
Abstract
The purpose of this study is to describe the underlying theory and the challenges involved in implementing an intervention to access health care services for migrants with precarious status (MPS) in Montreal. The description of the underlying theory of the intervention was based on a documentary analysis and a workshop with clinicians (n = 9). The challenges were identified through concept mapping (n = 28) and in-depth interviews (n = 13). The results of the study indicated that the aims of the intervention were to provide access to health care to MPS primarily to avoid any further health status deterioration. The most significant challenges identified were sustainable funding resources and improved access to care and protection for MPS. The interviews indicated that MPS are difficult to reach out; public health care system rules are unclear; resource constraints make it difficult to provide adequate and continuing care; and advocacy activities are difficult to organize.
Keywords
Introduction
Global migration is expanding and increased from 172 to 257 million migrants between the years 2000 and 2017, globally (United Nations Department of Economic and Social Affairs [UN DESA], 2017). According to recent reports by the Government of Canada, the proportion of permanent resident status is stable, whereas temporary resident status is increasing (Citizenship and Immigration Canada, 2014; Immigration, Refugees and Citizenship Canada, 2017). Although precise numbers are not available, estimations show that there may be up to 500,000 undocumented migrants in Canada—around 1.36% of the Canadian population in 2017 (Gouvernement du Canada, 2018; Magalhaes et al., 2010). While the province of Québec receives 70% of the immigration to Canada, the proportion of immigrants is lower in Montreal (22.3%) as compared with the other main cities of installation (Toronto and Vancouver with more than 40%) (Homsy & Scarfone, 2016). In 2011–2012, Canada received approximately 56,000 nonpermanent residents. Of this population, around 20% currently reside in Quebec and British Columbia, while another 40% live in Toronto (Bohnert & Statistique Canada, 2015).
Meanwhile, drastic changes in immigration policies in the recent past have negatively impacted migrants’ rights as well as their ability to obtain permanent status in Canada, further deteriorating what is an already precarious situation (Magalhaes et al., 2010). For the purposes of this article, migrants with precarious status (MPS) are defined as individuals born in another country and living in Canada who have limited or no access to health and social services due to health policy restrictions, and whose immigration status is temporary, dependent on a third party or not recognized at all (Sikka et al., 2011). In this article, the term “uninsured migrants” is sometimes used interchangeably with MPS.
In accordance with the Canadian Charter of Rights and Freedoms, health care services should be accessible for all Canadian residents without discrimination. All permanent residents and Canadian citizens are granted by a publicly funded medical insurance system (RAMQ), which covers, for of charge, all medical services, or services related to prevention, treatment, rehabilitation from an illness or injury. Depending on income, there is also the possibility to subscribe for an insurance covering most of the costs of prescribed medication. Nonetheless, inequities exist for many segments of the population, including refugees. Difficulties accessing health care are directly linked to immigration status (Brabant & Raynault, 2012a; Nkunu & McLaughlin, 2018). In other words, health coverage varies depending on immigration status: private insurance for visitors and students; Interim Federal Health Program (IFHP) for asylum seekers; and a 3-month waiting period for those who qualify for Medicare (RAMQ), that is, permanent residents and temporary foreign workers. Those whose status is pending a decision by immigration authorities—including deportation dates—and undocumented migrants are also without health coverage. To facilitate access to health care, the Ministry of Health and Social Services provides funding for three types of services directly aiming to respond to the needs of migrants as follows: (a) clinics to evaluate the needs of refugee and asylum seekers in all administrative regions (total annual budget of 2.9 million) (Ministère de la santé et des services sociaux, 2012); (b) a regional program offering services in Montreal for integration and immediate assistance to asylum seekers (PRAIDA) (total annual budget of 2.58 million) (Ministère de la Santé et des Services sociaux, 2017); and (c) clinics to accompany families with children aged between 0 and 5 years (total annual budget of 750,000 for three clinics in Montreal) (La Maison Bleue, n.d.). These services are interdisciplinary and will refer to regular services in the health system, where possible. However, none have the mandate to attend to uninsured migrants. Lack of services for uninsured migrants and precarious living and working conditions contribute to unfavorable health status among undocumented migrants when compared with other immigrant groups (Ortega et al., 2007). In particular, some health conditions such as infectious diseases are more commonly seen among migrants as compared with the general population, while having important health implications for the general population such as an increase in disease burden and deaths due to late detection and treatment (Hahné et al., 2013). It is therefore argued that access to health care for MPS must be addressed to reduce health inequities in Canada as a whole.
Despite being the most vulnerable groups, few studies have focused on interventions addressing access to health care services for migrants. Among these, a scoping review of 83 studies on health interventions designed for immigrants in high-income countries found that most interventions (60%) were carried out in the United States. These interventions mainly targeted specific migrant groups and took the form of individual interventions aiming to prevent, screen, or treat chronic conditions or cancer (62%) (Diaz et al., 2017). Moreover, in high-income countries, different models of care have been developed and evaluated specifically for undocumented or uninsured migrants. A survey of all free clinics in the United States (N= 754) shows that 92% see uninsured patients, and 56% are specifically tailored for those who are not medically insured, with volunteer physicians providing services in most instances (Darnell, 2010). Another such example is of student-run free clinics (SRFC) that offer interdisciplinary care by students under the supervision of health care professionals. A national survey in the United States identified 208 SRFC, from 86 different institutions (Smith, Thomas et al., 2014), which attest to serving uninsured populations, primarily (Simpson & Long, 2007). Meanwhile in Canada, there exist only eight such clinics for the underserved (e.g., the homeless, MPS, recent immigrants, and first nations) (Ng & Hu, 2017). The efficiency of such clinics has not been extensively evaluated. Major findings from studies conducted in the United States stress the importance of quality evaluations, and preventive care (Butala et al., 2012), particularly in the case of depression (Soltani et al., 2015), and diabetes management
Mobile health clinics (MHCs) are also a commonly used model of care. In the United States, an estimated 2,000 Mobile Health clinics aim to reduce health inequities by providing 6.5 million consultations to vulnerable and uninsured populations. These MHCs have been shown to improve (a) access to care by both migrants and minority groups; and (b) screening and management of chronic diseases (Yu et al., 2017). MHCs have also been effective in reducing the number of hospitalizations and the length of hospital stays (Yu et al., 2017).
Safety-net programs with minimal resources are also frequently used by nongovernmental organizations (NGOs) and faith-based organizations to provide free care for undocumented migrants, while benefiting from the help of volunteers and community networks. Studies in the United States and Israel have described the work of “safety-net programs” from anthropological (Tiedje & Plevak, 2014; Willen, 2011), ethical (Clark & Schadt, 2013), or patient-satisfaction perspectives (Feinglass et al., 2014). One faith-based program in Dallas was evaluated on the impact of its integrated community-based model for the uninsured, which includes screening and referrals for diabetes, cancer, depression, and other social concerns. The results showed a significant reduction in the number of emergency department visits, length of inpatient hospital stays, and as well as direct and indirect costs incurred (DeHaven et al., 2012). In Europe, there are 71 care models across 12 countries specifically developed for uninsured migrants. Mostly NGO-run, these models provide general, diagnostic, and mental health services (Biffl & Altenburg, 2012). There have also been some studies on the challenges faced by NGOs in providing care for undocumented migrants in Europe (Chimienti & Solomos, 2016; De Vito et al., 2016), one of which describes migrant health interventions by Doctors of the World (DoW) in European countries (Kentikelenis & Shriwise, 2016). It must be noted however that a consultation with DoW in 2017 found that no program evaluation had been conducted regarding the Organization’s interventions targeting migrants in Europe.
Restricted access to health care remains a major challenge confronting this growing population (Brabant & Raynault, 2012b). It is therefore imperative to address unmet health needs of MPS by providing services through community organizations and health clinics. Meanwhile, research on effective interventions for MPS in Canada is still lacking. Also, despite the presence of health care workers within Montreal’s public health care system who accept to see MPS free of charge, the extent of such practice remains unknown. Within the private sector, doctors will see patients with fees that range from 25 up to 300 Canadian dollars, per consultation. In this context, since 2011, DoW has been the only organization to provide free health care for migrants of all ages without requesting proof of identity or residency at their weekly clinic. Patients presenting at the clinic can be seen by a nurse, a social work intern, and a doctor for minor health problems. However, patients are required to pay out-of-pocket when referred to the public/private health care systems for tests, examinations, or medication. Considering that the cost of health services, fear of deportation, or impact on migration process are the main barriers to care for the uninsured migrants (Brabant & Raynault, 2012a), the possibility to consult freely and without the need to present immigration documents greatly facilitates the use of health care services. The DoW clinic is primarily run by volunteers and is providing more services as funding opportunities improve (addition of a mobile clinic in 2014 and a clinic for pregnant women and children in 2016). The number of volunteers at the clinic has also increased from 49 doctors in 2012–2013 to 438 in 2017–2018. The clinic receives funding mainly through donations, foundations, and the public health department.
In Toronto, the situation is quite different as certain community health centers are publicly funded to provide services for uninsured migrants (e.g., Non-Insured Walk-in Clinic [NIWIC]). The NIWIC is a free and confidential walk-in clinic with regular opening hours for residents of Toronto who do not have a health care insurance. They offer episodic care, midwife services to pregnant women, phone interpretation, and referrals. Midwives are not required to ask for health insurance when offering pregnancy care and over 12 sexual health clinics provide free counseling and testing for MPS. In addition, there are a number of other community and student-run initiatives that provide care for uninsured migrants (Ng & Hu, 2017). In Vancouver, the BC Women’s Hospital and Health Center offers free prenatal care and reproductive services to low-income women regardless of their migration status. Although there is a call for further population health intervention research in Canada, none of the above mentioned interventions have been documented (Hawe et al., 2012). The purpose of the present article is to describe the underlying theory and challenges involved in implementing health care intervention for MPS in Montreal.
Materials and Methods
Setting
The study was conducted at a Montreal-based NGO known as Doctors of the World (DoW). Since 2011, DoW has been implementing “the Migrant Project,” a public health intervention to serve urgent health care needs of MPS. The number of consultations by migrants without health insurance at the DoW clinic is increasing annually. In its first full year of operation (2012–2013), records show that 423 new patients received services. In the following years, this number of patients seen raised steadily to 537 (2013–2014), 681 (2014–2015), and 795 (2015–2016) (Médecins du Monde Canada, 2013, 2016). The main reasons for consultation are pregnancy examinations, screening for sexually transmitted diseases, osteoarticular disease, diabetes, cardiovascular diseases (including hypertension), digestive problems, and psychological distress (Médecins du Monde Canada, 2013).
Study Design
To understand this new intervention, a convergent mixed methods study design was used (Pluye & Hong, 2014) in which both qualitative and quantitative data are collected and analyzed, concurrently. A population health intervention research study was conducted to “produce knowledge about policy, programs and events that have the potential to impact health at the population level” (Hawe et al., 2012). While impact is not assessed, one of the key steps is to document the underlying theory as well as the implementation process (Weiss, 1998). This in turn helps avoid type III errors that involve evaluating an intervention that has not been fully implemented. It is important to consider that most social services are delivered in a nonstandardized fashion and depend on service providers, beneficiaries, and local context (Dobson & Cook, 1980). As a result, the evaluation may conclude that the program is ineffective, when in fact, it is the suboptimal implementation that undermines the effectiveness of the program (what is called type III errors) (Dobson & Cook, 1980).
Sample Selection
Purposeful sampling methods were used for this study (Palinkas et al., 2015). This method was selected to ensure the inclusion of people with different perspectives on the Organization’s work. More specifically, participants were selected based on their profession (nurse, social worker, physician, outreach worker, etc.), organizational status (staff members and volunteers), and time involved in the project (minimum 6 months).
The quantitative method in this study was used to explore challenges in delivering the intervention, while the two qualitative methods were used to describe the underlying theory of the intervention and further elaborate on the challenges identified. A convenience sample was selected for the quantitative method and for describing the intervention. All staff members and volunteers were invited to participate. The program manager helped to identify initial interview participants, and the rest were selected by using a snowball strategy until saturation of data was reached.
Data Collection and Analysis
First and foremost, it was important to gather and analyze all intervention-related documents. Next, all the staff members and volunteers of the DoW were sent an email that explained the project and asked for consent regarding their participation.
Participants were invited to a half day workshop organized in January 2013 to describe the intervention theory using documentary analysis. During the workshop, group facilitation methods (brainstorming, group review, meta-planning) and visual representations (PowerPoint, board, flipchart, post it) were used to help the participants describe their model of intervention. The intervention model prepared by the research team was presented during a team meeting and validated by the manager and staff members. To identify the challenges encountered in implementing the intervention, the research team benefited from the use of the following two methods:
The first method consisted of concept mapping
The second method consisted of in-depth semistructured interviews (Palinkas et al., 2015) with employees and volunteers. After obtaining verbal consent from respondents, 1 hr-long interview was conducted by the first author with each participant. Interviews were recorded and subsequently transcribed during the summer of 2013. The interview template was developed by the research team with questions emerging from the concept mapping and development of the intervention theory. It included questions on key components of the intervention theory and the challenges involved in implementation. Inductive analysis was carried out manually by one author (Palinkas et al., 2015).
In the fall 2013, the results were presented and validated by staff members involved in the project during a meeting of the Healthcare Committee of DoW, comprising all staff members and four volunteer doctors. Staff members were in agreement with the results proposed, and no changes were made. This study was subsequently authorized by the Board of Directors of DoW. As no data were collected on patients or MPS, the approval of the institutional ethics board advice was not required.
Results
Nineteen people participated in the first method pertaining to concept mapping (i.e., identification of intervention challenges): Participants were on average aged 36.8 years; mostly women (84%); DoW employees (42%); nonmedical volunteers (31%); family physician volunteers (16%); and nurse volunteers (11%). Participants’ average length of project involvement equaled 12.7 months. Theses participants produced, sorted, and rated the importance and urgency of challenges statements.
The nine workshop participants were on average aged 36.1 years; women (89%); DoW employees (67%); family physician volunteers (22%); and nonmedical volunteers (11%). The average length of project involvement by workshop participants equaled 14 months.
Subsequently, 13 interviews were conducted with three physicians, five employees (manager, project coordinator, and nurses), four volunteers, and one social work intern. All three methods considered, 100% of staff members and interns, 24% for volunteer doctor (12/49), and 33% of all other volunteers (18/43) participated in the study. At the time of the study, all the five staff members and one doctor participated in all data collection methods.
The Intervention Theory
In this article, the term “theory” is understood in the evaluatory sense of the word as, “the description of the intervention and its effects (to shed light on the causal chain of the intervention by describing the inputs, resources, activities and effects)” (Ridde & Yin, 2012, p. 182).
The target population for this intervention includes medically uninsured migrants who lack access to public health care for different reasons. This group includes but is not restricted to permanent residents during the 3-month waiting period for medical coverage, rejected asylum seekers (not covered by the IFHP), other people awaiting eligibility for protection, temporary migrant workers such as live-in caregivers, temporary agricultural workers who have lost the right to health care, and people with temporary visas and no private coverage. In the short term, DoW aims to provide basic health care to avoid the deterioration of patient’s health and thereby prevent serious illnesses and emergency room use. DoW’s intervention also aims to support MPS in exercising their rights (health, legal, social). Moreover, the project also engages in advocacy with health professionals and with the civil society.
The intervention by DoW mainly consists of providing free medical services, for a minimum of 6 days a month, to uninsured migrants, only. The clinic is primarily run by volunteer doctors, a nurse, and a social work intern. While the ultimate goal is to have a walk-in clinic which offers more flexibility for vulnerable populations, resource and space constraints limits services, which are offered by appointment only. The expected outcomes of the clinic include strengthening trust in DoW, reducing waiting time for consultation, improving treatment options, reducing risks due to untreated conditions, and anxieties related to health status. DoW also supports MPS in accessing the public health care system wherever possible and raises immigrants’ awareness of their rights (health, legal, work and living conditions, etc.). Volunteer staff, who are often licensed health professionals practicing in the public or private health care system, or students (law, social work, nursing, pharmacy, etc.), receive training on access to care related to migration status, resources available for the uninsured, as well as the most commonly observed health problems and treatments. These trainings aim to improve the staff’s sense of efficacy given that the level of experience with migrant populations varies greatly among professionals.
To access services offered by the clinic, migrants must leave a voicemail message to which a volunteer nurse responds within 7 days to conduct a triage. While the organization is aware that the process limits access to the clinic because volunteers are not always able to reach people to conduct the triage or experience language barriers to evaluate the situation properly, about 70% of callers are seen at the clinic (Médecins du Monde Canada, 2013). This will determine whether the person can be seen at the Clinic. If not, information is provided on where to seek services within the public system or community settings. Persons accepted for services at DoW will receive appointments based on medical priorities and slots available, after a nursing evaluation over the phone. At the clinic, patients may consult a social work intern, a psychologist, a physician, and/or the nurse. Generally, patients meet with the social work intern prior to consulting the nurse. This is done to evaluate eligibility for public health insurance, as well as to facilitate access to social services and regularized immigration status. Where the patient’s condition necessitates, staff also tries to facilitate access to medication, lab tests, or imaging as well as consultations with specialist doctors. To sustain its activities, DoW continuously recruits volunteer doctors and other health professionals both for work at the clinic, and for patient referrals within the health care system—most often for more specialized care.
As resources do not allow for the provision of continued prenatal care to pregnant women, DoW organizes information sessions on the resources and realities of giving birth without health insurance, covering topics such as when to go to the hospital, associated fees for anesthetist, gynecologist, and hospital stays. Other activities organized in partnership with community organizations include vaccination and information sessions on sexually transmitted diseases. Monthly, information and discussion sessions are also organized to break social isolation and stigma associated with status.
To inform communities of services offered by the Organization, an outreach worker also visits shops, restaurants, beauty salons, and places of worship in neighborhoods that have a dense migrant population. These visits also serve to better understand the needs of this community. This work is done in close partnership with community organizations. Such partnerships are of particular importance considering ongoing challenges in addressing unmet needs, including funding for new activities.
Figure 1 presents the intervention theory (the linear representation is heuristic, as the intervention is obviously complex).
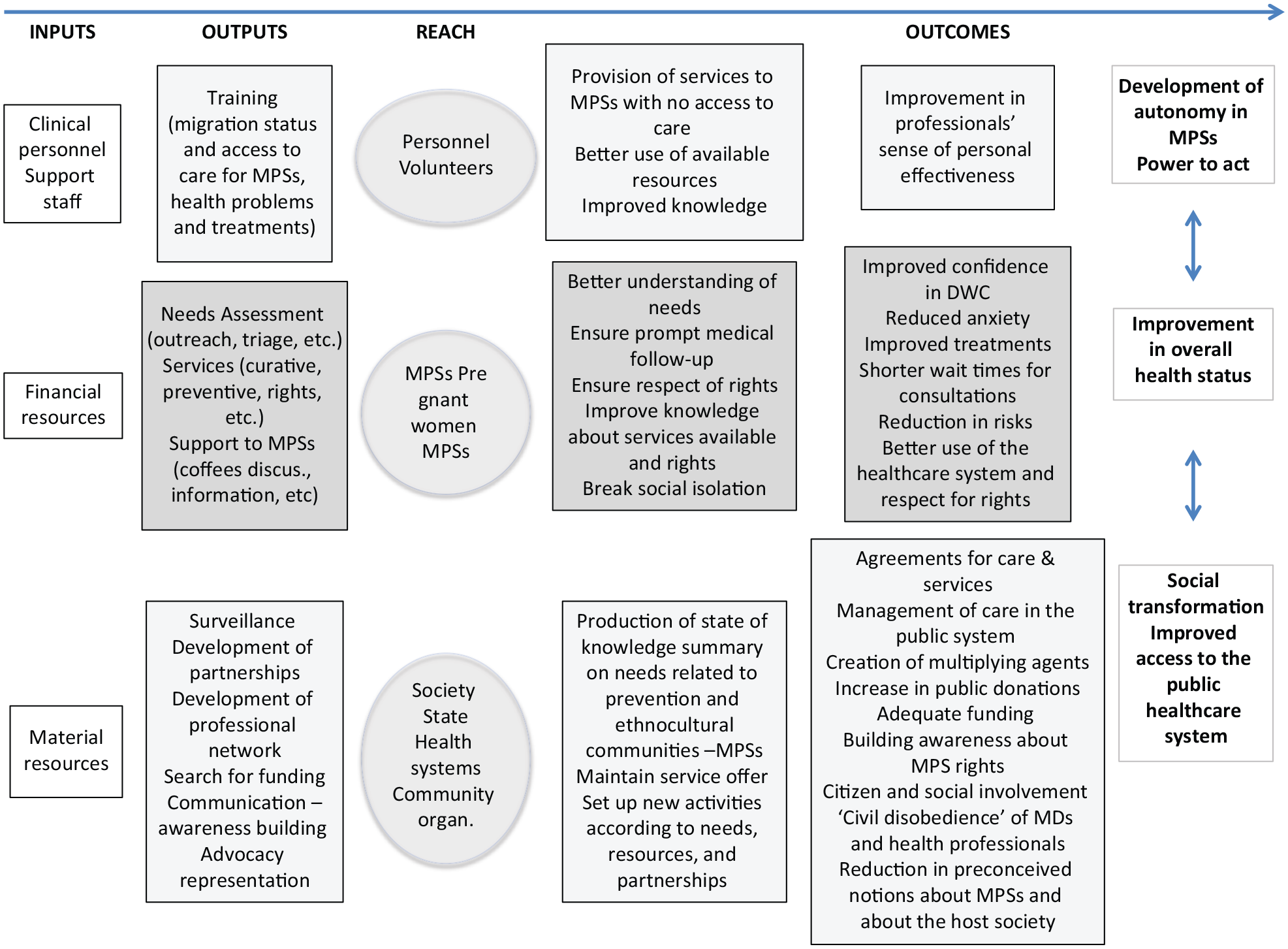
Logic model of the project migrants of DWC.
Findings From the Concept Mapping
The importance and urgency scores for the 107 challenges are provided in Online Appendix 1 to quantify intervention challenges. The term “urgency” refers to the speed with which problems must be addressed. The term “importance” refers to the scope of the problem to be resolved.
Table 1 presents the 10 most important challenges, and Table 2, the 10 most urgent.
The 10 Most Important Intervention Challenges.

Note. DoW = Doctors of the World.
The 10 Most Urgent Intervention Challenges.

Note. DoW = Doctors of the World.
The most important and urgent challenge identified is securing sustainable funding. The following four issues were also identified as urgent and important: (a) reaching individuals who do not wish to be found so that they may benefit from services offered by DoW, (b) providing good quality care, (c) addressing the organization’s funding deficits, and (d) reaching the maximum number of MPS possible. Challenges identified as important but not urgent relate to shifts in public opinion, advocacy for policies at the provincial level, public health care for all MPS, and sensitization regarding equity in health care. Challenges identified as urgent, but not rated among the 10 most important mainly relate to resources required for quality care in a context of limited resources. Among these are difficulties faced in ensuring adequate drug supply and expanding partnerships, as well as the challenges recruiting human resources including volunteers. The Pearson correlation coefficient between the two average scores (importance and urgency) for all statements is high (0.79).
Cluster analysis grouped the 107 challenges identified into 12 clusters. Table 3 presents the names given to the clusters as well as their average importance and urgency. All clusters were rated as more important than urgent. Some clusters are close to one another in terms of importance (I) and urgency (U). These are (a) improving access to care and protecting MPS (I: 4.08; U: 3.69) and advocacy for social change (I: 4.03; U: 3.31); (b) empowering MPS (I: 3.77; U: 3.31) and establishing partnerships and networking (I: 3.76; U: 3.43); (c) respecting the roles and responsibilities of providers (I: 3.64; U: 3.53) and ethical and professional issues (I: 3.62; U: 3.32); and (d) engaging in health promotion and prevention activities (I: 3.53; U: 3.12) and improving the care process (I: 3.50; U: 3.37). Online Appendix 2 lists the challenges in each cluster.
Names Given to the Clusters and Their Average Importance and Urgency.
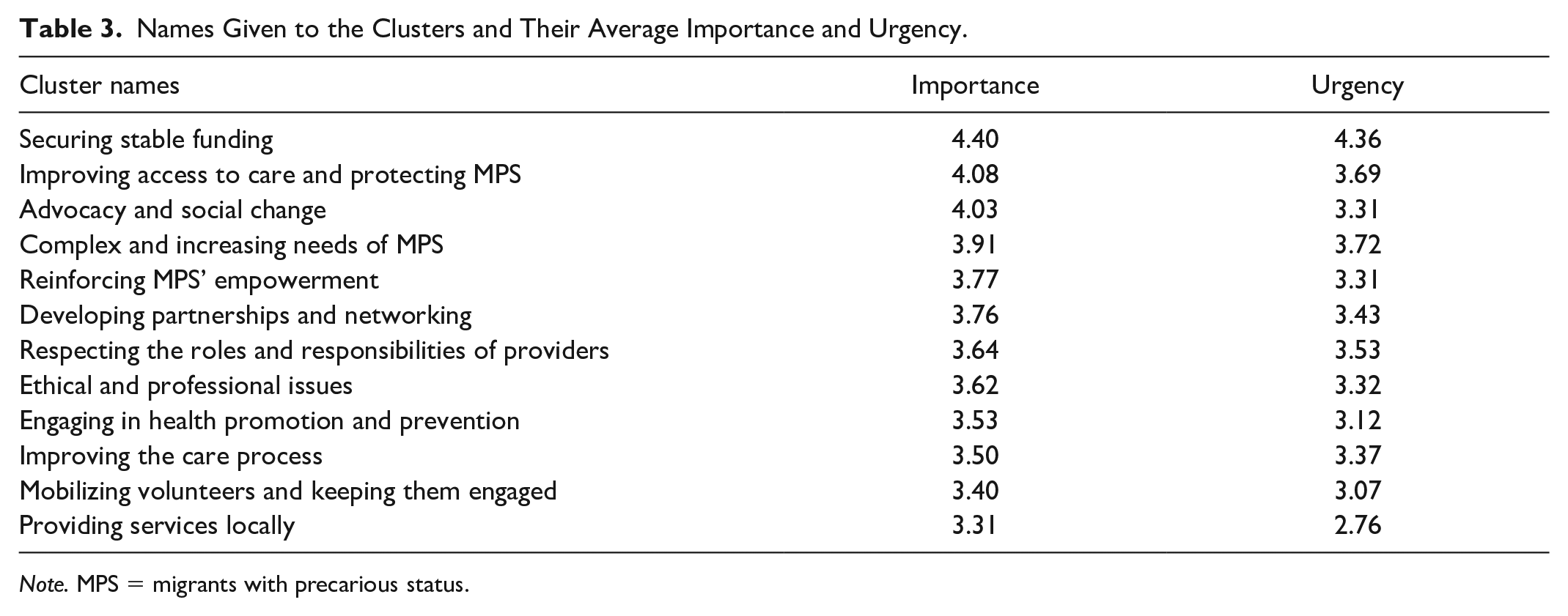
Note. MPS = migrants with precarious status.
Findings From the Semistructured Interviews
The qualitative component of the study identified four key challenges:
Difficulties reaching MPS
Undocumented migrants are the most vulnerable among migrants. Unsurprisingly, they are also the most in need of health services yet the hardest group to reach as they often have to hide mainly due to fear of deportation. Many undocumented migrants avoid all contact with public and community-based services: “Some are scared to get deported (if they use services), it’s not a fear that is wacky, it’s something that happen for reasons not necessarily linked to reporting to immigration authorities (leading to deportation)” (MD3). Telephone triage also constitutes a barrier in reaching the most vulnerable, as this group regularly change numbers or may not have a phone. Language barriers are also an impediment as most will not be able to explain their situation in the language spoken by the volunteer nurses (mainly French, English, and Spanish). Thus, “our patients . . . are those who are more organized; they’re able to use resources . . . but someone who is more isolated and really in a precarious position will not necessarily be looking to use resources” (STAFF2). Moreover, to protect patients from immigration authorities, the medical clinic has no signage, which in turn makes it less visible in the community.
The challenges faced in reaching MPS are linked to the cluster on improving access to care and protecting MPS—the second most important and urgent challenge. Challenges which fall under the same category and were identified in the concept mapping but not talked about in the interviews include not knowing the people we are serving; effectively doing outreach with populations that do not wish to be found due to their fear of deportation; and facilitating access to health care for the most vulnerable (those without status, LGBTQ+, and people with mental health problems).
The health system as an obstacle to access
The bureaucratic functioning of the health system has changed for the worse: There are strict rules. Things have gotten more rigid over the past 10 to 15 years. There are many more places where a sign at the reception desk says to show your health insurance card. I don’t know what it’s related to, but there’s a lot more checking. (MD3)
Staff members also worry about their patients’ safety within the health care system given that people are deported after being denounced in the course of their hospitalization. As for health care personnel, “Some are very open, respectful, and only want to help; they feel for the patient’s vulnerability. But there are others who decide that, morally, these patients have no right to health care, and they apply the rules” (STAFF5). In some cases, individuals within the health care system will reveal the identity of the undocumented migrant while trying to determine eligibility to access services: “Sometimes people from the financial department of the hospital call the government to ask if these people have the right to access services” (MD2).
Where an uninsured patient is able to access health services, they usually have to pay. Costs incurred vary greatly depending on the institution’s policy and doctor’s billing practices. While some hospitals offer and accept alternative options for payment of service, yet others refuse any arrangements whatsoever. In hospitals, fees are often demanded before the patient receives any service: “It happens regularly that we send patients to the emergency room and they’re charged $700 on arrival” (SWI1).
While some physicians charge reasonable fees when patients do not have public health coverage (RAMQ), there are no regulations to prevent practitioners from charging excessive fees. For example, whereas “the RAMQ reimburses physicians $450 for childbirth, some physicians charge MPS $1,000 to $3,000..” Thus, “as there are no rules, some professionals abuse the system and don’t take into account people’s precarious status” (MD1). Moreover, pregnancy is of particular concern because it’s a problem that divides the (hospital) teams, in the sense that all persons doing obstetrics work in team, because we can’t be on call 24h/7days a week. So, when a doctor accepts to see a patient without RAMQ, it creates a problem within the whole team. (STAFF 3)
There is no specific cluster pertaining to the experience of patients within the public health care system. However, some of the challenges identified among the complex and increasing needs of MPS cluster are related to these obstacles. These issues were also extensively discussed in participant interviews.
Difficulties to provide the needed care
Limited resources for the project lead to major difficulties in providing suitable, adequate, and continued health services that meet MPS needs. Most patients seen at the clinic require costly and long-term follow-up and/or complex care. This is especially true for pregnant women and people with chronic illnesses, whose needs make up a high proportion of the demands placed upon DoW. In taking treatment decisions, health professionals need to consider the Organization financial constraints, difficulties in accessing the public system, and the patient’s personal financial situation. “This is a constant headache for each patient . . . a lot of time is spent wracking our brains and trying to find the best solution” (STAFF4). In doing so, professionals view service provision to this population from opposite angles—that is, satisfactory and unsatisfactory. For instance, one participant states, it is very positive, it never happened that I was under the impression I am letting someone die because I could not do anything for the person, I always have the impression that I make a difference when I see a patient, we do good work. It’s a lot less frustrating than when I worked in Ethiopia and had to let a baby die. (MD3)
Meanwhile, another participant is of the opinion that it’s very rare to solve a problem completely, we can bring a small help, I don’t want to be pessimistic, but we need to be realistic, in most cases, we bring a temporary help, and we feel like we are in front of a wall. (SWI)
These challenges are well documented among the complex and increasing needs of MPS cluster, where the greatest number of challenges are identified (over 21), as the abovementioned challenges are also noted in the ethical and professional issues cluster.
Difficulties related to advocacy
All activities related to rights advocacy and advocacy for social change are considered extremely important: “The solution is above all political and is at the level of the health care system” (BEN2). Thus, “the objective is not to create a parallel system, but to defend their right to health and to re-enter the system” (BEN3). However, such activities are impeded by a lack of resources (namely, time and energy), the negative impact of restrictive policies on health-spending, and societal prejudice toward MPS: This is part of my work, to give examples that will touch people, but I know it’s a marginalized population, there will always remain tensions within society, it will never be smooth, even with all the good will or the best advocacy work, it’s like with sex workers, drug users and homeless people, they don’t get the sympathy. (MD2)
Other obstacles related to advocacy are lack of research to scope the problem of MPS access to care and inadequate financial resources for investment in communications and media.
Challenges identified in rights advocacy and social change cluster point to actions needed to ensure MPS access to the public health care system (public opinion and health care system education and political advocacy). However, statements made throughout the qualitative interviews focus on obstacles to achieving this objective.
Discussion
To our knowledge, this is the first study documenting the underlying theory and challenges involved in implementing an intervention to improve MPS access to health care in Quebec.
DoW continue to raise public awareness regarding the unmet needs. This is done with the knowledge the clinic would no longer need to exist if the health care system responded to the needs of MPS. In the meantime, the DoW “Migrant Project” provides much needed frontline health care services to an increasing number of MPS every year. Results show, however, that limited resources present obstacles for reaching those in greatest need of the intervention, as a drop-in clinic is not feasible and as DoW do not have sufficient funding to cover for additional costs for their patients when they are referred for tests and examinations. Nevertheless, with the addition of a drop-in and mobile clinic, there have been improvements in service delivery since our study was conducted. Moreover, while advocacy was considered important but not urgent by participants at the time of our student, efforts have since been made to conduct advocacy activities, which has led to an important campaign on access to care for pregnant women and children to be launched in Quebec in 2019 (Early Childhood Observatory, 2019). Nevertheless, the administration confirms that the challenges identified herein persist to the present time.
Mainly funded by civil society, the intervention also receives minimal funding from the public health care system. This is in contrast to most other best practices which rely on public funding and strong links to the health system (Beck, 2005; Biffl & Altenburg, 2012). Such examples are seen in Toronto and Vancouver, where some specific services for uninsured migrants are publicly funded (McKeowen, 2013).
In such a climate, community organizations have developed a number of intervention models to improve access to health care for uninsured migrants. These include providing free care in medical clinics, universities, and mobile vans (Biffl & Altenburg, 2012). Migrants are also assisted in accessing medical coverage or receiving care within the public sector (Biffl & Altenburg, 2012). Where this is not possible, access to health care is facilitated through collaboration with health institutions and other NGOs addressing the health care needs of uninsured migrants (Biffl & Altenburg, 2012). In this regard, the activities developed by DoW are similar to that of other NGOs or charitable institutions. These activities are tailored to meet the most urgent needs of vulnerable populations, depending on the context. For instance, the European division of DoW is providing medical services in nine countries, with a specific focus on infectious diseases and mental health support (Kentikelenis & Shriwise, 2016). In Montreal, DoW is faced with an important demand from pregnant women and people with chronic illness. Differing health services are also explained by migration trends and patterns, as well as different health policies. For example, many European countries provide free services for undocumented children and pregnant women, reducing demands stemming from unmet health care needs of pregnant women (Biffl & Altenburg, 2012). Successful health projects targeting uninsured migrants (including DoW-Montreal) commonly benefit from volunteer support and institutional partnerships (Biffl & Altenburg, 2012; Clark & Schadt, 2013; Ng & Hu, 2017; Tiedje & Plevak, 2014; Yu et al., 2017).
Challenges Involved in Implementing the Intervention
Securing sustainable funding is considered most urgent among challenges identified given that it affects long-term planning regarding service provision. In other Canadian cities including Toronto, resource constraints for advocacy work are also felt as a major challenge for health initiatives targeting MPS (Villegas, 2013). In general, financial constraints pose a major problem for health initiatives targeting this population, given the absence of sufficient public funding proven to ensure some measure of predictability and sustainability (Biffl & Altenburg, 2012; Ng & Hu, 2017; Yu et al., 2017).
Another important challenge identified was access to public services and the need to protect MPS from financial abuse and/or from being denounced to immigration authorities. Exploitative billing practices as a widespread phenomenon (Brabant & Raynault, 2012a) raise the questions about regulatory issues to standardize and monitor billing practices by the medical profession. As a first step, the Quebec code of ethics for doctors has recently included a specific article, requesting doctors to provide sufficient information for services not covered under the RAMQ (Code de déontologie des médecins, n.d.). Meanwhile, as per the recommendation by the Ministry of Health and Social Services, health institutions have issued policies clearly stating that noncitizens without a Quebec Medicare card (RAMQ) should be charged three times the regular cost of services rendered, regardless of their financial situation. It is our position, however, that such costs should, at least, not be higher for nonpermanent residents than the costs that are reimbursed to providers by the public medical insurance. The costs of this policy could be even greater for the health system, as people will tend to use health services only when their health situation is deteriorated, like a population study of uninsured populations in Toronto showed (Hynie et al., 2016).
In some European countries, where organizations are obliged to report undocumented migrants, confidentiality and anonymity are considered as major issues (Biffl & Altenburg, 2012). However, DoW can maintain anonymity in service provision, by only asking for first name, first letter of last name, date of birth, country of origin, and telephone number, even thus there is no obligation in Quebec nor across Canada to declare people’s status to immigration authorities. Notwithstanding, it remains difficult to guarantee confidentiality outside DoW parameters considering reports of cases within the health care system where immigration authorities have been seen to intervene (Solidarity Across Borders, 2013). The Toronto campaign titled “Access Without Fear: Don’t Ask, Don’t Tell campaign” serves as an example of policies and action plans developed by migrant-serving organizations to ban any workplace intervention by immigration authorities (Fortier, 2013).
Although the health care interventions discussed above offer suitable primary care, migrant-serving organizations continue to have to deal with constraints in health service provision in hospitals as well as elsewhere within the public health care system. Thus, access to obstetric care, specialists, and medication remains a major obstacle, regardless of city, care model, or type of regulatory restriction regarding service fees (Biffl & Altenburg, 2012). Staff impressions concerning suboptimal care and their inability to provide necessary follow-up is yet another important challenge faced by health professionals working with DoW. Similar results were found in health initiatives studied in the European context where health professional face the dilemma of accepting a greater number of undocumented persons with simple health conditions as compared with accepting fewer cases, but of people suffering from complex diseases (Biffl & Altenburg, 2012). In the case of DoW, the Organization wishes to reach those most in need but has good reasons to believe that this is not currently the case. Accordingly, a possible solution would be the operationalization of a mobile unit, which has proven efficient in addressing the needs of uninsured migrants elsewhere (Yu et al., 2017). Since data collection, a DoW mobile unit has begun its work in Montreal’s most remote and low-income neighborhoods. Meanwhile, services rendered may be further expanded to serve a greater number of vulnerable populations, including uninsured migrants. The main obstacle that remains to the use of the mobile clinic is one of acceptability, as MPS do not like to be associated with other hard-to-reach populations such as homeless and low income. To reach MPS that do not want to be found, DoW is trying to get its walk-in clinic known by engaging in outreach and linkage activities in many neighborhoods and communities on a long-term basis.
Access to Care for MPS in Montreal and Advocacy
Despite the invaluable nature of interventions for the uninsured to address health system gaps, such measures are taken under conditions of resource scarcity, rendering it impossible to adequately meet the needs of MPS. Moreover, response to MPS needs is heterogeneous in the health system. Some professionals adopt strategies that respect universal access to care and the physician’s code of ethics while others abuse shortcomings within the health system and exploit the vulnerable situation in which MPS find themselves. This raises major ethical issues (Giacomini et al., 2009), making DoW one of the only safe spaces for MPS to receive health care services in Montreal.
Issues pertaining to equity within the health system are central to this research. Research participants were very conscious of the limitations in intervention and the need for additional research and advocacy. In addition, to find a workable solution that respects both context and the law, myths about undocumented migrants need to be dispelled through open discussions within the public sphere (Rochefort & Cobb, 1993). Such discussions would also serve to raise awareness among vulnerable populations who are not adequately informed of their rights and help to bring their needs to the attention of the public. The absence of a clear sense of responsibility at the provincial and federal levels is also a major issue requiring due attention, especially given that this is a problem bearing consequences for both immigration (of federal and provincial jurisdiction) and the public health sector (of provincial responsibility). However, the problem persists due to a lack of accountability and the inability of those most affected to openly claim their rights—a situation very familiar to experts in the field of public policy (Rochefort & Cobb, 1993).
Close partnership with the main actors involved in this study is noteworthy and a primary strength, reinforcing the internal validity of conclusions drawn. Qualitative and quantitative results are found to be congruent and complementary, and results are validated through triangulation, further strengthening the study. Meanwhile, study limitations are as follows: First, as the study was carried out in a single setting with particular migration and health care access, results cannot be generalized to other setting. Second, given that the study is carried out in the early stage of the evaluation process with the aim to provide a better understanding of the intervention, it cannot yet evaluate the effectiveness of interventions carried out. Third, it is important to note that the current study is not inclusive of MPS perspectives, which is some work that we carried on afterward (Fête et al., 2019). Finally, as the actors introduce numerous innovations and are constantly adapting to a changing context, the results cannot be considered definitive and will need to be updated.
Conclusion
This study confirms that challenges faced by a Montreal-based NGO in providing care to uninsured MPS are caused by unstable funding and limited project resources—a phenomenon commonly observed among organizations working on improving immigrant’s health. Interventions are therefore constantly evolving, and its implementation is impending by challenges.
Health professionals taking part in this project face tremendous ethical dilemmas, which are sometimes dealt with by making comparisons with situations faced while working in humanitarian programs. It is therefore recommended that health-related social inequities, and potentially large-scale health implications for the general population, be considered when developing policies in this area. Access to health care by MPS is deemed a priority which necessitates public engagement and open discussions so as to collectively identify suitable solutions for reducing health inequities in Canada. Our research also underscores the need for expanding public health coverage for all. Where this may not be feasible, providing emergency care and treatment for infectious diseases as well as health care for pregnant women and children is of the highest importance. The experiences of European counterparts with similar projects also demonstrate advocacy as an integral part of policy change. Therefore, the advocacy work in the area of immigrant health requires further expansion to reach both the general population and policymakers. The production of knowledge translation tools such as videos and policy briefs, but also more direct interventions such as media appearance and meeting with Ministries should be part of a global advocacy strategy. Further quantitative research is needed in the areas pertaining to the mental and physical health, and health care needs of the population of MPS living in Canada, as well as the intersection between migration status and use of health services. Understanding the effects of different types of health interventions in the Canadian context is also highly pertinent, and would require nation-wide case studies. Finally, it would be important to give a voice to MPS to understand what are their main barriers in accessing health care and how to improve access to services.
Supplemental Material
Appendix_1_ – Supplemental material for Population Health Intervention Implementation Among Migrants With Precarious Status in Montreal: Underlying Theory and Key Challenges
Supplemental material, Appendix_1_ for Population Health Intervention Implementation Among Migrants With Precarious Status in Montreal: Underlying Theory and Key Challenges by Loubna Belaid, Magalie Benoit, Navdeep Kaur, Azari Lili and Valery Ridde in SAGE Open
Supplemental Material
Appendix_2 – Supplemental material for Population Health Intervention Implementation Among Migrants With Precarious Status in Montreal: Underlying Theory and Key Challenges
Supplemental material, Appendix_2 for Population Health Intervention Implementation Among Migrants With Precarious Status in Montreal: Underlying Theory and Key Challenges by Loubna Belaid, Magalie Benoit, Navdeep Kaur, Azari Lili and Valery Ridde in SAGE Open
Footnotes
Acknowledgements
We thank all the members of the DoW team for their availability during this study. Special thanks goes to Véronique Houle, Marylie Roger, and Sophie Richard. Thanks also to Lydie Diabri and Ludovic Queuille for their support in data collection and concept mapping, and to Normand Péladeau, Executive Director of Provalis Research, for graciously developing a module of his software for use in our statistical analysis. It is important to note that feedback from Marie-Éve Goyer, Marie-Jo Ouimet, Jill Hanley, and Marie Munoz on different versions of this article helped to improve it substantially. Thanks to Donna Riley for translation and editing support. No specific funding was used for this study. Magalie Benoit received a Rossiter Canadian Institutes for Health Research (CIHR) master’s scholarship.
Author Note
The author Navdeep Kaur is now affiliated to Centre de recherche du Centre hospitalier de l’Université de Montréal (CRCHUM).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by The Canadian Institutes for Health Research (CIHR), grant number 142332. CIHR The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.