
Abstract
The difficulty in understanding new virus strains affects scientific efforts to immediately develop drugs and vaccines to stem the spread of viral diseases. As a result, social measures remain handy tools to address viral diseases. Nigeria joined the rest of the world to introduce social containment measures for the new COVID-19 pandemic. The study examines the factors predicting adherence to COVID-19 containment measures in selected Nigerian communities. It adopts multi-stage cluster sampling in a survey involving 183 respondents from two states and Nigeria’s Federal Capital Territory, Abuja. Multiple regression and descriptive statistics were used to estimate the influences of social factors (religion, family, friends), demographic characteristics (age, residential area, gender), and credibility factors (perceived trust, ease of adherence) on attitudes toward media messages and social measures on COVID-19 prevention guidelines. Results show that age, gender, marital status, type of street, education, and state of residence have significant influence on adherence to COVID-19 messages. While age and gender positively correlated with credibility assessment, type of street was negatively associated with credibility assessment of COVID-19 messages. Social factors have more predictive influence on adherence to COVID-19 messages than credibility assessment of COVID-19 messages. The study discusses the implications of relationships between demographic factors and adherence to COVID-19 messages.
Introduction
Infectious diseases are one of the leading causes of death globally, with the attendant severe effects on global economy and social relationships (Bloom et al., 2017; Centre for Infection and Immunity, 2020; Fauci, 2001; Hussaini, 2020). The globalization of diseases is underpinned mainly by increased movement of people locally and internationally. Less than 3 months from the discovery of the novel COVID-19 in Wuhan, China in December 2019, the disease was declared a pandemic by the WHO on March 11, 2020 (Ekong et al., 2020). Over time, the trajectory of disease pandemics has undermined belief that vaccines and antibiotics would win the war against emerging infectious diseases, EIDs (Bloom et al., 2017; Fauci, 2001). EIDs are so named because their scale of effect has never been anticipated, recognized, experienced, or estimated. As a result, social measures are veritable universal standards to fight EIDs such as COVID-19 (Bloom et al., 2017; Lone & Ahmad, 2020; Oliver et al., 2020). The present study examines adherence to social measures among some Nigerian communities, namely, use of communications, personal hygiene, and avoidance of mass gatherings, movement restrictions, and physical distancing.
Studies indicate that citizen adherence to health promoting measures is basic to any effort to contain infectious diseases (Galasso et al., 2020; Okten et al., 2020). Adherence to disease prevention guidelines is associated with reduced risks of further spread (Matrajt & Leung, 2020; Soo et al., 2020). In just 1 month of implementing COVID-19 prevention recommendations in Italy, infections reduced by 78,000 and by 66,000 in New York City within 3 weeks (Galasso et al., 2020). Soo et al. (2020) studied influenza incidence under COVID-19 control measures in Singapore and found a marked decline (64%) in cases between periods of implementation of social preventive measures and when they were not in place. Matrajt and Leung (2020) found a strong positive link between periods of implementing and relaxing of social distancing in the US and increases or falls in positive cases, hospitalizations and deaths related to COVID-19.
While research is already growing on the factors affecting compliance with health measures during health emergencies, there is need to continue such studies in developing countries, where the health system needs more robust support from social measures (Obi-Ani et al., 2020). Experiences from different countries in disease prevention have become guides to other nations in their continuing attempt to control the spread of infectious diseases (Paules et al., 2017). Studies also need to focus on “rarely-considered” factors such as type of residential areas, which have been found to challenge adherence to health measures during health emergencies (Nivette et al., 2021).
Necessity of Measuring Adherence to Disease Containment Communications
Though studies are not conclusive on the effectiveness of high adherence to containment messages, there is consensus on the close association between likelihood of early containment and higher levels of adherence (Block et al., 2020; Okten et al., 2020). Studies have also observed that there is far higher consensus on the efficacy and necessity of protection guidelines than there is on general adherence to them, and that the situation is a result of variations in exposure to information sources (Al-Hasan et al., 2020; Farooq et al., 2020; Igielnik, 2020; Saey, 2020; Zhong et al., 2020). The level of trust in information source (media, medical experts, government officials, and interpersonal communication) was an important predictor of health risk perception, self-efficacy, and attitudes to hygiene during infectious disease outbreaks such as H1N1, SARS, and COVID-19 (Coroiu et al., 2020; Czeisler et al., 2020; Kings et al., 2018; Lau et al., 2011; Teasdale & Yardley, 2011; Williams et al., 2020). Some studies have reported lower levels of citizen trust in government information than in the media as well as reported self-adherence and belief that others were not adhering (Czeisler et al., 2020; Williams et al., 2020).
Apart from being veritable means to containing the spread of infectious diseases, social measures also help to relieve the struggling health system in many countries (Nussbaumer-Streit et al., 2020). Assessment of adherence to containment measures is even more critical as many countries (e.g., Nigeria) have since reopened their economies and are facing the risk of resurgence (Block et al., 2020). Similarly, while some nations have relaxed some preventive measures, the resurgence of COVID-19 in some areas means that countries may re-impose the restrictions. As of July 2021, a more contagious Delta variant was spreading fast, forcing many countries to reintroduce social control measures such as movement restrictions and compulsory wearing of facemasks in public. Following the detection of the Delta variant in Nigeria on July 8, 2021, there were 1,866 cases in just 2 weeks, and a 154% increase from the 735 cases recorded in 2 weeks before the announcement (Asadu, 2021). Consequently, inadequate understanding of the predictors of adherence to preventive messages may negatively impact future enforcement (Coroiu et al., 2020; Nivette et al., 2021).
Brooks et al. (2020) found that residents who experienced quarantine were subject to fears of infection, irritation and tedium, insufficient supplies, insufficient information, economic pressures, and stigma. Williams et al. (2020) found that after experiencing initial COVID-19 lockdown, participants in a UK study expressed fears about social reintegration and the future. Researchers therefore suggest that the long term need to sustain the containment measures makes it necessary to find and implement long-term strategies to help people. This would depend on knowledge of factors affecting adherence to containment messages (Al-Hasan et al., 2020; Williams et al., 2020). Studies have identified some of the factors, but have rarely indicated the links between the factors, health risk perception, and containment messages as done in the present study. Some of the demographic, media, and social factors are highlighted below.
Studies in 27 countries including Italy, the Democratic Republic of Congo, the UK, Canada, and the US have established that being female is associated with higher obedience to messages than men during COVID-19 (Daoust, 2020; Galasso et al., 2020; Nangsangna & Da-Costa Vroom, 2019; Ntoimo et al., 2018; Nzaji et al., 2020; Okten et al., 2020). There were also strong gender differences in the perception of COVID-19 as a health risk, and this was connected to the gender differences in mortality and vulnerability levels of the disease across countries (Galasso et al., 2020). Gender, literacy, age, occupation, and area of residence were associated with high levels of adherence to quarantine guidelines in Italy (Carlucci et al., 2020; Okten et al., 2020).
Studies have also pointed out the social and credibility factors affecting responses to containment communications. In Nigeria, low citizen trust in government guidelines, difficulties imposed by the health system, social media, and inadequacy of social amenities negatively impact COVID-19 containment efforts (Obi-Ani et al., 2020; Reuben et al., 2021). In South Africa, Jaja et al. (2020) report that COVID-19 infections spiraled in many communities due to gross violations of social distancing rules in burials, religious, and cultural events. Studies also found that measures that were easy for individuals to observe and those emphasizing protection of others received higher, though not perfect levels of adherence (Coroiu et al., 2020; Zhou et al., 2020).
In addition to identifying the foregoing factors, the present study links them (delineated into social, demographics, and credibility factors) to how they affect adherence to containment messages from government, the social media, social interrelationships, and the mass media. Specific questions were used to identify, for instance, the credibility assessment of COVID-19 messages from various sources. The study draws from the factors to gauge the beliefs, ratings, and perceptions of people about adherence to COVID-19 messages as well as in avoidance of risky behavior. The study thus puts adherence or non-adherence side by side perceived risk of contracting coronavirus.
Theoretical Framework
We applied the health belief model (HBM) to articulate this study. The model was developed by Hochbaum, Rosenstock, and others in the 1950s. It was further modified by Rosenstock (1974) and Becker (1974). The model which stands out as one of the most profound theories in health behavior research (Jacobs et al., 2017; Lambert & Loiselle, 2007; Onuora et al., 2021), is premised on the assumption that individuals’ health actions are prompted by their perception of the gains and benefits of health messages targeting a particular condition.
The HBM holds that the following basic constructs determine individuals’ ability and motivation to change their health behavior: risk susceptibility (i.e., belief about getting a disease or condition), risk severity (i.e., belief about the seriousness of the disease or condition), benefits of action (i.e., belief about the potential positive aspect of a health behavior), barriers to action (i.e., belief about the likely negative aspect of a health behavior), cues to action (i.e., factors needed to trigger decision making process to adopt a recommended action), and self-efficacy (i.e., an individual’s perceived confidence in their ability to engage in a health action) (Corcoran, 2007).
The HBM is currently being applied in several COVID-19 studies to understand COVID-19 preventive behaviors (e.g., Barakat & Kasemy, 2020; Jose et al., 2021; Raamkumar et al., 2020; Shahnazi et al., 2020). When situated within the context of the present study, these fundamental principles could help to inform scholarly understanding of the extent of trust or credibility that individuals have in COVID-19 protocols. It could also show how individuals perceive social cues concerning COVID-19 prevention as well as their attitude toward preventive measures. Examples of how the key constructs of the HBM might be linked to individuals’ preventive health behavior from COVID-19 are shown in the following questions and statements: “Do I have a very high chance of contracting coronavirus?” is a question related to perceived vulnerability of getting COVID-19. Also, a statement about risk severity may be summed as: “My overall health would be endangered if I contract COVID-19” (This might be particularly true for those with terminal conditions). “Can I prevent COVID-19 by practicing social distancing or washing my hands regularly?” describes the potential benefits of adopting COVID-19 preventive practices. A statement on the perceived negative aspect of COVID-19 preventive practices would posit: “I could not adhere to the COVID-19 messages because I thought they were impracticable.” Statements such as: “I was constantly persuaded by my housemate(s) to adhere to the messages” and “I adhere to the COVID-19 messages because I want to and for the sake of adherence” are examples of individuals’ cues to action and self-efficacy construct respectively. In terms of self-efficacy, the question could also be asked: Can I sustain the demands of continued adherence, and is it more profitable to do so?
Studies using HBM to explain COVID-19 preventive behavior have often undertaken such research within some socio-demographic, social, and structural contexts. The HBM construes these as modifying factors, which are critical to behavior change (Corcoran, 2007). For example, certain factors such as age, race, gender, health condition, socio-economic status, ethnicity, and residential areas have been associated with COVID-19 in an observational study (de Lusignan et al., 2020). As already noted, a number of studies have highlighted gender differences in attitude and behavior toward COVID-19 (e.g., Galasso et al., 2020; Okten et al., 2020). Furthermore, although empirical knowledge about older people’s attitude toward compliance to the COVID-19 protocol is scanty, a study of elderly people and responses toward the disease in 27 countries suggest that elderly respondents were less responsive to taking responsibility in terms of isolating, wearing of facemasks, etc. (Daoust, 2020). While certain categories of demographics have been identified as more susceptible to the disease than others, we are yet to fully understand to what extent categories with or without risk factors adopt COVID-19 preventive behaviors. Owing to the above discussion, we hypothesize that:
Age, gender, economic status, marital status, type of streets, state of residence, occupation, and educational achievement will significantly predict adherence to COVID-19 messages.
Age, gender, economic status, marital status, type of streets, state of residence, occupation, and educational achievement will significantly predict credibility assessment, social influence, and attitude toward media messages on COVID-19.
Credibility assessment, social influence, attitude toward media messages on COVID-19 will mediate the influence of respondents’ demographic characteristics on adherence to the messages.
Methods
The study adopted correlational survey research design. Correlation survey is a study of the relatedness of two or more groups (Paul, 2008). Correlation survey research focuses on the establishment of relationship between two or more variables in the same population or between the same variables in two or more groups (Gall et al., 2007; Leedy & Ormrod, 2010; Paul, 2008). This study adopted a correlation survey research design because the study intended to identify the relationship among credibility assessment, social influence on COVID-19, attitude to media messages on COVID-19, and adherence to COVID-19 messages among Nigerians.
Procedure
Multi stage cluster sampling, used for large heterogeneous populations, was applied in the study. Study participants were selected from Lagos State and the Federal Capital Territory, FCT, Abuja, which were epicenters of the pandemic in Nigeria. The third area of study, Enugu State, was an area of relatively low prevalence. As of July 28, 2021, Lagos State had the highest figure at 62,668 (36.5%) cases of Nigeria’s 171,728 diagnosed cases. Abuja had 19,951 cases (second highest—11.6%), while Enugu had 2,490 (14th most affected—1.44%).
The survey began on May 7, 3 days after ease of lockdown in Lagos and Abuja. Four research assistants were enlisted for face-to-face questionnaire administration in each study area, and they (the assistants) reported very uncordial atmosphere in data gathering in Lagos and Abuja as respondents needed substantial prodding to respond to the questionnaire. Eight local governments were randomly selected from the strata of local governments in Lagos and Enugu States, four for each. Being a federal capital, Abuja is divided into area councils, and the Abuja Municipal Area Council (AMAC) was randomly selected.
By simple random method, four residential areas and five streets were selected from the directory of streets for each of the selected local government areas and the AMAC. Systematic sampling through a table of random numbers was used to select households studied. Residents 18 years and above completed the questionnaire after granting verbal consent. The study computed a total population of 10,735,151 for the states and AMAC. Using an online calculator, a sample size of 364 was computed and shared proportionally to the study areas. After questionnaire retrieval, a total of 183 copies were adjudged fit for analysis from 212 copies recovered. The lockdown mood was still very much in Lagos and Abuja, and severely hampered questionnaire administration and retrieval.
Sample
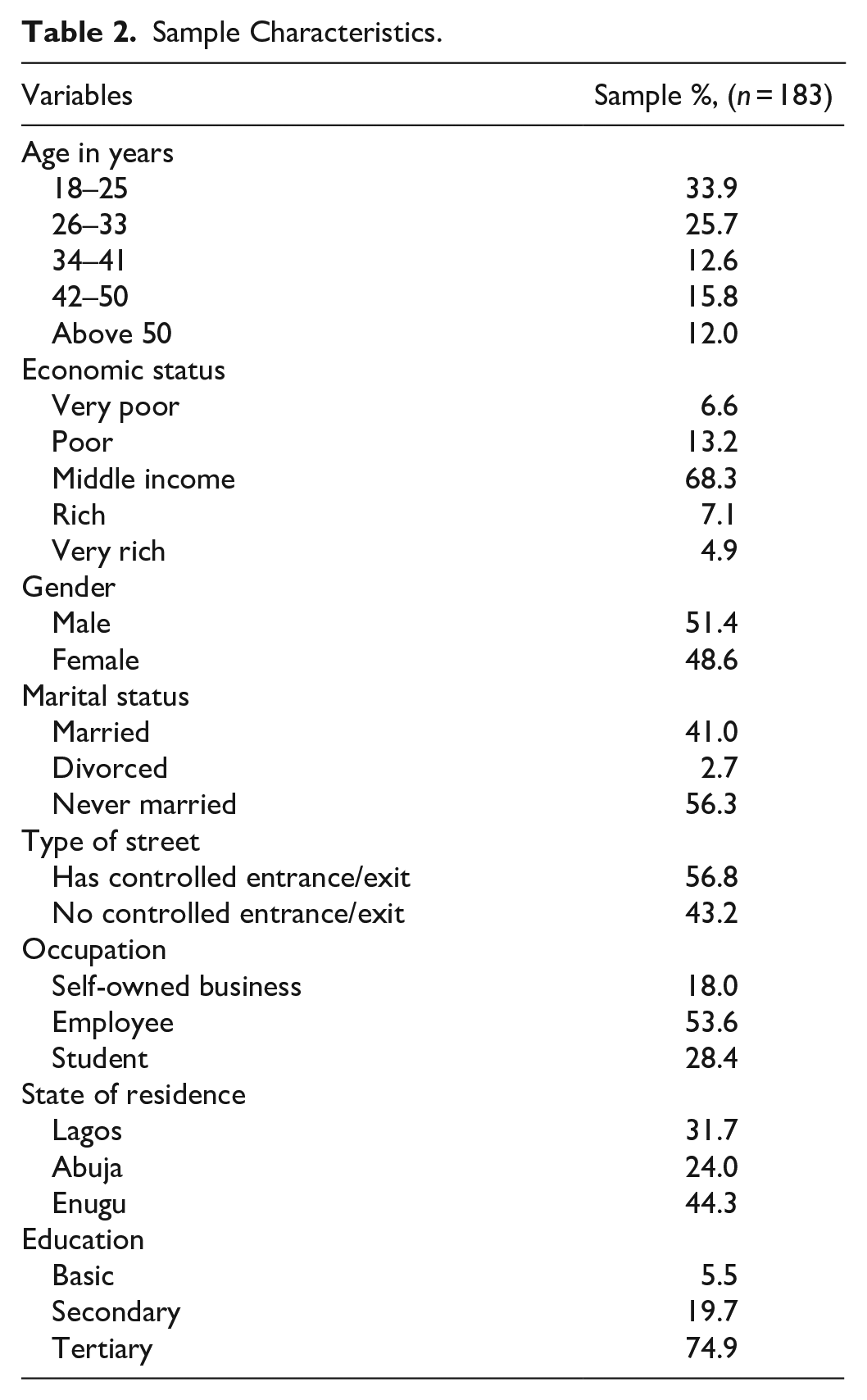
The participants comprised 54.1% males. The highest proportion of participants (33.9%) was between 18 and 25 years. The majority of participants (68.3%) were middle income earners. Details about the sample characteristics are shown in Table 2.
Measures
A self-developed, 46-item structured questionnaire with five sections was adopted for the study. The sections of the questionnaire include demographic characteristics of the study participants, adherence to COVID-19 preventive measures, credibility assessment of COVID-19 messages, social influence on COVID-19 and attitudes toward media messages on COVID-19. Demographic information of the participants was assessed using questions related to their age, economic status, gender, type of street, educational level, occupation, and participants’ state of residence.
The Adherence, Credibility Crisis, and Constraints to COVID-19 Messages Scale (ACCCCS)
A scale on the subject matter of the study was developed. The scale focused on the adherence, credibility crisis, and constraints issues about COVID-19 messages and was named ACCCCS. For this study, adherence to, credibility of, and constraints to COVID-19 messages served as the dependent variables. The independent variables on the other hand were respondents’ age, economic status, marital status, gender, type of street, occupation, state of residence, educational attainment, and type of COVID-19 messages.
For this study, adherence to COVID-19 messages was described as the extent to which respondents practiced the COVID-19 safety guidelines or general precautions as it were. Adherence was therefore measured with a 12-item, 5-point, Likert scale ranging from 0 = “never” to 4 = “very regularly.” Some examples of the items in the sub-scale include: “I wash my hands regularly,” “I practice social distancing,” etc. A reliable Cronbach’s alpha of .72 was obtained. Furthermore, credibility was defined in the study as the level of believability and acceptability of COVID-19 messages in Nigeria. Because a number of Nigerians have expressed profound doubt as to the existence and the actual severity of the disease, it becomes imperative to ascertain how our respondents perceive it. As a result, credibility was measured with a 10-item, 5-point Likert scale spanning from 0 = “strongly disagree” to 4 = “strongly agree.” For example, some of the items were worded as follows: “COVID-19 is actually in Nigeria,” “I think Nigerians like other Africans do not fall ill from the disease,” etc. We obtained a reliable Cronbach’s alpha (α) score of .76 for the scale. Equally, the concept of social influence on COVID 19 was conceptualized in the study as significant influencing factors (relating to COVID-19 messages) that affect perception, attitude, and behavior toward COVID-19 messages. Social influence was therefore measured with a 6-item, 5-point Likert scale anchored with 0 = “strongly disagree” and 4 = “strongly agree.” One of the items on the sub-scale was worded as follows: “media stories made me to doubt COVID-19 as a reality.” A reliable Cronbach’s alpha (α) score of .75 was obtained. Attitude toward the messages was then defined within the study context as individuals’ views of messages concerning COVID-19. Attitude was further measured with an 11-item, 5-point scale ranging from 0 = “strongly disagree” to 4 = “strongly agree.” Some of the items were worded like this: “media messages about COVID-19 are scary and capable of making me worry less of adhering to the safety precautions,” “messages coming from my housemates or significant others are enough to compel adherence,” “adherence to COVID-19 messages are impracticable,” etc. Again, a highly consistent Cronbach’s alpha (α) score of .78 was obtained. Altogether, the result of the combined reliability measure was good: α = .86 in our study.
Determination of Validity of the ACCCCS
The ACCCCS instrument was subjected to content and face validation by experts in the Department of Psychology, University of Nigeria, Nsukka. The experts were required to examine the instrument with regard to its relevance in terms of items, appropriateness of contents and representativeness of the various areas of the study. The experts evaluated whether the scale assesses all fundamental aspects of the study. The comments and observations made independently by the experts helped the researchers to modify and produce the final instrument.
Exploratory factor analysis was also used to examine the construct validity of the Adherence, credibility crisis, and constraints to COVID-19 messages scale (ACCCCS). With a sample size of 183, we were confident that it will be sufficient to carry out the factor analysis. Stevens (1996) note that a small sample size of 150 cases should be sufficient if solutions have several high loading marker variables. The reliability of the ACCCCS which was later divided into sub-scales (TCCAS = Total COVID-19 credibility assessment scale, TCSIS = Total COVID-19 social influence scale, and TCFAMS = Total COVID-19 factors affecting attitude toward messages scale) was further ascertained using the Cronbach alpha. The Cronbach alpha’s scores for each of the four sub-scales are presented in Table 1. The process of ascertaining the construct validity of the ACCCCS are discussed briefly in the following sub-section.
Factor Loadings and Communalities Based on a Principal Components Analysis With Obilim Rotation for 39 Items From the Adherence, Credibility, Social Influences, and Attitude Toward COVID-19 Messages Scale (ACCCCS) (N = 183).

Factor Analysis
Initially, the factorability of the 39 ACCCCS items was examined. Several well recognized criteria for the factorability of a correlation were used. Firstly, high correlations of .3 and above were observed with at least one other item, suggesting reasonable factorability. Secondly, the Kaiser-Meyer-Olkin measure of sampling adequacy was .81 (see Figure 1), above the commonly recommended value of .6, and Bartlett’s test of sphericity was significant (χ2(741) = 3,601.641, p = .000) (see Figure 1). The diagonals of the anti-image correlation matrix were also all over .5. Lastly, the communalities were all above .3, further confirming that each item shared some common variance with other items. Given these overall indicators, factor analysis was deemed to be suitable with all 39 items.
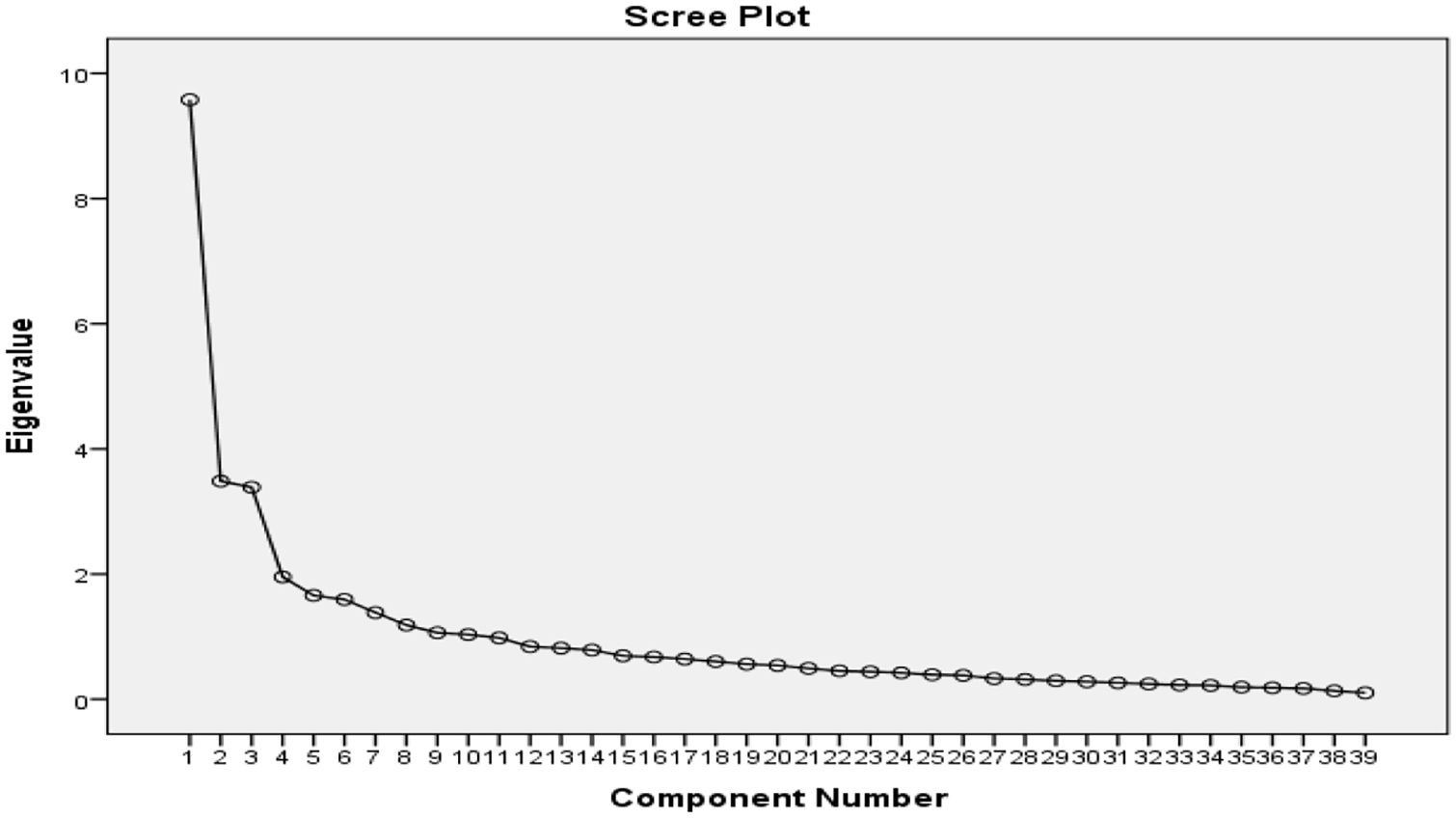
Scree plot showing eigenvalues for each components for items (variables) on the adherence, credibility crisis, and constraints to COVID-19 messages scale (ACCCCS).
Principal components analysis revealed the presence of 10 components with eigenvalues exceeding 1, explaining 24.5%, 8.7%, 8.6%, 4.9%, 4.4%, 4.1%, 3.5%, 2.9%, 2.8%, and 2.6% of the variance respectively. An inspection of the scree plot revealed a clear break after the fifth component. Using Catell’s (1966) scree test, it was decided to retain 10 components for further investigation. This was further supported by the results of Parallel Analysis, which showed only 10 components with eigenvalue exceeding the corresponding criterion values for a randomly generated data matrix of the same size (39 variables × 183 respondents). To aid in the interpretation of these 10 components, Varimax rotation was performed. The rotated solution revealed the presence of simple structure (Thurstone, 1974), with each component showing a number of strong loadings substantially on the first two components.
All retained components explained a total of 68.2% of the variance (see Table 2). Overall, these analyses indicated that these distinct factors were underlying participants’ responses to the ACCCCS items and that these factors were moderately internally consistent. For example, personal and social influence was a theme that was captured under the first factor with a very high loading. Among other factors (components), theme of adherence to COVID-19 measures was also observed with high loadings under the second factor (see Table 2). An approximately normal distribution was evident for the composite score data in the current study, thus the data were well suited for parametric statistical analyses.
Sample Characteristics.
Analysis
The data collected for this study were analyzed using IBM Statistical Package for the Social Science (SPSS) version 23. The socio-demographic characteristics of the participants were analyzed using percentage and frequency count (see Table 2). The variables—adherence to COVID-19 messages, credibility assessment of COVID-19 messages, social influence on COVID-19, and attitude toward COVID-19 media messages scale—were also described using mean and standard deviation (where necessary) and the degree of their relationship was affirmed using multiple regression analysis.
Results
Hypothesis 1. Age, gender, economic status, marital status, type of streets, state of residence, occupation, and educational achievement will significantly predict adherence to COVID-19 messages.
Linear regression was used to investigate the factors predicting respondents’ adherence to COVID-19 messages. The result of the regression suggested that these factors explained 53.6% of the variance in adherence to COVID-19 messages (see Table 3), R2 = .536, F(8, 174) = 8.765, p < .001. It was found that respondents’ age (b = .91, p = .015), gender (b = 2.31, p = .029), marital status (b = 1.40, p = .024), type of streets (b = 3.16, p = .003), state of residence (b = 1.64, p = .047), and educational level (b = 2.96, p = .015) significantly predicted adherence to COVID-19 preventive messages. The correlation coefficients of the predictive factors of adherence to COVID-19 messages are positive. This indicates that an increase in each of the predictive variables leads to a corresponding improvement in adherence to COVID-19 messages.
Hypothesis 2: Age, gender, economic status, marital status, type of streets, state of residence, occupation, and educational achievement will significantly predict credibility assessment, social influence, and attitude toward media messages on COVID-19.
Regression Analysis of Factors Predicting Respondents’ Adherence to COVID-19 Messages.

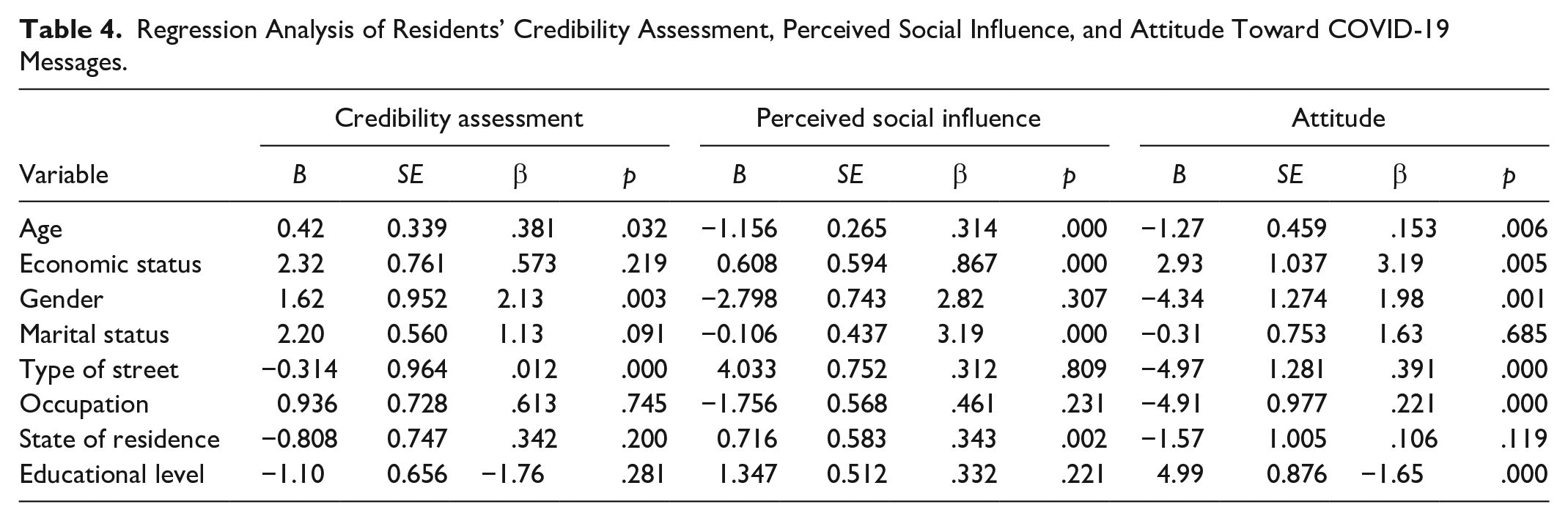
Linear regression was performed to ascertain the influence of respondents’ demographic variables on credibility assessment of COVID-19 messages (see Table 4). Findings showed that the predictors explained 31.8% of the variance in credibility assessment to COVID-19 messages, R2 = .318, F(8, 174) = 10.125, p < .001. Only respondents’ age (B = .42, t = 5.452, p = .032), gender (B = 1.62, t = 3.121, p = .003), and type of streets (B = −.31, t = 2.931, p = .000) significantly predicted credibility assessment of COVID-19 messages. While age and gender positively correlated with credibility assessment, type of street was negatively associated with the outcome variable. This indicates that streets with controlled entrance/exit (i.e., well organized) scored higher in credibility assessment of COVID-19 messages and vice versa. Furthermore, 42.9% of the variances in perceived social influence of COVID-19 messages were explained by respondents’ socio-demographic status, R2 = .429, F(8, 174) = 16.362, p < .001. Respondents’ age (B = .42, t = 4.132, p = .032), economic status (B = 1.62, t = 3.410, p = .003), marital status (B = 1.62, t = 3.810, p = .003), and state of residence (B = −.31, t = 5.020, p = .000) significantly predicted perceived social influence of COVID-19 messages. The correlation coefficients of the predictive factors of perceived social influence of the messages are positive. This is suggestive of the fact that an increase in each of the predictive variables leads to a corresponding improvement in perceived social influence of the messages. Finally, results showed that the predictors explained 46.4% of the variance in attitude toward to COVID-19 messages, R2 = .464, F(8, 173) = 18.720, p < .001. Respondents’ age (B = −1.27, t = 8.132, p = .006), economic status (B = 2.93, t = 4.110, p = .005), gender (B = −4.34, t = 6.311, p = .001), type of streets (B = −4.97, t = 3.101, p = .000), occupation (B = −4.91, t = 3.320, p = .000), and educational levels (B = 4.99, t = 5.331, p = .000) had a significant impact on attitude toward COVID-19 messages.
Hypothesis 3: Credibility assessment, social influence, attitude toward media messages on COVID-19 will mediate the influence of respondents’ demographic characteristics on adherence to the messages.
Regression Analysis of Residents’ Credibility Assessment, Perceived Social Influence, and Attitude Toward COVID-19 Messages.
Multiple hierarchical regression was applied to assess the ability of credibility assessment, social influence, and attitudes toward COVID-19 media messages on adherence to the messages after controlling for age, economic status, gender, type of street, educational level, occupation, and participants’ state of residence in Table 5. The demographic variables were entered at Step 1, explaining 21.0% of the variance in adherence to COVID-19 messages among participants and the variance was significant (R = .206, F(8, 173) = 5.599, p = .000; R2 = .21). After entering scores on credibility assessment, social influence, and factors affecting attitude toward COVID-19 messages at Step 2, the total variance explained by the model as a whole was 45.0% (R = .450, F(11, 170) = 12.638, p = .000; R2 = .375).
A Summary of Hierarchical Regression Analysis of COVID-19 Messages.

Note. TCCAS = total COVID-19 credibility assessment scale; TCSIS = total COVID-19 social influence scale; TCFAMS = total COVID-19 factors affecting attitude toward messages scale.
p < .01.
The three control measures explained an additional 27.1% of the variance in adherence to COVID-19 messages, after controlling for age, economic status, gender, type of street, educational level, occupation, and participants’ state of residence (R2 change = .41, F change(3, 170) = 25.156, p F change = .244). Thus, the result presented in Table 5 showed that social influence and other factors affecting attitude toward COVID-19 messages have more predictive ability on adherence to COVID-19 messages (B = −0.51, t = −4.013, p = .000) and (B = −0.18, t = −2.575, p = .011) than credibility assessment of COVID-19 messages (B = 0.02, t = −.291, p = .771). Meanwhile, participants’ gender was the strongest and only significant predictor of adherence to COVID-19 messages (B = 0.73, t = −3.615, p = .021) among demographic characteristics in the second model. The control variables were necessary to measure more exactly the influences of the independent variables on adherence.
Discussion of Findings
The study examines factors affecting responses to COVID-19 containment measures in selected states and the Federal Capital Territory of Nigeria. It addresses influences of social, credibility, and demographic factors on attitudes to media messages and adherence to COVID-19 preventive measures. The study was done in view of many controversies and contrasting approaches to social measures used in fighting COVID-19 in Nigeria.
Results show that adherence was high generally. Demographic factors such as age, marital status, type of street, state of residence, and educational level had significant positive influence on adherence to COVID-19 messages. The study upholds the importance of demographic factors in adherence to preventive messages as noted in previous studies on infectious diseases (Bloom et al., 2017; Carlucci et al., 2020; Daoust, 2020; Nzaji et al., 2020; Okten et al., 2020). Epidemiologists rate age as the most important factor in the survival rates and attitudes to prevention messages about many infectious diseases (Daoust, 2020). Older adults from 65 years and above are said to be at a higher risk of dying from COVID-19, though adherence to messages has not shown a linear relationship with this fact (Daoust, 2020; Galasso et al., 2020; Okten et al., 2020). However, this appears not to be the trend in the present study. School-age participants were less likely to adhere to the messages than the working class age group (34–41). This is despite the fact that the age range of 18 to 25 and 26 to 33 together constituted more than half of the respondents.
Notably, adherence was far higher for those actions that were strictly regulated such as interstate travels and attendance at large gatherings. Adherence was markedly low for actions that required complete personal discretion, actions seen as difficult to avoid, or those that could be flouted without detection such as helping others to adhere to containment measures, sneaking out of the neighborhood undetected, or going to the market. The forgoing shows that cost of adhering to containment measures, level and ease of enforcement, pressure of household resources, controlled nature of residential areas, and ease of containment measures are important factors to be addressed in future social approaches to infectious disease outbreaks.
Studies in Nigeria and South Africa have indicated the contributions of the uncontrolled exit structure in residential areas, inadequacy of social amenities, burials, and religious-cultural events in the violation of social distancing rules, which caused spikes in COVID-19 cases (Jaja et al., 2020; Obi-Ani et al., 2020; Reuben et al., 2021). Studies have also found that measures that were easy for individuals to adhere to received higher, though not perfect levels of adherence (Coroiu et al., 2020). Thus, adherence to the measures may be connected with people’s calculations and beliefs about the cost of self-protection and the choice between remaining indoors and suffering inadequate supplies. Studies show that people who experienced quarantine reported running out of supplies and lacking information, among other difficulties (Brooks et al., 2020; Williams et al., 2020), and in the case of the present study, such inadequacies were critical to adherence to COVID-19 measures. In Nigeria, comical comparisons have been made about the relative weights of contracting a deadly disease and dying more imminently of hunger (self-efficacy). This was as citizens heavily criticized government for failing to provide palliatives (Obi-Ani et al., 2020).
Self-efficacy therefore ranks above perceived severity and risk of contracting COVID-19. As a result, the first requirement of the HBM comes to the fore, that is, an incentive to ensure adherence to movement restrictions would be provision of palliatives and better controlled residential areas. While problems about trust in government and media information remain, provision of incentives would make people to see the benefit of obeying stay-at-home orders, which are also the ultimate goal of all government and media messages. This may influence the “cue to action” such as conversations among friends or contributions to media programs in a way to support others’ adherence.
Furthermore, respondents’ age and type of street significantly predicted credibility assessment of COVID-19 messages. While age and gender positively correlated with credibility assessment, type of street was negatively associated with the outcome variable. This indicates that streets with controlled entrance/exit (i.e., well organized) scored higher in credibility assessment of COVID-19 messages and vice versa. Respondents’ age, economic status, marital status, and state of residence significantly predicted perceived social influence of COVID-19 messages. The correlation coefficients of the predictive factors of perceived social influence of the messages are positive. This is suggestive of the fact that an increase in each of the predictive variables leads to a corresponding improvement in perceived social influence of the messages. Respondents’ age, economic status, type of street, occupation, and educational levels had a significant impact on attitude toward COVID-19 messages. Therefore, except for predictors such as economic status and educational levels which revealed positive coefficients, respondents’ age, gender, type of street, and occupation were negatively correlated with attitudes toward COVID-19 messages. This therefore suggests that being old, male, living in streets that are not well coordinated (not having controlled entrance/exit), and being a student were associated with negative attitudes toward COVID-19 messages. In the present study, female participants showed higher levels of adherence than males.
Other studies indicate similar findings. Gender, literacy, occupation, and area of residence were associated with high levels of adherence to quarantine guidelines in Italy (Carlucci et al., 2020; Okten et al., 2020). In the Italy study, women, the more highly educated, residents of Southern Italy, middle-aged people, and health workers were more likely to adhere to quarantine recommendations. Studies have linked women’s positive attitudes to health information with their higher tendency to seek and to use information than men and to their higher susceptibility to chronic diseases (Nangsangna & Da-Costa Vroom, 2019; Ntoimo et al., 2018). Future messages can incorporate aspects that encourage women to play bigger roles in encouraging men, especially in familial contexts, to adhere more to preventive guidelines.
Furthermore, while the various marital groups treated credibility assessment and social influence in the same way, they differed in their approaches to media messages. The effect of type of street on adherence was neither significantly influenced by social factors nor credibility factors. Type of street therefore impacted adherence to the messages more than it affected belief in the messages. Occupation and state of residence, however, affected credibility assessment, social influence on COVID-19, and attitudes to media messages. The negative influence of streets without controlled exit on attitudes to preventive messages means that enforcement of containment measures, especially movement, remains a potent tool in fighting infectious disease outbreaks as some studies have shown (Matrajt & Leung, 2020; Obi-Ani et al., 2020; Reuben et al., 2021; Soo et al., 2020).
Conclusion
The study found that adherence to containment measures was high. The influence of age and gender on adherence aligns with the results of extant studies. There were strong implications for the HBM in view of the roles played by areas of residence, credibility assessment of messages and attitudes to media messages toward adherence to preventive measures. That is, the relationship between adherence to prevention guidelines and attitudes to media messages on the one hand and certain social and credibility factors on the other implies that respondents may have had reduced risk perception and disease severity due to perceived cost of (non)adherence. The high influence of social factors may point to the effects of the social media and interpersonal communication in attitudes to COVID-19 while people were confined to their homes. Therefore, the social and infrastructural challenges to adherence are important to the fight against COVID-19. If adherence is related to perceived ease and level of enforcement, then government and the media must pay closer attention to the credibility assessment of their messages. The high-educational level of the participants in the present study may account for the high level of adherence, implying the effects of health literacy. Therefore, future studies can target less educated groups. Future studies should also use much higher samples to increase the generalizability of findings.
Footnotes
Authors’ Note
Respondents offered verbal consent prior to completing the questionnaire.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.