
Abstract
This study presents an emerging trend in medical tourism, cosmetic surgery tourism (CST). We explore tourists’ perceptions of CST for medical service quality as an antecedent to tourists’ emotional attachment, trust, and intentions to visit, which is underexplored in CST. This study examines the mediating role of value co-creation in influencing behaviors of CST-seeking tourists to experience a better quality of life. Using a sample drawn from 279 tourists, comprised of Australian, Japanese, and Chinese nationalities at two international airports in China, findings show that perceived medical service quality positively influences tourists’ emotional attachment, trust, and intentions to visit directly and through the mediating role of value co-creation across the three nationalities. CST-seeking tourists’ inputs in value co-creation may positively influence their behaviors, which are vital antecedents to promoting CST business. Implications for future research are discussed.
Keywords
Introduction
The notions of medical tourism, health, and well-being have gained academic attention due to their unprecedented growth. Yet, many of their emerging trends demand research attention, such as cosmetic surgery tourism (CST). Individuals are willingly crossing their national borders with hopes and financial resources to find a beautiful face and lose the fleshy body to improve their quality of life (Bell et al., 2011; Holliday et al., 2015; Viladrich & Baron-Faust, 2014). The willingness to travel and experience a surgical knife for beauty enhancement for overall health and well-being has given birth to CST in the recent era (Ackerman, 2010; Hallem & Barth, 2011; Miyagi et al., 2012). Tourists’ perceptions of medical tourism for health and well-being and behavioral intentions are complex to unravel (Majeed et al., 2018). Tourists’ perceptual complexities arise out of their sensitivity around exposing health and well-being needs at an offshore tourism destination.
Tourists expect valuable tourism experience; value is noted in terms of high quality of service (Oliver, 1997), and sometimes compared with price paid (Naumann, 1995; Rodríguez-Díaz & Espino-Rodríguez, 2017). In the medical tourism context, service quality is medical service quality and theoretical pieces point to it in terms of the services offered by doctors, nurses, paramedical staff, and the hospital or clinic where tourists are offered their desired health and well-being treatments (Majeed et al., 2018; Majeed & Lu, 2017). The service dominant logic theory presents the creation of service value with the resource integration of customers and service providers (Eletxigerra et al., 2018; Vargo & Lusch, 2016).
Value co-creation is defined as meeting customers’ expectations and perceptions alongside positively influencing their behaviors (Prebensen, Vittersø, & Dahl, 2013). Although value co-creation is gaining importance in tourism and hospitality (Chahthoth et al., 2013; Ramkissoon & Uysal, 2018), empirical research investigating the role of value co-creation in CST, where tourists and service providers both get better value for what they give, is yet underexplored. Value co-creation in tourism can generate unique values for tourists and service providers and demands more attention (Eletxigerra et al., 2018).
Tourists’ positive perceptions may determine their decision to visit a tourism destination (Ye et al., 2019). However, customers’ perceptions can further be linked to their behaviors around trust and emotional attachment (Rempel et al., 2001; Thi et al., 2002; Ye et al., 2019). Research investigating tourists’ perceptions of CST and the role of value co-creation in creating valuable CST experience and their decision-making to visit a CST destination is scant. There is a need to further explore the interplay of relationships between CST-seeking tourists’ emotional attachment, trust, and intentions to visit behaviors with their co-created value and perceived medical service quality.
Numerous countries show an increasing trend with people desiring to undergo cosmetic surgeries abroad (Connell, 2006). Australian cosmetic surgery tourists are estimated to comprise around 85% of the country’s total medical tourists who are interested in offshore wellness treatments (Connell, 2006). Wilson (2011) notes that the largest group of cosmetic tourists in 2006, using Thai hospitals’ services, came from Japan. Davies and Han (2011) note that approximately more than half of the individuals among 620,823 Chinese, who were interviewed in a 2010 survey, expressed their desire to avail themselves of Korean cosmetic surgical facilities. Although several scholars have documented the likely desires of Australian, Japanese, and Chinese tourists for offshore health and well-being treatments (Han et al., 2015; Hanefeld et al., 2015; Imison & Schweinberg, 2013; Pan & Chen, 2014; Yu & Ko, 2012), CST cross-culture research remains scarce in the tourism literature. This study incorporates the responses of Australian, Japanese, and Chinese tourists in describing the multitextured alignments of co-creating valuable CST services. Different cultural backgrounds may impact tourists’ behaviors differently. CST research on respondents from different geographies having different cultural backgrounds is warranted for more conclusive findings.
Given the importance of CST across the globe and its complex structure, this study aims to examine (a) how tourists’ perceptions of valuable CST are addressed?; (b) does value co-creation help in meeting the expectations of tourists for valuable CST?; (c) does value co-creation exert any influence on CST-seeking tourists’ behaviors?
This study develops and proposes a conceptual model drawing from previous theoretical underpinnings. It examines tourists’ perceptions of valuable CST experience in terms of perceived medical service quality and its impact on tourists’ emotional attachment, trust, and intentions to visit. More so, this study examines the mediating role of value co-creation between tourists’ perceptions of medical service quality and their emotional attachment, trust, and intentions to visit. Our findings contribute to the tourism literature, CST literature, and other interlinked industries, such as the medical industry and the tourism industry for tourists’ overall health and well-being, which will ultimately impact promoting CST business. Findings will stitch the broken connections of value co-creation in aesthetic surgeries and tourism in designing state-of-the-art valuable CST services and assist policymakers in improving tourists’ quality of life, in parallel with influencing their emotional attachment, trust, and intentions to visit.
Literature Review
Cosmetic Surgery Tourism (CST)
CST is described by some as a well-being traveling trend to find optimal beauty where tourists undergo different aesthetic surgeries, for example, facelift, liposuction, blepharoplasty, abdominoplasty, breast augmentation (Miyagi et al., 2012). Researchers argue CST offers a holistic change in the body by linking individuals’ self-esteem and confidence discourses to a new personality with a beautiful face and body (Edmonds, 2007, 2010; Gimlin, 2007b).
Medical tourists plan their offshore itineraries for various quality-of-life enhancement treatments, such as skincare and wrinkle removal (Esiyok et al., 2017; Lee et al., 2012). Some evidence shows cosmetic treatments are categorized separately as one of the special constructs under the scope of medical tourism for individuals’ overall health and well-being (Tourism Research and Marketing, 2006, p. 14). CST differs in its discursive terrain to other forms of medical tourism and tends to link itself to wellness tourism for overall tourists’ health and well-being. It encapsulates aesthetic notions in its scope, not just precisely targeting sick bodies.
Traveling for offshore health and well-being has received unprecedented attention in recent decades (Chen & Petrick, 2013; Esiyok et al., 2017; Ridderstaat et al., 2019). The hierarchy of healthcare paradigm shows that healthcare consumers prefer cosmetic surgeries with other lifestyle enhancement procedures to improve their overall health and well-being (Runnels & Carrera, 2012). One of the reasons for tourists’ increased medical spending might be due to rising age cohorts and higher disposable capital coupled with the availability of quality cosmetic procedures across different medical tourism destinations (Connell, 2013; Majeed & Lu, 2017).
It is estimated that there are approximately 780 million tourists across 96 medical tourism destinations; approximately 33% of tourists avail themselves of offshore cosmetic surgeries in such participating medical tourism destinations for their overall health and well-being (Majeed, Lu, & Javed, 2017). Well-being tourists are willing to spend approximately 130% more on their quality-of-life treatments as compared with other tourists (Noree et al., 2016). The importance of CST has been noted by many scholars in fields other than tourism and hospitality by documenting how CST may help to improve individuals’ quality of life (Majeed, Rahman, et al., 2019). Thus, CST is pervasively expanding its scope to meet individuals’ perceptions of a better quality of life in the recent context.
Tourists’ Perceptions and Behaviors: A CST Perspective
The psychic associations of individuals’ expectations, perceptions, and behaviors have been noted by many scholars (Xue et al., 2020). An individual develops positive intentions to visit a health care facility when his or her expectations of perceived medical service quality are appropriately addressed by the host facility with valuable health service (Lee, 2004; Shabbir et al., 2010), that is, high-quality health treatment with more benefits than what he or she gives up to avail themselves of the service (Zeithaml, 1988). The concept of valuable health service can further be supported from the premises of expectation confirmation theory, which holds that customers have unique perceptual filters that confirm or reject the expected performance of a product or service and may determine the behaviors of customers. Expectation confirmation theory supports the idea that customers may buy a product or service if the perceived quality of a product or service exceeds their expectations or vice versa (Oliver, 1997; Ye et al., 2019).
The theory of planned behavior proposes that individuals’ perceptions, which are unique and, sometimes, complex, are important in determining their behavioral intentions. Theory of planned behavior further narrates that consumers’ positive and negative decisions are dependent on the positivity and negativity of their perceptions, respectively (Ajzen, 1991). Thus, positive perceptions lead to positive intentions to avail themselves of the service and visit a service destination.
Tourists’ demands are shaped by the interacting phenomena of their perceptions and expectations (Wang, 2012; Xue et al., 2020). Alongside rising age cohorts, tourists’ changing perceptions of a healthy lifestyle and aesthetic means of care have fueled demand for global CST. The medical tourism and treatment motivation (MTTM) model proposes that medical tourism is experiencing a shift in tourists’ preferences from conventional western medical treatments to eastern medical treatments alongside conventional surgical procedures (where necessary), and tourism for overall health and well-being (Majeed, Lu, & Javed, 2017). The recent shift in tourists’ demands is due to their changing perceptions of high-quality cosmetic treatments and the availability of comparatively advanced, high-quality, and risk-free health and well-being service at an offshore tourism destination.
CST-seeking tourists’ perceptions are largely revolving around the provision of valuable quality-of-life improvement treatments with notions deeply grounded in health and well-being. Nevertheless, a perfect matching theory with a CST context has yet to be explored. The combined philosophies of expectation confirmation theory, theory of planned behavior, and the MTTM model argue that the notion of tourists’ health and well-being has started to align itself with the emerging phenomenon of the lifestyle improvement approach, which is helpful to support the infant concept of tourists’ perceptions of CST.
Perceived Medical Service Quality and Tourists’ Emotional Attachment, Trust, and Intentions to Visit
A service has three dimensions in its utility cycle, that is, service provider, the customer, and the place of service. To utilize a service, there must be a service delivery person and a place where service is delivered to the customer who generates demand for service (Moeller, 2010). In medical tourism, the concept of service quality is linked to the person who is delivering service (Han & Hyun, 2015). Customers’ perceptions and behaviors are considered as a parameter to evaluate the quality of service.
Medical tourists perceive the high quality of offshore medical service in terms of qualified medical staff, appropriate availability of health and well-being treatments, and technically advanced infrastructure of the host destination (Crooks et al., 2010; Majeed & Lu, 2017). Medical facilities with Joint Commission International accreditation, hospital staff’s attentive patient care, availability of comfortable hospital vehicles, and hotel-like rooms may contribute to ensuring the delivery of perceived medical service quality to medical tourists (Kangas, 2007). The discussed theoretical underpinnings help to develop two subconstructs of perceived medical service quality, namely, staff competency and medical facility.
CST involves traveling by customers to avail themselves of quality-of-life enhancement services. In doing so, tourists might undergo certain invasive and noninvasive procedures, such as dental work, oral and maxillofacial surgery, Botox injection, liposuction, breast implants, and facelift, in parallel with visiting the attractions of the host tourism destination (Holliday et al., 2015; Majeed, Lu, & Javed, 2017; Miyagi et al., 2012). In CST, whether it is invasive or noninvasive, perceived medical service quality pertains to medical staff including doctors, cosmetic surgeons, and plastic and reconstructive surgeons delivering cosmetic surgical services at a service place, such as hospitals or clinics. Perceived medical service quality may become more sensitive when explored from a CST perspective due to tourists’ preferences for high-quality beauty enhancement procedures, which are not possible without highly skilled cosmetic surgeons and high-tech facilities, which might be different from ordinary medical facilities.
The notion of high service quality is a formative construct of positive behaviors, such as emotional attachment, trust, and intentions to visit a tourism destination (Abubakar & IIkan, 2016; Han & Hyun, 2015; Ramkissoon & Mavondo, 2017; Žabkar et al., 2010). Tourists’ positive behaviors are shaped by the availability of their perceived medical service quality at host medical facilities (Hong, 2016). A medical tourism destination with state-of-the-art medical service attracts tourists more than its competitors (Smith & Forgione, 2007). Competent medical staff, in terms of high-quality surgical capabilities, professional caring attitude, responsive behavior, length of time consumed in delivering service, accurate and reliable legal and ethical information, and hospital’s overall environment may determine wellness-seeking tourists’ favorable behaviors (Guiry & Vequist, 2011; Majeed et al., 2018; Safavai, 2006; Schmeida et al., 2007; Stern, 2005).
Tourists may doubt offshore CST treatments due to the risk of poor medical service, such as incompetence of medical personnel, surgical side effects, rumors about postoperative complications, and substantial curative costs involved in correcting the health complexities developed after the surgery (Brunette, 2014; Honigman et al., 2004; Leve & Pusic, 2012; Majeed, Lu, & Javed, 2017; Yu & Ko, 2012). Turner (2012) notes some serious consequences of offshore cosmetic/bariatric surgical treatments by documenting 26 reported death cases from 1993 to 2011. Such consequences keep tourists from seeking health and well-being corrections. This situation, therefore, influences medical tourists’ perceptions of health and well-being negatively with ultimate impacts on their moving ahead with any wellness plans.
Tourist positive perceptions may generate a psychic association with the service experience and may promote emotional attachment (Buonincontri et al., 2017; Pestana et al., 2019; Ye et al., 2019). Perceived medical service quality, appropriate health information, and services delivered by staff may build tourists’ trust, emotional attachment, and positive intentions to visit tourism destinations (Rempel et al., 2001; Thi et al., 2002). Emotional attachment is described as a connecting bond between an individual and an object (Ramkissoon et al., 2013b). This relationship further unfurls itself to develop tourists’ trust and intentions to visit a particular destination.
Individuals’ positive feelings may develop their emotional attachment to particular service personnel (Nunkoo & Ramkissoon, 2012; Townsend et al., 2018) leading to trust and favorable behavioral intentions to visit a destination. Tourists’ understanding of perceived medical service quality is important in enabling destinations to promote tourists’ emotional bonds with their CST services, alongside developing trust and positive intentions to visit the tourism destination.
Based on the above, the following are proposed:
Protective Motivation Theory, Attachment Theory, and the Service Dominant Logic Theory
Value co-creation is an outcome of customer engagement while interacting with service providers, alongside co-creating personalized service experience, which further leads to interpreting their different roles in defining and designing different experiences (Jamilena et al., 2016; Ramkissoon & Uysal, 2014, 2018). Value co-creation differs from value coproduction, which is limited in its scope. Value coproduction is an interdependent mechanism of customers and firms where both parties exert their influence to coproduce goods and services. The process of value coproduction, which involves the inputs of consumer and the firm, is the precondition of the value co-creation that may develop the ground of the joint creation of service experience (Eletxigerra et al., 2018; Prahalad & Ramaswamy, 2004). Firms and customers engage in the coproduction of offerings using their distinctive operand and operant resources, which enhance meanings of value co-creation for the customers (Eletxigerra et al., 2018; Ordanini & Pasini, 2008).
Positive perceptions lead to customers’ positive decision-making (Majeed, Majeed, & Ajike, 2019; Pestana et al., 2019; Xue et al., 2020). Medical tourists may not have sufficient health-related information at the time of travel decision-making (Ramkissoon, 2018), which may influence their perceptions and put them into a high risk–bearing situation. Service providers attempt to understand customers’ expectations and perceptions and attempt to satisfy them. CST tourists expect high-quality medical service, the availability of desired health and well-being procedures, tourism attractions, rehabilitation time with safety, less risk of postoperative complications, surgical side effects, and little cost of redressed skin (if needed) while taking their medical tourism decisions (Majeed et al., 2018).
The protective motivation theory is considered appropriate to address the risk-avoiding scenario. This theory narrates that decision-makers use their information-seeking skills with mental efforts and attempt to critically analyze alternatives to avoid the obvious or latent risks associated with their decisions (Bieger & Laesser, 2004; Sonmez & Graefe, 1998). This phenomenon calls on decision-makers’ involvement in risk-avoiding behavior. Individuals input different levels of effort, due to the varying levels of their involvement, while choosing a destination (Decrop, 2000; Hawkin et al., 2001).
Service providers may involve their customers in designing, defining, creating, and completing the output at a coproduction platform by integrating their resources with customers’ skills, knowledge, and desires. This delineates the concept of value co-creation where values are derived in contexts by users (Eletxigerra et al., 2018). The involvement phenomenon further links itself to the personal relevance of utilizing services or buying goods. The personal involvement of customers and service providers may impact customers’ perceptions, decision-making, and the abilities to evaluate different alternatives.
Many scholars note that the involvement and personal relevance constructs all lead to the attachment concept, which is, in addition, related to trust and commitment (Spake et al., 2003; Thomson, 2006), as well as consumers’ willingness to make a quick choice, forgive defections, and pay for the services or products (Ahluwalia et al., 2001). A destination attachment concept shows a connecting bond between tourists and destination attributes that further shape tourists’ favorable decision-making for visits and repeat visits (Han et al., 2019). The concept of attachment is also referred to as emotional attachment because of its emotional nature (Bowlby, 1979; Ramkissoon et al., 2013a; Ramkissoon & Mavondo, 2017).
The option attachment concept refers to attachment before the actual possession of objects (Ariely & Simonson, 2003; Carmon et al., 2003). This notion supports the involvement, personal relevance, and attachment concepts and links these to value co-creation in service development. CST values, if co-created between CST-seeking tourists and service provider, fall in the option attachment concept, which hovers over value creation before the actual utilization of service.
Kleine and Baker (2004) note that the connecting bond between individuals and objects may be developed before the actual possession/utilization of service or product, which may dynamically change over a passage of time. Hence, the option attachment concept can arguably be stated as an emotional attachment concept. The object in this study is CST value co-creation, which is to be jointly created by CST-seeking tourists and service providers.
Tourists’ involvement, personal relevance, and emotional attachment notions are ensured through their linkage to the development and value co-creation of CST. This is because involvement and emotional attachment start before the possession of CST service values. These concepts further evolve over time and may strengthen the emotionally connecting bond between tourists and service providers. Consumers’ involvement in the value co-creation process is noted as an antecedent to emotional attachment (Thomson et al., 2005). The above theoretical underpinnings are important considerations in the development of CST where the risks of poor medical service, discontinuity of surgical care, malpractices, and postoperative complications are present.
Coultar and Ligas (2004) note that the customers of health care services expect certain values, that is, functional, emotional, and relational benefits, in a service encounter. In this process, there are chances that an emotional attachment with a particular service personnel is developed. Favorable perceptions of tourists about the quality of medical services may generate emotional bonds with the CST service provider. It may also generate favorable behavioral intentions to visit the service-providing destination.
The provision of desired information to tourists may help in increasing the chances of a better CST experience. However, the most relevant pieces of information, such as health status, are normally held by tourists because they know more about their health than the service providers (Majeed & Lu, 2017). The exchange of information between tourists and tourism service providers may develop a relationship of trust between them (Lanjananda & Patterson, 2009). Because value is measured in terms of price versus quality alongside benefits received for what is contributed, tourists expect the functional, emotional, and symbolic meanings of service values, which may emerge from the value co-creation of CST. The involvement of CST-seeking tourists and CST service providers create meaning in terms of efforts, money, time, skills, and so on (Gnoth, 2007).
As consumers and service providers make decisions to maximize their values (Gardiner et al., 2012), they attempt to contribute their ideas to produce new services to achieve their goals. The intention to fulfill customers’ unmet needs is matched by the existing market offerings, which fuel their visits or buying intentions (Hoyer et al., 2010). The seminal service dominant logic theory (Vargo & Lusch, 2008) endeavors to present the joint creation of service value by a firm and its customers (Prahalad & Ramaswamy, 2004).
Scholars note that the level and ability to co-create with complex situations and service providers may shape tourists’ positive feelings and behavioral intentions (Prebensen et al., 2015). Thus, tourists’ participation levels in value co-creation are vital. Hence, firms are willing to let consumers participate in the value co-creation process with intentions to reduce risk and improve product quality as well as to increase the market acceptance of the product or service (Hoyer et al., 2010).
Despite the health risks and complexities involved alongside substantial curative costs, a narrow research focus is centered on understanding CST-seeking tourists’ behaviors. Varied expectations of CST-seeking tourists about perceived medical service quality and their resultant associations in co-creating a CST service experience remain scarce in the health, wellness, and medical tourism literature. Consumers may be provided the liberty to idealize, co-design, and co-create their personalized experience of service with the greater volume of desired information (Jamilena et al., 2016).
Consumers expect benefits of improved service performance in return for their inputs, for example, emotional energy, effort, and time in the value co-creation process, which may further influence their behavioral intentions to visit a tourist destination (Chekalina, 2015). The DART (dialogue, access, risk, transparency) model of value co-creation supports the notions of providing detailed information to the value co-creators to access an adequate volume of information where risk is shared and trust level is maintained between the firms and value co-creators (Prahalad & Ramaswamy, 2004).
The co-creation of service may generate effective communication on how to achieve valuable CST experience, such as perceived medical service quality, low risk, low price, better care than home, advanced facilities, and so on, which may develop tourists’ emotional attachment to service providers, trust, and positive behavioral intentions to experience a better quality of life (Bennett et al., 2011; Ramkissoon, 2016). An individual’s feeling of relevance in helping in the co-creation may lead to developing personal responsibility for decisions while looking for solutions to problems. This situation elevates individuals/contributors/co-creators to become more like risk-takers, which may significantly impact tourists’ decisions to go on CST trips. Hence, CST-seeking tourists may be delighted with their CST co-created values by sharing risks with the service providers. The proper understanding of these premises is important to shape the perceptions of CST-seeking tourists with their positive behavioral intentions.
The following are proposed:
Material and Method
Questionnaire and Scale Measurement
Based on the above theoretical underpinnings, tourists’ perceived medical service quality is presented as a multidimensional second order reflective construct (see Ringle et al., 2012) with items reflective of first order constructs (staff competency, medical facility).
A survey questionnaire with a believable scenario was developed to test the associations between the constructs under examination (see Supplemental Appendix A). Scenario guidelines were borrowed from the work of Majeed, Lu, and Usman (2017) and adapted to the study. Validated scale items, that is, a total of 29 items, to measure the constructs were adopted from literature (e.g., Han & Hyun, 2015; Majeed et al., 2018; Prebensen et al., 2015) and measured on a 7-point Likert-type scale ranging from 1 = strongly disagree to 7 = strongly agree. A pretest of the questionnaire was conducted to ensure content validity. Minor changes were incorporated in the wording and expressions of a few questions changed following respondents’ recommendations for clarity. The questionnaire was translated from English to Japanese and Chinese languages, following the method of back translation (Soriano & Foxall, 2002). Native Japanese and Chinese speakers with English proficiency reviewed the translated questionnaires for accuracy (see Supplemental Appendix A).
Data Collection
The target population of this study was cosmetic surgery–seeking tourists. A total of 331 questionnaires were completed in the first 3 weeks of February 2018 by Australian, Japanese, and Chinese international tourists, who had an interest in CST, as they were sitting in the waiting lounges of Beijing Capital International Airport and Xiamen Gaoqi International Airport. Tourists above 18 years of age were considered in the present study to ensure the consent requirement was followed (Majeed, Lu, & Usman, 2017). After careful scrutiny, 24 respondents had negatively answered the screening questions (see Figure 1), 11 responses were found to have duplicates, that is, respondents gave more than one response to the same question on the same scale, and 17 responses were incomplete and, thus, excluded from final data analysis. In the second round of response evaluation, 11 questionnaires were again found to be incomplete and, hence, considered unusable. A total of 279 responses were retained for the final analysis. Respondents’ recruitment and exclusion details to reach the 279 sample size are shown in Supplemental Appendix B. The study respondents’ sociodemographic profiles are summarized in Table 1.

Structural model results.
Sociodemographic Profiles of Study Respondents.

Statistical Analysis
Scholars note that structural equation modeling helps to analyze first order and second order constructs with their latent associations (Hair et al., 2016). Partial least-square structural equation modeling (PLS-SEM) tool was used for data analysis. PLS-SEM is considered appropriate due to several reasons: (a) variance is to be predicted and explained in certain important constructs of the study, that is, perceived medical service quality, value co-creation, emotional attachment, trust, and intentions to visit; (b) a complex structural association among study variables is sketched on the canvas of this study; (c) the associations among perceived medical service quality, value co-creation, emotional attachment, trust, and intentions to visit are additional constituents in the development of a theory that endeavors to deeply study new systems; (d) and a relatively small sample size, that is, n = 279. SmartPLS 3.2.6 was used for PLS-SEM analysis to test the proposed hypothetical associations of this study.
Results
A two-step approach, that is, measurement model assessment and structural model testing (Nunkoo et al., 2013), was adopted while interpreting the results.
Measurement Model Evaluation
Findings show that all loading values were significant at .001, that is, above .70/.50 of the measurement model. Composite reliability and Cronbach’s alpha values of constructs were found above .70, presenting acceptable reliability. Average variance extracted (AVE) values were above the threshold limit, that is, .50. Discriminant validity was achieved. It means each AVE square root was found greater than the reflective items’ correlation, which meets Fornell-Larcker’s criteria (Fornell & Larcker, 1981; see Table 2).
Model Measurement.

Note. LV = Loading Values; CR = Composite Reliability; α = Cronbach’s alpha; SQRT = Square root; AVE = Average Variance Extracted; VIF = Variance inflation factor; Cor2 = Correlation (highest squared between model constructs); EA = Emotional attachment; T = Trust; IV = Intentions to visit; VCC = Value co-creation; PMSQ = Perceived medical service quality; SC = Staff competency; MF = Medical facility.
All loadings are significant at .05% level of significance (two-tailed).
Heterotrait-monotrait results were found below the cut-off level, that is, .85 or .90, in all the presented cases supporting the discriminant validity (Majeed et al., 2018; see Table 3).
Ratio Results HTMT Analysis.
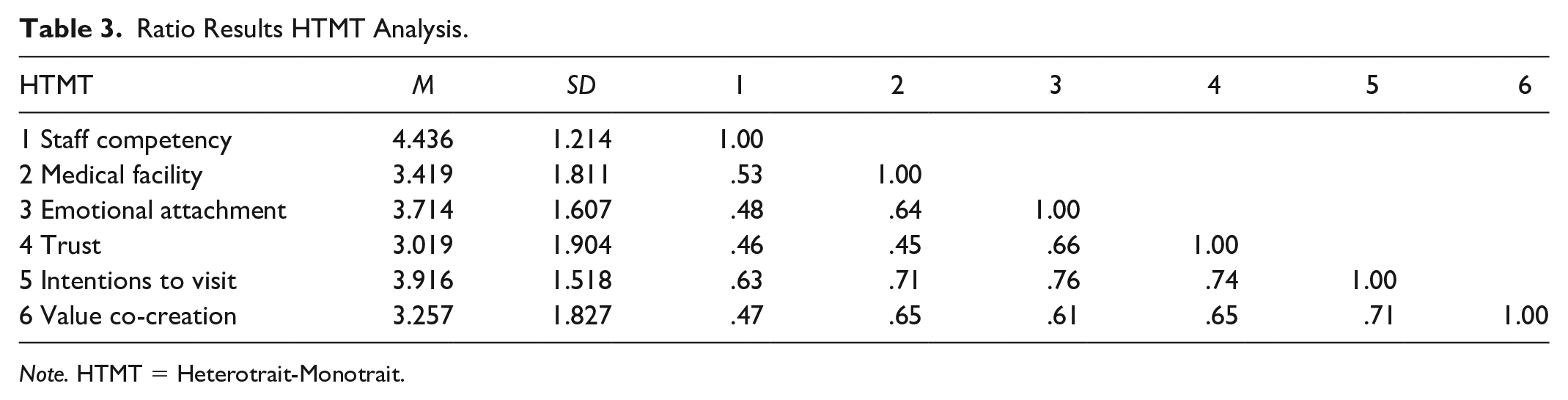
Note. HTMT = Heterotrait-Monotrait.
Structural Model Evaluation
For the structural model measurement, a five-step approach was adopted (Hair et al., 2013). First was the constructs’ collinearity assessment. To examine the probability of collinearity, the predictor sets of the present study were examined. Minimal collinearity with variance inflation factor (VIF) below the cut-off level of 5 was found in the results. The structural model predictor sets were found in line with the satisfactory level of collinearity. The second was the path-coefficients of the structural model (Hair et al., 2013). Estimation was assessed in the structural model through the magnitudes and signs of path coefficients between the latent variables and their path relationships (see Table 4 and Figure 1).
Path Coefficient of Structural Model (Direct Effect and Hypotheses Testing).

Note. PMSQ = Perceived medical service quality; EA = Emotional attachment; T = Trust; IV = Intentions to visit; VCC = Value co-creation; n.s. = Not significant.
t | N = 2.58 at p = .01 level. ****t | N = 3.29 at p = .001 level.
The third was the R2 values (coefficient of determination) as presented in Table 2 and Figure 1. Endogenous constructs were found satisfactory because their R2 values were found to be above 10% (Majeed et al., 2018; Majeed, Lu, & Usman, 2017). However, results show that the R2 value of trust was moderate, that is, .59, while R2 values of emotional attachment and intentions to visit were comparatively weak, that is, .36 and .53, respectively. The fourth was effect size measured by calculating f2 and q2 values. Effect sizes are noted as small and large if f2 and q2 values are .02 and .35, respectively; however, these values at around .15 are described at a medium level (Majeed et al., 2018; see Table 4). Finally, blindfolding and Q2 values (predictive relevance) were calculated (see Table 2). All Q2 values were above the zero threshold level, hence, supporting the predictive relevance of the model for the endogenous latent items mentioned in reflective constructs. Findings (Table 4) show that perceived medical service quality significantly influenced emotional attachment (β = .29***), trust (β = .32****), and intentions to visit (β = .34***), supporting hypotheses H1a, H1b, and H1c.
Mediation Testing
Boot estimates from the 5,000 bootstrap samples were used for mediation testing (Hair et al., 2013). Each bootstrap sample has an equal number of observations as the original sample, that is, 279, for t values and standard error of estimation (Hair et al., 2013). Variance Accounted For (VAF) was calculated to measure the ratio of indirect effect size to the total effect size (Hair et al., 2013).
Findings (Table 5) show that the associations between study constructs were significant, that is, t > 1.96 at the .05 significance level. VAF results show that partial mediation of value co-creation was found among all study constructs, that is, VAF between 80% and 20% (Majeed, Lu, & Usman, 2017). These results support hypotheses H2a, H2b, and H2c.
Bootstrapping-Mediation Effect and Hypotheses Testing.
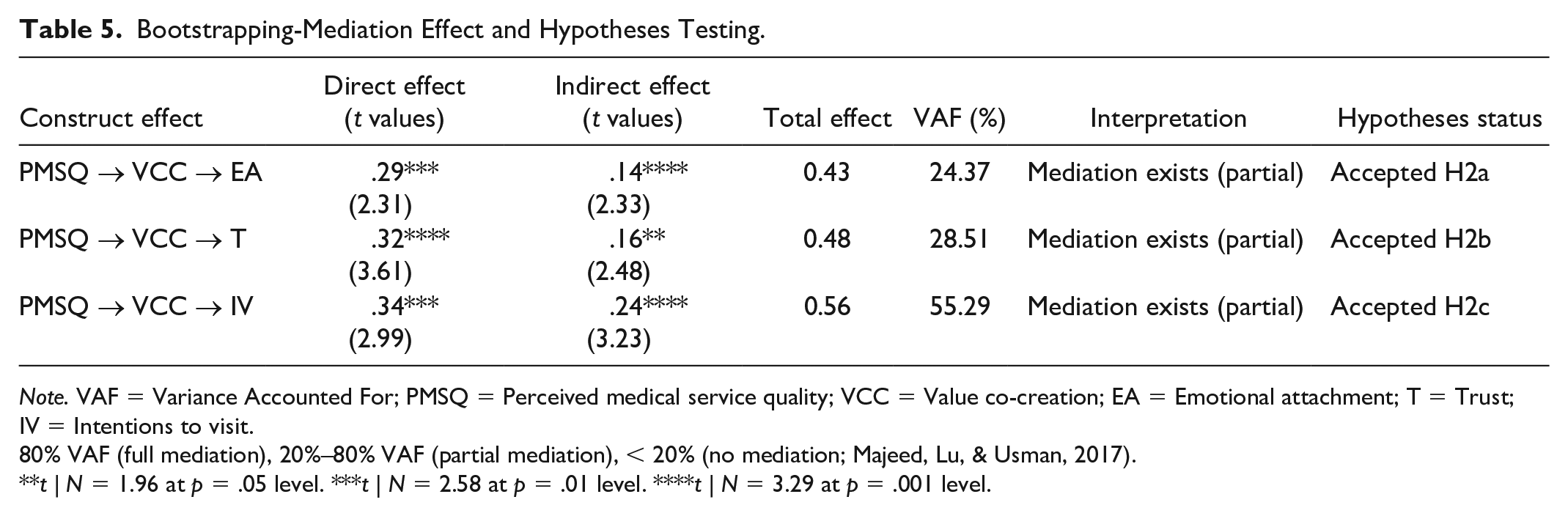
Note. VAF = Variance Accounted For; PMSQ = Perceived medical service quality; VCC = Value co-creation; EA = Emotional attachment; T = Trust; IV = Intentions to visit.
80% VAF (full mediation), 20%–80% VAF (partial mediation), < 20% (no mediation; Majeed, Lu, & Usman, 2017).
t | N = 1.96 at p = .05 level. ***t | N = 2.58 at p = .01 level. ****t | N = 3.29 at p = .001 level.
Discussion
Based on value co-creation theory, this study explored the associations of cosmetic surgery tourists’ perceptions of medical service quality and its impact on their emotional attachment, trust, and intentions to visit under the mediated influence of value co-creation for CST experience. Valuable CST in terms of tourists’ perceived medical service quality, with subconstructs of staff competency and medical facility, and behaviors, that is, emotional attachment, trust, intentions to visit, were examined. Our findings support H1a, H1b, and H1c, which argued for the positive impacts of tourists’ perceived medical service quality on their emotional attachment, trust, and intentions to visit. Our findings also support H2a, H2b, and H2c, which argued for the mediating role of value co-creation among the associations of tourists’ perceived medical service quality, emotional attachment, trust, and intentions to visit to present the woven phenomena of valuable CST.
The sociodemographic profiles of the study respondents show that approximately 68% of the tourists have middle- to low-income earning capacity. These statistics support the assumptions taken by Gimlin (2007a) and Casanova and Sutton (2013) that participants’ interest to avail themselves of CST is increasing in the middle- to low-income earners recently.
Cosmetic surgery is generally conceived of as hope for beauty enhancement. With the notions of beauty and elegant personality, existing theoretical underpinnings describe CST as women’s trendy phenomenon in the circuits of offshore beauty enhancement surgeries (Bell et al., 2011; Heyes, 2007; Holliday et al., 2015). Without disagreeing with the viewpoints of scholars working on the women-centered literature of cosmetic surgery, our study presents responses from men and women to show the interest of both genders in CST. These provide further support to Holliday et al.’s (2015) and Casanova and Sutton’s (2013) study on men’s interest in CST, for example, hair transplants and surgery to improve workplace competitiveness.
The empirical findings of this study emphasize notions of health, well-being, medical tourism, and wellness tourism highlighting future research prospects within the domain of CST.
Theoretical Implications
This study makes several contributions to literature, more precisely to medical tourism, wellness tourism, and health tourism. First, despite the growing discussion in hospitality and tourism, an examination of associations of perceived medical service quality and tourists’ emotional attachment, trust, and intentions to visit from a CST perspective is scant in the literature. Our findings from Australian, Japanese, and Chinese tourists for CST endeavor to validate certain theoretical associations of tourists’ perceptions of health and well-being, which contribute to developing the theoretical foundations of CST.
Second, this study used the service dominant logic theory to understand the role of valuable tourism experience in the emerging field of CST. The service dominant logic theory helped to understand and interpret the underlying patterns of tourists’ perceived medical service quality, emotional attachment, trust, and intentions to visit that interact to generate valuable CST experience. These findings may assist researchers in wellness tourism, medical tourism, and other niches of health tourism in developing a theoretical understanding of how to influence tourist behaviors with valuable tourism experience. It can be examined with an appropriate understanding of tourists’ perceptions of health and well-being with regard to increasing valuable tourism.
Third, this study investigated perceived medical service quality with subconstructs of staff competency and medical facility, which impact the phenomenon of CST. Although the understanding of medical service has been found in the discussions of health tourism (Ghosh & Mandal, 2019; Majeed et al., 2018), it is important to examine perceived medical service quality in relation to CST and how it can influence tourists’ emotional attachment, trust, and intentions to visit. This study’s findings help to define the precise meaning of perceived medical service quality in CST and to extend the theory that defined a service quality concept that can influence consumer behavior for business promotion in complex systems.
Fourth, our findings provide further empirical support to the existing knowledge of medical tourism (e.g., Elg et al., 2012; Hardyman et al., 2014) with additional discussions on CST-seeking tourists’ behaviors. This study confirms the findings of scholars who attempted to examine the instrumental role of medical service in driving desired tourists’ responses (González et al., 2007; Han & Hyun, 2015). Although contexts are different, meeting expectations and influencing tourists’ behaviors are also in line with past studies, for example, Nunkoo and Ramkissoon (2012b), Ramkissoon et al. (2012), and Thomson et al. (2005). Our findings show how they are related in the research domains of health and well-being and in the special case of CST, bridging the theoretical gaps in medical tourism and wellness tourism.
Practical Implications
Considering the whole working mechanism of CST encapsulated in the conceptual model (as presented in Figure 1), this study shows that value co-creation mediated the associations of perceived medical service quality and tourists’ emotional attachment, trust, and intentions to visit. This provides meaningful guidelines to the professionals of CST about how to positively influence behaviors of CST-seeking tourists by incorporating their inputs in generating valuable tourism experience.
Perceived medical service quality is an important source for the competitiveness of a CST destination. It is because the notion of perceived medical service quality reflects itself in terms of technical, high-quality, and nonsubstitutable services. Organizational willingness to improve tourists’ overall experience of visiting a destination supports the culture of value co-creation. However, perceived medical service quality may create friction in the beauty and well-being notions of CST if appropriate value co-creation grounds are not developed. This is because perceived medical service quality is deeply linked to the participation of cosmetic surgery-seeking tourists and service providers in the value co-creation process through the improved means of communication, pushing teamwork, co-ideation, co-designing, and co-creating cosmetic surgery service during the efforts’ collaboration phase. The role of professionals’ of CST, for example, physicians, cosmetic surgeons, dentists, skin specialists, dietitians, make-up artists, traditional and complementary medicine experts, tourism service providers, and government is thus important in the present context of medical tourism and wellness tourism.
Participating CST destinations need to understand the industry’s customers in more detail to serve them with their desired CST service. These may equally be applied in cosmetic clinics where detoxification procedures, massage, spa, Chinese traditional medicine, Ayurveda, naturopathic treatments, or other forms of traditional and complementary medicine treatments may be offered to improve the quality of life and well-being of both tourists and nontourists. Alongside global implications for health and well-being, this study’s findings are helpful in equipping the industry professionals of Japan, China, and Australia who are developing strategies for the promotion of aesthetic tourism (Mair et al., 2014).
Surgery-seeking tourists are increasingly hard-pressed to find well-trained medical staff including surgeons, physicians, and nurses and quality medical facilities for their health care (Brunette, 2014; Ruka & Garel, 2015). Overall, cosmetic tourists are looking for high-quality medical services that would mediate health-related complexities for a satisfactory tourist experience (Majeed et al., 2018). CST stakeholders’ appropriate preparations will not only serve the biggest exporters of CST-seeking tourists, that is, Australia, Japan, China, but also serve tourists from the rest of the world. In the changing time, place, and cost (TPC) dimensions of tourism (Majeed & Lu, 2017), CST stakeholders also need to devise state-of-the-art policies to cater to CST-seeking tourists’ perceptions of medical service quality and remain competitive with high-quality CST service.
Although the context of this study is CST and the target population was cosmetic surgery tourists, there might be many individuals who prefer cosmetic treatments over conventional tourism. Findings of the study may equip people who are not primarily tourists but interested in valuable cosmetic surgery, high-quality cosmetic treatment, to improve their health and well-being with the robust interpretations of medical service quality. Service providers of CST may target nontourists with state-of-the-art cosmetic surgeries, skilled cosmetic surgeons, skilled plastic and reconstructive surgeons, hygienic hospitals and clinics, as well as advanced medical technologies as a part of medical service quality, to provide cosmetic treatments to improve their quality of life.
Conclusion
By following a hypothetico-deductive research approach, our findings highlight the importance of value co-creation in resolving the complexities of CST with tourists’ inputs of perceived medical service quality and its impact on their emotional attachment, trust, and intentions to visit, which are vital antecedents to promoting CST business at host tourism destinations. The scope of this study includes the development of value co-creation associations between CST-seeking tourists and the professionals of the medical industry, the tourism industry, and the wellness industry.
Limitations and Future Research
There are a few limitations in this study, which open doors to future research. Although Beijing and Xiamen expect a high frequency of international tourists with different cultural backgrounds, the participants were approached at only two airport locations in China. Tourists’ responses may vary at other locations, for example, at health resorts, cosmetic clinics, and tourist sites. Moreover, all influencing CST attributes were not included while developing the theoretical model of the present study. Further research may incorporate other factors such as traditional and complementary medicine and healthy food for beauty-conscious patients in the contexts of medical hotels and restaurants. Participants from three countries, that is, Australia, Japan, and China, were considered for this study based on previous research. However, an individual’s response may be different in other countries due to their distinct national cultural values (Majeed et al., 2018; Majeed & Lu, 2016). Although CST is gaining attention, it is mostly considered by beauty-conscious individuals with affluent resources. Generally, CST has inherent limitations due to the special interests of individuals and their available resources. Thus, the likelihood of a low sample size was probable for this study due to the inevitability of finding few individuals who have an interest in CST. A wider and diversified sampling approach could be followed in future CST research in the light of guidelines sketched on the canvas of this research.
Supplemental Material
Appendix_1 – Supplemental material for Beauty and Elegance: Value Co-Creation in Cosmetic Surgery Tourism
Supplemental material, Appendix_1 for Beauty and Elegance: Value Co-Creation in Cosmetic Surgery Tourism by Salman Majeed, Zhimin Zhou and Haywantee Ramkissoon in SAGE Open
Supplemental Material
Appendix_2 – Supplemental material for Beauty and Elegance: Value Co-Creation in Cosmetic Surgery Tourism
Supplemental material, Appendix_2 for Beauty and Elegance: Value Co-Creation in Cosmetic Surgery Tourism by Salman Majeed, Zhimin Zhou and Haywantee Ramkissoon in SAGE Open
Footnotes
Acknowledgements
We acknowledge the cooperation of graduate students of the University of Science and Technology Beijing and Xiamen University in helping the authors to conduct the field surveys. Thanks to Ren Dashuai for translating the questionnaire into Chinese. Thanks to Yui Kimura for translating the questionnaire into Japanese.
Author Contribution
All authors directly participated in the research and development of the article. All authors have approved the final version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the National Natural Science Foundation of China (Grant No. 71772126) and Guangdong Provincial Major Scientific Research Projects (Grant No. 2016WZDXM006). The sponsors have no role in the study design; nor in the collection, analysis, and interpretation of data; nor in the writing of the report; nor in the decision to submit the article for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.