
Abstract
Despite older adolescence being a risk period for the development of mental health concerns, mental health service engagement is low among 16- to 18-year-olds. As therapeutic attendance is linked to clinical outcome, it is important to understand engagement in this population. There is a paucity of research looking specifically at the older adolescent engagement phenomenon. Previous qualitative research into adolescent experiences has provided rich and detailed results. Interpretative phenomenological analysis was chosen as the methodological approach. Ten 16- to 18-year-olds were recruited from two London-based child and adolescent mental health services. Each young person was interviewed to understand his or her personal experience of engaging in mental health services, and associated engagement barriers and facilitators. Interviews were transcribed and underwent analysis. Analysis revealed ten subthemes subsumed within four superordinate themes: engagement begins at help seeking, strength of inner resolve, evolution of the self and in the clinic room. Themes are discussed in detail. Conclusions are drawn in relation to previous theory and research. When considering 16- to 18-year understandings of the engagement phenomena, key elements include clinician and service developmental appropriateness, negotiation of developmental tasks in relation to engagement, experience of the physical building environment, and awareness of service policy. Suggestions for clinical practice in relation to engagement facilitators and threat are made, and recommendations for future research proposed.
Introduction
Adolescence is thought to be a risk period for the development of mental health concerns (e.g., Vyas, Birchwood, & Singh, 2015) with older adolescence/early adulthood seeing a significant increase in symptomology (Murphy & Fonagy, 2012; Royal College of Psychiatrists, 2012). This occurs alongside reduced mental health service use. A large proportion of service “dropouts” occur around 16 to 18 years old (Singh, Paul, Ford, Kramer, & Weaver, 2008). Traditionally, child and adolescent mental health services (CAMHS) provide interventions for young people up to 18 years. To ensure appropriate service provision, policy suggests CAMHS are responsive to client’s developmental stage (Department for Children, Schools and Families [DCSF] & Department of Health [DoH], 2008) and individual need (DoH, 2015).
Engagement in services may be an important part of effective mental health treatment (YoungMinds, 2014). Elements hypothesized to be part of engagement (e.g., King, Currie, & Petersen, 2014), such as the therapeutic relationship (Shirk & Karver, 2003), may be linked to treatment outcome. For older adolescents, service engagement could be a challenge (Royal College of Psychiatrists, 2012). Alongside experiencing mental distress, they may also be faced with societal (e.g., stigma; Eisenberg, Downs, Golberstein, & Zivin, 2009), familial (YoungMinds, 2006), and developmental (Erikson, 1968) pressures. In addition, 16 to 18 years is a potential time of transition between CAMHS and adult mental health services (AMHS), which may impose its own challenges (National Institute for Health and Care Excellence [NICE], 2016; Singh, Evans, Sireling, & Stuart, 2005; Singh et al., 2008).
Despite this, little is known theoretically and specifically about 16- to 18-year-old engagement. Definitions have been proposed for children, families, and the whole adolescent age range (e.g., Cunningham, Duffee, Huang, Steinke, & Naccarato, 2009; Staudt, 2007), which go beyond the definition of “merely turning up” (Gopalan et al., 2010) or “dropping out” (Johnson, Mellor, & Brann, 2008). More comprehensive definitions incorporate multiple elements such as behavioral (e.g., attendance) and attitudinal (e.g., emotional investment in treatment) components (Staudt, 2007), as well as considering the facilitating role of the therapeutic relationship (see King et al., 2014, below). However, definitions lack consensus (Kim, Munson, & McKay, 2012), and are not specific to the older adolescence. Help-seeking definitions also incorporate elements of engagement, such as seeking professional help (e.g., Rickwood, Deane, Wilson, & Ciarrochi, 2005), meaning the overlap between the two is apparent but undefined. Theoretical progress may be hindered because of unclear definition (Drieschner, Lammers, & van der Staak, 2004).
Models applicable to adolescent engagement are limited but some have been developed. King et al. (2014) proposed a child and adolescent motivational model. This focuses on ongoing engagement within treatment, from a therapeutic relational perspective, considering hope and confidence to be key. Both client and therapist bring emotional, behavioral, and cognitive elements to engagement, suggesting responsibility for engagement is not solely with one party. This model is not specific to older adolescents, and the fluctuating nature of engagement (Donnellan, Murray, & Harrison, 2012) is not accounted for.
Broome, Joe, and Simpson (2001) developed a model for young people who experience substance misuse. Multifaceted elements of engagement are incorporated such as “background factors” (e.g., family), treatment readiness, and session attributes (e.g., therapeutic involvement). The generalizability of this model outside of a substance-misuse population may be limited. Barriers to treatment, for children, adolescents, and their families, have also been considered. The ecological point of view model (McKay, Gonzales, Stone, Ryland, & Kohner, 1995), coming from a family therapy perspective, suggests that barriers can exist at multiple levels (e.g., individual, community), acknowledging the role of the “ecosystem” in engagement. The Barriers to Treatment Model (Kazdin, Holland, & Crowley, 1997) proposes difficult familial relations with therapists may contribute to treatment termination. These models highlight the role of families in engagement; however, they do not focus on the unique experiences of 16- to 18-year-olds, where families, communities, and so forth may be positioned differently. Research suggests adolescents may prefer peer support (e.g., Raviv, Raviv, Vago-Gefen, & Fink, 2009). Indeed, peers and perceived impact on self-esteem (e.g., threats to self-esteem model; Fisher, Nadler, & Whitcher-Alagna, 1982) may influence engagement.
The above models were developed through a process of scoping review, interview through predetermined outcome measures, or interview with parents (see Broome et al., 2001; Kazdin et al., 1997; King et al., 2014; McKay et al., 1995). It appears consultation with adolescents was absent. These conceptualizations are markedly adult centric in understanding, and, therefore, lack an adolescent-specific phenomenological focus. Attempting to understand young people through adaptations of developmentally inappropriate models may hinder theoretical progress (Weisz & Hawley, 2002).
Empirical research related to the adolescent engagement phenomenon has been extensive. However, this tends to focus on individual elements related to engagement, such as beliefs and expectations (e.g., Rickwood, Deane, & Wilson, 2007; Ronzoni & Dogra, 2012; Watsford, Rickwood, & Vanags, 2013), satisfaction (McCann & Lubman, 2012), interventions (see Kim et al., 2012, for review), disengagement (e.g., Schimmelmann, Conus, Schacht, McGorry, & Lambert, 2006), or role of family (see Gopalan et al., 2010, for review), rather than engagement in its entirety from the adolescent perspective. The closed, measure-led, and adult-centric nature of these studies may have limited exploration of the engagement phenomena beyond that prescribed by the selected questionnaires and the research investigators. Investigating older adolescent understandings of engagement as a whole, including the barriers and facilitators suggested above, from the young person’s perspective (YoungMinds, 2005), may allow for a deeper exploration, and understanding.
Some related research has adopted a more adolescent-led approach. These studies tend to use a qualitative methodology and have generated interesting and rich results. Harper, Dickson, and Bramwell (2014) investigated young people’s experiences of a 16- to 18-year-old mental health service as a whole. Themes emerged around young people valuing therapeutic relationships and the service meeting developmental needs. Adolescent understandings of engagement experiences were not explicitly discussed. Bury, Raval, and Lyon’s (2007) interpretative phenomenological analysis (IPA) investigation looked at adolescent experiences throughout a course of psychoanalytic psychotherapy. Engagement themes were evident but not explored in depth. The article suggested paying attention to client views of psychotherapy, and issues around control and power might help improve initial engagement. This study focused on one therapeutic modality and did not take into account wider issues such as service provision, which may also affect engagement (Munford & Sanders, 2016).
Using IPA as part of a mixed-methods investigation, Kapur et al. (2014) looked directly into service engagement among two young people who experienced voice hearing, and their parents. Superordinate themes included battling with mental health services and frustration with received care. However, one participant was 11 years old, and parent’s experiences were included, meaning the study was not wholly older adolescent specific. In addition, the focus was limited to one specific mental health presentation. As illustrated, the use of qualitative methods may facilitate in-depth and rich investigations to occur (Smith, Flowers, & Larkin, 2009), including when recruiting adolescent participants (O’Reilly & Parker, 2014).
To date, in-depth exploration of 16- to 18-year-old understandings of their service engagement experiences, facilitators, and barriers, has not been conducted. Research into older adolescent-specific understandings will contribute to a lacking evidence base. To ensure services are responsive to the population they serve, it is essential to understand the unique needs and views of the targeted client group. Investigation could contribute to the effective development of older adolescent tailored services, which may positively affect therapeutic outcomes. By engaging young people effectively in services, we may be able to prevent more serious and enduring problems later on in life (Birchwood & Singh, 2013).
Research Aims and Questions
The need for further investigation is highlighted by three coexisting issues: the rise in mental health concerns in older adolescence, the high service drop rate at this age, and the paucity of research into 16- to 18-year-old engagement. The current study aimed to explore older adolescent sense making of their engagement experiences, barriers, and facilitators, to contribute to a sparse understanding. Research questions were as follows:
Method
Research Design and Methodology
To aid in-depth exploration of the 16- to 18-year-old engagement phenomena, a nonexperimental, descriptive design was chosen. Due to the paucity and “adult-led” nature of previous research, and taking example from prior study designs that generated rich data, a qualitative methodology was used.
IPA (Smith, 1996) was chosen as the methodological approach. Informed by philosophical understandings of phenomenology, hermeneutics, and ideography (Smith et al., 2009), IPA enables insight to be developed into specific subjective meanings and interpretations people make of an experienced phenomena. This meant in-depth understanding of the 16- to 18-year-olds idiosyncratic sense making of their engagement experience could be generated.
Participants
Inclusion and exclusion criteria were developed to facilitate recruitment of a homogeneous sample (Hefferon & Gil-Rodriquez, 2011) while ensuring an understanding of engagement could be ascertained across adolescent experiences. The reason for focusing on the 16- to 18-year-old stage is that this is the period, when societally, adolescents begin to be defined as “adult” and, alongside this, separation from caregivers is an increasingly prominent issue. It is, therefore, important to understand how this relates to engagement with services, especially as previous models of help seeking/engagement (also mentioned in the “Introduction” section) have highlighted the importance of caregivers in accessing help. Research has also suggested that there is a shift developmentally, across adolescence, when it comes to help seeking/engagement (Rickwood, Mazzer, & Telford, 2015).
Inclusion criteria were as follows:
between 16 and 18 years old and
engaged with mental health services at interview. Engagement was defined as having been offered, and was attending appointments (e.g. McKay & Bannon, 2004), for any length of time.
Exclusion criteria were as follows:
active psychosis,
significant developmental delay, and
significant risk issues
Ten participants (Table 1) were recruited from two CAMHS services in London. All adolescents approached were interviewed and none ceased participation in the study. A small number of participants allowed for in-depth, rich data gathering and analysis. The sample size was in line with recommendations (Smith et al., 2009) and commensurate with previous IPA research (e.g., Colton & Pistrang, 2004; Huws & Jones, 2008; Roose & John, 2003).
Participant Pseudonyms and Their Dominant Themes.
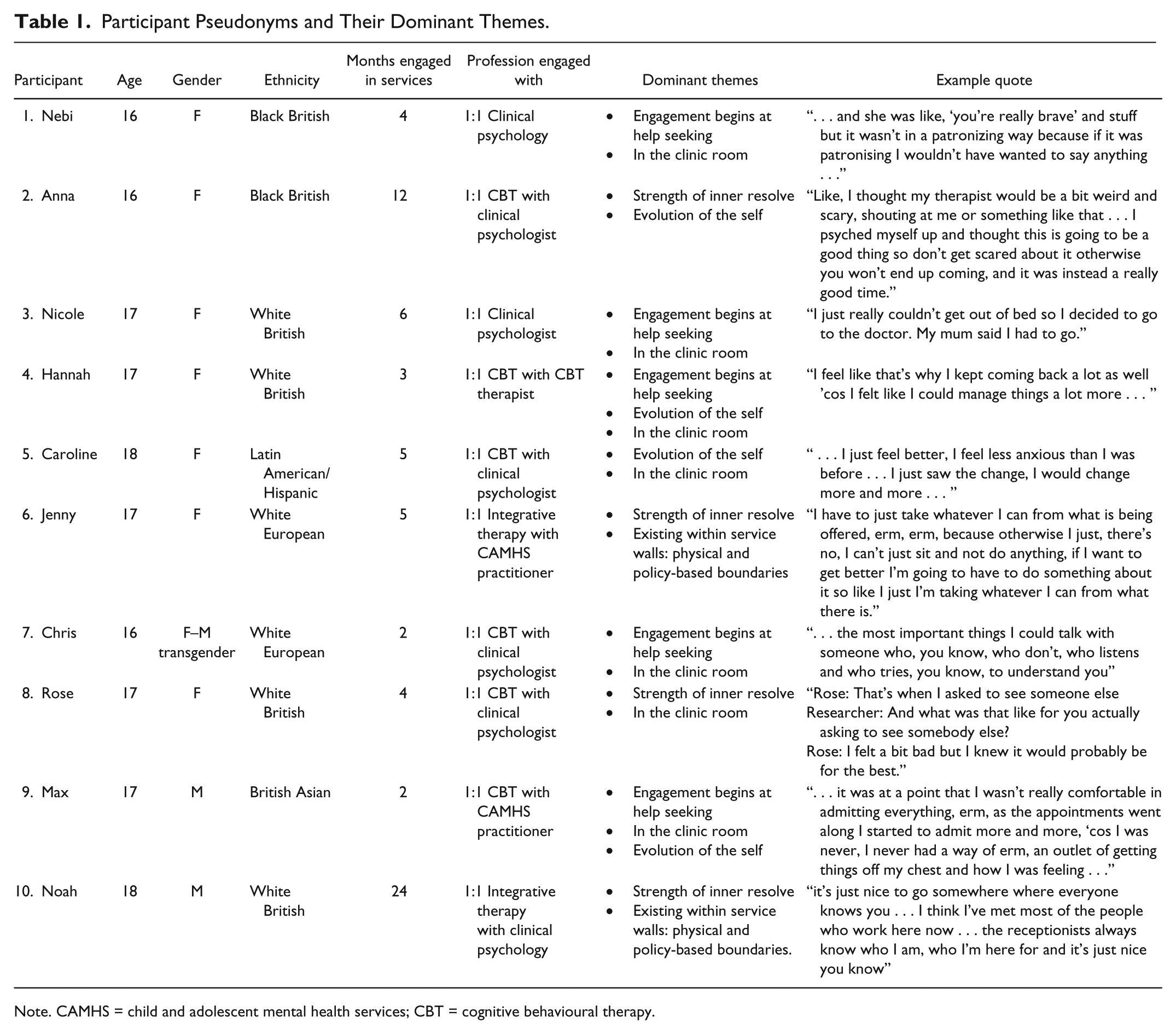
Note. CAMHS = child and adolescent mental health services; CBT = cognitive behavioural therapy.
Ethical approval
Ethical approval was requested and granted by an NHS Research Ethics Committee. Research and development, and CAMHS research approval, was granted by the recruiting NHS Trust. The British Psychological Society (BPS; 2013) code of human research ethics was followed.
Risk precautions
All interviews took place during clinic hours and the researcher familiarized themselves with service risk protocol. Participant’s clinicians were made aware of interview timings. Due to the potentially sensitive nature of the interview content, participants were informed of available support if they became distressed after leaving the service building.
Recruitment
Recruitment took place over 6 months. The researcher advertised the study in team meetings. Participants who met inclusion/exclusion criteria were identified by their clinician, and invited to take part at their next therapy session. If the adolescent showed interest, they were asked by their clinician to provide verbal consent for their contact details to be passed on to the researcher. Initial contact was made by telephone. Participants were invited to attend an introductory session (after a therapy session for participant ease) to read through the participant information sheet (PIS) and ensure they understood enough about the study to make an informed decision to participate. This was ascertained by asking them to repeat back what they understood about the study and their participation. If this was demonstrated, participants were invited back for a second meeting to sign the consent form and be interviewed. All participants demonstrated understanding and were invited back. A £10 high street voucher was given for participation.
Interviews
Data collection was via 1:1 semistructured interview. This provided a tentative framework but allowed for open conversation about the engagement phenomena, encouraging the participant to set the parameters of the discussion. The interview questions revolved around the following key areas: the young person’s experience of coming to the service; what they felt helped them to keep coming back and what would make them not want to attend the service. To ensure adolescent understanding of the schedule, PIS, and consent form, a group of five 16- to 18-year-olds, from a local school, were consulted. Two CAMHS-based clinical psychologists reviewed the final schedule to ensure relevance to the research questions. At the beginning of each interview, participants were reminded their participation was voluntary and were free to leave at any time. Interviews were audio recorded, transcribed for analysis, and anonymized. Interviews lasted between 30 and 65 min.
Analysis
Transcripts were analyzed following IPA protocol (Smith et al., 2009). To become familiar with the data, transcripts were read while listening to the audio recording. This allowed for linguistic or verbal nuances to be ascertained. Transcripts were then reread to ensure full immersion in the data, gathering an overall understanding of how different sections were connected and emerged.
Alongside the data, detailed notes were made on descriptive, conceptual, and linguistic understandings and explorations. The hermeneutic cycle was experienced as interpretations were made on participant understandings of their engagement experience, while remaining close to the original meaning.
The initial noting was read through closely and themes developed. These emerged by focusing on discrete chunks of data, while keeping in mind the interview as a whole. The developed emergent themes attempted to reflect the complexity of the data while drawing out key ideas.
Emergent themes were typed into a word document, in chronological order. Through a process of abstraction, themes were moved around the page, drawing together related items. Emerging patterns were developed into superordinate themes. The iterative nature of analysis was experienced, returning to the original transcript to ensure superordinate themes reflected the original data.
To move onto the next transcript, ideas from the previous interview were bracketed by noting assumptions and ideas developed from the analysis. This process was repeated for all transcripts.
All emergent and superordinate themes were printed, cut out, and laid on a large surface. Themes were moved around, using the abstraction process, until patterns and commonalities emerged. The hermeneutic and double-hermeneutic cycle was experienced as higher order concepts were developed and variance among individuals noted. Concepts were typed out and quotes collected from the transcripts. Following recommendations (Smith et al., 2009), the recurrence of the higher order concepts was considered in table form. Themes that did not occur in 50% of participants, or above, were removed. Remaining overarching, and embedded themes, were retained. Smith et al. (2009) state the analytic process may continue into the writing of results. Themes were reconsidered and revised as writing continued.
Quality Assurance
To ensure quality and validity, Mays and Pope’s (2000) criteria was followed. To assess analytic reliability, investigator triangulation took place. Four transcripts were analyzed and coded separately by two research supervisors. These were checked against the original coding by the main researcher. There was no full disagreement on emergent themes. Minor discrepancies around theme meanings were discussed to ensure intercoder reliability (Yardley, 2000).
The role of prior assumptions and personal characteristics were reflected upon and discussed with a research supervisor. The impact of age difference was considered. It was observed that some participants mentioned difficulties with opening up to adults, fearing judgment. In addition, the researcher had prior assumptions, from personal and professional experience, that adolescents may have been reluctant to engage with the interview process. By participating in the interview, the adolescent was experiencing a separate engagement process with the researcher. It was wondered how this may have affected the participant, and researcher’s responses, especially in the earlier stages of the interview.
As interviews progressed, positioning and power dynamics between researcher and adolescent were noted. Reflexive conversations focused on how participants may have expressed, or altered, their opinions about clinicians or services. They may have assumed the researcher would feedback to his or her clinician, or alter his or her perception of the participant (despite being informed of the confidentiality process), giving more socially desirable responses.
Before recruitment began, a bracketing interview was conducted with a trainee clinical psychologist about personal or professional assumptions and experiences. This bracketing interview, discussion with supervisors, and keeping a research diary were used to reflect on and work with these assumptions. Following each interview and transcript analysis, notes were made, to allow for biases or assumptions to be discussed or thought through. The limitations of this process were noted (e.g., Heidegger, 1927/2010), around how possible it can be to “truly” bracket off assumptions.
Attention was paid to cases, or sections of transcripts, which “deviated” from emerging themes, by disconfirming or contradicting analysis. This aided a process of broadening and refining themes.
Results
Analysis resulted in four superordinate themes, which subsumed 10 subthemes (Table 2). Superordinate themes were engagement begins at help seeking, strength of inner resolve, evolution of the self, and in the clinic room.
Superordinate Themes, Subthemes, and Illustrative Quotes.

Theme 1. Engagement Begins at Help Seeking
This superordinate theme conceptualizes engagement as beginning at help seeking. All 10 participants discussed their help-seeking journey to aid sense making of their engagement experiences. The boundary between the two may be overlapping for adolescents.
Reliance on adult acknowledgment of distress and facilitation of professional help seeking
All participants spoke about the role adults played in acknowledging their distress and facilitating professional help seeking, marking the start of their engagement journey. Hannah “. . . explained to my mum what was happening, like, in my head and she was like, ‘I think it’s time we go to the GP and get you some counselling’ . . .” Max’s distress was acknowledged by a teacher: “she noticed I wasn’t participating as much and I was looking down . . . we had a chat in her office and she said she’d put me on the waiting list for a counsellor.” [Max]
It appears reliance on adult acknowledgment may have been important for participants in times of crisis due to uncertainty about whether their distress warranted, or how to seek, professional help. For some participants, there may have been a dilemma between negotiating independence and adult reliance, reflecting a challenging pull between adolescent-as-a-child and adolescent-as-an-adult within the initial engagement stage: I think there’s a part of every teenager really when your mum says something like “oh you need help” that’s like . . . just don’t! (laughs), erm, I think part of it was also that I was kind of worried . . . so the fact that she said it, I think it was necessary really . . . [Jenny]
Cognitive preparedness
A theme emerged around the role of participant’s “cognitive preparedness,” personal beliefs around their need for professional help (see Table 2), and their understanding of what could be gained from this. For example, Nebi understood, “. . . to make myself feel better I had to start coming . . .”
Understanding previous coping strategies were no longer beneficial played a role, for some, in developing cognitive preparedness. Jenny “came to the realisation that . . . the default thing I always fell into wasn’t working.” Hannah felt her usual “bottle it all up” strategy had become “counterproductive as you just build up all the negativeness and it all comes out crazy (laughs).”
Cognitive preparedness may potentially set the stage for adult acknowledgment and facilitation of further help seeking. Rose illustrates,
What was it like for you? [Mum] saying, I think you need to get help now?
It wasn’t that surprising, because I did.
Participants may have been reliant on an alignment between adult suggestion and their own cognitive preparedness. As seen from Jenny above, this alignment however, may be experienced as a challenging negotiation between personal cognitive acknowledgment and “the part of every teenager” that desires independence.
Theme 2: Strength of Inner Resolve
This superordinate theme relates to participants’ inner determination to “get better” [Nebi]. There was evidence this acted as a key engagement motivator, as each participant made reference, throughout the process of their sense making, to the impact their personal resolve had on their experience.
Striving against engagement threats
A sense of striving to maintain engagement in the face of “threats” came through strongly from the data. All participants identified threats they had experienced throughout the engagement process. These included mental health symptomology, engagement practicalities, and disappointments with the service.
Some participants spoke about contending with the very symptomology they were seeking help for. Despite feeling anxious, Caroline attended “because I wanted the help” and Anna “psyched [herself] up and thought this is going to be a good thing so don’t get scared otherwise you won’t end up coming.” Noah maintained engagement, despite having difficult “draining” sessions as “I’d like to be more functional and mentally healthy than I am . . .” Max explained how his depression affected his engagement experience: . . . there are times as I said when I don’t want to get better, because I’m feeling so crap, erm . . . but then there are times when I know I need to get better because this is not me, I won’t do myself justice in a way, and so coming here I guess is helping with that.
Regarding practicalities, Nebi explained she was, “determined to get help” despite finding it difficult to remember appointment times. Rose felt her initial therapist was not helping her in the way she needed, so requested to see a different clinician, despite feeling uncomfortable:
What happened when you were thinking about how to resolve this issue?
I was nervous but I felt like if I saw someone else then it would be a lot better.
Jenny spoke about feeling disappointed with the care she received. When prompted to discuss what maintained her engagement despite these experiences, she explained, I have to just take whatever I can from what is being offered . . . because otherwise I just, there’s no, I can’t just sit and not do anything, if I want to get better I’m going to have to do something about it so like I just I’m taking whatever I can from what there is.
What was striking from these data was the strength of participant’s inner striving against experiences identified as difficult, and their resolve to weather storms-of-engagement. Despite there being bias in the fact all participants were actively engaged at time of interview, few had experienced a smooth journey to be where they were. It appeared they strived to maintain their engagement through an inner sense of purpose to receive, and maintain receiving help, for their distress.
Responsibility to others
Maintaining engagement through a sense of “responsibility to others” emerged. This responsibility was mainly in relation to parents. Noah felt “bad about letting people down” when he had not attended appointments in the past, and Max initially attended, in part because, “mum and dad were, I couldn’t, you know, they urged me to go.” When Anna thought further about her reasons for engaging she realized, “part of it was for me and part of it was for my mum . . .”
Data suggested that participants responded to an awareness of the impact their behavior had on those around them, considering more people than just themselves were invested in their engagement journey. There appeared to be complexity around how reliance on parents/adults to aid engagement sat alongside the responsibility participants may have felt for them. It appeared once this noticing occurred, and professional help facilitated, participants may have then felt responsible to manage their engagement, for themselves, and for those around them.
Theme 3: Evolution of the Self
This superordinate theme relates to participant accounts of their journey through their engagement process and the sense of themselves “evolving” as this progressed.
Progression through suspense and release
Nine participants spoke about their experience of anticipation before initial attendance and the subsequent relief. What was marked within this presession build-up were the expectations participants had, mainly around anticipating the service/clinician to be “stern” [Nebi] or “not friendly” [Chris]. They also described the “anxious” [Rose] or “nervous” [Max] feelings accompanying this. Hannah explains, It was nerve-wracking to come . . . and already I was really nervous when I was in the like, erm, in the reception.
She went on to consider the thoughts behind this: I thought it was going to be a really officey looking woman who was going to talk down to me.
The time between referral and session attendance has an element of being a no-mans-land of suspense between help seeking and engagement, which was managed by some participants by either putting it “out of my mind” [Max] or “kind of losing hope” [Caroline]. Despite nervousness, two participants also spoke about “looking forward to” [Jenny] attending as they felt “excited” [Anna] about receiving help. This contributes to an idea of suspense before attendance rather than anxiety. Participants spoke about how this initial “build-up” was followed by release, describing the “relief” [Caroline, Chris, Max] felt as they began their first session. To continue following Hannah’s journey, here she illustrates this release: . . . I’m finally talking about it and having to face things rather than bottling it up, so fizzing coke bottle, and then letting it go and letting it out . . .
The commonly expressed anticipation around “formality” from the service/clinicians is interesting when considering 16- to 18-year-old engagement. This sheds light on older adolescent’s relationships to, and expectations of adults, and hints toward the complexity of this population’s engagement experience, for example, negotiating whether they are relating to adults/clinicians as independent adults themselves, or as children. This is illustrated by Caroline, discussing independence from adults, while seeing them as authority, during initial engagement suspense and release: . . . like, I feel like in general when you’re young you kind of feel like “oh I’m independent, I don’t need adults” . . . I feel like, if you, when you speak to an adult it just feels like they’re authority and they’re going to tell you off kind of thing so it’s nice when someone is friendly with you and not talking down on you . . .
Growth through familiarity and trust affect
This subtheme relates to participant’s growth as they became familiar with the engagement process. This sense of familiarity and trust appeared to be described by some participants as something felt. Chris explained how he “. . . felt support” from the service. In addition, this “. . . buil[t] up slowly, like a process . . .” [Caroline], and felt like, “. . . a natural thing . . .” [Jenny], which made it “easier to go” [Nicole]. Through this, Max explained he “started to admit more and more.” This contributes to a sense of “growth,” for example, in confidence, through the process, which encouraged participants to continue attending. For Caroline, “it just encouraged me to do it more and more.”
Trust in the engagement process appeared to develop as therapeutic gains emerged, contributing further to the idea of growth. Two participants illustrate: . . . I’ve changed my attitude quite a lot . . . I feel like that’s why I kept on coming back a lot as well ’cos I felt like I could manage things a lot more . . . [Hannah] . . . then I realized that I’m actually getting a bit better and that every time I went and then was on my own in like normal life, I just felt a little bit better. [Nicole]
This feeling of growth appeared to play an important role in the engagement experience, “feeling” like progressions were being made. Being able to tangibly see “the change” [Caroline] and “feel like I’m getting help” [Rose] was of key importance.
Negotiating as an adolescent through choice, transparency, and control
This subtheme is concerned with the negotiation, from the unique older adolescent perspective, of choice, transparency, and control, and the contradictions that come with this around autonomy and reliance on adult direction.
This can be seen in negotiating the balance between participants feeling clinicians were “. . . trying to make me do something . . .” [Max] versus, “suggestions.” For Nicole, the subtleties between this could be seen across the interview. She spoke about how clinicians “telling” her what do acted as an engagement de-motivator, however, later spoke about how “suggesting things to help” aided engagement. Nebi discussed how she doesn’t “really like being told what to do so I would probably wouldn’t have done it” but later replied,
. . . how helpful do you think it was then not being given a choice of what you had and just being told, this is what you’re going to do . . . ?
Good because I think my other therapist kind of knew me better that I knew myself . . .
Choice was also linked to perceptions of “transparency” about the thinking behind the therapeutic process, which in turn aided the participant’s sense of control over this—something that appeared important. For Rose and Max, being made aware of the usual procedure to have parents involved in early sessions gave them the opportunity to request for this not to happen. This control allowed Max to experience “. . . less stress . . . less issues.” For Noah, who was making the transition from CAMHS to AMHS, through discussions with clinicians, was clear about the process this involved, suggesting this “help[s] me adjust.” Jenny, with decisions about location of care, felt once she was made aware of the process behind this “was fine with it ’cos we talked about it so I wasn’t completely like shut out of decisions.”
Theme 4: In the Clinic Room
This superordinate theme is concerned with participants making sense of their experiences, of both therapist and therapy, within sessions.
Developmentally appropriate responsiveness
This subtheme is around how participants made sense of their engagement experiences in relation to (lack of) clinician responsiveness to their developmental stage. Participants consistently touched on themes about the perception of (not) being spoken to in a “patronizing” manner [Nebi, Noah]. These concerns were presented as “advice” to future clinicians, as explained by Max, who suggested, “make it relatable to teens” and Chris who put forward, . . . understand everything from the perspective of young people because in a different age people view things differently and sometimes we, erm, an issue might be minor for adults but for young people it’s big . . .
Hannah spoke about how a risk assessment “. . . was a bit condescending,” which made her think, “you’re talking to me like I’m five, I’m 18 this year . . .,” displaying concerns about her developmental stage was not being respected. Jenny discussed the differences between separate therapists in their responses to her age. A previous therapy made her feel “a bit like a child” by asking her to paint, however a later therapist “. . . just put things in a way which made me understand . . .” Interestingly, no participant spoke about being spoken to as “too much of an adult” but instead, considered being responded to in a perceived developmentally inappropriate manner as key barrier to older adolescent engagement.
Centrality of a human relationship
This subtheme is based around the experience of the “human” elements to the relationship developed between participants and clinicians. Hannah sums up this subtheme succinctly explaining she experienced her clinician as “a real person.”
Some participants made sense of this by describing relationships with therapists as similar to that with friends, but with professional boundaries: “. . . it doesn’t feel like I’m just speaking to my therapist, I’m speaking to a friend . . . but with a lot of knowledge!” [Anna]. Noah described his clinician as “pro-friend-ssional” to indicate the balance between amiability and professionalism. Others frequently used the adjectives “nice” or “kind” when considering their clinicians. This was often difficult for participants to articulate further when promoted, explaining that this was simply part of them as people, for example, “I don’t know, I think just how she was” [Hannah].
An appreciation of authenticity was expressed, for example, “. . . I thought she was genuinely maybe concerned . . .” [Chris]. Valuing the authentic was shown by some participants by talking about the antithesis of this, and of “human” relationships, which was expressed as concerns about formality. Caroline explained, “. . . if I had got someone that, like, . . . ok so like this [sat up straight], I know I wouldn’t be able to be honest, it just doesn’t feel natural, like.” Noah expressed a concern about “. . . seeing someone who belonged in a bank . . .” For Chris and Hannah, a lack of authenticity was displayed by sensing clinicians were “forced to do their jobs.” The impact of this feared formality may have also affected the participants’ sense of safety, and judgment, within the relationship. Hannah explained, “I wouldn’t want to open up as much” but experiencing a safe relationship lead to “the kind of environment where I felt I could say anything and I wouldn’t be judged . . .”
Tangibility of techniques
This theme centers around therapeutic techniques that have an active and practical element to them—something the young person could “do.” Most young people spoke about appreciating the more concrete techniques, which gave them the opportunity to actively “do” something to aid their therapy, for example, Nebi spoke about the use of thought diaries: “writ[ing] down my negative thoughts and [writing] down another thought that contradicts that thought.” Most participants referred to the tangibility/“doing” techniques as “reassuring” [Caroline] and proving evidence that therapy “actually helps” [Chris]. Rose found the “measureable progress” of practical help beneficial, creating certainty about therapeutic aims and facilitating an experience of “I’m getting help.” Anna explained, “the more she told me about how I can manage my low moods, my anxiety, and sometimes my OCD, it made me want to come here more.”
Rose and Max spoke about how “just talking” [Rose], “didn’t really solve anything” [Max], and expressed the need to be actively working to reduce the impact of symptomology. This may have offered participants motivation to continue their engagement. “Seeing” improvement, and understanding the “point” of therapy, signaled to participants that engagement was necessary: . . . we would write down experiments we were doing and at first I wouldn’t really do them, and then, I started to do more and more of them, so it was good. [Nicole]
Jenny appeared to have preconceived ideas about what constituted therapy, which later conflicted with what she experienced to be therapeutic: “. . . it was very practical and very skills based and we didn’t really talk about my feelings, so it wasn’t really therapy . . .” She further explained, “I felt more prepared for my exams and that I could handle them . . . we talked about specific techniques and things and, erm, yeah, it felt like I’d actually, kind of, I’d achieved something . . .” Noah, the only participant who did not discuss tangible techniques, explained how engagement itself was his therapy: “a big part of what helps about coming here is the routine of seeing people I’ve known for a long time . . .”
Discussion
The present study aimed to explore 16- to 18-year-old sense making of their mental health service engagement experiences and their understanding of contributory facilitators and barriers. As research focusing solely on older adolescent engagement is limited, this contributes to a sparse evidence base.
Links to Previous Research and Theory
The interplay between participant’s understanding of their engagement experience, and the context of the 16 to 18 developmental stages, was of key importance. Dominant theories of adolescent development (e.g., Erikson, 1968) propose separation from parents/adults occurs as adolescents mature. Participants appeared to understand themselves to be reliant on adults to acknowledge their distress and facilitate professional help seeking, possibly opposing theoretical comprehension. Older adolescent experience may differ from models suggesting this is wholly reliant on adult input (Costello, Pescosolido, Angold, & Burns, 1998) and partly supports models suggesting the key role of the adolescent’s “ecosystem” (McKay et al., 1995). Adult reliance sat alongside participant’s own internal cognitive readiness to receive help, supporting previous models (Broome et al., 2001). As the adolescent ages, a shift may occur from total adult reliance, toward a developed sense of cognitive preparedness, inner resolve, and responsibility toward others (Christie & Viner, 2005). This reveals an interplay between internal and external influences, and a complexity around the phenomenon as a whole. Indeed, as participants spoke about help seeking to make sense of their engagement experience, further evidence is contributed to the ideas around the difficulties of engagement conceptualization (Staudt, 2007), and the blurred distinction between help seeking and engagement. Some studies have spoken about how peers are preferred to adults (e.g., Rickwood et al., 2007) when it comes to help seeking/engagement. However, the results of the present study suggest that, in the first stages of engagement, the participants were in fact reliant on adults.
Intricacy was also evident within the idea of developmental appropriateness, reflected in the themes around choice, transparency, and control. For some, having their older adolescent status respected by “not-being-told-what-to-do”/“not-being-patronised” was imperative. This sat alongside appreciating “suggestions,” “teen-relatibility,” and tangible therapeutic techniques (which by their very nature require clinician direction). This reveals an additional layer of complexity around what is understood about engagement facilitators/barriers. The key element of developmental appropriateness supports previous research (Harper et al., 2014) as does the importance of within-session topics (Broome et al., 2001). It is wondered whether what distinguishes “being-told-what-to-do” and “suggestions” is transparency of process. This in turn may aid a sense of control. Indeed, the tangibility of techniques mentioned above may have also provided a sense of control, but over symptomology rather than engagement. Experiencing control is thought to be an important facilitator within adolescent engagement (Bury, Raval, & Lyon, 2007).
During engagement, it appears there is a growth and evolution within the adolescent themselves, and the relationship they have to the engagement process. As this progresses, the older adolescent inner resolve, and perceived usefulness of therapy/continued engagement, may be key in facilitating engagement. This finding supports within-treatment engagement models (King et al., 2014) around the need for client hope and the development of confidence. It is wondered whether the human, “informal” relationship developed with clinicians may take the place of the initial trusted adult, with this engagement growth existing on the foundations of the therapeutic relationship (Harper et al., 2014). In opposition to models (Kazdin et al., 1997), the role of the relationship between parent and therapist did not emerge as a theme. This may be due to the developmental stage of participants. Parents may have a role in initial attendance, but continued attendance is more reliant on the adolescent themselves and the therapeutic relationship, rather than alliance between parent and therapist. This may also not have been an emergent theme as some participants actively requested for parents to not attend sessions, and all therapy was 1:1 based.
The role of peers was limited within participants’ narratives. Research and theory suggest, as adolescents grow older, a social shift occurs from family to peers (e.g., Bronfenbrenner, 1977). This implies their influence could have been more present in the current study, however, it may not have been considered to be of key significance to participant sense making. Previous research suggests peers play a role within help seeking (e.g., Rickwood & Braithwaite, 1994); however, when considering the ongoing engagement phenomenon, peer input may be less influential. The lack of peer discussion may also be due to concerns around stigma (Fisher et al., 1982). For example, peers may have been less aware of service attendance due to participant concerns about judgment. The role of stigma was also marked in its absence from emergent themes. Stigma may play more of a role when considering help seeking (Gulliver, Griffiths, & Christensen, 2010) rather than engagement. The lack of emergence of peer and stigma themes may suggest that 16 to 18 engagement is less of a “social” phenomenon than help seeking.
The impact of symptomology on engagement, and engagement (de)motivation, is absent from models. Previous research has investigated links between dropout and “diagnosis” (e.g., Johnson et al., 2008). The current study suggests symptomology, rather than “diagnosis” may play a role in engagement, especially around the interplay between initial anticipation and determination to engage. This finding supports research recommending therapist exploration of adolescent beliefs during engagement (Bury et al., 2007).
Study Strengths, Reflexivity, and Limitations
The employment of an exploratory design, rooted in older adolescent lived experience, allowed for rich, participant-centered data to emerge. Semistructured interview encouraged participants to lead on discussions, and therefore, on the type of data collected. As emergent themes were developed from participant sense making, the results of the study may reflect a unique 16- to 18-year-old–centric experience of a complex phenomenon. The selection of IPA allowed for the specific older adolescent developmental context to be explored in relation to engagement understandings.
When considering reflexive research practice, participants may have experienced a separate engagement process with the researcher, mirroring their wider service engagement experience, for example, engaging, in part, due to concerns about letting others down. Power dynamics, and social desirability, may have affected the direction, and content of interview, as it was unclear how the participants viewed and responded to the researcher—either understanding them to be a clinician based within the service, or as an independent party. As the lead researcher was a trainee clinical psychologist, the role researcher-as-researcher and researcher-as-clinician may have required more conscious negotiation of positioning and adopted language, through the use of reflexivity.
Recruitment procedure required clinicians to consider potential participants from their caseloads. There is potential bias here as participants may have been selected based on certain clinician biases, that is, quality of relationships. According to clinician reports, all adolescents approached agreed to participate. This has possible implications around power and the ability to say “no” to clinicians, meaning some may have felt obliged to participate. There was variation in the length of engagement among participants, which may have influenced interview content, for example, around strength of therapeutic relationships. As engagement may be a phenomenon that varies over time (Cunningham et al., 2009), and models suggest elements of initial engagement may differ from ongoing engagement (e.g., Broome et al., 2001; King et al., 2014), it is possible participants were making sense of different stages of the phenomenon.
Respondent validation (Mays & Pope, 2000) was missing from the current study due to a tight research timeline. There has been debate about the necessity of this (Giorgi, 2006) due to the interpretative nature of IPA. Exclusion criteria dictated that more complex presentations were not included in the current study, which limits applicability. However, IPA on the whole is less focused on generalizability but more with rich, deep exploration of the selected phenomenon. Following guidance (Smith et al., 2009), a 50% cutoff of emergent themes was adopted to ensure relevance to the sample as a whole. This may have resulted in a less thorough exploration of divergence across cases. As IPA is reliant on researcher interpretation, despite the employment of reflexivity and bracketing techniques, the potential for bias remained in emergent theme development reflecting researcher beliefs or preconceptions of the engagement phenomenon.
Clinical Implications
The therapeutic relationship has been extensively researched (e.g., Karver, Handelsman, Fields, & Bickman, 2006). The current study suggests the area of this, which may be crucial for clinicians to cultivate are the “human” elements—remaining genuine and nonjudgmental, balancing amiability with professionalism, and avoiding “formality.” The prominence of cognitive preparedness, determination, and anticipation before first session attendance was marked. This suggests more consideration may need to be given to engagement facilitation in the time between referral and attendance. This may lie more with refining multiagency service provision (Joint Commissioning Panel for Mental Health [JCPMH], 2013) rather than direct clinical intervention. Engagement may be facilitated by clinicians discussing cognitive preparedness (Bury et al., 2007), with adolescents at initial attendance. By making sense of help seeking (Reder & Fredman, 1996), and avoiding separating this from engagement, clinicians may develop understanding of client’s idiosyncratic engagement facilitators and/or barriers.
Emergent themes suggest the key importance of appropriate responsiveness to developmental stage, through offered control and transparency. Engagement may be facilitated by clinicians involving clients in areas there may be potential for control (such as, content of therapy sessions), transparent about areas less open to change, and discussion of potential disappointments with the service. Facilitating perception of usefulness of sessions and tangibility of techniques may also encourage engagement. The above suggests combining and balancing the relational and cognitive, by providing key developmentally appropriate engagement facilitation.
Future Research
As a key message throughout this study has been one of developmental appropriateness, it may be important when planning research, policy, or service developments to consult young people on topics and design (YoungMinds, 2005, 2011) to maintain relevance to adolescent needs.
As the conceptualizations and boundaries between help seeking and engagement remain blurred, further research into the development of clearer definitions and models, from the adolescent view, may be beneficial to ensure developmentally appropriate theoretical progressions (Drieschner et al., 2004; Weisz & Hawley, 2002).
Research into the relationship between factors internal and external to adolescents, for example, inner resolve/cognitive preparedness in relation to the role of families at this developmental stage, may provide further insight into the engagement phenomenon. This may in turn influence the development of strategies targeting adolescents who may be at risk of disengagement, or who do not seek service help.
Conclusion
Due to the paucity of research, this IPA study aimed to investigate the 16- to 18-year-old understanding of their mental health service engagement experience, facilitators, and barriers. Overlap between help seeking and engagement understandings was demonstrated. The key role of developmental context emerged, regarding autonomy negotiation and adult reliance, and factors internal (e.g., inner resolve) and external (e.g., family) to the adolescent. Participant experiences of service buildings and policy also emerged. Implications for clinical practice involved ensuring developmental responsiveness through cultivating a human therapeutic relationship, and responding to cognitive preparedness, control, and transparency. It was suggested future research focuses on ensuring adolescent participation. Potential topics for investigation included developing help seeking and engagement conceptualizations, and further investigation into 16- to 18-year-old experience of service buildings and policy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.