of material deprivation and living in a household with low work intensity. The linear rate of change for individuals was not significant in this model. The long-term unemployment rate also showed a significant effect, though positive in this case (model 4). The inclusion of long-term unemployment and Gini index (model 4) and interactions between income (level 2) and social inequalities (level 3) (model 5) did not produce a significant change to the fit of the models.
Multilevel Estimated Effects of Region-Level and Individual-Level Variables on Repeated Measures of Self-Rated Health: Individual Continuous Income.

p < .001. **p < .01. *p < .05.
Distribution of the population in income quintiles (Table 5) had a significant association with SRH, such that the two lower-income quintiles comprised a homogenous and disadvantaged group in the resulting gradient. The results obtained are similar to those described in the preceding paragraph. Models 1 and 2 were consistent with their counterparts in Table 3. It is worth noting that the interaction between income (quintiles, in this case) and time was significant, but only in the case of quintile 3, for which the passage of the years of crisis was related to a deterioration in health, taking quintile 5 as a reference point. The main differences between the results shown in Tables 3 and 4 were identified on introducing the level-3 variables. The inclusion of macrosocial exclusion dimensions (model 3) resulted in a non-significant effect on linear rate of change (“time” variable). Moreover, model 4 was not significant: the significant effect of long-term unemployment did not result in an increase in the explanatory capacity of the model. Additionally, unemployment at level 3 did not have a significant effect when interactions were incorporated into model 5, in which context a significant effect was found for the Gini coefficient. A significant interaction was found in this model between income quintiles (level-2 variable) and the Gini coefficient (level-3 variable), such that quintiles 2 and 4 were related to higher levels of health as the Gini coefficient increased, taking quintile 5 as a reference point.
Multilevel Estimated Effects of Region-Level and Individual-Level Variables on Repeated Measures of Self-Rated Health: Income Quintiles.

Only significative interactions are included.
p < .001. **p < .01. *p < .05. †p < .10.
Robustness Checks
To check the robustness of the finding, we conducted analyses to determine whether our results were driven by urbanization and living with a partner. The fit of model 3 (see Tables 4 and 5) was analyzed for people with and without partners, on one hand, and for those living in densely populated areas (at least 1,500 inhabitants per km2 and a minimum population of 50,000), intermediate areas (density of at least 300 inhabitants per km2 and a minimum population of 5,000) and thinly populated areas (the remainder). The results are shown in Tables 6 and 7. The pattern of association of the level-2 variables with SRH—particularly individual income and the income quintiles—was consistent and robust for the various sample categories defined in both tables. The same applies to the association between level-3 variables (regional) and SRH. In this regard, the main variations are related to the “with partner vs without partner” variable. As may be observed in Tables 6 and 7, the results obtained suggest that having a partner implies a degree of protection against the consequences of inequality in our societies. This result may be linked to the importance of loneliness as a risk factor for health (Beutel et al., 2017), especially in the case of older people (Cohen-Mansfield et al., 2016). In general terms, in any case, the results of the robustness checks suggest a stability and consistency in the results obtained in this study.
Multilevel Estimated Effects of Region-Level and Individual-Level Variables on Repeated Measures of Self-Rated Health, by Living with Partner and Urbanization: Individual Continuous Income.
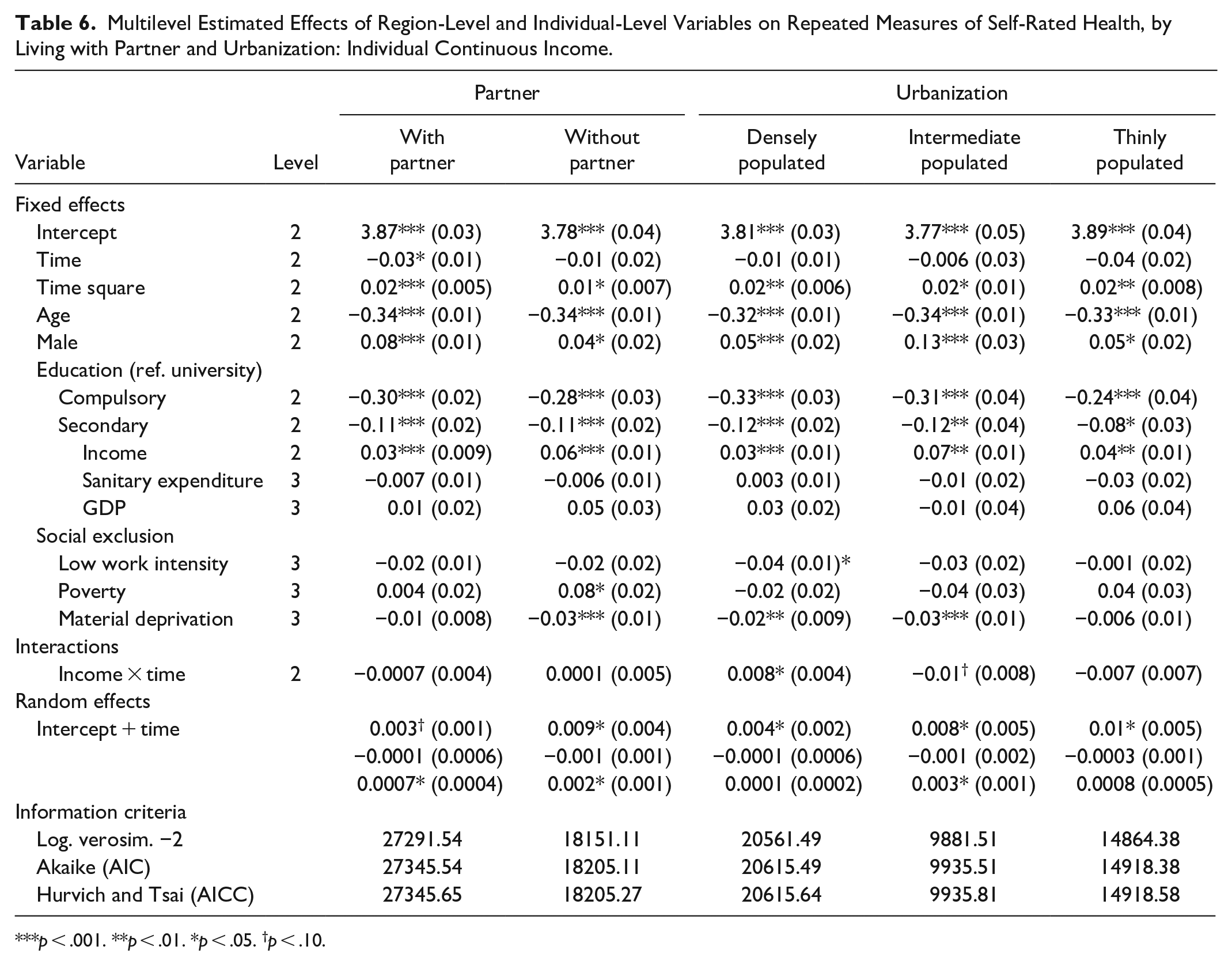
p < .001. **p < .01. *p < .05. †p < .10.
Multilevel Estimated Effects of Region-Level and Individual-Level Variables on Repeated Measures of Self-Rated Health, by Living with Partner and Urbanization: Income Quintiles.
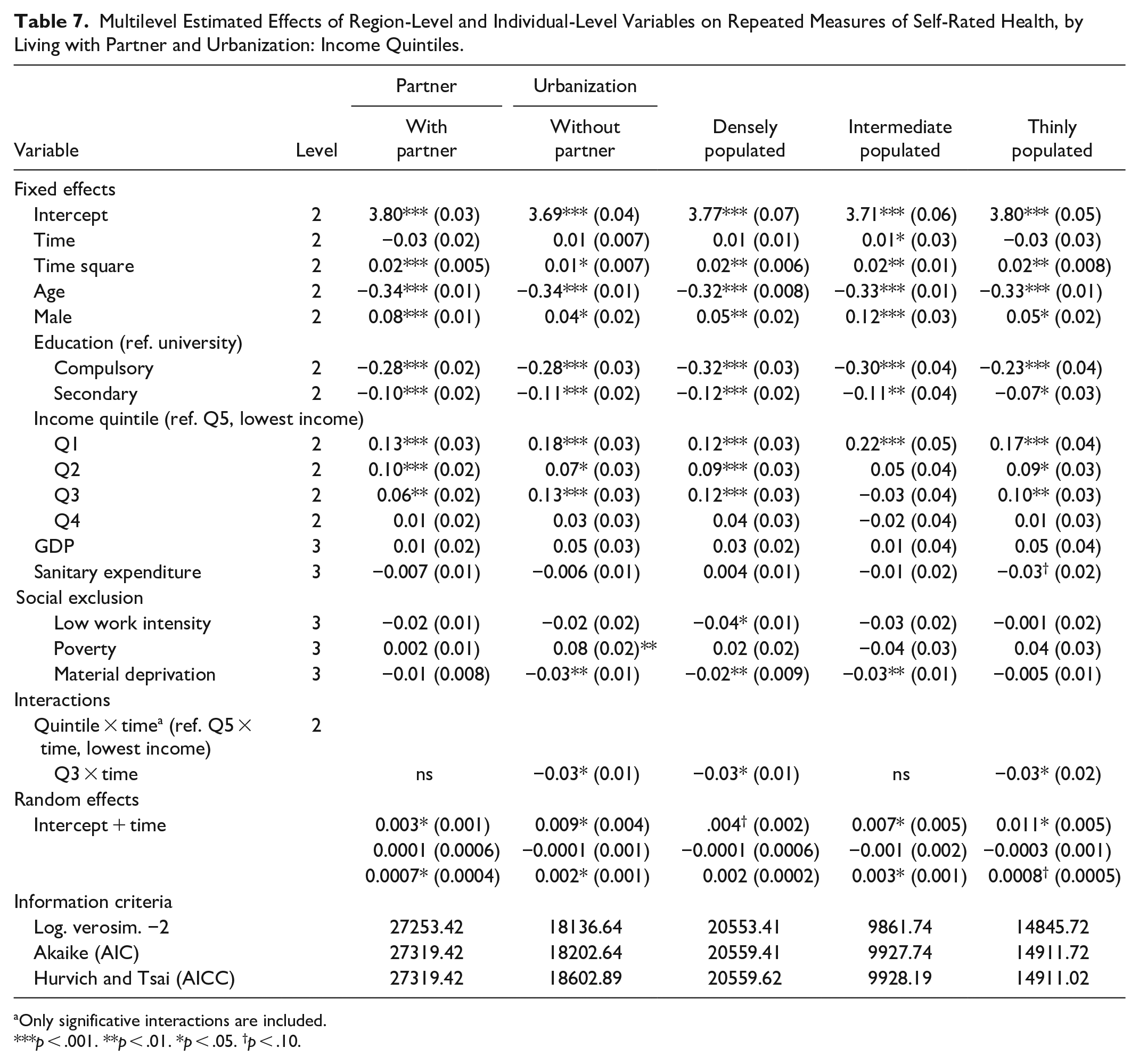
Only significative interactions are included.
p < .001. **p < .01. *p < .05. †p < .10.
Discussion
Our findings suggest a short-term impact of the Great Recession on SRH, such that the crisis had a negative and significant effect in the phase immediately following its onset. However, this initial linear association was completed with a non-linear effect during the four years taken into account in this study, meaning that average health scores in the 2011 wave tended to return to pre-crisis values. These findings are consistent with previous studies (Toffolutti & Suhrcke, 2014) and specifically with studies referring to Spain (Regidor et al., 2014). However, this study proposes that in order to understand the relationship between economic recession and health, it is not sufficient merely to analyze the direct association; rather, it is also essential to analyze the role played by the socioeconomic context. The hypotheses were that (1) the effects of the Great Recession vary among different socioeconomic groups and (2) the effects of the crisis on individual health depend on the structure and extent of socioeconomic inequalities as a whole. The main innovation of our study is that it estimated the association of both individual-level variables and regional-level variables with an outcome variable measured at the individual level (SRH), making use of multilevel analysis techniques with longitudinal data gathered during the onset of the Great Recession.
In our findings, personal income showed a positive association with health during the development of the crisis. This association is present for both the current income measure and the measure reflecting ranking in terms of income distribution (quintile). Specifically, the results suggest the existence of two homogeneous groups defined by an association between income and health, namely those composed of lower-income quintiles (Q4 and Q5) and the rest of the population. This evidence is added to that which is already available (Aittomäki et al., 2014), with the particular feature that our longitudinal data were obtained during the initial phase of the crisis. In fact, there is an interaction between income and wave across all models, meaning that the positive association between income and health becomes more significant as the effects of the Great Recession develop. Along these same lines, our findings show the significance of education (Mackenbach et al., 2008), in this case as a mechanism for alleviating the effects of the crisis on health.
However, the main contribution of this study is the identification of an association of regional-level social inequality measures (level 3) with individual health. The relation of the Great Recession with the population’s SRH varied as a consequence of regional differences (level 3) in the magnitude of social inequality. This evidence is consistent with the findings of previous studies (Karanikolos et al., 2016). The particular feature of our study is that it addresses the impact of ecological inequalities on health during the Great Recession from a multilevel perspective. This means that it is possible to include in our analyses the role of regional variables (level 3) on individual health during the financial crisis of 2008. To date, there is notable evidence as to the impact of income distribution (Subramanian & Kawachi, 2004), in the sense that societies with higher differences tend to show worse health indicators. Our research expands this interpretation, suggesting that the role played by economic crises in population health can be understood through differences in their socioeconomic inequality structures and in the extent of said inequalities among the population. For example, the interaction between income quintile and Gini coefficient (Table 4) suggests that the SRH of individuals located in the lowest income quintile deteriorates in comparison with the intermediate quintiles as population income inequality grows in the context of crisis.
Along these same lines, the social gradient in health during the crisis includes a multilevel association with SRH of both individual socioeconomic status and the socioeconomic inequalities that characterize and distinguish the regions in which those individuals are resident. One of the most significant findings in this regard is the negative association of health with material deprivation rates and with the percentages of households with low work intensity in the region of residence. These results emphasize the central role of social exclusion in understanding contemporary socioeconomic inequalities. The consequence of the Great Recession was the consolidation of a model of inequalities based on social exclusion processes. These processes do not respond to measures in terms of presence/absence (employment/unemployment; poverty/no poverty) or to solid social class anchors (Sassen, 2014); rather, they develop more flexibly and subject to changes in relatively short periods of time. In this vein, our results show that the regional indicators of material deprivation and work intensity (indicators of social exclusion) have an effect on the SRH of individuals even when variables are included in the model whose effects have traditionally been studied, such as the Gini coefficient and the percentage of the population not in employment (Cox et al., 2007).
It is also striking that the regional Gini coefficient had a significant association with SRH scores exclusively when family income (level 2) were classified by distributing the population in quintiles (Table 4). The Gini coefficient thus only has an statistical effect on SRH levels when one considers the ranking in terms of income distribution (quintiles), but not when absolute current income is taken into account (Table 3). This suggests that it is the inequality associated with income distribution, rather than individual differences in current income, which makes the larger contribution to explaining the association of this variable with SRH at the onset of the crisis. Along the same lines, Table 4 indicates that the inclusion of long-term unemployment did not result in an increase in the explanatory capacity for our model (model 4). Taken as a whole, these results underline the important for health of the emerging patterns of social inequality in contemporary societies. Material deprivation and low work intensity describe a collective scenario that is characterized by uncertainty and social fragility (Afifi et al., 2015). A high rate of material deprivation identifies a lifestyle short of activities and needs commonly accepted as basic (annual holiday; telephone; TV; car; keeping the home sufficiently warm) or intense situations of daily financial stress (arrears on mortgage or rent payments; meals with meat, chicken, fish or vegetarian equivalent every other day; unexpected financial expenses). In turn, a high rate of low work intensity describes an insecure, precarious and fluctuating socio-employment context. Recent studies (López Gómez et al., 2017) suggest that the fluctuations and changes that characterize a flexible working life (such as frequency and duration of periods of inactivity and number of contracts) have growing importance for health. As such, material deprivation and low work intensity refer to a systematic and long-term issue affecting daily life, which in a context defined by social exclusion is no longer exclusively – at least, not necessarily – linked to situations of unemployment or to differences in terms of social class. Put differently, our results suggest that the social gradient in health that crystallized in Spanish society during the Great Recession can most satisfactorily be explained by reference to an emerging pattern of socioeconomic inequality based on the concept of exclusion.
Therefore, even the sign of the relationship for the level 3 (regional) variables is inverse in our results. In the case of the long-term unemployment rate, our study adds its voice to those already in existence suggesting that at the times when unemployment becomes widespread in society, its effect on health may not be significant (Buffel et al., 2017) or may be counterintuitive, meaning that this situation of high aggregate unemployment would allow individual/family socioeconomic situations to be attributed to external causes (Oesch & Lipps, 2013). Our results are also consistent with those obtained in numerous studies that find a positive relationship between economic crisis and health (or a negative relationship between economic crisis and mortality), since the majority of these studies take increased unemployment as a key indicator to identify the onset of crisis (Sánchez-Moreno et al., 2016). In contexts of high unemployment, processes of social comparison would permit a form of self-serving bias involving the individual situation of economic disadvantage being reduced in importance as an indicator of individual social status. However, the social context molded by social exclusion renders this kind of bias difficult to maintain, giving rise to a framework in which there is an increased likelihood of psychosocial impairment. As such, in the context of the Great Recession, material deprivation and low work intensity among the population gave rise to a deterioration in daily lives and in social interaction of particular significance among the middle classes and for disadvantaged socioeconomic groups, producing limitations on social participation and access to the social and material resources that define the standard of wellbeing in Spanish society. This entails an erosion of cohesion, cooperation and social support (Kondo et al., 2008). This importance of exclusion indicators during the onset of crisis (specifically, the proportion of the population in situations of material deprivation and low work intensity) entails an increase in uncertainty and socioeconomic risk associated with daily life. This is a change in patterns of inequality that has previously been described in other contexts. A study by Son et al. (2012) addresses the impact of the crisis that developed in South Korea at the end of the 1990s and whose results show a significant widening of the inequality gap in terms of mortality and life expectancy. The authors link this result to an increase in socio-employment inequalities arising from the impact of the crisis and the growing importance of atypical, irregular forms of employment that had been practically non-existent in that country. It is specifically this increase in the flexibility of the labor market that represents one of the distinctive features of models of exclusion and which has been contemplated in our analyses through the concept of work intensity.
The result is an emerging pattern of social comparison and socioeconomic differentiation (Wilkinson & Pickett, 2007) that crystallized in the case of Spain during the early years of the Great Recession. The impact of this situation on health can be explained by its association with psychosocial processes involved in deteriorating health and directly related to the distribution of inequalities in material living conditions, extensively described in the literature. The role played by social exclusion indicators in health during the Great Recession can thus be explained via their impact on processes such as daily or chronic stress (Wilkinson, 2016), access to and management of information on healthy behaviors and medical treatment (Pampel et al., 2010), the quality of social relationships (Wilkinson & Pickett, 2006), reduced social support (Thoits, 2010) and the importance of social capital (Islam et al., 2006). In this regard, research is needed to identify the specific mechanisms pursuant to which the interaction between distribution of inequalities and the place occupied by individuals and households in said distribution has an impact on health during periods of recession and socioeconomic crisis.
The analysis and design of social and healthcare policies represents a fundamental challenge in this context. The main limitations of this study should be noted in this respect, as they directly affect this issue. First,the use of a self-reported measure of health must be taken into account. Although this is a widely-used strategy in international health research, the reliability of responses can nonetheless be a matter of concern. The question here is whether or not there is major measurement error when individuals have to self-assess their own level of health. This error may be the result of biased responses, owing to misunderstanding of the question, memory lapses when self-assessing health or the existence of biases (including being self-serving or a particular response being socially desirable) resulting from a respondent’s individual characteristics. It is also necessary to note that different populations may use different assessment patterns when asked about their health. This is described as the reporting heterogeneity problem (Shmueli, 2003). In the specific case of this research, there is no reason to suspect a non-random distribution of measurement errors. Moreover, cultural differences between different regions in Spain do not seem sufficiently intense to imply a reporting heterogeneity problem, since the participants form part of a single population. Finally, previous longitudinal studies have shown that respondents provide reliable information on their own health status and how it changes over time (Vaillant & Wolff, 2012, p. 96). In any event, it would be useful to have studies that analyze the effect of economic crises by using a combination of subjective health data and clinical measures (Onur & Velamuri, 2018).
Third, there is a need to exercise caution when establishing causal relationships, particularly of a one-directional nature, between the exposure variables of our analysis and health (in our case, SRH). First in this respect, our study might have omitted exposure variables of significance in the multilevel analysis, especially in the level-3 (regional) range of variables. Research regarding social inequalities and health, and specifically the empirical evidence regarding the social gradient in health, has produced noteworthy progress in the identification of variables that are significant in understanding health. Based on said empirical evidence, the design of models verified in this study through multilevel analysis includes control variables that are particularly significant in the case of SRH. This is true of age and sex (level 2, individual) and healthcare spending and regional wealth (level 3). However, it is possible that a significant variable might have been omitted. Second in this context, the literature on inequalities in health is marked by the dialectic between the hypotheses of social causation and social selection. As is well known, there is empirical evidence to support both hypotheses (Kim & von Dem Knesebeck, 2018; Vancea & Utzet, 2017) and it is reasonable to conclude that they are both present in the social reality. In fact, it is possible—indeed probable—that health has reciprocal effects on social processes usually incorporated as exposure variables such as educational attainment, employment and occupational status, income, and socioeconomic inequalities. Due to all of this, the existence of a relationship of reverse causality is an issue that poses notable difficulties in research on the social gradient in health (Lynch & Brown, 2011).
It is necessary to bear both problems in mind when drawing conclusions from the results of this study. Specifically, the second (simultaneity bias) may give rise to an overestimation of the association between one or more exposure variables and the outcome variables—in our case, an overestimation of the variables measuring social inequalities. The proposal of this article—that is, the importance of inequality-related social processes for understanding differences in health in contexts of economic crisis—is based on sound theoretical and empirical foundations as regards the social determinants of health. Moreover, the robustness checks performed show a notable degree of consistency of the statistical model. Finally, it should be emphasized that the incorporation of two variations of the key variable at level 2 (income and quintiles) generates results that are consistent with each other and with the theoretical and empirical precedents on which this study is based.
Third, the data analyzed correspond to the initial phase of the Great Recession and are limited to a 4-year period. It is hence impossible to address potential changes in trends regarding the association between the Great Recession, social inequalities and medium- and long-term health. As a result, a second limitation arises. The data do not permit a proper analysis of the impact of policy responses to the crisis in Spain on health indicators and their relationship with inequalities. We are fundamentally referring to policies based on the principle of austerity. However, the broadening of focus in order for our analysis to include both the processes traditionally studied at times of recession (unemployment, income, GDP) and emerging elements related to social exclusion makes it possible to examine the processes that impact on the social gradient in health. One of the main gaps in the existing evidence concerning the impact of the Great Recession on health is that it has failed to capture the mechanisms that affect health outcomes (Parmar et al., 2016). This limitation is particularly important from the policy design perspective. Our study contributes to closing this gap, by showing that the social gradient in health at the onset of the Great Recession in Spain became steeper as a result of the effects of the crisis on the consolidation of an inequality structure based on social exclusion. In this context, austerity policies (Greer, 2016; Mestres et al., 2018) represented an added problem for daily life with relation to key dimensions (pharmaceutical spending, healthcare, social services, housing, etc.), which both increased the impact of unequally distributed resources (especially income, in light of our results) and meant an increase in future costs for the healthcare system (in the event of reversal of the measures based on cuts to public spending) or rendering chronic the situations of social deterioration and worsening quality of life affecting growing numbers of the population (Global Burden of Disease Group, 2018).
Taken as a whole, the findings of this study reveal the complexity of the factors related to individual wellbeing at times of crisis and social change. The data for Spain suggest that the impact of the Great Recession of 2008 on health is directly shaped by the context of inequality in which the crisis took hold. It is worth emphasizing that the role played by contextual variables is to a large extent independent of their impact on inequality measures among individuals and/or households, as is observed from the absence of significant interactions between level 2 and level 3 variables in our analyses. In turn, this social distribution of inequality is also influenced by the recession and its effects on the labor market and the distribution of resources among the population. Specifically, the 2008 crisis consolidated a model of inequality linked to exclusion processes whose influence on population health indicators may be ever greater in the future (Morgan et al., 2007; O’Donnell et al., 2018), while the effect of other socioeconomic components of inequality models whose contemporary validity may be fading (such as class stratification or income distribution) may be reduced (Beckfield, 2004). It is necessary to generate empirical evidence that facilitates identification of the characteristics of this potential change to the social gradient in health, incorporating into our analytical models complex and appropriate ways of measuring exclusion in economically developed societies.
Specifically, it appears important to distinguish exclusion-related processes and consequences from poverty-related processes and consequences. The concept of social exclusion is not limited to insufficient income; it also implies that a proportion of the population is deprived of connection to many of the jobs, services and resources they need in order to fully participate in society (Madanipour et al., 2015). It is therefore a problem affecting access to citizen status as defined in the reconstruction of European democracies that began following the Second World War, and represents a de facto breakdown in access to valuable resources (education, housing and neighborhood conditions, labor market, etc.) as a key element for understanding social inequalities in health (Andriani & Karyampas, 2010). As stated by Levitas et al. (2007, p. 25): “Social exclusion is a complex and multi-dimensional process. It involves the lack or denial of resources, rights, goods and services, and the inability to participate in the normal relationships and activities, available to the majority of people in a society, whether in economic, social, cultural or political arenas. It affects both the quality of life of individuals and the equity and cohesion of society as a whole”.
There hence appears to be a need for research that examines the measurement and analysis of processes of economic, social, political and cultural exclusion that create barriers to participation in those spheres for certain social groups or for a growing segment of the citizenry in contemporary societies. This implies taking steps to operationalize social exclusion as a range of social processes, rather than an exclusively economic source of inequality. It is necessary to improve the measurement tools that are available to us, emphasizing the distinction of the concept of social exclusion from others (especially that of poverty) (Andriani & Karyampas, 2010). Progress in this regard would permit an analysis of the relationship between the content of social exclusion and health, would provide particularly valuable information for analyzing the social gradient in health, and would facilitate the tackling of situations that are particularly serious for wellbeing and quality of life such as deep exclusion (Miliband, 2006). Along these lines, the results of our study invite reflection regarding the growing importance of exclusion for understanding health and wellbeing in contemporary societies.
Moreover, the construction of a theoretical approach to exclusion based on the existence of a limitation on access to valuable collective resources should incorporate the role played by the breakdown or malfunctioning of major societal systems. These social processes generate an unequal distribution of resources and also limit participation in (and access to) the different spheres of social life (economic, cultural, political, etc.) in which those resources are generated, which in fact implies a lack of citizenship.
The crisis set in motion processes involving the review of social and economic policies, which, based on austerity principles, may have influenced the form and intensity of the social gradient in health. In Spain in particular, far from impacting on the transformation of the social relationships that are at the root of social exclusion, these policies deepened the differentiation that these relationships of inequality imply, increasing limitations on access to resources and the full participation of a growing cohort of citizens. Austerity policies represented a practice that is obstructive to the transformation of social relationships required to construct inclusive societies (Sealey, 2015). The increased impact of exclusion in the social organization of inequalities represents a collective challenge that must be confronted. In this regard, alignment of institutions and public policies with the objective of reducing social inequalities in health is essential. This objective must be decisively included on the political agenda. The situation of social and economic uncertainty caused by the COVID-19 pandemic has tested supranational political institutions, and particularly the European Union (EU), which has to meet the challenge of establishing social inclusion and fighting exclusion as basic criteria of the recovery and development model in the economic context arising from the pandemic. Applying the arguments used by Veit-Wilson (2006, p. 333) before the Great Recession in the area of child poverty, one may argue that if specific elements are not incorporated for the design, articulation and assessment of State anti-exclusion policies, “the rights remain declamatory but have no means of enforcement, and therefore they cannot be treated as rights in any serious sense”. In this regard, the impact of the 2008 crisis on the health of the population was significantly lower in those countries in which the policies implemented before and during the crisis were not based on cuts to services and social protection, and specifically to universal health system coverage (Latif, 2020). During the development of the crisis in Spain, the measures adopted to combat the effects of the economic shock were largely directed by the State/central government and included the introduction of spending limits, budgetary restrictions, reduced salaries for public employees and cuts in universal access to public services and benefits. However, the executive capacities of regional (local) governments in terms of health, social, educational and other budgets led to notable differences in the level of implementation of austerity measures and public spending cuts (Bacigalupe et al., 2016). In our results, no significant association was found between public health expenditure or GDP per capita and SRH. However, both variables were considered as control variables. Studies are therefore required that engage in detailed and specific examinations of the potential effect of local differences in the application of austerity measures on differences in health during times of economic downturn.
The findings of this study point to social exclusion as a fundamental factor in understanding the impact of the economic crisis on health. In this regard, our study reinforces the hypothesis pointing to socioeconomic inequalities as a fundamental cause of differences in health (Phelan et al., 2010). These inequalities must hence be incorporated into global strategies as risk factors (Stringhini et al., 2017). This implies that social exclusion shapes a range of factors that can be affected by the implementation of policies aimed at reducing inequalities, eliminating material and social deprivation, securing universal access to resources and medical technology, creating safe and healthy environments and reducing the risk of poverty associated with flexibility and at-risk situations in the labor market (Farrants et al., 2016; Lundberg et al., 2008; Voßemer et al., 2018; Wulfgramm, 2014).
Conclusion
The aim of this study was to analyze the impact on individual SRH level score variations of (a) interindividual socioeconomic inequalities and (b) macrosocial (ecological) inequalities, as well as to evaluate any interaction between these levels. The results show a significant and positive association between income and education (level-2, individual) and SRH. This association is maintained when ecological variables (level-3) are incorporated. Of these variables, those related to social exclusion have the greatest predictive capacity for SRH values (low work intensity and material deprivation), as opposed to variables such as the Gini Index and unemployment. As regards multilevel interaction, our results suggest that contexts involving higher levels of income inequality increase the probability of deterioration in the health of low-income groups. These results suggest that changes in SRH among the Spanish population during the Great Recession are directly related to the consolidation of a model of inequality based on social exclusion. As such, the findings obtained reinforce the line of research establishing the fundamental role of macrosocial processes that shape contexts of socioeconomic inequality. Contexts involving more exclusion (in our case, the regions with higher levels of exclusion) generate health differences and contribute to explaining the relationship between economic crisis and the distribution of health among the population.
In this regard, this work provides a contribution with a clearly international dimension, despite its limitations. As stated in the analysis of the available empirical evidence, the effects of the Great Recession on health have been documented on a global scale across a large number of countries. Our study adds to the existing evidence, in addition to suggesting the need to increase efforts to understand the role played by social inequalities, from a multilevel perspective, with special emphasis on the identification of emerging elements that articulate the change in models of inequality. This implies focusing attention on exclusion as a particularly important social determinant of health. Along these lines, several studies have reported an increase in global-level inequalities as a result of the Great Recession (Bogliacino & Maestri, 2016). This increase in inequalities has even been detected among social groups that were traditionally affected by lower levels of inequalities in the traditional variables of socioeconomic status (income and education). We are referring to an increase in inequalities among different countries, but also and particularly to increased inequalities within the different societies. For example, there has been a striking increase in socioeconomic inequalities since the Great Recession in European countries in which the Welfare State had contributed to reducing the size of inequalities (Eurofund, 2017). It appears that the increasing inequality gap is a process that is taking place on a global scale and which is patently affecting the development of the globalization process. As a result, the findings of this study would not only be useful to analyze the social gradient in health in countries with high levels of inequality that are undergoing phases of economic crisis. Our findings are also significant in analyzing the social determinants of health in societies where inequality gaps have traditionally been smaller but might have grown recently or could be affected by subsequent crises. This is an especially significant debate in the current context, in which the COVID-19 pandemic represents a challenge to health not only from the medical and healthcare perspective, but also as a result of its impact on the economic cycle. The clear threat of a new global recession increases the value of results from studies such as this one that attempt to understand the processes involved in the deterioration of health in a context of severe economic crisis.
Our study used data based on self-reported conditions and coming exclusively from the initial phase of the Great Recession. The available empirical evidence suggests that the short, medium and long-term effects of the cycles of economic crisis can differ in quantitative and qualitative terms. This study focused on the onset of the Great Recession because its main aim consisted of analyzing the impact of socioeconomic inequalities on said effects (van der Wel et al., 2018). Specifically, the study proposal consisted of identifying the emergent vectors of inequality—creating social exclusion—that contribute in contemporary societies to understanding the uneven impact of the effects of the economic crisis on population health. It was particularly useful to analyze data relating to the first years of the crisis for this purpose, thereby supplementing previous studies that had aims focused on categories related to socioeconomic status (income, education, etc.) or employment status. With this strategy, in short, it was possible to analyze and compare the impact of social exclusion measures that attempt to capture the complexity of inequality in contemporary societies.
In any case, both limitations (the use of SRH in a sample from the initial phase of the Great Recession) invite further investigation along certain lines of analysis. Further research should address the effects of social inequality on health in crisis and post-crisis contexts in the medium and long term. This is particularly important in global contexts of economic, social and healthcare-related uncertainty such as the circumstances resulting from COVID-19. The use of several outcome variables, including health measures that do not come from self-assessment, would increase the usefulness of the knowledge generated and contribute to the design and implementation of effective policies and programs to reduce social exclusion and mitigate its impact on citizen health during any period in the economic cycle, and particularly at times of uncertainty and recession.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440211052925 – Supplemental material for From Income Inequalities to Social Exclusion: The Impact of the Great Recession on Self-Rated Health in Spain During the Onset of the Economic Crisis
Supplemental material, sj-docx-1-sgo-10.1177_21582440211052925 for From Income Inequalities to Social Exclusion: The Impact of the Great Recession on Self-Rated Health in Spain During the Onset of the Economic Crisis by Esteban Sánchez-Moreno and Lorena Gallardo-Peralta in SAGE Open
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Access to the data was granted by Eurostat through research project: RPP 141/2015-EU-SILC-EHIS: The impact of the Great Recession on health inequalities in Europe (Eurostat). This work was partly funded by Fundación FOESSA (Spain), research project “Desigualdades sociales y bienestar en España: biografías de exclusión durante la gran recesión y su impacto en la salud y la calidad de vida”.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.