
Abstract
In line with the current psychological approach to health in general, mental health is perceived not only as the absence of psychopathological disorders, but also the presence of well-being. The study contributes to the identification of possible sources affecting mental health in adolescence. This cross-sectional study focuses on the role of personality traits, dispositional optimism, and perceived social support in predicting mental health in adolescence. Mental health was assessed using Mental Health Continuum, personality traits using Big Five Inventory, dispositional optimism using Life Orientation Test—Revised and social support by Close Relationships and Social Support Scale. The research sample consisted of 1,239 respondents aged 12 to 19 years (mean age 15.56 years), 54.3% females and 45.7 % males. Sequential regression analysis revealed that demographic variables and personality characteristics together explained 33.5% of mental health variance, the strongest predictors being extraversion and neuroticism. Including dispositional optimism and perceived social support resulted in a significant increase of the explained variance. All predictors together explained 46.0% of the mental health variance.
Introduction
Current Euro-American society places strong emphasis on health, supporting active health care and protecting all health components: ecological, biological, psychological, and social health (Ansseau et al., 2004). Increased interest in mental health is driven by high prevalence of certain mental disorders, particularly depressive, anxiety, and neurotic disorders, which among other things, leads to spiraling health care costs (Murray et al., 2012). In 2014, Baxter et al. (2014) published a systematic overview of the scientific literature on the incidence of depressive and anxiety disorders. Based on the overview, they suggest that there is a general increase in the psychological load in the contemporary achievement-oriented world. Between 1990 and 2010, the number of clinical cases increased by 37%. Unfortunately, the increase in the incidence of mental disorders is true for the Czech Republic as well (Dzurova et al., 2000).
While the incidence of mental disorders is on the rise, the age of onset is gradually shifting toward younger age (Belfer, 2008). First onset of mental disorders usually occurs in childhood or adolescence (Kessler et al., 2007), with adolescence (and the period of transition to young adulthood characterized by an increasing number of stressful situations (Racic et al., 2017)) representing an especially risky period (Uhlíková, 2012). The psychosocial consequences of mental health problems in adolescence may have detrimental effects on an individual’s transition into adulthood (Lee & Loke, 2005), which emphasizes the importance of research in the field of mental health in adolescence.
Mental Health
Mental health is defined as the presence of positive well-being together with the absence of psychopathological disorders (Lamers et al., 2012). This characterization is in accordance with the definition of mental health by the World Health Organization (WHO, 2005), taking into account the concept of mental health as seen by Keyes (2005), who defined mental health as a complex state given by the presence or absence of symptoms of mental health and mental disorder. Since the term mental health has long been used primarily in relation to mental disorders, Keyes (2013) proposed another term: positive mental health. The above conception of mental health emphasizes the positive aspect of psychological functioning, which is not concerned with assessing the presence or absence of psychopathology. In this perspective, mental health is rather operationalized as the level of flourishing, which is reflected in an individual’s psychological, emotional, and social well-being. The importance of research into positive mental health was underlined by research findings of Hoyt et al. (2012) and by the results of a longitudinal study conducted by O’Connor et al. (2017), which confirm that the level of positive mental health in adolescence is related to the level of mental health in adulthood.
Role of Personality
The WHO (2016) defines personality characteristics as one of the three main health-determining categories. The role of personality characteristics in relation to maintenance, loss, and restoration of one’s mental health has been explored as well (Sadeghi et al., 2015), but this relationship has not been satisfactorily verified in relation to adolescence, particularly with respect to the concept of positive mental health. Yet, adolescence is generally considered a key developmental period, during which many important habits and attitudes toward one’s own mental health and strategies in health supporting/threatening behavior are created. In this process, personality traits play an undoubtedly very important role.
A suitable theoretical framework for understanding the nature of the relationship between mental health and personality appears to be the Big Five theory, which comprises the following factors: extraversion, agreeableness, neuroticism, openness to experience, and conscientiousness (McCrae & Costa, 2008). In the last decades, this five-factor model has become a widely accepted framework for describing and explaining personality traits. In terms of mental health, based on research studies, the pivotal factors seem to be neuroticism, extraversion, or conscientiousness (Qi et al., 2016). High level of neuroticism is associated with higher risk of mental disorders (Hudek-Knezević & Kardum, 2009), while the correlation of lower levels of conscientiousness with high levels of neuroticism leads to subjective higher measure of stress (Carver & Connor-Smith, 2010). In psychological literature, two key personality traits tend to be used in connection with mental health, which can probably be regarded as central: neuroticism and extraversion (Otonari et al., 2012). These characteristics seem to play the most significant role in influencing, through biological and behavioral mechanisms, the affective components of mental health (Lamers et al., 2012). Among other personality traits, higher levels of neuroticism is typically connected with worsen mental health (Friedman et al., 2010) and, as such, neuroticism is discussed as a risk factor for physical and mental health. On the contrary, extraversion together with agreeableness are usually linked to higher levels of good health (Jokela et al., 2013), including mental health (Carver & Scheier, 2014).
Role of Dispositional Optimism
Dispositional optimism is a psychological trait associated with both physical and mental health. It is viewed mainly as a health-protective characteristics with respect to both mental and physical health. It therefore occupies a significant position among those psychological factors considered health producing (Egger, 2013). Carver and Scheier (2014) define dispositional optimism as a generalized expectation that good rather than bad things will happen in one’s life. And it is precisely positive and negative expectations regarding the future that are important with respect to vulnerability to mental disorders, in particular, mood and anxiety disorders, as well as to physical illness (Conversano et al., 2010). Optimistic individuals are more likely to have protective attitudes, they are more resilient to stress and are inclined to use more appropriate coping strategies (Carver & Scheier, 2002).
Adolescence is a period of rapid changes, in which emotional and behavioral difficulties commonly occur. An increasing amount of evidence is pointing to the fact that optimism plays a major role in physical and mental health of adolescents. Dimensions of dispositional optimism turned out to be the strongest set of predictors of positive mental health in adolescents (Nes & Segerstrom, 2006). Dispositional optimism can affect mental health in varying ways, through its impact on self-efficacy, anxiety, coping, healthy lifestyle, risk perception, and so on (Junbo et al., 2015).
Role of Social Support
Another important factor related to mental health, particularly in adolescence, is the amount and quality of social support provided by parents and peers (Mahalik et al., 2013). Social relationships can be considered a highly important aspect in adolescent life, helping adolescents to find and assert their place in society and playing many other important roles in an individual’s transition into adulthood (Kenny et al., 2013). As has been shown by a number of studies, these effects can have both positive and negative aspects (Cheng et al., 2014). The relationship between social support and indicators of mental health has been the subject of numerous research works, which highlight particularly the role of low levels of loneliness combined with high levels of social support, as significant predictors of positive mental health. Low social support levels, on the contrary, are typically the strongest predictor of anxiety and depression (Van Lente et al., 2012). The importance of the role of social support was confirmed by the results of a study by Umberson et al. (2010), who report positive effects of social support on both mental and physical health. The authors view social support as an inseparable part of healthy lifestyle not only in adolescence but throughout an individual’s life. Seligman et al. (2012) stresses the importance of social support as a functional factor of mental health and agrees with Friedman et al. (2010) that mental health, personality, and social relationships are inseparable.
Problem Statement
In line with the current psychological approach to health, which considers it important to link the individual aspects of health together and view them as a whole (Coleman et al., 2007), this article maps the role of basic personality characteristics, dispositional optimism, and perceived social support in predicting mental health in adolescence. More specifically, we suggest that neuroticism is negatively associated with mental health, while the relationship between mental health and extraversion, agreeableness, optimism, and the quality of social support lies in the positive direction.
Methods
Procedure
The data in this study were collected using paper/pencil questionnaire administered in school settings during academic year 2014/2015. The schools that agreed to participate in this project were intentionally sampled to cover the variability in school types. The administration of the questionnaire took one class period. The schools received feedback on their students’ performance (e.g., via school counselors).
Research Sample
The questionnaire was administered to 1,297 respondents. Fifty-eight participants did not provide sufficient number of responses to compute individual scale scores (more than 1/3 of scale items were skipped) or other study relevant information and were removed from the sample. The research sample consisted of 1,239 respondents aged 12 to 19 years (mean age 15.56 years, SD = 2.14). Description of the sample is provided in Table 1.
Sample Characteristics.

Instruments
Mental Health Continuum Short Form (MHC-SF) (Keyes, 2009) is a shortened, 14-item version of the Mental Health Continuum Long Form questionnaire. The respondents rate each item from a list of feelings on a 6-point response scale (0–5) with respect to the frequency of occurrence in the last month. Those participants achieving higher scores can be considered flourishing in life, whereas those with low scores can be viewed as languishing in life. According to the author, three subscales can be distinguished: Psychological well-being, emotional well-being, and social well-being. In this study, we used only the overall score, because the scale can be assumed to be unidimensional (the ratio of first-to-second eigenvalues was greater than 5). Cronbach’s alpha was 0.90 for the whole scale.
The Big Five Inventory (BFI) (John et al., 1991) comprises the following basic personality factors: extraversion, neuroticism, openness to experience, agreeableness, and conscientiousness. The BFI is a 44-item self-report inventory designed to measure the Big Five dimensions. BFI utilizes short sentences or phrases, which represent prototypical markers of the model’s dimensions. The participants record their answers on a 5-point Likert-type scale, where 1 means strongly disagree and 5 strongly agree. An extensive validation of the method in relation to the Czech sociocultural environment showed a sufficient level of psychometric properties of the adapted version (Hřebíčková et al., 2016). In our study, Cronbach’s alpha was 0.78 for extraversion, 0.67 for agreeableness, 0.74 for conscientiousness, 0.80 for neuroticism, and 0.71 for openness.
Life Orientation Test—Revised (LOT-R) (Scheier et al., 1994). This method focuses on assessing individual differences in generalized pessimism and optimism. The shortened and revised version of the measure, Life Orientation Test—Revised (LOT-R), uses six items with 5-point rating scale (1–5). The authors report high internal consistency of the method as well as good stability over time. We verified the internal consistency of the scale using our sample; Cronbach’s alpha was 0.69.
Close Relationships and Social Support Scale (Cefai & Camilleri, 2009). The scale is a part of an extensive set of tests, which was designed for the purpose of assessing the level of mental and physical health and social and emotional well-being in university students. In our study, we used the items focused on the overall satisfaction with relationships (with a 4-point response scale ranging from “highly dissatisfied” to “highly satisfied”), perceived loneliness (“Do you sometimes feel lonely?” with possible responses “Yes, very often; quite often; rarely; no, never”), and number of close friends (“none,” “one,” “two or three,” “more than three”). These three indicators were standardized and averaged and used as a measure of social support.
Data Analysis
The relations between variables were analyzed using correlation and regression analyses. First, the relationships between variables were described using Pearson correlation coefficient. Then, a linear regression was used to predict the overall level of mental health. Given the size of the sample, statistical significance of the relationships was assessed only at the .01 level.
Results
Descriptive Statistics and Correlation Analysis
Table 2 presents descriptive statistics and correlations expressing the relationships between demographic variables, personality characteristics, optimism, social support and overall mental health.
Descriptive Statistics and Relationships Between Variables.
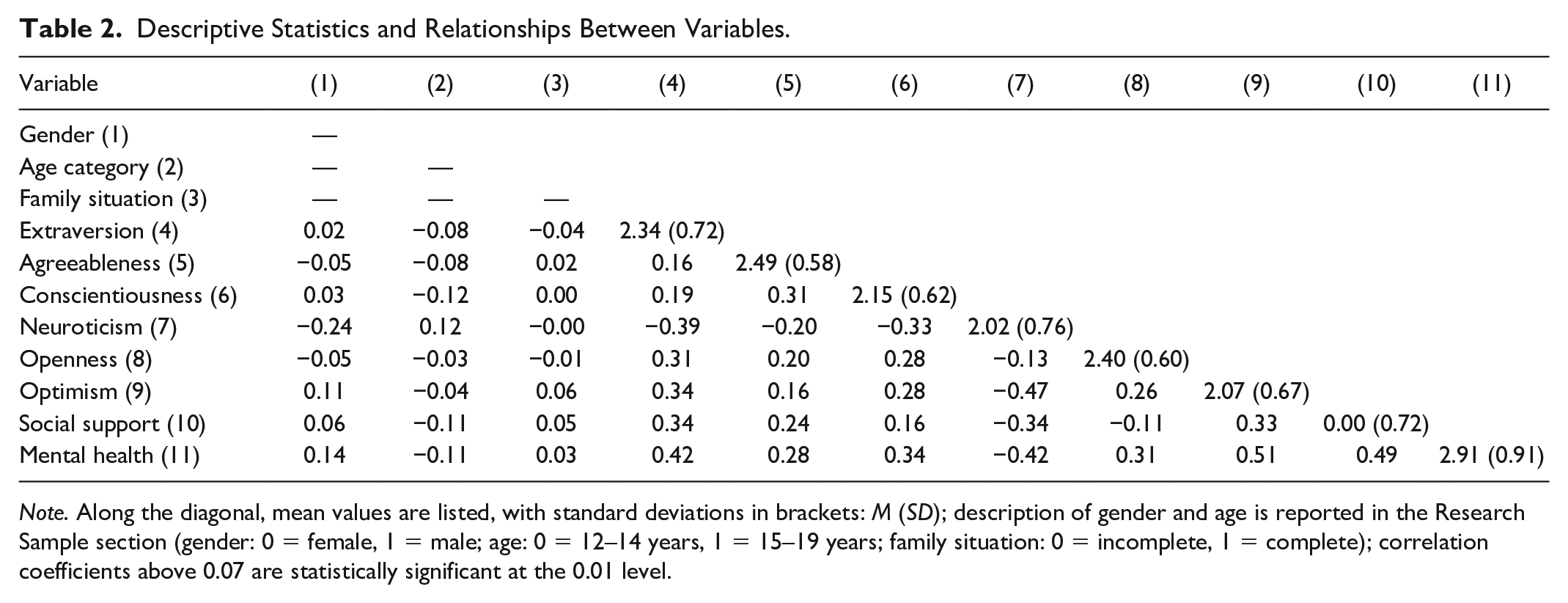
Note. Along the diagonal, mean values are listed, with standard deviations in brackets: M (SD); description of gender and age is reported in the Research Sample section (gender: 0 = female, 1 = male; age: 0 = 12–14 years, 1 = 15–19 years; family situation: 0 = incomplete, 1 = complete); correlation coefficients above 0.07 are statistically significant at the 0.01 level.
It is clear from Table 2 that the overall degree of mental health shows a relatively close relationship with all the personality dimensions, the strongest relationships being found with extraversion (r = .42) and neuroticism (r = −.42). In addition, it follows from the table that mental health is also related to dispositional optimism (r = .51) and perceived social support (r = .49).
Prediction of Mental Health Based on Demographic Variables, Personality Characteristics, Optimism, and Social Support
We used the sequential regression analysis to predict the level of mental health. The predictors were entered in three blocks: the first block consisted of demographic variables (gender, age, and family situation; variables were coded as dummy variables; gender: 0 = female, 1 = male; age: 0 = 12–14 years, 1 = 15–19 years; family situation: 0 = incomplete family, 1 = complete family); the second block consisted of the BFI dimensions; the third block contained variables reflecting the overall degree of dispositional optimism and social support. Gender, age, and family situation together explained 3.0% of overall mental health variance. Higher levels of mental health were observed in males. Moreover, late adolescents reported lower levels of mental health; family situation had no effect on mental health. Adding personality variables increased the explained variance by 30.6%. Of the demographic variables, only gender continued to have a statistically significant effect. All the personality characteristics were found to contribute to the explanation of mental health, the strongest predictors being extraversion and neuroticism. Adding variables from block 3 (dispositional optimism and social support) again resulted in a significant increase of the explained variance by 12.5%. All the predictors together explained 46.0% of mental health. The results of regression analysis are summarized in Table 3.
Prediction of the Level of Mental Health (MHC)—Results of a Regression Model With All the Predictors.
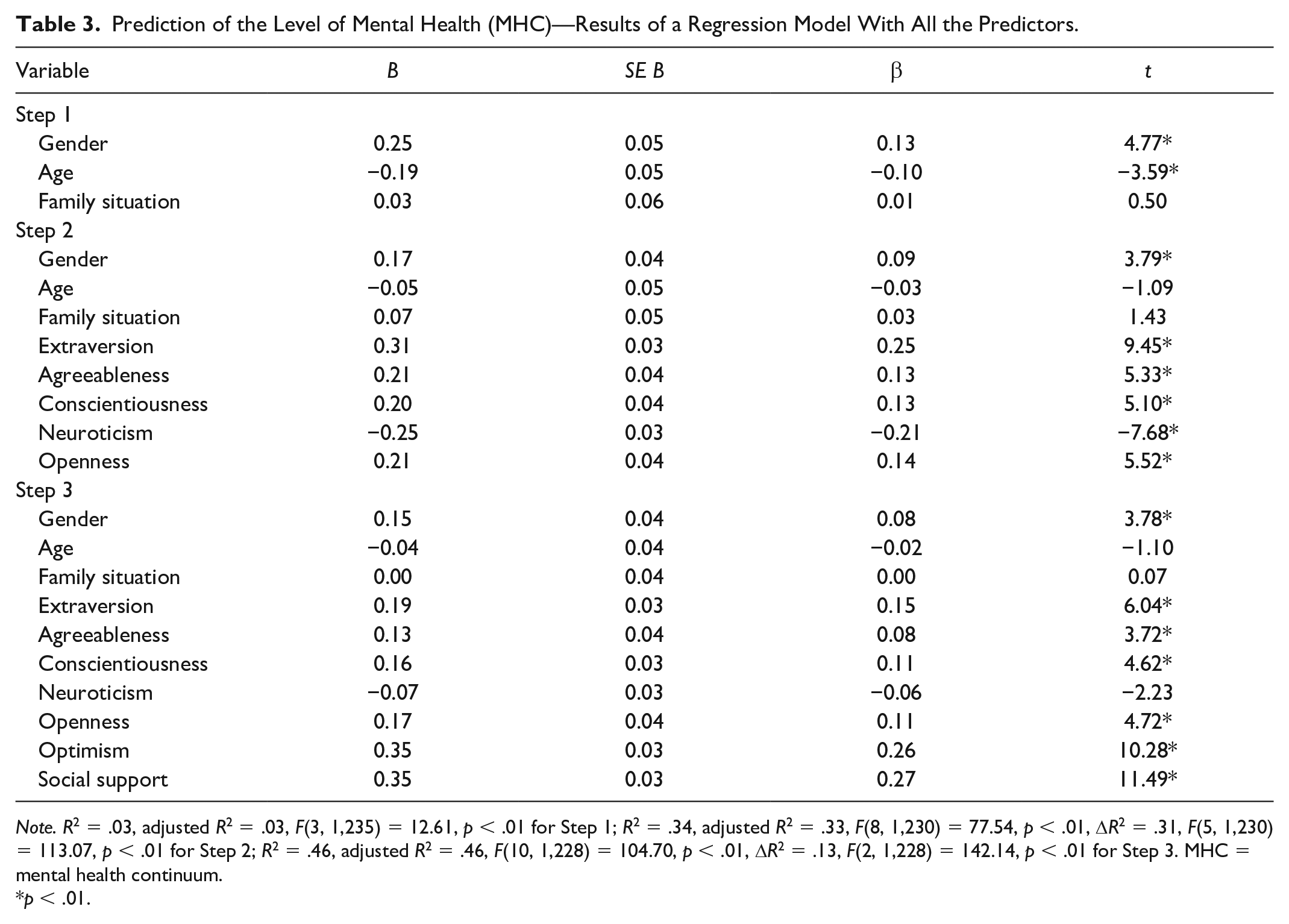
Note. R2 = .03, adjusted R2 = .03, F(3, 1,235) = 12.61, p < .01 for Step 1; R2 = .34, adjusted R2 = .33, F(8, 1,230) = 77.54, p < .01, ΔR2 = .31, F(5, 1,230) = 113.07, p < .01 for Step 2; R2 = .46, adjusted R2 = .46, F(10, 1,228) = 104.70, p < .01, ΔR2 = .13, F(2, 1,228) = 142.14, p < .01 for Step 3. MHC = mental health continuum.
p < .01.
The strongest predictors of mental health are dispositional optimism and social support. Compared to the previous step of the analysis, the effect of personality characteristics is greatly reduced. This is apparent particularly in relation to neuroticism, the effect of which, after the addition of dispositional optimism and aspects of social support, has all but disappeared. The elimination could be explained by the massive overlap of neuroticism, dispositional optimism, and social support (see Table 2).
The next step of the analysis consisted in testing the possible interaction between the effects of the predictors on mental health on one hand and gender and developmental stage within adolescence on the other hand. The interaction was tested by adding the relevant interaction components into the model. No significant increase in the explained variance of mental health was observed in either case, ΔR2gender = .00, ΔFgender(7, 1,220) = 0.78, pgender = .60; ΔR2age = .01, ΔFage(7, 1,220) = 2.12, page = .04.
Discussion
This study maps the role of demographic variables, personality, dispositional optimism, and perceived social support in predicting the state of mental health in adolescence. The results have shown that all the investigated variables play a certain role in forming and maintaining mental health. Sequential regression analysis revealed that sex, age, and family situation explained 3.0 % of overall mental health. Adding personality variables increased the percentage by 30.6%. All of the personality characteristics were found to contribute to the explanation of mental health, the strongest predictors at this stage of analysis being extraversion and neuroticism. The above is in line with the results of research studies focusing either on the same developmental stage or on the period of adulthood (Moreira et al., 2014; Otonari et al., 2012; Steel et al., 2008 and others). Lamers (2012) adds that neuroticism and extraversion seem to influence the affective components of mental health through both biological and behavioral mechanisms. The BFI may lead to a greater clarity of concepts and interpretation of the results (Chen et al., 2012). Low level of neuroticism is associated with positive emotions, lower level of anxiety or worry, with more positive cognitive approach to stressful situations, and with less negatively perceived impact of stressors (Mirnics et al., 2013). Furthermore, emotionally labile individuals view stressors as more threatening and they consider their situation coping resources as less effective (Carver & Connor-Smith, 2010). In addition to the above, neuroticism also plays a role in subjective perception of symptoms, where more emotionally labile individuals experience aggravation, which ends up negatively affecting the level of perceived stress (Hřebíčková, 2011). The high level of this personality trait is also connected with increased occurrence of health-threatening behavior (e.g., using addictive substances), which is very significant in the context of the development of risky forms of behavior during the key developmental period of adolescence. Previous research studies have indicated a connection between higher level of extraversion and active coping strategies in the form of active problem-solving (Karimzade & Besharat, 2011), thus making extraversion an important variable in the life of an individual coping with stressful situations. Research results have shown that extraversion also has a positive effect on obtaining social support or enlisting help.
Adding dispositional optimism and social support resulted in another significant increase of the explained variance of mental health by 12.5%. Thus, all the predictors combined explained 46.0% of overall mental health. At this step of sequential regression analysis, the strongest predictors of mental health were dispositional optimism and social support, while the effect of neuroticism was significantly reduced. It can be ascribed to a massive overlap being found between neuroticism, dispositional optimism, and social support. According to Suls and Martin (2005), neurotic people are more sensitive to negative effects, generally experience more negative life events, which are interpreted in more negative terms, and their negative feelings tend to spill over from one life area to another, which is a description that fits to a lack of dispositional optimism as well (Monzani et al., 2014). In the same manner, Kardum and Hudek-Knezevic (2012) note that the strong overlap between optimism measured by Life Orientation Test and neuroticism has been confirmed by a number of studies (Sharpe et al., 2011). Like neuroticism, dispositional optimism also appears to be reflected in perceived social support, which has been confirmed by the results of other studies (Orejudo et al., 2012; Sumer et al., 2009).
In the context of mental health of adolescents, we consider it important to mention the results of a study by Kawachi and Berkman (2001), who found that perceived social support can play an important role in maintaining mental health. Similar importance can be ascribed to findings by Jones et al. (2011), who state that loneliness predicts indirectly affected self-harm behaviors and suicidal thoughts through depression and behavior problems. No interaction has been found between any of the predictors of mental health and either gender or developmental stage within adolescence. The impact of these predictors was not found to undergo any significant changes across different stages of adolescence; nor was it found to be affected by gender.
A limitation of this study should be noted. The main limitations of the study are associated with self-selection bias both on the level of participating institutions and on the level of individual respondents. We aimed to cover different types of educational institutions, from middle schools to high schools, but only the schools, which actively agreed to participate in the research were included. The same applies to the participating students, who had the option to refuse filling out the questionnaire.
In summary, mental health in adolescence is closely related to psychological and social characteristics of adolescents. Besides basic personality traits, dispositional optimism, and social support also play an important role in maintaining mental health.
Footnotes
Ethical Approval
Approval for the project was received from the Research Ethics Committee of Masaryk University. Informed consent was obtained from all participants or their legal representatives.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Czech Science Foundation (project no. GA13-19808S).