
Abstract
This study examined the relationship between women’s empowerment and different dimensions of emotional violence in Zimbabwe using cluster analysis and logistic regression. We used data from the 2015 Zimbabwe Demographic and Health Survey, a nationally representative household study of fertility, health, and mortality indicators among women aged 15 to 49 years. Our sample consisted of 2,966 currently partnered women at the time of the survey. Our results revealed that more than 60% of the women had experienced emotional intimate partner violence (IPV), of which controlling behaviors were the most prevalent form. The results showed that women empowerment in Zimbabwe is primarily characterized by economic empowerment, household bargaining power, and freedom of movement. At the same time, educational attainment, health decision-making, and attitudes toward gender-based violence had expected relatively weak empowerment effects. The results also revealed that economically empowered women were less likely to experience denigrating or threatening behaviors, whereas those who had high levels of freedom of movement had a lower risk of experiencing all forms of emotional IPV except for threatening behavior. These findings suggest that emotional IPV is a considerable societal problem in Zimbabwe, and interventions that increase economic empowerment and freedom of movement may reduce the risk. Future research studies may examine the likelihood of reverse causality between women empowerment and emotional IPV.
Introduction
Violence against women is considered a major global health and human rights development issue, yet it is often the least punishable crime (Kabir & Khan, 2019; Wekwete et al., 2014; Werwie et al., 2019). Acts of violence against women occur daily in different geographic locations, cutting across different ages, religions, societies, and ethnic groups (Dalal, 2011; Kim et al., 2007). Recent global statistics show that more than a third of women have been victims of physical or sexual violence from intimate and non-intimate partners at some point in their lives (United Nations, 2020). These figures exclude cases of sexual harassment. In sub-Saharan Africa, violence within intimate relationships ranges from 42.3% in Nigeria to 67.7% in Ethiopia (Beyene et al., 2019). Statistics from Zimbabwe indicate that almost a third of young girls have been sexually victimized by the age of 18 years (Zimbabwe National Statistics Agency, 2014), while one in four women have experienced violence within an intimate relationship (Bengesai & Khan, 2020).
Domestic violence, which usually occurs within a marriage or family, is the most common type of violence against women (Kabir & Khan, 2019; Kim et al., 2007; Tran et al., 2018; Wekwete et al., 2014). Terms such as women abuse, women battering, marital violence, intimate partner violence (IPV), or spousal violence have also been used to describe domestic violence (Kabir & Khan, 2019; Kim et al., 2007). In this study, we are concerned with male perpetrated IPV that occurs in the context of intimate relationships (Kabir & Khan, 2019; Kim et al., 2007; Wekwete et al., 2014).
IPV manifests in different forms, such as physical, sexual, emotional, and financial abuse (Gibbs et al., 2018). However, most empirical studies, including those from Zimbabwe, have focused on physical and sexual IPV (e.g., McDougal et al., 2019; Sethuraman et al., 2006; Shamu et al., 2018), with comparatively fewer studies on emotional violence and financial abuse as subtypes of IPV (Dokkedahl et al., 2019). This is despite the fact that emotional violence (a) has now been identified as an indicator of progress under Sustainable Development Goal 5.2 (Sachs, 2012) and is (b) the most experienced type of IPV globally (Dokkedahl et al., 2019; Gibbs et al., 2018; Mills, 1999; Tran et al., 2018). Available evidence suggests that emotional violence might also affect 25% to 30% of Zimbabwean women (Bengesai & Khan, 2020; Wekwete et al., 2014).
One of the major challenges identified in the literature on emotional IPV is the lack of consensus on defining it. For instance, while the World Health Organization (WHO, 2012) makes a distinction between emotional violence (e.g., insults, belittling, constant humiliation, and threats) and controlling behavior (e.g., isolation from friends and family, monitoring and restricting movements, and access to resources), some scholars argue that this separation might be artificial (Dokkedahl et al., 2019; Karakurt & Silver, 2013). Rather, emotional violence should be conceptualized from the perspective of harm, in which case coercive control is seen as a subtype of emotional abuse (Dokkedahl et al., 2019). Indeed, some scholars have shown that control in an intimate relationship is often the underlying factor for other types of IPV (Jewkes, 2002; Johnson, 2001). This is because controlling behaviors do not only reflect a motive of power but also are often a precursor to both physical and sexual forms of IPV (Antai, 2011). A WHO multicountry study found that male partners who had controlling behaviors were more likely to be physically violent relative to their less controlling counterparts (García-Moreno et al., 2005). Other researchers have suggested that the term psychological aggression might be a more useful term representing “the full range of potentially negative intimate interpersonal behaviours without implying, at this point, that all psychological aggression is abusive” (Follingstad, 2009, p. 272). Dokkedahl et al. (2019) argue that while the particular acts of violence might separate the diverse definitions of emotional IPV, the overall psychological harm that these acts cause brings them together. For Karakurt and Silver (2013), emotional violence must be defined as “any nonphysical behaviour or attitude that is designed to control, subdue, punish, or isolate another person through the use of humiliation or fear” (p. 1).
Despite the lack of definitional consensus, some scholars have provided a promising schema for classifying emotional abuse (Follingstad, 2009; Maiuro, 2001). Included in this schema are acts that are intended to (i) denigrate and damage a partner’s self-image or self-esteem, (ii) passive-aggressive withholding of nurturing and support (e.g., punitive use of avoidance or withdrawal, sulking, and emotional abandonment), (iii) explicit or implicit threatening behaviour as well as, (iv) restricting personal territory and freedom. (Maiuro, 2001, p. xi)
Thus, rather than using overly broad classifications, this schema organizes abusive behaviors as multidimensional and according to the areas of impact upon the victim (Villa, 2014). Guided by the schema, this study examines the effect of women empowerment on emotional IPV. We specifically focus on the following emotional IPV dimensions (denigrating, coercive, and threatening behaviors) and use data from the 2015 Zimbabwe Demographic and Health Survey (ZDHS).
Correlates of IPV
Several theories have been used to understand the distinct and overlapping factors that augment a woman’s vulnerability to IPV, including emotional violence (Dutton, 1995; Heise, 1999). For instance, the feminist theories dominant in the literature have focused on the influence of patriarchal beliefs that reinforce male superiority and women’s acquiescence to male dominance (Dutton, 1995). Other scholars have argued that violence is often used to maintain control over limited household resources or to control the behavior of family members (Bulte & Lensink, 2019; Eswaran & Malhotra, 2011; Gelles, 2007). The literature on IPV is also clear that no single theory can sufficiently explain IPV. However, the ecological model, which sees IPV as multidimensional and resulting from the interplay of factors operating at the individual, relational, community, and societal levels, is seen as the most compatible (Heise, 1998; WHO, 2012).
At an individual level, factors such as age, employment status, alcohol and drug use, educational attainment, and history of IPV, among others, have been identified as factors that can either promote or deter IPV (Gibbs et al., 2018; Tu & Lou, 2017). Factors that occur at the relational level include the conflict between a woman and her partner, which can be due to economic stress, the number of wives in a household, and the woman’s position in the family (Djikanovic et al., 2010). Some of the community-level and societal factors contributing to IPV risk include poverty and weak sanctions against perpetrators, and traditional beliefs that rationalize violence against women (Dalal, 2011; Heise, 1998; Tenkorang, 2018). In patriarchal societies such as Zimbabwe, especially among the Shona people in the more traditional rural areas, the wife “belongs” to the whole family, although the husband has exclusive sexual rights (Chitakure, 2016). As a result, the husband’s mother, sisters, brothers, and so on, can force the wife to do domestic chores for them, and if she refuses, they have the “right” to scold her or report her to her husband, who is expected to show his power by disciplining her. If the husband fails to discipline by beating or scolding her, he is labeled a weakling under a “petticoat government” Chitakure, 2016; Siyawamwaya, 2016). Such rigid gender scripts about the role of the wife in the home have made spousal violence, and especially emotional violence in the form of verbal attacks, generally acceptable (Chitakure, 2016; Makahamadze et al., 2012).
Undoubtedly, the relationship between men and women has long been characterized by the unequal distribution of power (Huis et al., 2020). Therefore, it is not surprising that women empowerment has often been identified as one of the approaches for addressing IPV forms (United Nations, 2012). This study contributes to the growing debate by examining the dimensions of women empowerment among Zimbabwean women and their association with emotional IPV. There is a shortage of research studies that have focused on emotional IPV in developing nations such as Zimbabwe, particularly examining the link with women empowerment. For example, we only came across one study in Zimbabwe (see Wekwete et al., 2014), which addresses this aspect, albeit operationalizing women empowerment differently. Thus, there is an apparent gap in knowledge that our study seeks to address. What also makes this study relevant to the Zimbabwean context is the widespread emotional violence, in particular, the constant denigration and humiliation of women, which cuts across all spheres of life ranging from music (Chari, 2008) to politics (Manyonganise, 2015) to marital relations (Chitakure, 2016).
Conceptualizing Women Empowerment
Women empowerment is a multidimensional phenomenon with various indicators used to measure it (Hansen et al., 2020; Kabeer, 1999; Kabir & Khan, 2019). For example, Rowlands (1995) has proposed three dimensions, namely, personal (developing a sense of self-confidence, capability, and undoing effects of oppression), relational (ability to negotiate and influence the nature and decisions made in a relationship), and collective relationships (individuals working together to achieve an outcome as opposed to what each one could have achieved on their own). According to Hansen et al. (2020), the various measures of empowerment are categorized into three distinct but related dimensions, namely, personal empowerment (e.g., self-esteem), empowerment in relation to others (e.g., financial household decision-making), and societal empowerment (e.g., representation of women in parliament). Kabir and Khan (2019) measured the concept of empowerment of women at an individual level and within the confinement of her household, consisting of the ability to make decisions, control over financial issues, and reproductive health. The authors further stated that self-confidence and self-esteem were critical aspects of these forms of empowerment.
Evidently, there is no standard understanding of women empowerment indicators although certain broad domains can be derived from the literature. In this article, we conceptualize women empowerment as a function of a woman’s access to and control over resources and her ability to use these to improve her well-being, that of her family, community, and society at large (Hansen et al., 2020; Kabeer, 1999). Thus, empowerment relates to expanding a woman’s ability to make “strategic life choices” where this ability had been previously denied (Hansen et al., 2020; Kabeer, 1999; Kabir & Khan, 2019). The ability to exercise these choices is dependent on three factors, that is, agency, resources, and achievement (Kabeer, 2001). We also make the assumption that, if IPV operates at the individual, relational, and societal levels, then empowerment at these levels might as well be protective.
Method
To examine the relationship between women’s empowerment and emotional IPV, we used data from the ZDHS, a cross-sectional survey on a range of indicators on population, health, nutrition, and domestic violence. Using the 2011 population census as a sampling frame and a two-stage cluster sampling technique stratified by rural and urban residence, roughly 11,000 households were sampled from the country’s 10 provinces. Further details on the sampling methods for the ZDHS are provided in Zimbabwe National Statistics Agency and ICF International (2016).
For this analysis, we used the couples’ file and extracted 3,499 records of ever-partnered women. We excluded 533 women who were not currently partnered as they were not asked the domestic violence questions. From the remaining sample of 2,966, 140 (representing 4.7% of the sample) women had missing information on our independent variable. As a missing rate of 5% or less is considered inconsequential (Schafer, 1999), we used the listwise deletion approach in our analysis.
Variables
Outcome Variable
Our primary outcome variable was emotional IPV. The women in the ZDHS were asked whether their husband or partner had done the following: (a) humiliated them in front of others, (b) threatened with harm, or (c) insulted them. Using the schema recommended by Maiuro (2001) and adopted by other researchers (e.g., Follingstad, 2009; Villa, 2014), we opted to broaden our definition of emotional IPV to include the full range of nonphysical behaviors that potentially lead to “degradation of the self, which lowers worth and interferes with human development and productivity” (Mills, 1999, p. 553). Thus, we also included the following behaviors: whether the husband or partner (d) was jealous if respondent talks with other men, (e) accused the respondent of unfaithfulness, (f) did not permit respondent to meet female friends, (g) limited respondent’s contact with her own family, and (h) insisted on knowing the whereabouts of the respondent. These behaviors are classified as controlling behaviors in the ZDHS.
We reclassified (a) and (c) as denigrating behavior, (b) as threatening, and (d) to (h) as coercive behaviors. If a woman responded yes to any of these questions, they were coded as having experienced that dimension of emotional IPV. Thus, our outcome variables (denigrating, threatening, and coercive behaviors) were binary (0 = no, 1 = yes). We also constructed a composite dichotomous dependent variable: any emotional IPV equal to 1 if a woman ever experienced denigrating, threatening, and coercive behaviors, and 0 otherwise.
Prevalence of Emotional Violence
Figure 1 presents the profile of emotional IPV among Zimbabwean women.
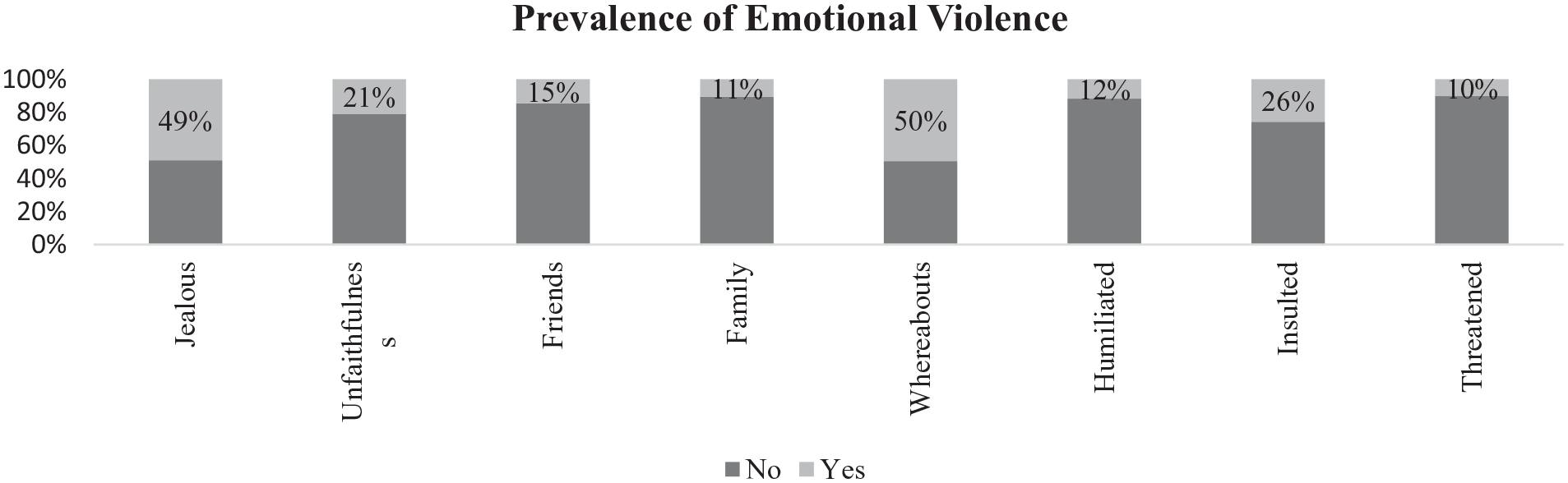
Prevalence of emotional violence.
Acts of jealousy (49%) and demanding to know one’s whereabouts (50%) were the most prevalent forms of emotional IPV. This was followed by acts of insulting (26%) and accusations of unfaithfulness (21%), while threatening behavior (10%) was the least common dimension of emotional IPV.
Women Empowerment
Our main explanatory variable was women empowerment. This variable was derived from 19 questions, as shown in Table 1. The options in italics were considered as the empowered categories. Drawing on Kabeer’s typology of empowerment as agency, resources, and achievements (Kabeer, 2001), we use the following indicators in our women empowerment variable. We considered a woman’s educational and literacy attainment (achievement) and economic independence (resources, that is, ownership of land, house, and earnings) as forms of personal empowerment. At the same time, the ability to negotiate and make decisions (agency) within the relationship was operationalized as relational forms of empowerment.
Empowerment Indicators.

Source. Derived from 2015 ZDHS data set.
Note. STI = sexually transmitted infection; ZDHS = Zimbabwe Demographic and Health Survey.
We included joint ownership of property and joint decision-making as forms of empowerment for various reasons. First, Zimbabwe’s patrilineal nature dictates that although wives may benefit from the family wealth, they may not claim ownership, even when they have contributed to the family’s wealth (Chitakure, 2016). Therefore, we see the ability to negotiate joint ownership as not only a direct challenge to this social norm but also evidence of empowerment. Second, decision-making in the patriarchal Zimbabwean society is the privilege of men (Bengesai & Khan, 2020). As such, women’s involvement in decision-making is a sign of their improved status and suggest better spousal understanding (Dalal et al., 2014).
Given our premise that IPV is a manifestation of unequal gender relations, we see the acceptance of acts that perpetuate this status quo as indicative of the status of women in any society (Sardinha & Nájera Catalán, 2018). Therefore, we also included attitudes that support wife-beating as a measure of women (dis)empowerment. We hypothesize that a combination of these forms of empowerment can potentially decrease the risk of IPV, including emotional IPV.
To determine whether our selected variables can explain women empowerment, we first used principal component analysis (PCA). We used the proportion of variance rule (Wilcox, 2012) to determine whether to retain the variables in our analysis (Table 2).
Empowerment Variable Loadings.
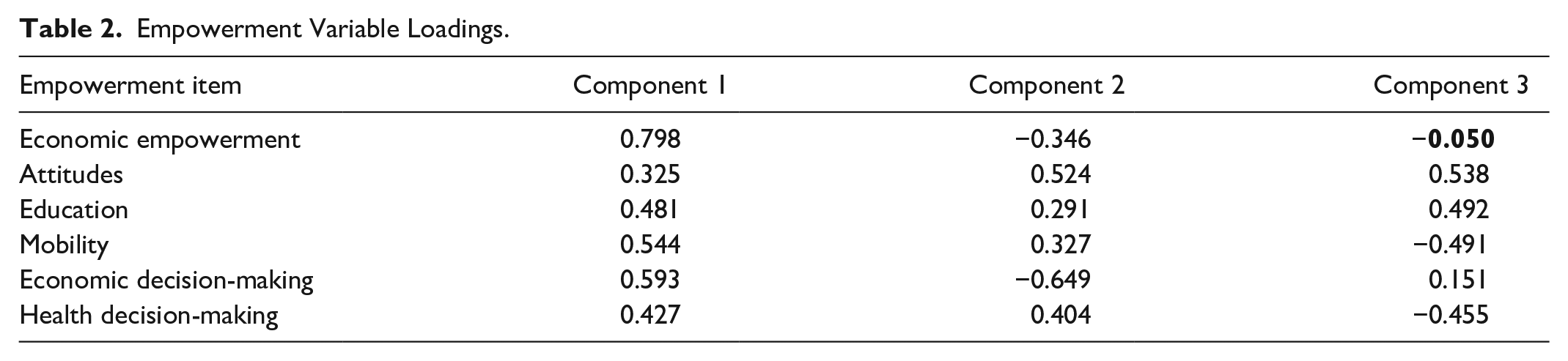
Almost all of our variables loaded with sufficient magnitude on the three components (above 0.1; Wilcox, 2012), except for economic empowerment (value in bold), which had a weak loading on the third component. The PCA analysis also revealed that the first three variables explained 66% of the variance.
After determining that our selected variables had sufficient interpretive value, we then applied the k-means clustering algorithm (Figure 2), an unsupervised classification approach that finds statistically similar groups in a data set (Hartigan & Wong, 1979). Given the variability in the data, we first applied z scores (Mohamad & Usman, 2013) to standardize all the empowerment variables so that they would have a common scale. This involved subtracting the mean of each of the variables and then dividing it by its standard deviation. Thus, each variable had a mean of 0 and a variance of 1. Although we set the k-means algorithm to run in 25 iterations, convergence was reached after the seventh iteration. For each iteration, the algorithm determined “the centroid coordinates, the distance of each object from the centre and grouping objects based on minimum distance” (Mohamad & Usman, 2013, p. 3299).

Empowerment cluster membership.
The average distance from the centroid was lowest for Cluster 2 (2.145), followed by Cluster 3 (2.794) and highest for Cluster 1 (3.377). This suggests that Cluster 1 had the least variability and Cluster 3 had the most variability. However, Cluster 1 also had the least observations (426), whereas Cluster 2 (1,143) and Cluster 3 (1,257) had more observations. This perhaps explains the difference in variability. Nonetheless, the analysis of variance (ANOVA) test results indicated that the three clusters were significantly different (p < .001).
Figure 2 shows that all the variables loaded negatively for the women in Cluster 1, suggesting that these women had low levels of empowerment in all domains, with freedom of movement and economic decision-making being the lowest among all the three clusters. We consider this group to be the “least empowered.” In the second cluster, all the variables loaded positively, suggesting that women in this cluster were empowered across all domains, with economic empowerment and economic decision-making being the highest. We refer to this group as the “most empowered.” The final cluster consisted of women who had high freedom of movement and some health decision-making power. These women also had very low economic empowerment and economic decision-making power. This group is referred to as the “less empowered.”
Other Covariates: Relationship Characteristics
Spousal age difference
To create this variable, we subtracted the woman’s actual age from that of her husband/partner. A negative score indicated that the wife was older than the husband, whereas 0 indicated no age difference between the woman and her husband or partner. We reasoned that the age difference would result in an imbalance of power, where the older husband or partner was more likely to wield more control over the wife, and the wider the gap, the more control the husband/partner would have. Following the literature on age-disparate relationships (Beauclair & Delva, 2013), we categorized spousal age difference as follows: 1 = 0–4 years, 2 = 5–9 years, 3 = 10 years and above, and 4 = wife older.
Age at marriage
The effect of age at marriage on IPV is likely to be positive or negative. Women who marry early, especially before their 18th birthday, are more likely to be at risk of IPV than those who marry later. Thus, we categorized this variable (1 = ≤17, 2 = 18–21, 3 = 22+) such that it would tease out the effect of child marriage (before 18th birthday) on emotional IPV.
Other Covariates: Sociodemographic Covariates
We also included sociodemographic covariates, namely, age, religion, residence, and wealth quintile, which were categorized as follows: age (1 = 15–24 years, 2 = 25–34 years, 3 = 35–49 years), religion (1 = Christian, 2 = other, 3 = Apostolic), residence (1 = urban, 2 = rural), and wealth quintile (1 = poor, 2 = middle, 3 = rich).
Analytical Method
We employed three levels of analysis. The first level involved running the cluster analysis classification for the empowerment variable (Figure 2). This was followed by the descriptive statistics on the association between explanatory variables and our outcome variables (Table 3). Finally, we conducted binary logistic regression (Tables 3 and 4) because the dependent variables were binomial. All analyses were conducted using the SPSS V. 27.
Descriptive Statistics of IPV and Cluster Membership (ZDHS, n = 2,826).

Note. IPV = intimate partner violence; ZDHS = Zimbabwe Demographic and Health Survey.
p < .10. **p < .05. ***p < .005.
Odds Ratios From Logistic Regression Analysis of the Association Between Emotional IPV and Women Empowerment, ZDHS, 2015.

Note. IPV = intimate partner violence; ZDHS = Zimbabwe Demographic and Health Survey; OR = odds ratio; CI = confidence interval.
p < .10. **p < .05. ***p < .005.
Table 3 presents descriptive statistics on the association between women empowerment clusters and the experience of IPV. The results show that 29.1% of women in the less empowered cluster, 27.2% in the most empowered cluster, and 35.4% in the least empowered cluster had experienced denigrating behavior from their husbands or partners. Approximately 9.8%, 9.7%, and 13.6% of less empowered, most empowered, and least empowered women had experienced threatening behaviors, respectively. The most common form of emotional IPV was controlling behaviors experienced by 61.7% of the less empowered, 66.8% of most empowered, and 69.0% of least empowered women. Again, 65.6%, 71.2%, and 72.8% of less empowered, most empowered, and least empowered women had experienced some form of emotional IPV from their husbands or partners, respectively. For the most part, most of our controls were significantly associated with emotional IPV and mainly threatening and coercive behaviors.
Results
Descriptive Statistics
Logistic regression
Table 3 presents the unadjusted models for the four emotional IPV variables, whereas Table 4 presents the adjusted odds ratio (aOR) models that included all the covariates identified in this study.
Denigrating behavior
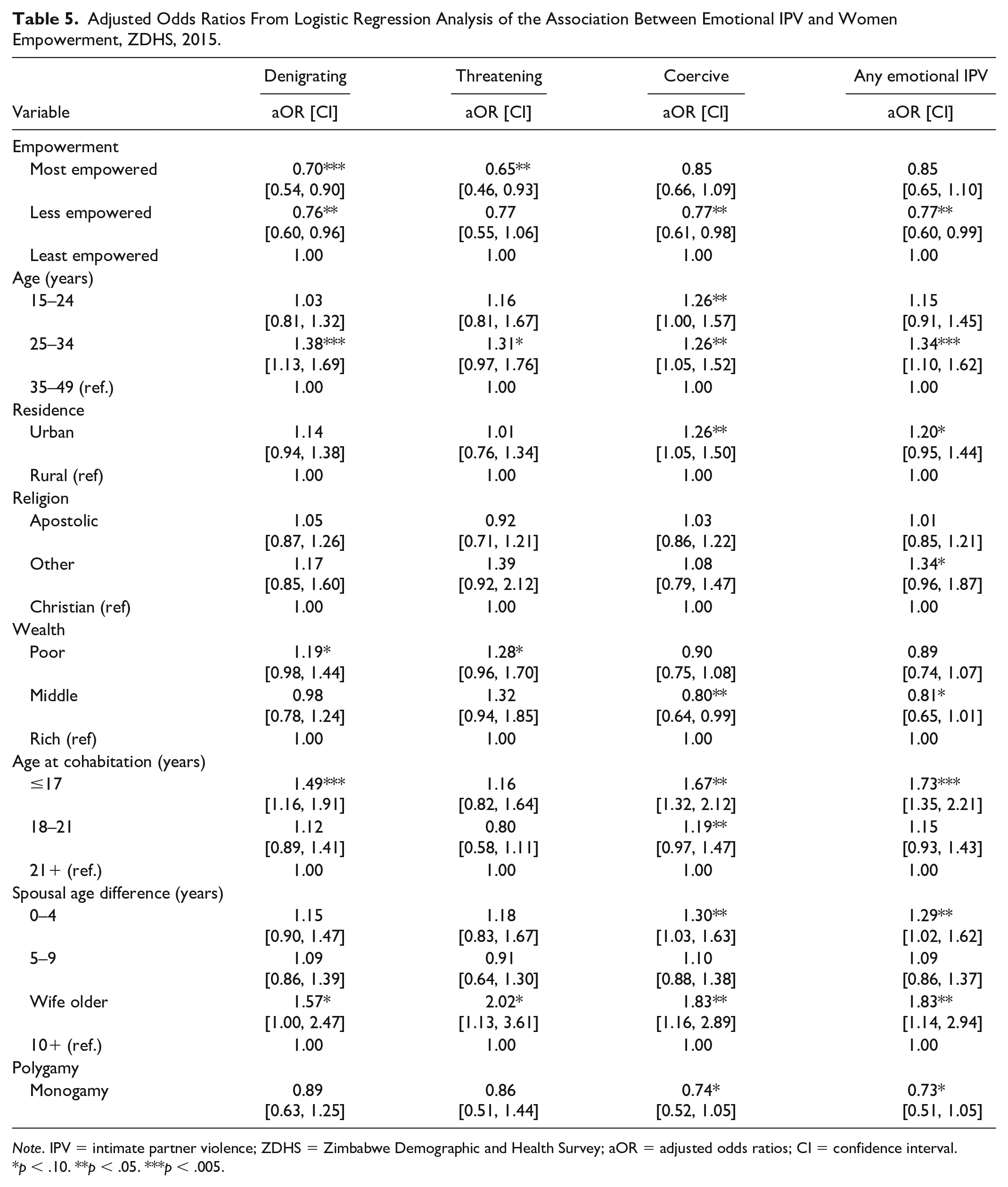
Women who were classified as most empowered and less empowered (Tables 4 and 5) were less likely to experience denigrating behavior in both the unadjusted and adjusted models (odds ratio [OR] = 0.68, aOR = 0.76). Women aged 25 to 34 years (aOR = 1.38), who were from the poor wealth quintile (aOR = 1.19), were married before the 18th birthday (aOR = 1.49), or were older than their husbands (aOR = 1.57) were more likely to be at risk of denigrating behavior (Table 5).
Adjusted Odds Ratios From Logistic Regression Analysis of the Association Between Emotional IPV and Women Empowerment, ZDHS, 2015.
Note. IPV = intimate partner violence; ZDHS = Zimbabwe Demographic and Health Survey; aOR = adjusted odds ratios; CI = confidence interval.
p < .10. **p < .05. ***p < .005.
Threatening behavior
Women classified as most empowered were less likely to be at risk of being threatened in both the unadjusted (OR = 0.63; Table 3) and adjusted models (aOR = 0.65; Table 4). Women who were aged 25 to 34 years (aOR = 1.31), were poor (aOR = 1.28), or older than the husband or partner (aOR = 2.02) had a higher probability of experiencing threatening behavior (Table 4).
Coercive behavior
The less empowered women were 24% (unadjusted; Table 3) and 23% (adjusted; Table 4) less likely to experience controlling behaviors from their partners or husbands, respectively. Factors that increased the likelihood of women experiencing controlling behavior include ages 15 to 24 years and 25 to 34 years (aOR = 1.26), marriage before the 18th birthday (aOR = 1.67), ages 18 to 21 years (aOR = 1.19), age difference 0 to 4 years (aOR = 1.30), and wife older (aOR = 1.83). Being in a monogamous marriage or belonging to the middle wealth quintile reduced the risk of experiencing coercive behavior by 26% and 20%, respectively.
Any emotional IPV
Less empowered women were up to 24% less likely to experience any form of emotional IPV (Table 3). Factors that increased the risk of emotional IPV include (Table 4) ages 25 to 34 years (aOR = 1.34), urban residence (aOR = 1.20), religion category “other” (aOR = 1.34), marriage before the 18th birthday (aOR = .73), and spousal age difference of 0 to 4 years (aOR = 1.29), wife older (aOR = 1.83). Belonging to the middle wealth quintile reduced the risk of any emotional IPV (aOR = 0.81), while being in a monogamous marriage also reduced the risk (aOR = 0.73).
Discussion and Conclusion
Emotional violence is one of the most prevalent forms of IPV. Although its impact is undeniably severe, affecting an individual’s self-esteem, agency, and autonomy (Karakurt & Silver, 2013; McLaughlin et al., 2012), it is often the least researched form of IPV (Gibbs et al., 2018). This study examined the association between women empowerment and emotional violence, using cluster analysis and logistic regression. Drawing from literature, we considered educational attainment and literacy, economic independence (ownership of properties and cash earnings), attitudes toward wife beating, and bargaining power relating to health, freedom of movement, and household purchases as proxies for women empowerment (Dalal, 2011; Hansen et al., 2020; Kabeer, 1999).
Our analysis revealed three empowerment clusters. The first cluster, which we refer to as the least empowered, was characterized by very low levels of empowerment across all domains, with freedom of movement and economic decision-making power being the lowest. The second cluster, which we classified as the most empowered, was characterized by high economic independence and economic decision-making levels, whereas the third cluster had low levels of economic independence and economic decision-making power but with a high level of mobility. From a theoretical perspective (Hansen et al., 2020; Kabir & Khan, 2019), women in the most empowered cluster had individual and relational empowerment, while those in Cluster 3 (less empowered) had more relational empowerment. Thus, our findings suggest that women empowerment in Zimbabwe is characterized mainly by economic independence (resources), household bargaining power, and freedom of movement (agency).
In contrast, educational attainment (achievement), health decision-making, and attitudes toward gender-based violence (societal empowerment) had expected but relatively weak empowerment effects. However, given that education is an investment that improves the economic worth of an individual (Stromquist, 2002; Unterhalter & North, 2011), we assume that this effect would have been picked up in the classification of the economic independence variable in our cluster analysis. It is also possible that Zimbabwe’s fragile economic landscape, characterized by high unemployment, closure of companies, retrenchments, and poverty, has minimized the effect of education as a form of empowerment (Mlambo, 2013). Although poverty can generally be catalytic in attaining increased education, it is likely that the high levels of unemployment among university graduates (Mutambara et al., 2018) has forced some young people in Zimbabwe to be reluctant to enroll for postsecondary education in favor of self-employment.
Our findings also point to the multidimensionality of women empowerment (Bayissa et al., 2018; Kabeer, 2019; Shimamoto & Gipson, 2015), often difficult to capture using traditional methods of measuring empowerment. In other words, our findings from cluster analysis reveal that one might have significant empowerment in one dimension, such as mobility, yet less empowered in another, such as economic independence. Hence, there is a need to consider approaches that tease out this complexity when examining the connection between empowerment and IPV.
In terms of IPV, our results suggest that emotional IPV is a persistent issue in Zimbabwe. Overall, up to 69% of the women experienced some form of emotional IPV, with the least empowered women being the most affected. The results contrast with the findings of prior studies, which found a prevalence of 25% to 30% IPV (Bengesai & Khan, 2020; Wekwete et al., 2014). However, these studies used a narrow definition of emotional IPV. We also found that controlling behaviors were the most common form of emotional violence experienced by up to 65% of the women, followed by denigrating and threatening behaviors, in that order. Previous research profiling victims of IPV has shown that emotional IPV might just be as detrimental as physical IPV, if not worse (Antai, 2011; Dokkedahl et al., 2019; Karakurt & Silver, 2013). Indeed, most victims of physical IPV have been subjected to long periods of intimidation, isolation, and control extending before the physical attack (Stark, 1995). As a result, there is a need for research that seeks to understand the role of emotional violence as a separate construct of IPV, worthy of its own theories and prevention strategies (Karakurt & Silver, 2013).
Contrary to studies that have shown that women empowerment can potentially increase IPV (Oduro et al., 2015; Panda & Agarwal, 2005), including emotional violence, our results from the logistic regression suggest that this might not be the case in Zimbabwe, as we found a positive association. In particular, our findings show that women who were economically empowered, including in economic decision-making, were less likely to experience denigrating or threatening behaviors. Those with high levels of mobility were also less likely to be victims of denigrating and coercive behaviors or composite emotional IPV. Although similar findings have been reported in other countries (see Dalal, 2011; Sabarwal et al., 2014; Tu & Lou, 2017), direct comparisons cannot be made, given the variations in context, methodologies, and the conceptualization of both emotional IPV and women empowerment. For instance, most studies that have included emotional IPV (e.g., Bengesai & Khan, 2020; Wekwete et al., 2014) did not include controlling behaviors, while women empowerment has been measured using domains and statistical methods different from our study (Dalal, 2011; Kabir & Khan, 2019).
Nonetheless, our results suggest that economic empowerment and the freedom of movement might be protective from emotional IPV, at least in the Zimbabwean context. In a patriarchal society, freedom of movement is a sign of trust. It suggests that men are not suspicious of their wife’s or partner’s motives for wanting to go out (Samuels et al., 2017). Hence, it comes as no surprise that women who were highly empowered in this dimension were also less likely to be victims of controlling behaviors from their husbands or partners.
The unequal education opportunities that have been afforded to boys and girls in Zimbabwe, especially in pursuing postsecondary education, have resulted in many women being economically dependent on their husbands (Chitakure, 2016). Some people call economically dependent women “broilers” or “home defenders” (Chitakure, 2016), denigrating terms that suggest they just stay at home waiting to be provided for by the husband. On the contrary, economic independence is seen as attractive, given that it increases outside options for a woman. As a result, husbands of financially independent women often feel challenged to ensure that the woman’s happiness in the marriage remains above her outside options (Heath, 2012). Economic independence is highly valued such that when a woman leaves her husband and still makes it in life (Chitakure, 2016), it is seen as a direct challenge to the husband, which can subject him to ridicule as someone who could not keep his wife.
In terms of our covariates, women aged 15 to 24 years and 25 to 34 years reported experiencing the most emotional abuse, relative to those aged 35 to 49 years. However, this effect was, for the most part, not significant for the former category. We assume that the insignificant results were due to the possible correlation with our age at marriage variable; thus, some of the effects of the age category 15 to 24 years might have been picked up in the age at first marriage variable. Nevertheless, the finding is consistent with other studies, showing that older age can be protective against IPV (Issahaku, 2017; Rivara et al., 2009; Shamu et al., 2018).
The increased risk of emotional IPV among younger women relative to those aged 35 years and above could be linked to several factors. For instance, it has been suggested that younger women are likely to lack both social and economic power and conflict management skills, which might act as stressors in the relationship while limiting their ability to negotiate the power dynamics in a marital relationship (Eisikovits, Band-Winterstein, 2015). If this is the case, there might be a need for intervention studies that target younger people (both male and female) with IPV prevention and conflict management skills (Shamu et al., 2018). These have been tried in other countries and found to be effective (Gibbs et al., 2018). Another factor might be the intersection between gender inequality and age. In a patriarchal country such as Zimbabwe, age often comes with power and greater status (Issahaku, 2017), especially when the woman has been married for long and has sons of marriageable age (Chitakure, 2016). These women often become the next generation of patriarchal mothers, enforcing gender norms on their new daughters-in-law.
The risk of experiencing both denigrating and coercive behaviors was common among women who were married as children, that is, before their 18th birthday. This finding was expected as a large body of research has shown that child marriage is a risk factor for IPV in general (Kidman et al., 2015; Nasrullah et al., 2015; Yount et al., 2016). In fact, child marriage in itself is a form of violence (Yount et al., 2016) and a human rights violation that has been perpetuated by forced marriage practices such as kuzvarira (virgin pledge) and chimutsamapfiwa (replacement bride) in Zimbabwe (Chitakure, 2016). Given that child brides do not have any input into whom they are marrying, it is most likely that this lack of familiarity with their future partners creates conflict in the marriage (Kidman et al., 2015). In addition, child brides are generally socially and economically vulnerable; hence, they do not have much bargaining power, limiting their ability to challenge any form of IPV (Marphatia et al., 2017).
Polygamous marriages have been shown to be risk factors for all forms of IPV (Ashimi & Amole, 2015). This is comparable to our findings that revealed that women who were in a monogamous marriage were less likely to experience both coercive behaviors and our composite emotional IPV variable, although this effect was marginal, while no association was found with denigrating or threatening behaviors. Similarly, we found marginal effects of place of residence and religion (“other”) on our composite emotional IPV variable. However, women who lived in urban areas had a lesser likelihood of experiencing controlling behaviors. This is likely because social norms which justify male dominance and abusive behaviors are more normalized and rationalized in traditional contexts such as rural areas (Chitakure, 2016). For instance, it is common among older women in rural areas to advise women that violence or acts of jealousy signal love, thus, framing these abusive behaviors as positive cultural traits (Makahamadze et al., 2012). However, urban women who might have more access to mass media and social networks are likely to hold liberal norms and recognize such behaviors as abusive (Bucheli & Rossi, 2019; Kishor & Johnson, 2005).
The association between wealth status and emotional violence also varied according to the IPV dimension. Women from the poor wealth quintile were less likely to experience denigrating and threatening behaviors although this effect was marginal. In contrast, those from the middle wealth quintile had a lower risk of experiencing the controlling behaviors and any emotional IPV relative to women from the rich quintile. These findings were somewhat surprising as we had expected wealth status to be protective (Gautam & Jeong, 2019). However, they seem to concur with Pambè et al.’s study, which reported that women from the wealthiest quintile were most likely to be at risk of psychological abuse (Pambè et al., 2013). Most importantly, the finding suggests that improving household wealth alone might not be adequate in eliminating emotional IPV. Instead, a comprehensive approach that takes into consideration relational and personal empowerment factors might be more effective.
The finding that a spousal age discrepancy of 0 to 4 years and where the wife was older elevated the risk of IPV was rather unexpected and inconsistent with theories of hegemonic masculinity and our expectations of age-heterogamous relationships (Adebowale, 2018). We had anticipated that, when the age gap is wider, the men would most likely be controlling, resulting in a power imbalance, whereas non-disparate relationships would be more protective (Adebowale, 2018). However, these results seem to align with the study conducted by Jewkes et al. (2002), which found that having an intimate partner at least 5 years older was protective against IPV.
Perhaps the most interesting finding regarding spousal age difference is that the risk of all forms of emotional IPV increases significantly for women who were older than their partners. In Zimbabwean society, wife older unions are considered taboo (Manyonganise, 2015). Women who are older than their husbands or partners are often called all sorts of derogatory names, the most typical being “chembere” (old lady; Manyonganise, 2015), even when the spousal age difference is as narrow as 1 or 2 years. Such negativity is likely to make its way into the relationship, leading to tension. For instance, during marital conflict, the husband might repeat the demeaning words used by society in a way to silence the woman (Chitakure, 2016). Again, when the age gap is wider, conflict can also arise when the husband wants children and the older woman does not. Such differences in opinion are also likely to deepen the conflict and the possibility of emotional IPV (Lehrer, 1996).
Limitations
This study is not without limitations. Of concern is the potential endogeneity between women empowerment and IPV in general, which could be due to omitted variables, simultaneity, or selection bias. However, the methods used in this study did not control for this sort of bias; hence, the results should not be interpreted as causal relationships. Second, the experience of emotional IPV was drawn from self-reported data. Thus, there is the possibility of both over- and underreporting of IPV.
Conclusion and Recommendations
These limitations notwithstanding, our study has shown that emotional violence is still prevalent in Zimbabwe, affecting a significant proportion of women. Moreover, women empowerment has been shown to be protective against emotional IPV. In this regard, our study has potentially valuable implications for stakeholders, such as policy makers, development partners, social workers, and other parties interested in reducing IPV in general. Given that emotional violence is often a precursor of physical forms of violence, there is a need for interventions that can help decrease its occurrence. This can be done through promoting economic empowerment, which has been shown to be protective in this study. In the Zimbabwean context, economic empowerment might increase the respect that a woman has in her home, thus reducing the likelihood of being called names and experiencing other forms of abuse. Most importantly, interventions meant to eliminate emotional IPV must adopt a comprehensive approach that focuses on strengthening both personal and relational dimensions of empowerment while addressing unequal gender relations that remain the root cause of all IPV forms.
Footnotes
Acknowledgements
The authors would like to thank the Zimbabwe Demographic and Health Survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study uses secondary data which are already in the public domain. However, permission to use these data was granted by the Demographic and Health Survey Program.