
Abstract
This study was conducted to assess the impact of health belief model based educational intervention on knowledge, health beliefs, preventive behaviors, and biochemical levels of women about osteoporosis. The study was design as a population-based and randomized experimental study by pretest and posttest design between July 2014 and July 2015. The sample (N = 1,792) of women were aged 18 to 49 years, who resided in Cubuk, Ankara, Turkey, and 75 women (nintervention = 45; ncontrol = 30) with a high risk of osteoporosis constituted the intervention group of the study. The questionnaires on osteoporosis knowledge and health beliefs were given to the participants before the intervention, immediately after the intervention, and repeated 3, 6, and 12 months. Women in the intervention group had received education and consultation, while those in the control group had not. Bone mineral density and clinical outcomes measured at the lumbar spine and femur before, immediately after the intervention, and 12 months after the intervention to measured osteo-protective performance. The average age of the women in the study was 33.49 ± 9.8 (min = 18, max = 49) years. After the intervention, a significant increase was found in the intervention group’ knowledge and health beliefs scores (p < .05). Sunlight exposure and physical activity increased (p < .05) but the levels of the bone mineral density (BMD), ionized Ca and 25 (OH) vitamin D, calcium intake, and smoking did not change after the intervention (p. > .05). This study showed that the health belief model based educational intervention had a positive effect on increasing knowledge, beliefs, and risk reduction behaviors to prevent osteoporosis.
Introduction
Osteoporosis is a global health issue that increases the fragility of the bone as a result of low bone mass density and deterioration of the micro architectural particularly of the hip, spine, wrist, and shoulder (Kanis, 2008; Shuler et al., 2012). Osteoporosis decreases the life quality of the individuals in physical, social, psychological, and economical aspects increasing the risk for mortality and morbidity. Osteoporosis affects more than 75 million people worldwide and causes more than 8.9 million fractures annually, resulting in an osteoporotic fracture every 3 s. By 2020, osteoporosis-related fractures will rise to approximately $19 billion in costs (National Osteoporosis Foundation, 2008). Women’s lighter, thinner bones and longer life spans are some of the reasons why they are a key target group in preventive intervention for osteoporotic fractures. They start losing bone at a younger age (about 10 years earlier) and at a faster rate than men. Women are also four times more likely than men to develop osteoporosis and two times more likely to have osteopenia compared to men. The risk for osteoporosis-related fracture is 50% for women after the age of 50 (especially during the first 5 years after menopause), while this rate is 20% for men (Hernlund et al., 2013; Tuzun et al., 2012). As silent, preventable and modifiable in nature, women need to be aware of the risk of osteoporosis and engage early counseling strategies from adolescence to premenopausal prior to an irreversible period of declining bone mass. In Turkey, there are no specific statistics about the prevalence of osteoporosis among women. In previous studies, the level of osteoporosis was 27% to 33% for women after the age of 50 (Gemalmaz et al., 2007; Kayacan, 2011; Keskin et al., 2014; Pinar et al., 2017; Tuzun et al., 2012).
The World Health Organization (WHO) indicates that risk factors for osteoporosis include age, sex, long-term glucocorticoid use, secondary osteoporosis, genetics, prior fragility fracture, low body mass index (BMI), smoking, excess alcohol consumption, sedentary lifestyle, having a diet lacking calcium and Vitamin D, nulliparous, late menarche, and early menopause (Jeihooni et al., 2015; Khoshnood et al., 2015; Stetzer, 2011). Acquisition of peak bone mass around the mid-20s for men and women, then it begins to decline around the age of 30, and the incidence increases steadily with age. Health belief model (HBM) is the most commonly used theory as evidence-based and cost-effective approach in educational intervention. Changing lifestyle or understanding the reasons for people’s osteo-protective behaviors depending on their individual and social factors is a complex situation. The HBM assumes that individual’s perceptions of their health plays an essential role in changing osteo-protective behaviors and reducing the risk of osteoporosis throughout their life span (Chahal et al., 2014; Dempster, 2011; Ghaffari et al., 2012; Jeihooni et al., 2015; Khoshnood et al., 2015; Malak & Toama, 2015; Stetzer, 2011; Wei et al., 2015; Zhang et al., 2012). We therefore decided to use this model with health promotion and education program (HPEP) in the present study. The HBM was developed in the early 1950s and updated in the 1980s, which is a conceptual framework used to understand health behavior and possible reasons for non-compliance with recommended health action (Becker, 1974; Champion, 1984). The underlying major components of the model; perceived susceptibility, perceived seriousness, perceived benefits, perceived barriers, self-efficacy, and motivation factors. In addition to health promotion movements initiated by the WHO Ottawa Charter in the mid-1980s, have become major pillars of health promotion reform worldwide and the WHO set a goal to increase the number of females trained regarding osteoporosis prevention. Several studies have also shown positive impacts of HBM on modifying health behaviors (Al-Otaibi, 2015; Edmonds et al., 2012; Elsabagh et al., 2015; Evenson & Sanders, 2016; Sanaeinasab et al., 2014). In our country, no studies were found that examined the effects of education program on knowledge, preventive behaviors, beliefs, and clinical outcomes of women aged 18 to 49 years old toward osteoporosis. The present study aimed to assess the effect of a program based on HPEP on the knowledge, beliefs, risk reduction behaviors, and clinical outcomes regarding osteoporosis among women aged 18 to 49 years.
Four hypotheses were developed to be tested at baseline, immediately, at 3 months, at 6 months, and at 12 months post intervention among women in this study: I: the Turkish women who engage in the HPEP will demonstrate higher levels of knowledge about risk factors and preventive measures of osteoporosis than those who do not engage, II: the Turkish women who engage in the HPEP will demonstrate stronger health beliefs regarding osteoporosis than those who do not engage, III: the Turkish women who engage in the HPEP will demonstrate higher levels of preventive behaviors in terms of osteoporosis than those who do not engage, and IV: the Turkish women who engage in the HPEP will affect clinical outcomes (bone mineral density [BMD], 25 [OH] vitamin D, ionized calcium (Ca) levels and dual-energy X-ray absorptiometry [DXA]) a year later than those who do not engage.
Method
Design and Participants
This rural population-based and prospective randomized-controlled interventional study was performed between July 2014 and July 2015. (Figure 1). The first stage includes field application of the research. In the field application content, all of the members living in that family and the women aged 18 to 49 were listed within the boundaries of Cubuk district in Ankara, Turkey (N = 17.641). Turkish Statistical Institute (TUIK) conducted a population and housing census, which was designed as a comprehensive sample survey based on administrative registers in 2013 (Turkish Statistical Institute, 2013). The sample size for the study was estimated using the formula (G*Power level at 0.80) for when the number of the individuals in the rural population was known. It was accepted as p = .30 (incidence of osteoporosis) and p = .70 (infrequency of osteoporosis). Standard deviation was calculated at ±2. Alpha errors were defined as 5% (n = 1,792). Household addresses were obtained from the TUIK. The data were collected in face-to-face interviews by researchers in accordance with the research criteria. Three visits were undertaken for each family, and in case the person to be interviewed was absent during the first visit, a date and time was appointed to visit her for the second time. If only one female lived in the household, that female was chosen for the interview. If two or more women lived in a household, the Kish selection method was used to select a female (age: 18–49 years) at random after excluding the household contact (Kish, 1994). The inclusion criteria for the sampling group were women aged 18 to 49 who voluntarily accepted to participate in the study. The exclusion criteria included any women who were postmenopause, already diagnosed with osteoporosis, lack of fractures, without any physical, cognitive disability, pregnant, rheumatoid disease, hyperparathyroidism, rickets, and osteomalacia. None of the participants were studying health sciences.

Study flow diagram.
In the second stage of the research, based on Osteoporosis Risk Estimation Scale (ORES), 123 women were accepted as high-risk for osteoporosis. These women were selected through purposive sampling method at the second part in the present study. The final sample size was 75 voluntary women (homogeneous with regard to socio-demographic characteristics), they were randomly assigned to either intervention (n = 45) or control groups (n = 30) by drawing lots.
Instruments
A total of four forms were used in the study consisting of (a) the Survey Form (SF), (b) ORES, (c) Osteoporosis Knowledge Test (OKT), and (d) Osteoporosis Health Belief Scale (OHBS). The HPEP-based HBM was also used to improve of women’s osteo-protective knowledge, belief, and behaviors in the study. All of the forms were found to be clear, and participants took an average of 20 min to complete. SF and the HPEP were prepared in compliance with the literature, and also five different opinions of experts were received in terms of the clarity, readability of the Turkish language, and accuracy of content. The content validity of the booklet was found to be 0.90. The reliability of the instrument was assessed using the internal consistency method. The overall Cronbach’s alpha was .94 for the OHBS and .82 for the ORES in the study. These questionnaires were pilot tested for applicability with 10 women who met the study admission criteria but were not residing in the study area. Then necessary modifications were done according to the results of pilot study and expert opinions.
The Survey Form-SF
This form consisted of 18 questions using a two part to identify socio-demographic history- SF I (such as age, BMI, education level, marital status, occupation, social security, number of pregnancy, source of information, history of other co-morbidities, and history of performing a BMD examination) and osteoporosis preventive and modifiable behaviors SF-2 (risk reduction behavior such as physical activity and consumption of calcium-rich foods, motivation performing health activities, and sunlight exposure) with combined close and open responses that were gathered from different literatures by the investigators (Al-Otaibi, 2015; Edmonds et al., 2012; Elsabagh et al., 2015; Evenson & Sanders, 2016; Sanaeinasab et al., 2014). In the classification of some of the questions on the SF, some activities like “walking a minimum of 3 times a week for at least 30 min, jogging, swimming, and doing sports” were considered as physical activity (National Osteoporosis Foundation, 2008). To obtain dairy products intake, women reported how many times per day they drank milk and ate cheese, yogurt, and ice-cream (cup/dish/glass/matchbox-size of one for seldom or never to two and over for several times). Those who benefit from sunlight in direct contact/exposure with the body in sunny weather are considered to be “benefiting from sunlight..” Other behavior changes assessed were smoking per day ranged from 6 to 30.
Osteoporosis Risk Estimation Scale—ORES
ORES was developed by Kayacan and accepted to be valid and reliable for the Turkish population in order to identify the osteoporosis risk in women. ORES includes 16 Likert type question. The total average score of the scale changes from 0 to 48. In the scale, no osteoporosis risks scores 0 to 14, low risk scores 15 to 28, medium risk scores 29 to 40, and high risk scores 41 to 48 (Kayacan, 2011). In this study, the Cronbach’s alpha of scale value was set at .82. The scale offers better resources to patients who are at higher risk for osteoporosis.
Osteoporosis Knowledge Test—OKT
The OKT was developed by Kim et al. in 1991 consists of 2 subscales and 24 items (16 items exercise and 8 items calcium intake subscale). Each item is rated by the subject using more likely, less likely, neutral, and don’t know. For the total instrument, there was only one correct answer for each question, and the maximum score for the OKT was 24 and the lowest was 0 (0–8 ranked poor, 8–12 ranked average, > 12 considered good). Kılıc and Erci (2010) developed this scale for the Turkish population, Cronbach’s alpha for OKT calcium was .75 and OKT exercise was .76. In this study, Cronbach’s alpha OKT calcium was .72 and OKT exercise was .75.
Osteoporosis Health Belief Scale-OHBS
OHBS that developed by Kim et al. (1991) and includes a 42-item consisting of 7 subscales (min: 42, max: 210). The subscales address susceptibility, seriousness, benefits of exercise, benefits of calcium intake, barriers to exercise, and barriers to calcium intake, self-efficacy, and health motivation. Each subscale consists of 6 items (min: 6, max: 30). Each item was rated by using a 5-point Likert-type scale with 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, and 5 = strongly agree. The OHBS was equal to five and a minimum total score was equal to one. For the five subscales, higher scores indicating extremely healthy beliefs, for the two subscales; concerning barriers, higher scores indicate more negative health beliefs. The high score indicates that the individual’s self-efficacy and self-care behaviors for protection from osteoporosis will be high. Kılıc and Erci (2010) developed this scale for the Turkish population. Cronbach’s alpha for total score was 0.94. In this study, Cronbach’s alpha was .88.
HBM-Based Health Promotion Education Program-HPEP
The purpose of the HBM-based HPEP programs is to promote early identification of risk factors and to encourage the adoption of risk-reducing behaviors in women from adolescence to premenopausal period to develop a healthy lifestyle. The booklet was also an instructional tool giving information on osteoporosis management by the researchers in the light of the literature on the subject. The content of the HBM based on education program was comprised of four components (perceived sensitivity, severity, benefits, barriers, a cue action, and self-efficacy practices); (a) orientation and introduction to the program, (b) general information about osteoporosis (include definition of osteoporosis, prevalence, and controllable risk factors; symptoms, complications, diagnosis, and treatment of osteoporosis), (c) preventive measures (including improving calcium intake through low fat food selections), and (d) initiating exercise activities. The duration of the HPEP is 2 hr of theoretical (presented via lecturing, question-and-answer, pamphlets, flow-charts, booklet, video, slides and discussion method) and 2 hr of practical (presented via show posters and demonstration of exercises techniques) education. The education program was planned face to face by researchers using small groups (approximately = 10 women), on two sessions. Within the framework of the HPEP, each woman in the intervention group was provided telephone counseling to start and continue osteo-protective behaviors after the education (follow-up at 3 months). It is worth noting that the educational materials were distributed to and discussed with the women in the control group after intervention, to meet the research ethics and to protect the rights of women in the control group.
Lab and Radiology Form
Classification of participants was based on the average T-value for the lumbar vertebral (anterior position between L1-4) and proximal femur (neck, trochanter and Ward’s triangle) using DXA (Hologic QDR-4500, USA). This is the gold-standard method for assessing BMD (WHO, 2003). The normal range of vitamin D 25(OH) is 10 to 55 ng/mL (National Osteoporosis Foundation, 2008). Ionized Ca test is a simple blood test to measure the level of free calcium, with a normal laboratory range between 4.8 and 5.2 mg/dL (between 1.2 and 1.3 mmol/L). When thinking of bone health, we look for high-ionized calcium as a possible indirect indicator of excessive parathyroid hormone activity. A low ionized calcium level might be related to low albumin and low protein status (Hernlund et al., 2013). Based on WHO criteria, individuals with a BMD value within 1 standard deviation of that for healthy young adults were classified as having normal bone mass (i.e., T-value > -1); those with BMD values 1 to 2.5 standard deviations below the mean value for healthy young adults were diagnosed as osteopenia (i.e., -1 > T > -2.5); those with BMD 2.5 or more standard deviations below the average value for healthy young adults (i.e., T < -2.5) were diagnosed with osteoporosis (WHO, 2003).
Application of the Research
The implementation steps of the study are presented in Figure 1.
First phase: Household interviews were carried out on 1,792 women and according to ORES, 123 (6.9%) were identified as having a high risk of osteoporosis in this group. Women in high-risk group were invited to the hospital by phone (n = 84 voluntary women). The researchers interviewed the illiterate subjects and answered their questions. Then, these women were referred to radiology center in the hospital and their bone density of L1 to L4 vertebrates and femoral neck was measured using DXA method (Hologic QDR-4500, USA). Also, all subjects were referred to the blood sampling unit to examine the 25 (OH) vitamin D and ionized Ca values. The densitometry data were collected according to the WHO t-score values, which is the gold-standard method for assessing BMD (WHO, 2003). Two days later, women were invited by the researchers to the hospital to learn about their results by telephone. A physical therapist at the research hospital evaluated blood and DXA results and 9 women were diagnosed with osteoporosis (for the lumbar vertebra). Those women who were diagnosed were excluded from the study and were directed to their treatment at the study hospital. The remaining 75 women (being osteoporosis free) were separated by simple random sampling method (n = 54 intervention; n = 30 control).
It was ensured that women lived in different neighborhoods to prevent the possibility of groups being affected. The participants were divided into five groups, for each group different timings were allocated (morning, afternoon, week day, or weekend) according to needs of the participants. After both groups filled the SF, OKT and OHBS were pretested. The HPEP was presented by the researchers in the training room of the hospital. The intervention included two educational sessions of 45 min, and it was completed in small groups in a week. Various training methods were used including lectures, group discussion, questions, and answers, demonstration, brainstorming, showing posters, short videos, and Power-Point displays. Moreover, osteoporosis booklet and pamphlets were distributed to the participants at the end of the last session. Immediately after training, the women in the intervention group were post\tested. No training was given to the women in the control group.
During the third month of the study, women in both groups were asked by telephone to inquire about the risk behaviors of osteoporosis and to investigate any changes. While no counseling was provided by the telephone to the control group, the women in the intervention group were counseled through telephone about what they would be careful about to protect themselves from osteoporosis; their questions were answered and their osteo-protective activities were motivated. Each counseling session lasted 10 to 15 min.
Second phase: Women also again attended educational sessions after the sixth month in the training room of the hospital so that the researchers could investigate any changes their activities, beliefs, and knowledge of osteoporosis. The intervention group was divided into small groups women (n = 10) and the training process was completed in 4 days face to face by researchers (presented via pamphlets, video, slides show, demonstration, and discussion method). In this context, three hospital staff members (1 physician therapist and 2 nurses) were trained again to raise awareness and ensure cooperation during research. To assess the effect of training intervention based on osteoporosis, the knowledge, beliefs, and practice of the participants were evaluated at the beginning of the study and 6 months later for the intervention group in face-to-face interviews by researchers.
Third phase: The average scores were calculated for all subjects to assess the effect of training on participants’ knowledge and beliefs before and after intervention. Scales were applied to the control group but no training intervention was done. Twelve months of the study were used in blood sampling, DXA, and using scales in each group; n = 28 in the intervention group and n = 28 women in the control group were completed.
Ethical Considerations
Written permissions were obtained from the Ethics Board of University for implementation of the study and from the hospital for research application. Furthermore, written consents were received from the women who accepted to participate in the study. Rules specified in the Helsinki Declaration were observed in the data collection phase. The women were free to withdraw from the study at any time without consequences.
Analysis of the Data
Analysis of the data was performed using SPSS 22.0 (Chicago, IL, USA). Descriptive statistical analyses were used (frequency, percentages, mean, and standard deviation). The differences in frequencies of categorical data between groups were tested by the Pearson Chi-square test and Fisher’s exact test. The Kolmogorov-Smirnov test was used to evaluate the variables containing and due to non-normality data, the Wilcoxon signed-rank test for within-group comparisons, and the Mann–Whitney U test for between-group comparisons. Multivariate repeated-measures analysis of variance (ANOVA) was applied to determine changes in the groups over time (pretest = T-0 before education; posttest-immediately after education = T-1; after education in 6 months = T-2; follow-up after 12 months = T-3) and interaction effects between time and group from pre–post test period with posthoc (Bonferroni) test. The significance level was set at p < .05.
Results
The average age of the women in the study was 33.49 ± 9.8 (min = 18, max = 49) years. Few women (18.0%) were in the 45 to 49 years old age group (intervention group: 36.76 ± 9.37, control group: 34.77 ± 9.10). A majority of the women were married (71.6%) and had given birth to children (64.0%), nearly 70.0% were housewives, 85.2% had social security, and 67.1% had middle incomes. The main source of information was media (63%), friends (24%), and health staff (13%). In both groups, socio-demographic and medical characteristics, lifestyle, and habits were similar (p > .05).
Very few women smoked (24.0%). The women seemed to be very active, with 67.4% indicating that they exercised at least once a week, and more than half (54.3%) more than twice a week. According to the self-reported intake of calcium, milk was the most popular diary product, with 49.6% of the participants indicating that they optimally consumed milk in two cups or more daily before the intervention. This percentage increased to 72.4% after the intervention. The results demonstrated that before the educational program 52.0% and 55.0% of the control and the intervention groups, respectively, had moderate knowledge, followed by 28.0% and 25.0% had little knowledge, then 13.0% and 15.0% had poor knowledge, and 9.0% and 11.0% had good knowledge. To give more detailed information, in preintervention stage, more than half of the control and the intervention group knew and answered correctly about advanced aging (68.0%; 71.0%), and low Ca intake (62.0%; 65.0%) as risk factors for osteoporosis. Controversially, 23.0% and 25.0% of the control and the intervention groups, respectively, knew and answered correctly about low exercise, lack of exposure to sunlight (22.0%; 16.0%), and smoking (24.0%; 20.0%, respectively). In postintervention stage, 70% to 90% of the women scoring correct responses were observed for risk factor items in the intervention group. The intervention group’s first month (immediately after the education) posttest OKT total score average (22.06 ± 2.07) was higher than the pretest (before the initial education) score average (16.22 ± 4.27) (p < .05). Similarly, it was determined that the sixth month posttest OKT total score average (23.07 ± 1.70) was higher than the pretest score average (20.93 ± 2.46) (p < .05).
The analysis of the mean points of the intervention and control groups in the OKT subgroup is presented in Table 1. The mean total score of the first month of the intervention group was 16.22 ± 4.27, while it was 15.30 ± 4.93 (p > .05) in the mean control group. The exercise knowledge score for the first month of the intervention group was 9.91 ± 3.45, while in the mean control group it was 9.33 ± 3.71 (p > .05). The calcium knowledge score at the first month of the intervention group was 11.93 ± 2.98, while in the mean control group it was 11.46 ± 3.64 (p > .05). The mean 6 months OKT total score of the intervention group was 20.96 ± 2.27, which was 14.82 ± 3.27 (p < .05) in the mean control group. The 12 months OKT total score average was 22.66 ± 1.69 and 15.95 ± 3.98 in the intervention and control group, respectively (p < .05). The results showed statistically greater increases in the intervention group’s T1, T2, and T3 for each subscale of OKT (p < .001).
Comparison of OKT Scores by Group.

Note. OKT = Osteoporosis Knowledge Test; p =* independent t test, p** = analysis of variance repeated measures; posthoc (Bonferroni) test.
The OHBS score averages of the intervention and control group evaluated at different times are given in Table 2. The results of the study showed that prior to the intervention, there was a good belief of perceived susceptibility, seriousness and health motivation of osteoporosis, followed by the benefits of calcium intake, but there was a low belief of perceived benefits to exercise and calcium intake in the two groups. When group comparisons examined in more detail; the mean total OHBS score for the first month was 138.33 ± 10.36 in the intervention group and 132.03 ± 11.24 in the control group (p > .05). The mean total OHBS score at 6 months was 153.36 ± 16.30 in the intervention group and 138.19 ± 13.55 in the control group (p < .05). Also, in the intervention and control group, the mean total OHBS score for the 12 months was 158.09 ± 17.07 and 138.74 ± 14.12, respectively (p < .05). According to ANOVA test after the intervention program (T1, T2, T3), the intervention group showed a significant increase compared to the control group in all OHBS and subscales (p < .001).
Comparison of OHBS Scores by Group.

Note.*p < .05, Analysis of variance repeated measures; Posthoc test, other p values = independent t test. OHBS: Osteoporosis Health Belief Scale.
There was no statistically significant difference (p > .05) between groups in terms of all elements of the OHBS at the first month of the education (p > .05). In the 6 and 12 months, the intervention group’s susceptibility, perception of seriousness, benefits of physical activity, and benefits of calcium intake were higher when compared with the OHBS subscales point average control group; barriers of physical activity of OHBS subscales were lower (p < .05). In addition, there was no statistically significant difference between the groups at 12 months (p > .05), while the health motivation of OHBS subscale at 6 months of study was higher in the intervention group (p < .05).
A comparison of the behaviors of the intervention and control group for prevention from osteoporosis, assessed at different times, is given in Table 3. There was no statistically significant difference in the physical activity habits of the intervention and control group at the 1 month (immediately after the intervention) of the study (p > .05). Compared with the results of 3, 6, and 12 months, the physical activity habits of the women in the intervention group were found to be higher (p < .05). At the 1-, 3-, and 6-months evaluations, there was no statistically significant difference in the sunlight exposure behaviors of both groups (p > .05). However, at 12 months, women in the intervention group were found to benefit more from sunlight compared to the control group (p < .05). In addition, it was determined that there was no statistically significant difference between the consumption of dairy products (Ca intake) and smoking habits of both groups evaluated at different times (p > .05).
Comparison of Behaviors of the Women for Prevention From Osteoporosis by Group.

1 and 6 months follow-up includes the pretest results. bp value < .05; χ2-kare test.
There was no statistically significant difference between the mean scores of ionized Ca and 25 (OH) vitamin D at 1 month and 12 months between the groups (p > .05). In the intervention group, the mean score of ionized Ca at 1month was 6.64 ± 0.37 mg/dL and in the control group was 6.58 ± 0.27 mg/dL. The mean ionized Ca level at 12 months was 8.39 ± 13.54 mg/dL and 4.75 ± 1.11 mg/dL, respectively (p > .05). In the intervention group, 25 (OH) vitamin D mean values were 7.00 ± 2.39 ng/mL in the control group, 6.60 ± 2.34 ng/mL in the control group, and 13.75 ± 6.98 ng/mL and 12.53 ± 5.92 ng/mL at the 12 months, respectively (p >.05) (Table 4).
Comparison of Women’ Lab Results by Group.
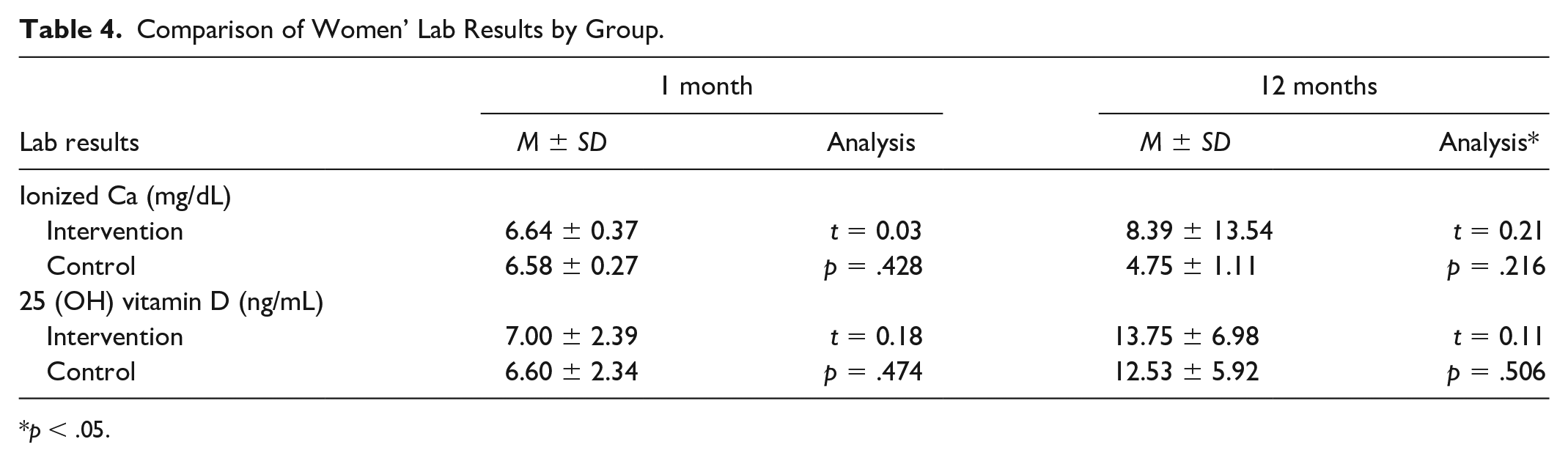
p < .05.
There was no statistically significant difference between the mean values of BMDFN and BMDLV at 1 month and 12 months (p > .05). The mean BMDFN value in the intervention group at the s month of the study was -0.56 ± 1.35 g/cm2 and in the control group it was -0.54 ± 1.00 g/cm2, at the 12 months evaluation 0.94 ± 1.55 g/cm2 and 0.48 ± 1.52 g/cm2, respectively, p > .05)). Mean BMDL2-4 value was -0.54 ± 1.33g/cm2 in the intervention group and -0.58 ± 1.03 gr/cm2 in the control group at the first month of the study. At the 12 months, it was -0.70 ± 1.32 g/cm2 and -0.43 ± 1.07 g/cm2, respectively (p > .05) (Table 5).
Comparison of DXA Results of Participants by Group.

Note. DXA = dual-energy X-ray absorptiometry, BMD = bone mineral density.
FN (femur neck), LV (lumbar vertebral).
Discussion
The findings of this study indicated that the HPEP was successful in increasing knowledge of osteoporosis (p < .05) (Table 1). Similarly, several studies have already been conducted on osteoporosis preventive interventions using this model, in most of which knowledge improved after the intervention (Abushaikha et al., 2009; Chan et al., 2007; El-Sayed & Abdel, 2013; Turner et al., 2004). In this study, a significant increase was seen in the women’ belief of perceived susceptibility to osteoporosis, perceived severity of osteoporosis, perceived benefits of exercise, and perceived benefits of calcium intake to prevent osteoporosis among the intervention group, besides it was seen that perceived barriers of calcium and perceived barriers of physical activity were low after the intervention (p < .05) (Table 2). In this study, the HPEP based on the HBM indicates that education was effective in changing the behaviors of women to reduce the risk for osteoporosis. This result was expected, so that the hypotheses of the research (I-II) have been proven. The results of our study were consistent with the previous studies (Drieling et al., 2011; Ghaffari et al., 2012; Kim et al., 1991; Ziccardi et al., 2004). Ziccardi et al. (2004) found perceived barriers including calcium intake and exercise behaviors were reduced by education. Drieling et al. (2011) reported that exercise barrier beliefs of the women in the intervention group were lower than those in the control group after education. Interestingly, Zhang et al. (2012) found that education could not change the physical activity and nutrition barriers, though the subjects were young.
Osteoporosis is not curable, and irreversible chronic disease once established. Thus, prevention is better than treatment. Fortunately, the risk of osteoporosis can be recognized and also potentially the onset of bone loss prevented or delayed with modifiable health behaviors such as cessation of smoking and reduction of alcohol consumption, adequate exercise, dietary calcium and vitamin D intake, and fall prevention (National Osteoporosis Foundation, 2008). Currently, health strategies for the prevention of osteoporosis as a cost-effective approach have gained more importance than treatment methods for dealing with this major public health problem. Identification of women with increased risk for osteoporosis and taking the required precautions is the most efficient way to decrease the load on the health system (Stetzer, 2011). Knowing the risks and providing education on bone health is the first step in the fight against osteoporosis. However, the comparable studies have focused mainly on the postmenopausal adult population whose bone losses had already started and not that of young and middle age individuals (Abushaikha et al., 2009; El-Sayed & Abdel, 2013; Sanaeinasab et al., 2014; Stetzer, 2011). Essentially, primary prevention program of osteoporosis should be initiated at early age (Ford et al., 2011; Keskin et al., 2014).
Modifiable lifestyle at an early age will have a greater impact on the prevention of osteoporosis, which include health education and promotion programs such as increasing calcium intake and physical activity should be emphasized for bone health maintenance (National Osteoporosis Foundation, 2008; Shuler et al., 2012). Several studies showed that the health behaviors of women about osteoporosis significantly increased after intervention (Al-Otaibi, 2015; Edmonds et al., 2012; Elsabagh et al., 2015; Evenson & Sanders, 2016; Ford et al., 2011; Turner et al., 2004). Despite this, some studies reported that high OKT score was not associated with osteoporosis health beliefs and preventive behaviors among women (Drieling et al., 2011; Ziccardi et al., 2004). According to Khoshnood et al. (2015) and El-Sayed and Abdel (2013), there is no significant change between groups for unhealthy behaviors (especially low calcium intake) after osteoporosis education. In a different study performed by Puttapitakpong et al. (2014), the women did not seem to have appropriate osteoporosis preventive behaviors. Similarly, in our study, there was no significant difference between health behaviors such as dairy products consumption and smoking in the intervention group who had a higher mean total score of OKT (p > .05) than those in the control group except for exercise and sunlight exposure (p < .05) (Table 3). It was found that ionized Ca and 25 (OH) vitamin D levels increased in parallel with HPEP for 12 months, but this increase was not statistically significant (p > .05) (Table 4). In addition, no statistically significant difference was found between the BMD of the women in the intervention and control group (p > .05) (Table 5). We found that developments in osteoporosis knowledge and beliefs did not fully translate into changes in osteoporosis preventing actions. Therefore, the hypotheses (III-V) have not been accepted. Our findings are consistent with the current studies (Gemalmaz et al., 2007; Khoshnood et al., 2015; Malak & Toama, 2015). Samia et al. (2018) conducted a study on 212 women in Malaysia to determine the effect of an HBM-based osteoporosis educational program, they reported that health motivation and perceived benefit for exercise and calcium intake was not significant for both groups at baseline and after intervention. Similar findings reported that there were no significant changes to be reached for osteo-protective behaviors in the mean scores obtained by the women in the intervention group compared with the control group for knowledge and all the HBM constructs 1 month after the educational intervention (Hala et al., 2015; Sharifikia et al., 2019). On the contrary, different studies indicated that high OKT and OHBS scores were positively associated with health behaviors for osteoporosis after training (El-Sayed & Abdel, 2013; Malak & Toama, 2015; Vahedian-Shahroodi et al., 2016). A study conducted by Jeihooni et al. (2015) on Iranian women (n = 120) showed that 6 months after the intervention, lumbar spine BMD T-score increased significantly to 0.127 ± 0.061 in the intervention group but reduced to -0.043 ± 0.059 in the control group. Kalkım and Dağhan also found positive effects of training on women’s health behaviors and lifestyle regarding osteoporosis (Kalkım & Dağhan, 2017). Ghaffari et al. (2012) conducted a study in Iran to determine the effect of HBM-based intervention on promoting calcium intake and regular exercise to prevent osteoporosis among women, which showed a significant increase in the mean score of perceived susceptibility, seriousness, benefits, and barriers among women in the experimental group; immediately before, immediately after, and 2 months after the intervention which is consistent with our findings. In the light of all these findings, it seems that additional interventions are required to study the impact of education on women’s cultural and economic aspects to carry out preventive behaviors.
Conclusion and Recommendations
As a result of the study, it was found that HBM-based HPEP provided information on increase of osteoporosis protection and positive beliefs (p < .05), but was not enough effect in altering some osteoporosis preventive behaviors, even though adaptive behavior change was observed (p > .05). This result should also be taken into consideration when developing strategies and prevention programs for osteoporosis. More importantly, health providers should focus more extensively on the health promotion and more high-quality research with comprehensive design. In conclusion, this program could be used as a model for promoting a healthy lifestyle to prevent osteoporosis.
Limitation and Strengths
The present study had both strengths and limitations. The result of the study may be generalized to the women recruited that represented a study hospital in Turkey. While our study determines the behavior of women to protect from themselves from osteoporosis, the use of their statements can be considered a limitation to the study. Strengths of the study include long-term (12 months) follow-up and interim monitoring, and consulting by phone or face-to-face interview after first education. Increased motivation has also been achieved with intermediate monitoring. The repetition of education is another strength of study and has been influential in the transformation of knowledge into some healthy behaviors and measurement levels of the BMD, ionized Ca, and 25 (OH) vitamin D. In addition to this, the experts in the field of the training provide this intervention with interactive training methods at an early age, and it is mainly given to the application of the strengths of the study. The findings may provide particularly useful references for future educational intervention in health organizations.
Footnotes
Acknowledgements
The authors would like to thank all their coworkers for their skillful contributions to the data collection and management in this study.
Author Contributions
G.P. and T.P. conceived the study, designed the study, conducted the statistical analysis, interpreted the data and wrote the manuscript. G.P. and T.P. approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by The Scientific and Technological Research Council of Turkey (TUBITAK) as project. The Project number was 113S277.