
Abstract
The current study includes Urdu translation and validation of Borderline Personality Features Scale–11 (BPFS-11) in two phases. Phase 1 included forward and back translation of BPFS-11, and Phase 2 included establishment of psychometric properties for BPFS-11. For this purpose, 930 adolescents were selected from different hospitals, schools, and colleges. The reliability value of the scale was .72. Exploratory factor analysis revealed factor structure with four principal dimensions; besides confirmatory factor analysis, goodness-of-fit indices indicated good fit of model to data, and two dimensions of scale and factors showed good values of internal consistency. The obtained value for goodness-of-fit index was .995, for adjusted goodness-of-fit index was .989, for comparative fit index was .998, for incremental fit index was .998, and for root mean square error of approximation (RMSEA) value was .019. Good values of composite reliability and convergent validity were measured for both dimensions of the scale. The analysis of criterion-related validity showed significant positive correlation of BPFS-11 with Affective Lability Scale, Deliberate Self-Harm Inventory, and neuroticism scale of Big Five Inventory. Significant differences were found between scores of individuals having borderline personality disorder and scores of normal individuals. The results of the current study indicated that BPFS-11 is short and easily administered diagnostic tool that has good psychometric properties and can be helpful for diagnosis of borderline personality features in adolescents. It can enhance the understanding of the participants regarding the statements of the scale for Urdu natives.
Keywords
Borderline personality disorder (BPD) is a psychiatric state that is associated with dysregulation of emotions, bad temper, fear of rejection, feelings of worthlessness, self-harm, and unstable relationships with others. It is common in both psychiatric population and in the general community (Brune, 2016). BPD is an emotionally unstable personality disorder, and patients with this disorder mostly have difficulty in the management of problems (Winston, 2018).
The prevalence of BPD is increasing day by day. Some non-clinical surveys of general population of the United States estimated that the prevalence of BPD is 1.6% and lifetime prevalence is 5.9%. The ratio of females to males with the disorder is greater in clinical populations than it is in general population. The ratio is 3:1 in clinical settings; however, lifetime prevalence of BPD does not differ significantly between men and women (Skodol, 2019). A study conducted in Iran concluded that the prevalence rate of BPD in adolescents is 0.9% (Mohammadi et al., 2014).
In Pakistan, prevalence rate of BPD is also increasing. A study conducted on 3,500 individuals from different cities of Pakistan concluded that the prevalence rate is 18% for BPD. The study also concluded that the adolescents between 13 and 19 years of age and young adults between 20 and 29 years of age had significantly higher tendencies toward mental disorders (Hussain, 2018).
Pakistan is a developing country and faces a lot of problems related to health, education, employment, poverty, availability of resources, and political instability. All these problems lead to negative mental states, which in turn may lead to psychological disturbances. In a study, Hasan et al. (2011) selected all registered cases of 2003–2009; there are 2.22% cases that were diagnosed on Axis II (personality disorders). Out of these, 18.18% were diagnosed as BPD. Availability of reliable and valid tools to measure personality disorders is very less. Urdu is a national language of Pakistan, as well as largely spoken language in many Indian states. It is a widely spoken language in South Asia; besides South Asia, Urdu is a spoken language of many emigrants and their children who are working in Middle East region, Australia, the United Kingdom, and other European countries. So, it is very difficult for less educated or uneducated individuals to understand questions in English.
Unfortunately, none of the diagnostic tool is available in Urdu. So, there is a need to translate a scale in Urdu that can be easily administered on educated, uneducated, and less educated persons, belonging to rural or urban areas of Pakistan. The current study translated the Borderline Personality Features Scale–11 (BPFS-11) in Urdu to make it applicable for Pakistani population and population of other countries who can understand Urdu but cannot understand English.
The BPFS-11 is a short version of original Borderline Personality Features Scale for Children (BPFS-C; Crick et al., 2005). BPFS-C is a 24-item scale that is widely used measure to diagnose borderline personality characteristics in children above 9 years as well as in adolescents. It has four subscales: Negative Relationships, Affective Instability, Self-Harm, and Identity Problems. BPFS-C was translated and validated in different languages; Lui and Wang (2019) translated and validated this scale in Chinese language, and concluded that BPFS-C was a reliable and valid measure to assess borderline personality features in Chinese children and adolescents. The BPFS-11 includes 11 items that were selected from BPFS-C by using item response theory methods. It includes items related to all four factors of BPFS-C, but there was not enough support for these factors in BPFS-11. So, it is a unidimensional scale, with scoring criteria of 5-point Likert-type scale, ranging from not at all true to always true (Sharp et al., 2014). Other researchers translated and validated both BPFS-C and BPFS-11 original English scales in Portuguese language, and concluded that both scales are reliable and valid measures to diagnose borderline personality features in adolescents (Carreiras et al., 2020). The Italian version of the Borderline Personality Features Scale for Children–11 (BPFSC-11) was tested on a community sample and presented adequate internal consistency, and confirmatory factor analysis (CFA) supported a bifactor model with all items significantly loading on a general factor with two specific factors (Fossati et al., 2019). Another study conducted by Haltigan and Vaillancourt (2016) on Canadian adolescents between 13 and 16 years had made efforts to confirm the four-factor model of BPFS-C, but was not successful, but EFA (exploratory factor analysis) and CFA of the study provided support to two-factor models of BPFS-C, intra-/interpersonal preoccupation and impulsivity/reactivity.
The items of BPFS-11 are related to four subscales: Affective Instability, Self-Harm, Identity Problems, and Negative Relationships. Affective instability is quick variations or fluctuations of severe affect, having difficulty in regulation of these variations and their behavioral consequences (Marwaha et al., 2014). Affective instability in BPD is due to a marked reactivity to environmental events. Affective instability is a crucial part of impulsive personality functioning (Herpertz et al., 1997). Self-harm is to perform behaviors that provide injury to own self. These behaviors may or may not include suicidal attempts. It is any type of self-injury (Muehlenkamp et al., 2012). Self-harming behaviors are common in adolescents and young adults, and adolescents involved in self-harming behaviors are at a greater risk of suicide (Sanchez-Teruel et al., 2020). BPD often involves in a number of disruptive behaviors, such as self-destructive actions, impulsivity, and suicidal ideations. So, they are at a considerable risk of providing harm to their selves and others if they are left unmanaged (Shaikh et al., 2017). Self-harm behaviors are part of impulsivity; impulsivity can cause harm to yourself and those around you (Salters-Pedneault, 2020). So, in a broad sense, both of these factors (affective instability and self-harm) are closely related to or part of impulsivity/reactivity factor of BPD.
Identity is related to sense of self and individuality, which depends on social recognition. There are a number of identity problems such as identity crisis and identity diffusion. All these problems depend on self-evaluation and evaluation of others (Sollberger, 2013). Several symptoms in interpersonal domain of BPD are actually manifestations of intrapersonal difficulties (e.g., difficulty being alone and misperception of the intentions of others as wicked), and identity problems are part of intra-/interpersonal preoccupation (Ramarajan, 2014; Stanley & Siever, 2010).
Negative relationships are hostile relationships with others and based on disagreement or rivalry behaviors with others (Easley & Kleinberg, 2010). Disturbance in interpersonal relationship is the main characteristic of BPD. Gunderson et al. (1996) found that two interpersonal criteria, avoidance of abandonment and unstable relationships, differentiated borderline from other personality disorders; disturbances in interpersonal relationship are part of intra- and interpersonal preoccupation; and this domain is unique part of BPD (Siever & Weinstein, 2009). So, in general, both of these factors, identity problems and negative relationships, are part of intra-/interpersonal factor of BPD.
Somma et al. (2016) used BPFS-11 on Italian adolescents and concluded that it is an excellent screening instrument to measure borderline personality features in adolescents, and it showed positive correlation with Deliberate Self-Harm Inventory (DSHI) and Difficulties in Emotion Regulation Scale.
The current study has made an attempt to translate and validate the BPFS-11 into Urdu language and to establish the psychometric properties of BPFS-11 in Pakistani culture. Research instruments in Urdu have a great value in Pakistan as well as in neighboring countries, and for conducting research on South Asian population who are working in European countries or in any area where majority Urdu speakers live in. So, the current study aimed to translate and validate the BPFS-11 in Urdu, according to Pakistani culture for Urdu speakers, especially for those who are unable to understand the scale in English. As it is a national language of Pakistan, for Pakistani population (especially for children and adolescents), it is easy to understand the scale in Urdu.
The current study has three main aims: first is to translate and adapt the BPFS-11 in Urdu, second is factor analysis of the translated and adapted BPFS-11 on indigenous population, and third is to validate BPFS-11 to establish psychometric properties of scale and to measure concurrent and construct validity of scale.
Method
The current study was conducted in two phases. Phase 1 includes translation of BPFS-11 in Urdu and Phase 2 includes establishment of psychometric properties of scale. To examine the factors of BPFS-11, CFA was used. The scores of BPFS-11 were correlated with scores of Affective Lability Scale (ALS), DSHI and neuroticism (NEU) scale by using correlation. As disturbances in affective components and emotional regulation are basic characteristics of BPD, ALS was selected to check criterion-related validity of BPFS-11. Similarly, individuals with BPD also attempt self-harming behaviors, and because self-harm is a characteristic of BPD, deliberate self-ham inventory was selected to check criterion-related validity of BPFS-11. Both of these scales were also used to check criterion-related validity of BPFS-11 original English scale (Sharp et al., 2014). As borderline personality has positive association with NEU personality trait (Furnham & Crump, 2014), NEU scale was used for measuring related validity of BPFS-11. Independent t test was used to compare the scores of borderline patients with scores of normal adolescents.
Measures
In the present study, the following measures were used.
BPFS-11
BPFS-11 was developed by Sharp et al. (2014). It is a short version of BPFS-C (Crick et al., 2005). It includes 11 items, with scoring criteria of 5-point Likert-type scale, ranging from 1 = not at all true to 5 = always true. Higher scores indicate high level of borderline personality features. Cutoff point is 34; adolescents having scores higher than 34 are considered as having features of BPD and adolescents having scores less than 34 are considered as normal.
ALS
It was developed by Oliver and Simons (2004). ALS has 18 items. Scoring criteria is a 4-point Likert-type scale, ranging from 0 = very uncharacteristic of me, to 3 = very characteristic of me. ALS yields total scores as well as scores on three subscales: Depression/Elation, Anger, and Anxiety/Depression. The higher scores indicate high affective lability.
DSHI
It was developed by Gratz (2001). It is a self-report measure that has 17 items; it measures presence and frequency of a range of self-harming actions. In the present study, the DSHI was used to evaluate the construct validity of Urdu translation of BPFSC-11. High scores on this scale show greater frequency of self-harming behaviors, whereas low scores show low frequency of self-harming behaviors.
Big Five Inventory (BFI)
It was developed by John et al. (1991). It has 44 items, and eight to 10 items are related to each trait. It has five subscales. In the current study, NEU subscale was used. NEU has eight items (4, 9, 14, 19, 24, 29, 34, and 39). Items 9, 24, and 34 are reverse-scoring items. Scoring criteria is a 5-point Likert-type scale, ranging from 1 = strongly disagree to 5 = strongly agree.
Phase 1: Translation of BPFS-11 in the Urdu Language
Translation of BPFS-11 was done, from the source (English) to target language (Urdu) with the assistance of six bilingual experts (three assistant professors, one professor, and two lecturers). They were requested to translate the scale word-by-word, so that meanings of words cannot change. The next step is a careful evaluation of all items by a committee of six experts in clinical psychology field (one associate professor, one assistant professor, and four lecturers). These experts deeply examined every item with respect to style, grammar, and word selection that seems closer to the original test. The next step was back translation of the scale by using the Brislin (1976) method. Two lecturers of Urdu, two lecturers of English, and one lecturer of psychology were requested to translate the Urdu items back into English. These lecturers did not have any idea or familiarity with the original English version scale of BPFS-11. Then these selected items were administered on a small sample of 20 adolescents with age ranging from 12 to 19 years. Results revealed that there is no ambiguity in scale items. All items are clear and logical, and they can be used for further analyses.
Phase 2: Psychometric Properties of BPFS-11
To determine the psychometric properties of Urdu translation of BPFS-11, Cronbach’s alpha was used for reliability analysis of scale. Analysis of Moment Structure (AMOS 20; CFAs) was used for evaluating construct validity of factors of BPFS-11. Correlation with ALS and DSHI was used to determine the convergent validity of BPFS-11. The scores of healthy adolescents were also compared with the scores of adolescents having borderline personality.
Sample
A sample of 1,600 adolescents was approached from different hospitals (diagnosed borderline patients), schools, and colleges and universities of Pakistan by using convenient sampling technique. Initially, participants who were seeking treatment for psychiatric illness were approached in different private- and public-sector hospitals of Pakistan. Written permission was obtained from relevant hospital authorities for data collection. Participants who gave written informed consent were included in the study. Similarly, in educational settings, participants were approached by obtaining written permission from relevant authorities and by taking written informed consent from participants. BPFS-11 was administered on all those participants. Based on the initial screening on BPFS-11, those 930 participants, who showed BPD symptoms, by obtaining greater scores than cutoff point on the scale, were short-listed for further assessment. Out of these 930 adolescents, 414 (44.5%) were boys and 516 (55.5%) were girls. The data of remaining 670 adolescents, who have low scores on the scale, were used as a comparison group to compare the scores of borderline patients with non-borderline adolescents.
Procedure
The prior approval for data collection was taken from relevant authorities (hospital in-charge and administration, school and college principals). Approval from the ethical committee has also obtained. Participants were residents of Pakistan. Subjects were approached, and written informed consent was obtained from them. Necessary instructions were given to the subjects to complete the questionnaires as honestly and completely as possible. In hospital settings, subjects were approached in out-patient departments (OPDs) and psychiatry wards, and BPFS-11 was administered on diagnosed borderline patients within the age range of 12 to 19 years. In educational settings, BPFS-11 was administered on students within age range of 12 to 19 years, both girls and boys. All the participants who have obtained scores greater than cutoff point of BPFS-11 were selected for final analyses. Participants who have obtained scores less than cutoff point of BPFS-11 were used as comparison group, to compare their results with the results of those adolescents who have borderline personality features.
Out of the selected adolescents who have greater than cutoff scores on BPFS-11, 200 adolescents (100 boys [50%] and 100 girls [50%]) were requested to fill the BPFS-11 in both languages, Urdu translated scale and original English scale, to find out correlation between both scales. Other 200 adolescents (100 boys [50%] and 100 girls [50%]) were requested to fill the ALS along with BPFS-11, next 200 (100 boys [50%] and 100 girls [50%]) were requested to fill the NEU subscale of BFI along with BPFS-11, and other 200 (100 boys [50%] and 100 girls [50%]) adolescents were requested to fill the DSHI along with BPFS-11. All the additional scales were administered in English language because all of the subjects can understand both Urdu and English language easily.
After completion of the data, all participants were thanked to take part in research. Some of the data were discarded because of incomplete questionnaires.
Data Analyses
After collection of data, appropriate statistical analyses were applied for data analyses. EFA in SPSS-20 was used for factor structure and principal dimensions of the scale. CFA in AMOS-22 was used to evaluate the factors of BPFS-11. The Pearson product–moment correlation coefficient was used for measuring correlation among all scales; t test was used for measuring differences between the scores of adolescents with borderline personality features and adolescents without borderline personality features.
Results
The results of the present study are as follows.
Reliability of BPFS-11
The reliability analysis of BPFS-11 was conducted. BPFS-11 showed satisfactory levels of reliability. The alpha value for total scale was .72. For Factor 1, alpha value was .79, and for Factor 2, alpha value was .82.
Correlation analysis indicated that BPFS-11 Urdu translation has a significant positive correlation with BPFS-11 original English scale at .01 level of significance, so both Urdu translation and English version are significantly correlated with each other.
Validation of BPFS-11
EFA was used for factor structure and principal dimensions of the scale. CFA was used to evaluate the factors of BPFS-11. CFA is a widely used method of factor analysis. Based on the primary criteria, all the observed factors had acceptable standardized regression values, that is, greater than .35 (Field, 2009). Thus, in the present study, the factor loadings of CFA for the two dimensions of BPFS-11 were above .35. For comprehensive analysis, the graphic representation of factors is given below:
Figure 1 showed the factor models of two dimensions of BPFS-11. All the values are greater than .35, which is an acceptable criterion for standardized regression value.
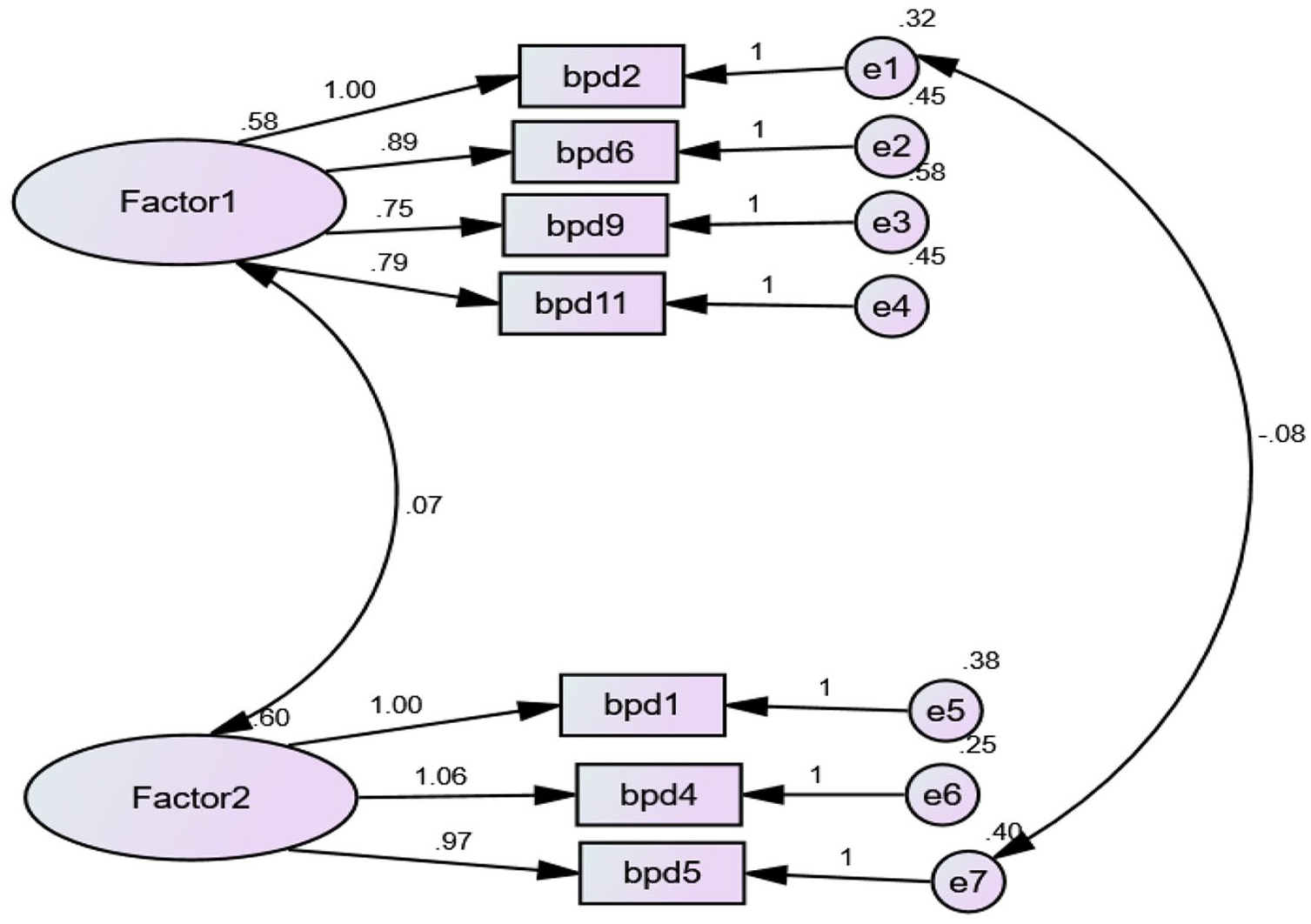
Graphical presentation of two dimensions of BPFS-11.
Table 1 indicated demographic characteristics of sample with respect to age, gender, education and monthly family income alongwith their frequency and percentage.
Demographic Characteristics of Sample With Borderline Personality Features (N = 930).

Table 2 showed extraction value of all items of BPFS-11 and showed that all of the 11 items have satisfactory value and can be used to measure borderline personality features.
Communalities Values of Extraction Method by using Principal Components Analysis of BPFS-11 (N = 930).

Note. BPFS-11 = Borderline Personality Features Scale–11.
Table 3 showed factor loading value of two factors of BPFS-11 Urdu translation.
Factor Loading for Exploratory Factor Analysis by Using Varimax Rotation Analysis of BPFS-11 (N = 930).

Note. BPFS-11 = Borderline Personality Features Scale–11.
Table 4 showed CFA for goodness-of-fit index (GFI) for two subscales of BPFS-11. The acceptable values for GFI (goodness-of-fit index), AGFI (adjusted goodness-of-fit index), CFI (comparative fit index), and IFI (incremental fit index) are .90 or greater and the current study obtained values between .995 and .998. So, the current study has significant findings.
Model Fit Indices for BPFS-11 (N = 930).

Note. BPFS-11 = Borderline Personality Features Scale–11; GFI = goodness-of-fit index; AGFI = adjusted goodness-of-fit index; CFI = comparative fit index; IFI = incremental fit index; RMSEA = root mean square error of approximation.
Table 5 indicated satisfactory values of Cronbach’s alpha, composite reliability, and convergent validity of two factors of BPFS-11.
The CFA Reliability and Validity Results for Final Model of BPFS-11 (N = 930).
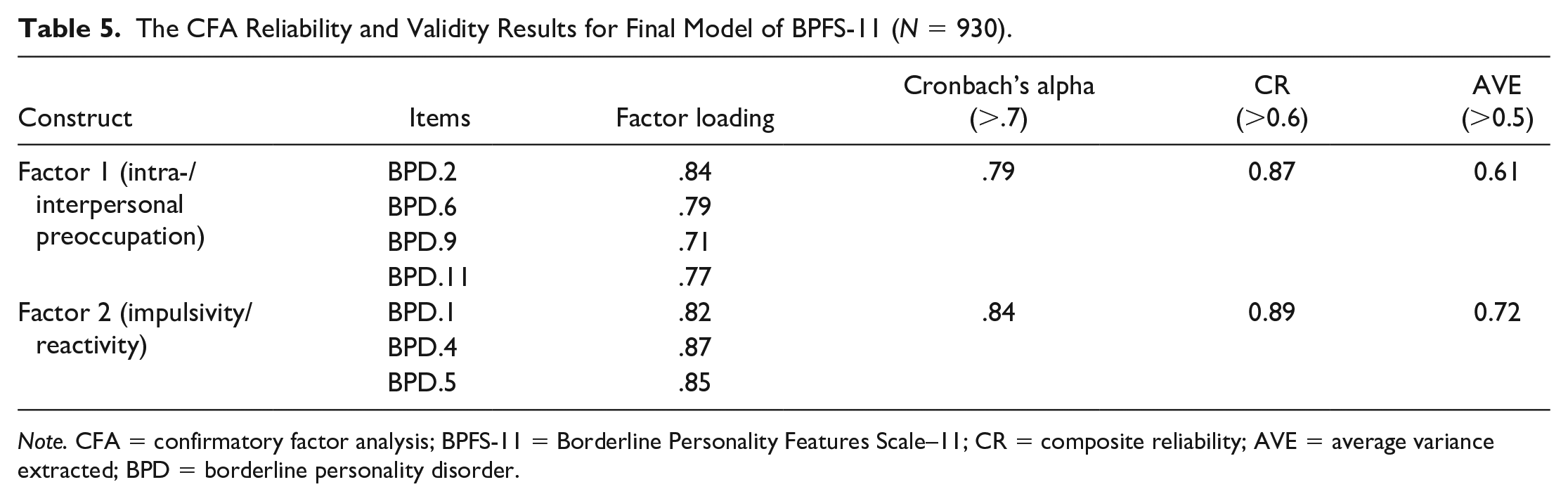
Note. CFA = confirmatory factor analysis; BPFS-11 = Borderline Personality Features Scale–11; CR = composite reliability; AVE = average variance extracted; BPD = borderline personality disorder.
Table 6 shows that BPFS-11 has significant positive correlation with DSHI, ALS, and NEU scale.
Correlation Among BPFS-11, DSHI, AFL, and NEU Scale (N = 600).

Note. BPFS-11 = Borderline Personality Features Scale–11; DSHI = Deliberate Self-Harm Inventory; ALS = Affective Lability Scale; NEU = neuroticism.
p < .05. **p < .01.
Table 7 shows that all subscales of BPFS-11 have significant positive correlation with DSHI, ALS, and NEU scale.
Correlation Among Subscales of BPFS-11, DSHI, AFL, and NEU Scale (N = 600).
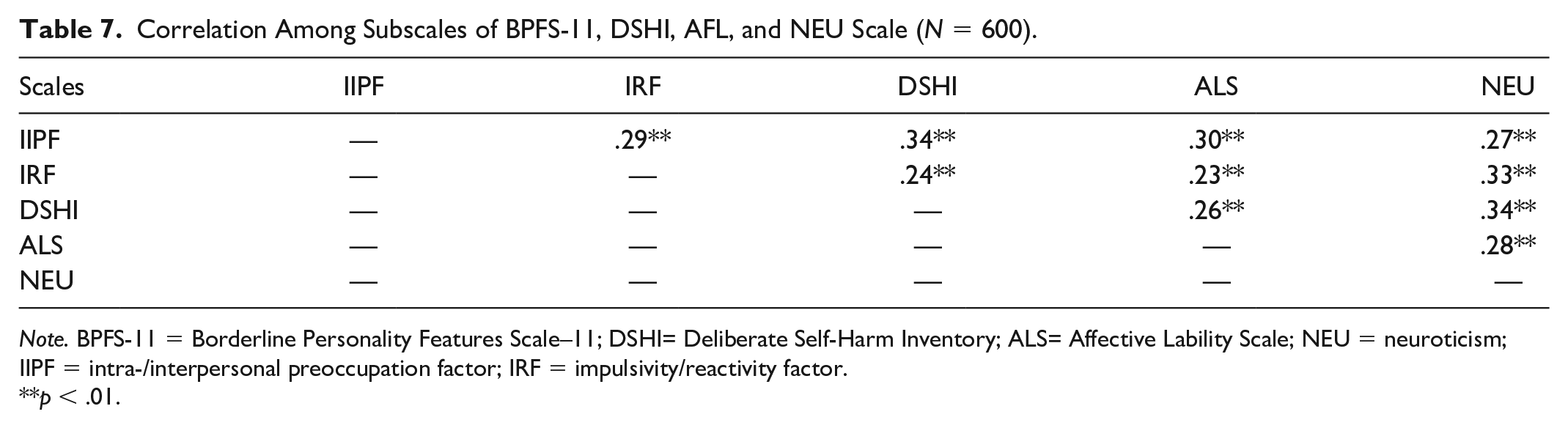
Note. BPFS-11 = Borderline Personality Features Scale–11; DSHI= Deliberate Self-Harm Inventory; ALS= Affective Lability Scale; NEU = neuroticism; IIPF = intra-/interpersonal preoccupation factor; IRF = impulsivity/reactivity factor.
p < .01.
Table 8 indicated comparison between healthy and non-healthy individuals on BPFS-11 and its subscales. The comparison was made between the two groups, 300 healthy adults and 300 diagnosed with BPD. The analysis of independent t test indicated significant differences between the scores of healthy individuals and borderline patients on BPFS-11 and both of its subscales. The value of Cohen’s d indicated differences between the mean scores of two groups on BPFS-11 and its subscales.
Comparison Between the Scores of Adolescents With Borderline Personality Features and Adolescents Without Borderline Personality Features on BPFS-11 and Its Subscales.

Note. BPFS-11 = Borderline Personality Features Scale–11; CI = confidence interval; LL = lower limit; UL = upper limit; IIPF = intra-/interpersonal preoccupation factor; IRF = impulsivity/reactivity factor.
Table 9 indicated significant gender differences on BPFS. It indicated that borderline personality features are greater in females as compared to males. The value of Cohen’s d indicated differences between the mean scores of two groups on BPFS-11.
Gender Differences on BPFS.

Note. BPFS = Borderline Personality Features Scale; CI = confidence interval; LL = lower limit; UL = upper limit.
Discussion
The current study was conducted to translate and validate the BPFS-11 in Urdu. Results showed satisfactory level of reliability (.72). Results of EFA indicated a factor structure with four principal dimensions. CFA was used to analyze the factors, which showed good level of model fit indices for two factors of BPFS-11. The reliability values for two subscales were .79 and .84, respectively. Both factors of BPFS-11 showed good values for composite reliability and convergent validity. The estimated composite reliability for Factor A was .87, and the estimated value for convergent validity of Factor A was .61. Similarly, the calculated value of composite reliability for Factor B was .84, and calculated value of convergent validity for Factor B was .89. BPFS-11 and its two dimensions showed good construct validity as all the items have significant positive correlation with total scores. Both dimensions of BPFS-11 showed satisfactory level of goodness-of-fit indices. The value of χ2 was 16.03; χ2/df value was 1.336, which is less than its accepted standardized value, that is, χ2/df value should be less than 3. Concerning the chi-square test, the value of χ2/df = 1 is considered as perfect; value of χ2/df that is fewer than 2 is considered as good value; if obtained value is lesser than 5, it is taken as acceptable value and if the obtained value is 5 or more, it is considered as an unacceptable value, this value of χ2/df is related to the size of the sample (Marques et al., 2014). Similarly, the obtained value for GFI was .995, for AGFI .989, for CFI .998, for IFI .998, for TLI (Tucker–Lewis index) .997, and for NFI (normed fit index) .993. All of these values are greater than .90, which is a standardized criterion value. According to Schumacher and Lomax (2010), these values range from 0 to 1, values near 1 indicate perfect fitting of the model. Values from .90 to .95 range or above show good model fit (Hair et al., 2006). The obtained value for root mean square error of approximation (RMSEA) was .019, which is less than .05 that is the accepted standardized value of RMSEA, this value should be less than .08 for acceptable model fit and for a good model fit this value should be less than .05. In the present study, the obtained value of RMSEA was .019, which shows good model fit of the scale. A good characteristic of RMSEA is that it provides 95% or 90% assurance that model is in the acceptable fit range (Hu & Bentler, 1999).
So, the BPFS-11 and its two dimensions indicated very good values on all three levels of model fit indices, that is, AGFI, IFI, and parsimonious fit. The analysis showed that Urdu translated scale of BPFS-11 has a significant positive correlation with its original scale, that is, BPFS-11 original English version. For measuring criterion-related validity of BPFS-11, three scales—ALS, DSHI, and NEU—were used for correlation with BPFS-11 as well as with its subscales. The results indicated significant positive correlation of all subscales of BPFS-11 with ALS, DSHI, and NEU. These results are supported by some of the previous studies. A study concluded high positive correlation between self-harm inventory and borderline personality (Sansone et al., 1998). Some other studies also concluded positive relationship between non-suicidal self-harming behaviors and BPD (Brickman et al., 2014; Sleuwaegen et al., 2017).
Similarly, BPD has high positive correlation with ALS (Reich et al., 2014). Some recent studies found significant positive correlation between affective lability and BPD (Carpenter & Trull, 2013; Schoenleber et al., 2016).
Similarly, some other recent studies concluded strong positive correlation between BPD and NEU (Few et al., 2016; Saldanha-silva et al., 2019).
Discriminant validity of BPFS-11 was estimated by comparison of scores of normal adolescents and adolescents having borderline personality features. Findings indicated significant differences between scores of healthy individuals and borderline patients on BPFS-11, as well as significant differences between scores of healthy individuals and borderline patients were concluded on both dimensions of the scale.
As a result, Urdu translation of BPFS-11 was found to be a reliable and valid measure for the assessment of borderline personality features in adolescents.
Limitations and Suggestions
The present study has taken ALS, DSHI, and NEU for correlation with BPFS-11; it is suggested that future research should include any opposite construct for correlation, to determine the divergent validity of the scale.
Conclusion and Implications
It was concluded that Urdu translation of BPFS-11 is a reliable and valid tool for diagnosing borderline personality features in adolescents. The results of CFA indicated multidimensionality of the scale. BPFS-11 would be very helpful for clinical psychologists and psychiatrists to diagnose borderline features in adolescents. The correlation with ALS, DSHI, and NEU also provides great contributions in the literature. It was concluded that BPFS-11 is a short, concise, and easily administered scale that has good and satisfactory psychometric properties. It can enhance the development of patient’s strength and enhance self-worth.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Prior ethical approval from heads of institutes has been taken for data collection.
Inform Consent
Written informed consent has been taken from all participants to know about their willingness to participate in the study.