
Abstract
The aim of the study was to investigate surgical patients’ pain experience and the quality of nursing care in managing acute postoperative pain. A descriptive cross-sectional study using a Strategic and Clinical Quality Indicators in Postoperative Pain Management Questionnaire collected data of 247 patients who underwent surgery in the surgical clinics of a state hospital. Data of 141 patients were included in the analysis. The mean scores for the scale items indicated that the quality of care was acceptable or low. The level of postoperative care, nursing interventions, and environmental subscales of the questionnaire were at an acceptable level, but pain management subscales of the questionnaire were low. These results suggest that health care, including measurable, applicable quality indicators, should be planned and evaluated to maintain professional nursing services, to achieve postoperative pain management and to relieve pain.
Introduction
Pain is an important problem for postoperative patients, and postoperative pain management (POPM) is an important part of patient care in surgical clinics (Meissner et al., 2018). Every year, millions of people undergo surgery and experience postoperative pain at various levels. It has been reported that nearly three quarters of patients undergoing surgical interventions have acute pain, and that 20% to 80% of postoperative patients experience pain (Gan, 2017; Meissner et al., 2018).
It has been reported that although pain management is an important part of intraoperative and postoperative care, approximately 30% to 75% of patients experience moderate to severe pain postoperatively, and that this rate is 41% to 61% in developed countries (Buvanendran et al., 2015; Gan et al., 2014; Meissner et al., 2015). Meissner et al. (2015) determined that 80% of postoperative patients experienced acute pain, and 75% of them experienced severe or extreme pain. The incidence of postsurgical pain in Turkey is reported to range between 30% and 80% (Acar et al., 2016; Ayhan & Kurşun, 2017). Although there is no accurate data on the incidence of postoperative pain in the Turkish Republic of Northern Cyprus (TRNC), it was found that of the patients having undergone abdominal surgery, 73% experienced pain on the first postoperative day (İzveren & Dal, 2011). In another study conducted in surgical patients, the mean score of “the most severe pain in the first 24 hours” was found as 8.33 ± 0.88 (0–10; Tokpınar, 2019).
Effective pain management is an integral part of modern surgical practices. Postoperative pain should be prevented and controlled. The goal of acute pain management is to prevent postoperative complications, to speed up healing, to minimize side effects caused by analgesics, to prevent acute pain from becoming chronic pain, and to reduce the frequency and severity of pain (Gordon et al., 2016; Meissner et al., 2015).
Pain management is recognized as an important indicator of standards of accreditation in health and quality of health care. For this reason, it cannot neglect the importance of pain management quality in postoperative care (Vatansever & Akansel, 2014). Quality development includes an assessment of the quality of care at regular intervals (Dirimeşe et al., 2014; Gan et al., 2014; Meissner et al., 2018).
The quality of health care services is monitored by analyzing the structure, processes, and outcomes of health care. It should manifest the opinions of the health professionals on the indicators of quality (de Meij et al., 2018). Currently, patient-reported outcome measures (PROMs; symptoms, health situation, quality of life, and so on) and patient-reported experience measures (PREMs; length of waiting period and so on) are used to evaluate the quality of health care services (Devlin & Appleby, 2010). Pain management is an important problem for the patients. Pain management outcomes (Zoëga et al., 2015) and satisfaction with pain management (Bozimowski, 2012) have been important indicators to evaluate the quality of health care in pain management (Bozimowski, 2012).
The American Pain Society (APS) recommends that to improve the quality of pain management, focus should be put on the severity of pain and the effects of pain on patient outcomes (APS, 1995). In Gordon et al. (2016), six quality indicators were proposed to increase the quality of pain management. These indicators are as follows: recording the severity of pain with a numeric rating scale or a verbal descriptor scale at frequent intervals, management of pain with treatment methods other than intramuscular injection methods, regular pain management, pain relief, management of pain to facilitate the quality of life and activities of daily living, and informing patients about pain and pain management. Establishing quality management systems in pain management is recommended; quality management systems have a positive effect on patients’ postoperative quality of life and satisfaction. Ensuring effective pain management is one of the key elements of patient satisfaction, which is a quality indicator in hospitals (Glowacki, 2015; Usichenko et al., 2013).
The best method to assess the quality of pain management is the assessment of pain management by patients (NHS Quality Improvement Scotland, 2005). A study investigating the quality of POPM determined that nurses believed that patients experience pain, that nurses and physicians cooperated in POPM, that the severity of pain and effects of analgesics were not regularly assessed, and that the severity of pain and the patient’s gender, and that receiving information about pain management were among the factors affecting quality of care in pain management (Milutinović et al., 2009; Siu et al., 2019). In another study, as the severity of the pain experienced by the patients increased, their satisfaction with the quality of care of pain management was found to be reduced (Patanwala et al., 2018). However, there are many studies showing no or only a weak association between satisfaction and pain intensity (Phillips et al., 2013; Schwenkglenks et al., 2014).
In a study in which the quality of pain management of orthopedic patients was assessed, it was found that the patients’ mean quality of care scores ranged from 2.9 to 4.6. The minimum and maximum possible scores to be obtained from the scale were 1 and 5, respectively. The higher the score was, the higher the quality of care was. The study also determined that the quality of health professionals’ assessment of the severity of pain, ranging between 0 and 10 in the morning, at noon and in the evening, was low (Idvall & Berg, 2008). In their study conducted to assess satisfaction with pain management, Shill et al. (2012) found that satisfaction levels of the patients who were administered sufficient analgesics, who were talked to regarding their pain, and who received oral opioids were high.
Because there is a gap in Turkish literature related to studies investigating the quality of pain management, we think the results of the present study will contribute to improvement in the quality of care by assessing patients’ pain experiences with standard measurement tools, determining the areas necessary for the improvement of care, identifying and implementing effective nursing interventions, and determining patients’ satisfaction with pain management. The aim of the study was to investigate surgical patients’ pain experience on the third postoperative day and the quality of the care given for pain management.
Research Questions
Methods
Design
This descriptive, cross-sectional study was carried out in general surgery, orthopedics, urology, and neurosurgery units in a state hospital.
Sample and Setting
The study population comprised 247 patients who underwent surgical intervention during the 4-month period when the study data were collected at the surgical clinics in a state hospital. All the patients in the study population were intended to be included in the study. However, of the patients in the study population, 103 were excluded because they did not meet the inclusion criteria. Of the remaining 144 patients, three did not agree to participate in the study; therefore, the study sample included 141 patients. The participation rate in the study was 96%. Inclusion criteria were the following: (a) being older than 18 years, (b) being able to understand the study guidelines, (c) being in the hospital on the postoperative third day, and (d) not having been diagnosed with cancer.
Instruments
The study data were collected using the Patient Information Form and Strategic and Clinical Quality Indicators Postoperative Pain (SCQIPP) in POPM.
Patient Information Form
The form prepared by the researcher through a literature review included 23 items questioning variables such as age, gender, marital status, education status, diagnosis, surgical procedure, surgical intervention period, factors increasing or decreasing pain, duration of pain management process, and presence of a chronic illness (Idvall & Ehrenberg, 2002; Usichenko et al., 2013).
SCQIPP
The questionnaire was developed by Idvall and Ehrenberg (2002) to measure the quality of POPM. The reliability and validity of the Turkish version of the questionnaire was performed by Vatansever and Akansel (2014). The Cronbach’s alpha of the scale was .81. The scale consisted of 14 items. The SCQIPP consists of three subscales: pain management, nursing intervention, and environment. The items in the SCQIPP were rated on a 5-point Likert-type scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The minimum and maximum possible scores that could be obtained from the scale were 14 and 70, respectively. The higher the score, the greater the satisfaction with the postoperative management.
Although a mean score lower than 4 for an item indicated that the quality of health care was low, a mean score between 4 and 4.5 indicated that the quality of health care was acceptable, and a mean score greater than 4.6 indicated that the quality of health care was high.
In addition to the aforementioned 14 items, the questionnaire included another two questions about patient satisfaction and three questions about pain severity. In this study, the Cronbach’s alpha was .69.
Data Collection
The researcher informed the participants who met the inclusion criteria about the purpose and method of the study at the clinics where the study was conducted. Informed consent was obtained from the patients who agreed to participate in the study. Patients answered a questionnaire on the third postoperative day. It took about 15 to 20 minutes to administer the questionnaire. The data of the research were collected by the researchers between December 19, 2016, and April 19, 2017.
Data Analysis
The study data were analyzed using the SPSS (20.0) for Windows Software Package Program. Patient characteristics were assessed using numbers, percentages, and mean scores for pain severity, factors increasing and decreasing pain and satisfaction with pain management. The factors affecting pain and satisfaction with pain management were assessed with the Kruskal–Wallis and Mann–Whitney U tests.
Ethical Considerations
Written informed consent was obtained from the patients who agreed to participate in the study. In addition, to carry out the study, permissions were obtained from the Ministry of Health Institution (Decision number: SAB005/3344) and the Scientific Research and Publication Ethics Board of the University (Decision number: ETK00-2016-0190).
Results
Characteristics of the Participants
Of the patients participating in the study, 29.8% were in the 36 to 50 age group, 56.0% were male, 84.4% were married, 35.5% were primary school graduates, 49.7% were treated in the orthopedic clinic, 44.0% were operated on for 1 to 2 hours, and 62.4% underwent general anesthesia, whereas 92.4% of the patients took nonsteroidal anti-inflammatory drug for POPM. Ninety-eight percent of the patients waited less than 10 minutes for the treatment of their pain (Table 1).
Patient Demographic and Clinical Variables (N = 141).
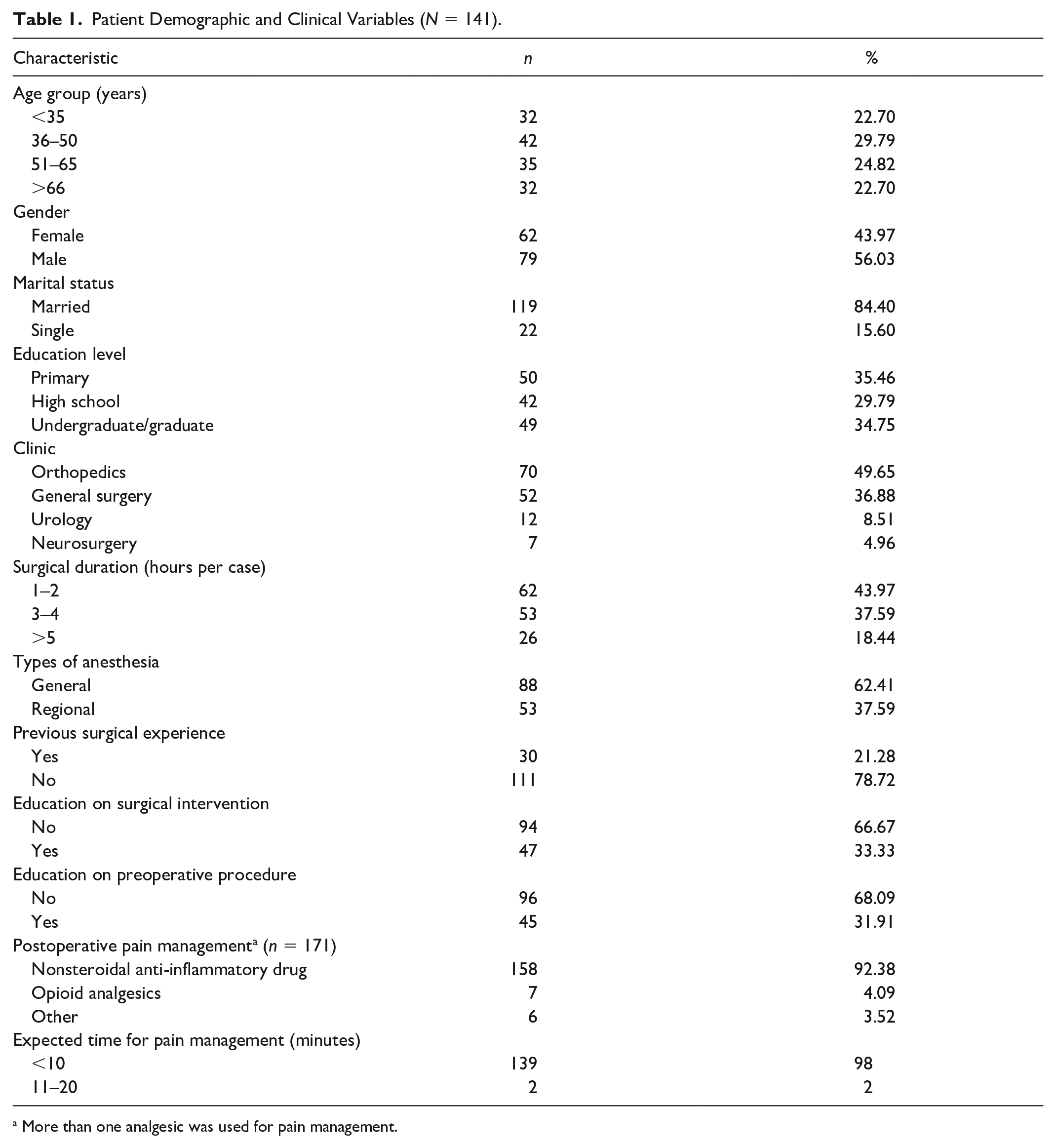
More than one analgesic was used for pain management.
Of the patients participating in the study, 21.3% had a previous surgical experience, 31.9% had preoperative education, and 33.3% had education in surgical intervention (Table 1). However, almost all of them (99.3%) received no training for pain.
Pain Characteristics and Pain Severity of Participants
The mean score for the most and least severe pain experienced within the first 24 hours was 7.5 ± 1.4 and 2.8 ± 1.4, respectively. When the questionnaire was administered, the mean score for the severity of pain was 2.8 ± 1.4. The patients’ mean satisfaction score for postoperative pain relief was 8.9 ± 0.7, and 63.1% of the patients gave 9 points when defining their postoperative satisfaction
Of the participants, 87.9% described their pain as tingling, 87.9% experienced pain while getting out of bed, 86.5% stated that movement increased their pain, and 61.7% stated that their pain was relieved by rest (Table 2).
Characteristics of Pain Patients Experienced and Factors Affecting the Pain (N = 141).

More than one response.
Postoperative Quality of Care and Affecting Factors
The mean score the participants obtained from the overall SCQIPP was 49.8 ± 2.9, and the lowest and highest scores they obtained were 42 and 61, respectively. The mean scores the participants obtained from the subscales of the SCQIPP were 28.3 ± 1.8, 13.3 ± 1.4, and 8.2 ± 0.7, respectively (Table 3).
Patients’ Mean Scores (SD) for the Subscales and Items in the Strategic and Clinical Quality Indicators in Postoperative Pain Management Questionnaire (N = 141).

Note. SD = standard deviation.
Based on the levels: <4.0 = low, 4.0–4.5 = acceptable, and >4.5 = good.
The comparison of the mean scores for the items of the SCQIPP revealed that the participants obtained the highest score (4.1) from questions Q4 and Q8; the lowest score (1.8) came from Q1. The highest score corresponded to “acceptable care quality”; the lowest score corresponded to “low care quality” (Table 3).
The difference was statistically significant between the participants obtained from the SCQIPP and its subscales in terms of some variables such as marital status, education, the clinic where they are treated, the duration of the operation, and receiving training about the operation (p < .05; Table 4).
Comparison of Patient Demographic and Clinical Variables and the Scale and Subscale (N = 141).

Note. M = mean; SD = standard deviation.
Z: Mann–Whitney U test. b χ2: Kruskal–Wallis test.
p < .05.
There were no statistically significant differences between the participants’ mean scores for the quality of postoperative care in terms of variables such as age, gender, presence of a chronic disease, type of anesthesia applied, and previous surgical experience (p > .05).
Discussion
People may experience fear and anxiety if they have had a negative previous pain experience, if effective pain management is not provided, if their pain is not relieved, or if they have severe pain. On the other hand, if the pain the person experiences is effectively managed, the person can cope better with the pain (Acar et al., 2016).
Every year, millions of people undergo surgery and experience postoperative pain at various levels. About three quarters of patients undergoing surgery have acute pain, and the severity of the pain is moderate to severe in 80% of these patients (Buvanendran et al., 2015; Weiser et al., 2016). In Patanwala et al.’s (2018) study, the patients experienced moderate to severe levels of pain intensity in the first 24 hours after surgery. Of the participants, 32% gave 1 to 3 points to rate the severity of pain measured when the study data were collected. In another study, the patients reported moderate (36.7%) to severe (21.55%) levels of pain intensity (Ramia et al., 2017). In the present study, more than half of the patients were found to have moderate to severe pain after a surgical procedure (Postoperative Day 3). According to the study results, although patients waited less than 10 minutes for pain treatment, half of the patients experienced severe pain within the first 24 hours. The patients’ severe pain was thought to result because opioid-type drugs were not used for severe pain, and anti-inflammatory drug therapy was implemented in 85% of the cases.
An important step in the evaluation of pain in POPM is the identification and recording of the characteristics of pain. Determining the characteristics of pain is very useful in evaluation of the origin of pain or underlying pathophysiology (i.e., nociceptive vs. neuropathic pain). Nociceptive pain occurs as a result of the stimulation of nociceptors (mechanic, thermal, or chemical stimulation and so on). On the other hand, neuropathic pain stems from the damage or injury in nerve fibers. Determining the characteristics of pain is highly important because it may change the treatment approaches (Swift, 2015). Postoperative pain that patients experience is defined as pulsating, tingling, burning, blunt, sharp, and pressuring (Tsai et al., 2015). Büyükyilmaz and Aştı (2010) studied postoperative pain in orthopedic surgical patients (n = 150) and determined that 78% of the patients experienced pulsating pain and 52.7% experienced tingling pain. In the study performed by Akyol et al. (2009), 32.5% of the patients had pulsating pain and 76.7% of the patients felt pain at the incision site. In the present study, evaluation of pain-related characteristics revealed that the patients experienced tingling and pulsating pain, and the results of the study were consistent with those reported in literature (Table 2).
Another step in ensuring effective POPM is identification of the factors increasing and reducing postoperative pain, planning nursing interventions and implementation of pain management. In studies performed on the issue, activities such as getting out of bed, coughing, positioning, moving, and dressing of the incision site after surgery are reported to cause pain (Patanwala et al., 2018; Ramia et al., 2017; Yılmaz & Gürler, 2011). As in literature, in the present study, patients experienced pain while getting out of bed, positioning, and coughing and during dressing of the incision site, and pain intensity increased in the majority of the patients when moving and after the effects of analgesics wore off. Given the conditions causing postoperative pain at the clinics where the study was conducted, pain management was not planned before the patient got out of bed or he or she was positioned and so on; the majority of patients experienced pain in these conditions, which shows the importance of timely and effective pain management planning in reducing painful conditions.
Pain management is one of the most important roles of nurses working in surgical clinics (Vatansever & Akansel, 2014). In surgical patients, untreated and unmanaged pain can cause fatigue; thus, the assessment of postoperative pain and management of the pain is the most important nursing intervention (Frodin & Stomberg, 2014). The score the participants gave for the quality of care given for pain relief during the postoperative period was higher than the average (Table 3). In literature, the patients’ satisfaction with pain management was also high: 7.4 of 10 (Juszczak et al., 2016; Patanwala et al., 2018; Vatansever & Akansel, 2014). In studies conducted to assess the quality of pain management, although one third of the patients experienced more pain than they expected, 90% of them rated their satisfaction level as moderate to high (Magidy et al., 2016; Subramanian et al., 2016). Patient satisfaction depends on patient perceptions about health care or meeting the expectations of the patients (Aslan et al., 2018). Consideration of postoperative pain as normal and unavoidable by the patients (Brown et al., 2013) and postoperative caring attitudes toward patients may positively influence patient satisfaction (Darawad et al., 2014).
In the Magidy et al. (2016) study, the quality of pain management in acute (n = 160) and elective surgery patients (n = 140) was generally found to be low. In the Juszczak et al. (2016) study, the level of quality of care of postoperative pain was found to be high. In the present study, it was observed that the patients should be given education about pain management before and after the operation, that the evaluation of pain severity showed that the quality of care was low, and that the quality of care the nurses provided during the evaluation and implementation of pain management was acceptable (Table 4). In the present study, although the score for the general quality of care was high, the mean scores for the scale items indicated that the quality of care was acceptable or low. In clinics where the study data were collected, although there were no pain management guidelines or health care standards and the rate of use of opioid therapy was low, the mean scores for the quality of care and satisfaction were high, probably because 98% of the patients waited less than 10 minutes to receive pain treatment.
Pain management practices in surgical clinics are a factor affecting the quality of nursing care for postoperative acute pain. Based on the level of postoperative care, nine questions were assessed as “acceptable” and five questions were assessed as “low level of postoperative pain management.” None was assessed as “high level of postoperative pain management.” According to subscales, the level of postoperative care, nursing interventions, and environmental subscales of the SCQIPP were at an acceptable level, but pain management subscales of the SCQIPP were low. None was valued as good (Table 3). It is important in the quality of pain management and patient comfort for nurses to manage pain by using advanced care procedures. In addition, and contrary to Juszczak et al. (2016) results, in the present study, POPM quality was found to be low. This may be due to different POPM procedures. In the hospital where the work was conducted, no pain management protocol was applied. These results suggest that there is a need to develop care protocols for pain management in hospitals.
The guidelines published by the APS (1995) stated that health professionals should educate patients and their families about pain management individually and should prepare plans for the care given during preoperative and postoperative pain management. One of the quality indicators of pain management is to provide patients with pain management training (Best et al., 2018; O’Donnell, 2018; Subramanian et al., 2016). The present study determined that the patients who were instructed about the operation preoperatively obtained high scores in the SCQIPP and its pain management subscale (Table 4). In their study, Innis et al. (2004) investigated the effect of patient education on satisfaction with pain management and found that education increased patient satisfaction even though there was no change in the patients’ pain intensity. These results suggest that educating a patient in pain management increases the quality of care regarding pain management.
Limitation of the Study
This study has some limitations. The study sample size compromised a small number of patients from only a single state hospital and nonrandom, and, therefore, findings are not generalizable to all patients undergoing surgery. There is a need for further studies in a larger sample. Another possible limitation is that the study was descriptive and cross-sectional. Therefore, in this study, only the quality of pain management and patient satisfaction were identified in the study.
Conclusion
The results of the present study revealed that the majority of the surgical patients experienced tingling pain, that they experienced more pain while getting out of the bed, that moving increased postoperative pain, and that rest and analgesics relieved the pain. In the present study, although the score for the general quality of care in pain management was high, the scores for the assessment of care, education about postoperative pain relief, pain management and the quality of nursing care were low.
Implications for Practice
These results suggest that health care, including measurable, applicable quality indicators, should be planned and evaluated to maintain professional nursing services, to achieve POPM and to relieve pain. Management of postoperative pain in surgical patients is needed to enhance patient outcomes. To increase satisfaction with the quality of care in POPM, it is necessary to determine patients’ preoperative pain management–related educational needs, to plan the education for each patient individually, and to include this education in standard nursing care activities.
Footnotes
Acknowledgements
The authors acknowledge the voluntarily contribution of the patients who participated in this study. We also thank Sedat Yüce for her suggestion regarding the statistical methods.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.