
Abstract
A multigroup structural equation model was used to investigate the processes underlying health care use between Black and White children. Data from the 2003 National Survey of Children’s Health (NSCH), a computer-assisted telephone survey, were used. The sample for this research consisted of 28,064 Black and White children, ages 4 to 11 years, drawn from the larger pool of children whose families participated in the survey. Results showed that the processes underlying health care use were similar for Blacks and Whites; however, there were some differences in factor loadings between Blacks and Whites. Furthermore, there were differences between Blacks and Whites in the effects of (a) family economic resources on health problems, (b) health problems and access to care on parental distress, and (c) access to care and health problems on prevention- and curative-based use. No interaction effects were found for Blacks and Whites in the associations between (a) parental distress, and satisfaction with physician interaction and health care usage, and (b) satisfaction with physician interactions and health care utilization.
Introduction
There are significant racial/ethnic disparities in African American and non-Hispanic White children’s health care utilization; African Americans are less likely than Whites to utilize health care (Crocker et al., 2009; Flores & the Committee on Pediatric Research, 2010; Flores, Olson, & Tomany-Korman, 2005; Flores & Tomany-Korman, 2008; Piper, Glover, Elder, Baek, & Wilkinson, 2010). In addition, research on the factors associated with health care utilization, such as health problems (Mehta, Lee, & Ylitalo, 2012; Schuster et al., 2012; Waidmann & Rajan, 2000; Weinick, Zuvekas, & Cohen, 2000; Wen, 2007), family socioeconomic resources (Malat, Oh, & Hamilton, 2005; Mayberry, Mili, & Olifi, 2000; Smith, 2000; Wen, 2007), access to care (Flores et al., 2005; Mayberry et al., 2000, Shi & Stevens, 2005; Weinick et al., 2000; Zuvekas & Taliaferro, 2003), quality and satisfaction with physician–patient interaction (Blendon, Aiken, Freeman, & Corey, 1989; Chen, Fryer, Phillips, Wilson, & Pathman, 2005; Hambidge, Emsermann, Federico, & Steiner, 2007; Lillie-Blanton, Brodie, Rowland, Altman, & McIntosh, 2000; Mayberry et al., 2000; Stevens & Shi, 2003), and parental well-being (Centers for Disease Control and Prevention, 2008; Williams, 2000) reveal significant disparities between African Americans and their non-Hispanic White counterparts.
The present study extends past analyses by integrating the aforementioned constructs in a multigroup structural equation model (SEM; Figure 1) using a sample of African American (Black) and non-Hispanic White (White) children to understand the processes underlying health care utilization. Three questions were investigated across racial/ethnic groups: “Are the latent factors and causal associations (Figure 1) structurally equivalent (pattern invariance)?” “Do the indicators of the factors load similarly (factorial equivalence)?” and “Does race/ethnicity moderate the relations among predictors and outcome (structural invariance)?”
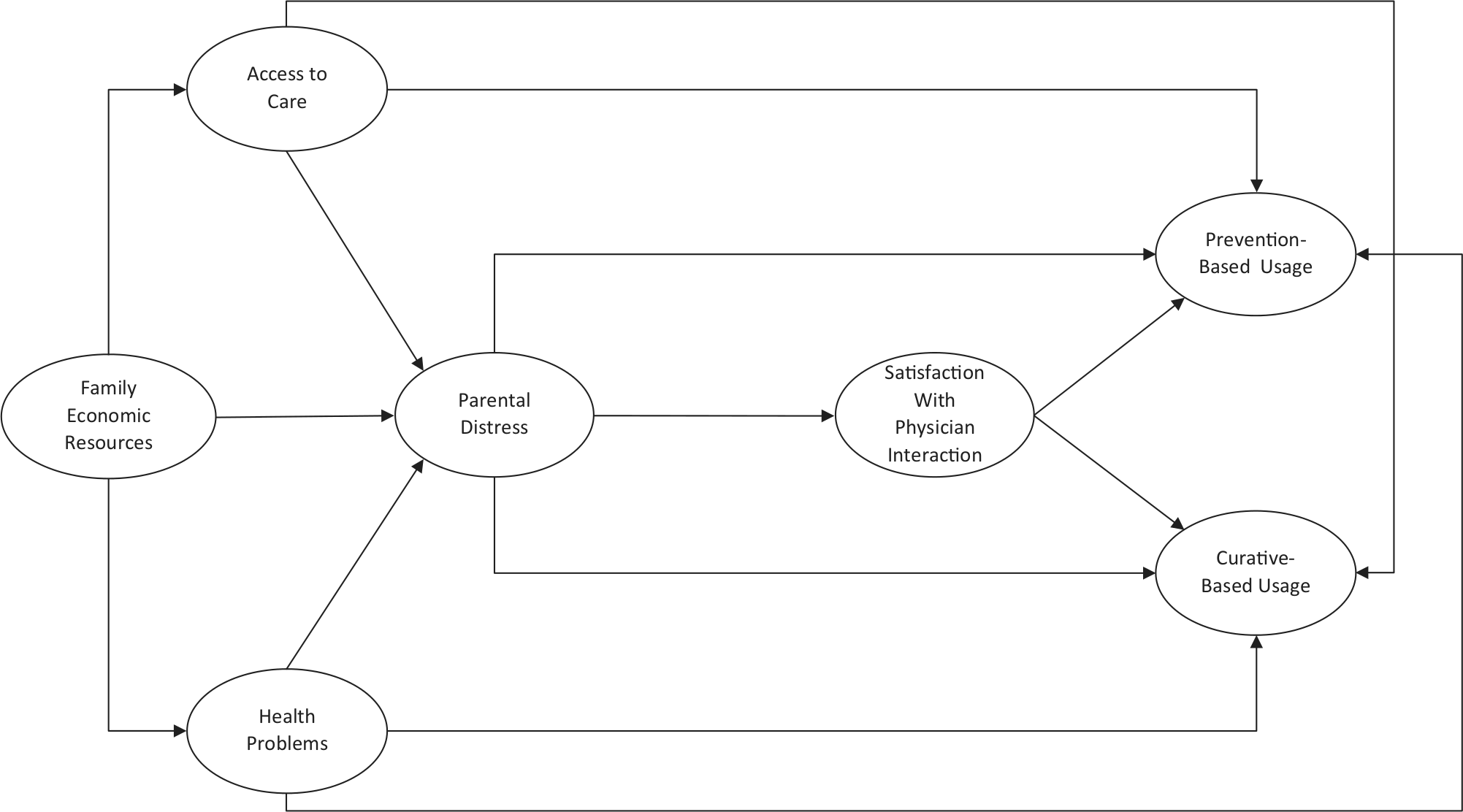
Model linking constructs to health care utilization.
Several reasons drive the interest in racial/ethnic disparities in children’s health and health care utilization. First, although attention is committed to health and health care disparities, little of such attention is focused on children (Flores & Tomany-Korman, 2008). Second, the evidence for ethnic/racial disparities is inconclusive; some studies report that racial disparities in access to care and utilization remain after adjusting for health insurance and socioeconomic status (SES; Currie, 1995; Zuvekas & Weinick, 1999). Other studies suggest that for all access-to-care indicators, there were no marked differences between Black children and their White peers after adjusting for income, insurance status, and usual source of care (Newacheck, Hughes, & Stoddard, 1996).
Furthermore, the mechanisms through which family economic resources, access to care, health problems, parental distress, and satisfaction with physician interaction interrelate to influence health care utilization are still poorly explicated. Given data and statistical constraints, a majority of prior investigations did not differentiate between preventive and curative utilization of health care, nor did they examine parental factors, health problems, access to care, and satisfaction with physician interaction simultaneously across racial/ethnic groups (Flores, Bauchner, Feinstein, & Nguyen, 1999; H. Kim, Kieckhefer, Greek, Joesch, & Baydar, 2009). A rationale-driven view of health care utilization (Aday & Andersen, 1974; Andersen, 1995; Scheppers, van Dongen, Dekker, Geertzen, & Dekker, 2006), whether prevention- or cure-oriented, may offer some insights into the differences in health care utilization across ethnic/racial groups.
Method
Data/Survey Design
The 2003 National Survey of Children’s Health (NSCH), a cross-sectional telephone survey conducted by the National Center for Health Statistics (NCHS), was used (Child and Adolescent Health Measurement Initiative [CAHMI], 2003). The NSCH was designed to produce national and state estimates for a variety of physical, emotional, and behavioral health indicators and measures of children’s experiences with the health care system (Blumberg et al., 2005). The NSCH used the sampling frame on the National Immunization Survey (NIS), a large-scale random-digit-dialed (RDD) telephone survey designed to collect immunization history for children. Households identified as having any children younger than 18 years of age were eligible for NSCH. When NIS/NSCH telephone numbers were called, regardless of whether an NIS interview was conducted, if children were in the household, one child younger than 18 was randomly sampled for the NSCH interview.
Data Collection/Sample
Computer-assisted telephone interviewing started on January 29, 2003, through July 1, 2004, resulting in 102,353 completed interviews. A letter was mailed prior to telephone calls. Potential responders used this number to alert interviewers that there were no children in their household, to ask questions about the study, or to complete an interview (Blumberg et al., 2005). Consent for participation was obtained when it was determined that a household contained an age-eligible child. The respondent was the adult in the household who was most knowledgeable about the sampled child’s health and health care. In a majority of households, the respondent was the child’s mother, father, or male/female guardian. For the present study, data on 28,064 Black and White children, ages 4 to 11 years, were used (Table 1).
Unweighted Descriptive Statistics of Study Sample.

Constructs
Family Structure
Family structure was coded into four family types: two-parent biological or adoptive family (1), two-parent stepfamily (2), single mother no father present (3), and other family type (4).
Child Gender and Age
Boys were coded 1, and girls were coded 2. The mean age of the African American sample was 8.13 years, and that of the non-Hispanic White children was 8.07 years.
Family Economic Resources
Three items were used as indicators of this construct: parental education, income–poverty ratio, and receipt of household cash assistance. Parental education was categorized as less than high school (1), 12 years or high school graduate (2), and more than high school (3). Income to poverty–ratio was derived by using household income, household composition, and family size. The derived measure was compared with Federal Poverty Guidelines (Blumberg et al., 2005). Income–poverty ratio was categorized in eight levels (1 = less than 100% of poverty level through 8 = at or above 400% of poverty level). The last item asked whether anyone in the household received cash assistance (0 = no, 1 = yes).
Satisfaction With Physician Interaction
Two items were loaded on this latent construct: How often does the child’s personal doctor or nurse (a) spend enough time with him or her and (b) explain things in a way that the parent and child can understand (1 = never through 4 = always)? The second question was only asked if the child was older than 3 years.
Parental Distress
Three items were used as observed indicators of this construct. The first question asked how well the parent was coping with the demands of parenthood (1 = very well to 4 = not well at all). The other two questions asked about parents’ general health status, and mental and emotional health (1 = excellent through 5 = poor).
Access to Care
Two items were used as observed indicators of this latent factor. The items asked whether the child had (a) any health insurance coverage and (b) a personal doctor or nurse (0 = no, 1 = yes).
Health Problems
Four questions answered were used as observed indicators of this construct. The observed indicators of this factor were based on yes or no questions (0 = no, 1 = yes) that asked whether the child has (a) limitations in the ability to do things, (b) asthma, (c) hay fever or respiratory allergy, or (d) food or digestive allergy. These questions were used as indicators of health problems because of the frequency of occurrence or report among children.
Health Care Utilization
The construct of health care utilization was separated into prevention- and curative-based utilization factors. Three items were used as observed indicators of prevention-based utilization, two of which were (1 = yes or 0 = no) questions that asked whether in the past 12 months the child has (a) had preventive medical care visits or (b) seen a doctor/health professional. The third question asked about the frequency of preventive medical visits in the past 12 months. In regard to curative-based utilization, three items were used as observed indicators of this factor, two of which were (1 = yes or 0 = no) questions that asked whether in the past 12 months the (a) child needed care right away for which medical care was sought or (b) the caregiver called a doctor/health professional for the child’s health problem. The third question asked about the frequency of visits to a doctor/health professional for health problems.
Data Analytic Approach
A four-step multigroup structural equation modeling was conducted using the AMOS 6.0 program (Arbuckle, 2005) with maximum likelihood (ML) estimation procedures. SEM (a) examines the degree to which a model agrees with the observed data and (b) enables the simultaneous investigation of the relationships among latent constructs and observed variables, and the assessment of indirect effects. A multigroup analysis gives a test of significance of group differences (Arbuckle & Wothke, 1999).
An unconstrained baseline model (Step 1) was used as a baseline model against which nested models in Steps 2 to 4 were compared using the chi-square difference test (a significant difference means the groups differ in some manner; Byrne, 2001). The baseline model was also used to assess whether the structural patterning of causal associations among the constructs were similar for Blacks and Whites. In Step 2 (invariant factor weights), all factor loadings were equality constrained to examine whether the factor loadings were similar across groups. Factor loadings that were group-invariant in Step 2 were equality constrained in Step 3 (partially invariant factor weights). In Step 4 (invariant structural weights), structural paths were equality constrained; this step examines group differences in regression weights. Steps 2 to 4 are analogous to testing for moderation effects in multiple regression.
Goodness of Fit
The goodness-of-fit indices were used to determine whether the model being tested should be accepted or rejected. The χ2 statistic was used to assess overall model fit; but the χ2 value is affected by sample size increasing the probability that a given model would be rejected. However, a significant χ2 is not a reason by itself to modify a model if other fit indices provide a good fit (Kline, 1998). Consequently, the comparative fit index (CFI), the root mean square error of approximation (RMSEA), and probability of close fit (PCLOSE) were used to augment the χ2 index. For a good fit, Hu and Bentler (1999) suggested a CFI value of at least 0.95 and a RMSEA of p < .06, and Loehlin (1998) argued for a PCLOSE of p > .05.
Results
Question 1: Test of Pattern Invariance
The fit indices—Table 2, χ2(df = 290) = 4227.43; CFI = 0.95; RMSEA = 0.02; PCLOSE = 1.00—for the baseline model (Step 1) show that it had a good fit to the data. The finding of a good fit means that the hypothesized associations among the latent constructs in the model and the observed variables used to indicate the latent constructs are plausible. Furthermore, it supports the notion that the processes underlying health care utilization operate similarly for Blacks and Whites.
Comparative Goodness of Fit for Models.
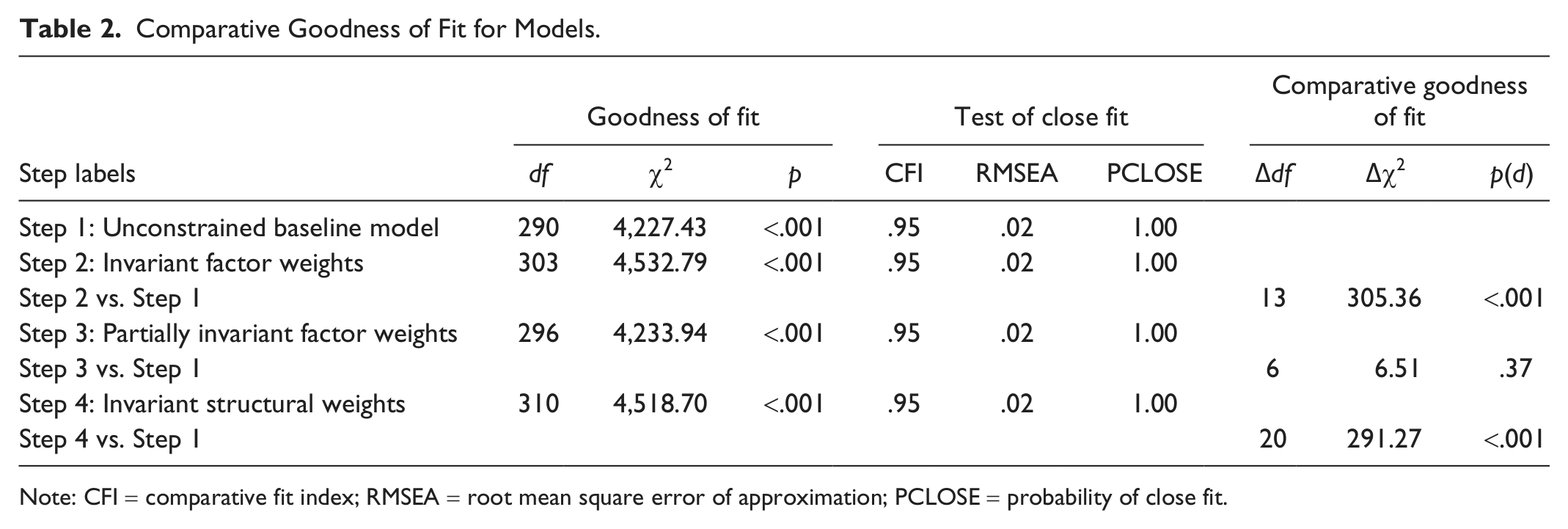
Note: CFI = comparative fit index; RMSEA = root mean square error of approximation; PCLOSE = probability of close fit.
Question 2: Test of Factorial Invariance (Differences in Factor Loadings)
A comparison of the baseline model against the invariant factor weights model (Step 2) revealed a significant difference between the models—Table 2, Δdf = 13; Δχ2 = 305.36; p < .001—signifying that some of the factor loadings differed between Blacks and Whites. Unstandardized factor weights were compared because using standardized weights can mask differences that may exist across groups (Kline, 1998). The observed indicator of parental mental and emotional health was strongly associated with parental distress for Blacks compared with Whites. The indicator for health insurance was more strongly correlated with access-to-care factors for Whites than for Blacks. The observed indicators of whether a child has seen a doctor in the past 12 months for preventive care and the frequency of doctor visits for preventive care in the past 12 months were strongly associated with prevention-based utilization for Blacks compared with Whites. Having hay fever or respiratory allergy and having food or digestive allergy were more strongly associated with the health problems factor for Whites than for Blacks.
Finally, the indicator of needing care right away was strongly correlated with curative-based utilization for Blacks compared with Whites. These patterns of item loadings indicate that the salience of some of the items differed across racial/ethnic groups, and underscores the differential experiences of Blacks and Whites. Factor weights found to be invariant were equality constrained in the partially invariant factor weights model (Step 3). A comparison of the partially invariant factor weights model with the baseline model showed that it did not have a significantly worse fit (Table 2, Δdf = 6; Δχ2 = 6.51; p = .37).
Question 3: Test of Structural Invariance (Interaction Effects)
A comparison of the baseline model against the invariant structural weights model (Step 4) revealed that some of the path weights differed across groups (Table 2, Δdf = 20; Δχ2 = 291.37; p < .001). First, the effects (Figure 2) of family economic resources on access to care were marginally stronger among Blacks than among Whites (z = 1.46, p = .07; Blacks, b = .03; Whites, b = .02). Family economic resources were associated with a marked decline in health problems among Whites than among Blacks (z = 2.42, p < .01; Whites, b = −.01; Blacks, b = −.003), and with a significant attenuation of parental distress among Whites compared with Blacks (z = 6.72, p < .001; Whites, b = −.03; Blacks, b = −.01).

Associations among constructs showing unstandardized (SE), and standardized coefficients (bold type face) for African Americans and non-Hispanic Whites, respectively.
Access to care was associated with a distinct decline in parental distress among Whites compared with Blacks (z = 2.46, p < .01; Whites, b = −.11; Blacks, b = −.03, n.s.), and with a significant increase in prevention-based (z = 2.33, p < .01; Whites, b = .50; Blacks, b = .17) and curative-based utilization (z = 4.92, p < .001; Whites, b = 2.92; Blacks, b = 1 .13) among Whites than among Blacks. Health problems were related to a marked increase in parental distress (z = 4.05, p < .001; Whites, b = .77; Blacks, b = .42), prevention-based utilization (z = 6.00, p < .001; Whites, b = 1.88; Blacks, b = 1.17), and curative-based utilization (z = 5.86, p < .001; Whites, b = 32.84; Blacks, b = 20.45) among Whites than among Blacks.
No significant racial/ethnic differences were found in the effects of parental distress on satisfaction with physician interaction and both prevention-and curative-oriented utilization. Specifically, parental distress was associated with a marked reduction in satisfaction with physician interaction (Blacks, b = −.32; Whites, b = −.34), prevention-based utilization (Blacks, b = −.11; Whites, b = −.13), and curative-based utilization (Blacks, b = −3.23; Whites, b = −3.03). As well, satisfaction with physician interaction was correlated with an increase in prevention (Blacks, b = .13; Whites, b = .15) and curative-based utilization (Blacks, b = 1.17; Whites, b = 1.25).
Discussion
Three questions were investigated: “Are the latent factors and causal associations structurally the same across racial/ethnic groups (pattern invariance)?” “Do the indicators of the factors load similarly across racial/ethnic groups (factorial invariance)?” and “Are there any racial/ethnic differences in the causal pathways linking health care utilization (structural invariance)?” First, the findings for pattern invariance suggested that the observed indicators of the factors are good representations of the underlying constructs, and that the processes linking those factors to preventive and curative health care utilization among Black and White children are analogous. In short, the processes that underlie health care utilization among Black children and their White peers appear to be similar in nature. Second, the observation of partial factorial invariance highlights the differential experiences of Black children compared with their White counterparts in regard to some of the indicators of the factors in the model.
In terms of interaction effects or structural invariance, the findings that family economic resources were associated with a much greater reduction in health problems and parental distress among Whites compared with Blacks support the view that at similar levels of economic resources, Black children compared with their White counterparts were more likely to have greater health problems (Newacheck, Stein, Bauman, & Hung, 2003; Weitzman, Byrd, & Auinger, 1999). Mehta et al. (2012), using a large national data set examining trends from 1998 through 2009, reported that racial/ethnic economic disparities have increased over time. Black parents may also experience heightened levels of emotional distress compared with their White counterparts as a result of economic pressures. The above finding is consistent with the view that White parents tend to be of higher SES than Black parents (Williams, 2000), and with the “causation argument” for family economic resource effects, which suggests that economic pressures are associated with parental distress and well-being (Link, Lennon, & Dohrenwend, 1993; Turner, Wheaton, & Lloyd, 1995).
The observations that health problems were associated with a much stronger increase in parental distress and health care utilization among Whites than among Blacks imply that (a) comparable experiences of child health problems may be more detrimental to the well-being of White parents and (b) White children with the same experiences of health problems may be more likely to utilize health services compared with their Black counterparts (Flores et al., 2005; Weinick et al., 2000; Zuvekas & Taliaferro, 2003). What explains the interaction between health problems and parental distress? It is possible that there are representational differences in parental views of children’s health problems. Some research (e.g., Eisenhower, Baker, & Blacher, 2005) suggest that children’s physical and emotional well-being may have implications for parental well-being. Further research may be needed to demonstrate whether the observed ethnic/racial differences in the association between health problems and parental distress are consistent.
Differences in health beliefs between Black parents and their White counterparts may explain the observed interaction between health problems and utilization of both preventive and curative health care. Health beliefs may mediate symptoms and health behaviors, such as seeking care (Welch, Botelho, & Tennstedt, 2011), because such beliefs form a schema that parents use to interpret children’s health problems.
The differential effects of access to care on parental distress and utilization of care suggests that (a) equality in access to care was more beneficial to the well-being of White parents than their Black peers and (b) at comparable levels of access to care, Whites were more likely to use both preventive and curative care than were Blacks (Flores et al., 1999; Weinick et al., 2000). Various explanations—at the patient, provider, and system levels—have been offered for the discrepancies observed in health care utilization (see Scheppers et al., 2006). For example, at the patient and provider levels, some relate to differences in the quality of care received, and interactional patterns between health care providers and patients (National Research Council, 2004), and others are associated with the ability to pay, or wait time for appointments (Scheppers et al., 2006).
That parental distress was associated with a decline in parental satisfaction with physician interaction, and health care utilization among Black and White parents is consistent with reports that parental psychological distress adversely affects perceptions of satisfaction with doctor–patient interaction quality and health care utilization (Ashiabi, 2008; Minkovitz et al., 2005). However, the finding is inconsistent with evidence that parental depression (Kinsman, Wildman, & Smucker, 1999; Mandl, Tronick, Brennan, Alpert, & Homer, 1999; Sills, Shetterly, Xu, Magid, & Kempe, 2007) or distress (Lipstein, Perrin, & Kuhlthau, 2009) are associated with increased health care utilization. No interaction was found in the association between satisfaction with physician interaction and health care utilization—a finding that is inconsistent with evidence that Blacks are more likely than Whites to report being less satisfied with the quality of physician–patient interaction (Blendon et al., 1989; Hewins-Maroney, Schumaker, & Williams, 2005; Lillie-Blanton et al., 2000; Mayberry et al., 2000).
Limitations of the Study
Although the present study adds to the existing literature, there are some limitations worth mentioning. First, given that this was a secondary analysis of survey data, it has the limitations generally encountered when using preexisting data. Also, the construct of health care usage employed in the study may not capture many dimensions of usage because of its restricted range. In addition, the construct of health problems does not incorporate all possible medical conditions children may experience, just some of the most common medical conditions children experience. Furthermore, the study was cross-sectional in nature; thus, it cannot address the longitudinal pathways to health care utilization. Another issue is that, although the hypothesized factorial and causal structures of the model were supported, equivalent models with different causal structures than those included in this study could also account for the variation observed. Another limitation was that the data used represented only a selection of age and racial/ethnic groups, so the results may not be generalizable to the entire U.S. child population. Because of data constraints, parental attitudes regarding perceived susceptibility and perceived severity of children’s health were not included in the model. Finally, the data set used did not directly assess respondents’ preferences for medical care and discrimination-related experiences that may impact utilization decisions.
Given the shortcomings of the present study, some recommendations are proposed to further the understanding of the causes of the racial/ethnic disparities in health care utilization. First, because gaps in access to care and a medical home adversely impact health care utilization (Cassedy, Fairbrother, & Newacheck, 2008; Hill, 2011), we need data on how both insurance status and medical home (as dynamic experiences) change over the course of time to impact racial/ethnic differences in access to health care and utilization.
Second, health beliefs and representations have been observed to differ along ethnic/racial lines (Y. Kim, Pavlish, Evangelista, Kopple, & Phillips, 2012; Sidora-Arcoleo, Feldman, Serebrisky, & Spray, 2012). The model of illness representation suggests that illness perception leads to planning of a course of action or coping responses, followed by appraisal of the success or failure of performance. Consequently, further research should incorporate parental illness beliefs and representations into models of health care use to examine how those beliefs and representations impact parents’ decisions to seek medical care. To further understand the “true causes” of racial/ethnic disparities and build on the current study, a multilevel analysis is needed that takes into account all the possible sources of disparities at the patient (e.g., education, income, health beliefs, and attitudes), provider (e.g., skills, behavior, communication style, and cultural knowledge), and system levels (e.g., appointments and waiting time, consultation and treatment, and opening hours; Scheppers et al., 2006).
Conclusion and Implications
Notwithstanding the aforementioned limitations, the following conclusions can be drawn from this study. First, the processes linking family economic resources, health problems, access to care, parental distress, and satisfaction with physician interaction to health care utilization are similar for both Blacks and Whites. Second, there is some evidence to support the differential health and health care experiences of Black and White children. Third, race/ethnicity moderated the effects of (a) family economic resources on health problems and parental distress, (b) health problems and access to care on parental distress, and (c) health problems and access to care on both prevention- and curative-based utilization. Fourth, race/ethnicity did not moderate the effects of parental distress and satisfaction with physician interaction on both prevention- and curative-based utilization.
In totality, these findings point to the following conclusion: When we adjust for the effects of family economic resources, parental distress, and satisfaction with physician interaction on health care utilization, White children with health problems or those with access to care are more likely to utilize health care than their Black peers. These findings highlight the fact that we still need to investigate sources of racial/ethnic disparities that lie beyond the domains of access and medical need.
Implications
Efforts to address disparities in health and health care use should be multipronged given the myriad of contributory factors. One approach could involve increases in income or cash transfer programs that enable families to invest in health care. Although such policies may be desirable, the level of implementation (local, state, or federal) is not clear (Williams & Jackson, 2005). In addition, policies involving income or cash transfers have to be evaluated to determine their effectiveness in reducing or eliminating disparities (Williams & Jackson, 2005). Finally, cash or income transfer programs, federal or state (Medicare, Medicaid, and State Children’s Health Insurance Plan [SCHIP]), do not deal with the noneconomic barriers to utilization. Consequently, it is also important to address noneconomic sources of disparities at the patient, provider, and system levels as well as the environmental and sociocultural factors that maintain and exacerbate health care disparities (Institute of Medicine, 2003).
Footnotes
Author’s Note
Data used were from the Child and Adolescent Measurement Initiative (CAHMI). DRC Dataset: 2003 National Survey of Children’s Health. Data Resource Center for Child and Adolescent Health, ![]() .
.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Author Biography