
Abstract
We assessed how the everyday work challenges that frontline health workers (FRHWs) face in the government health sector in northern Uganda influence their trust in the Ministry of Health (MOH). We employed qualitative research techniques, including interviews and participant observation, over a 9-month period to examine FRHWs’ viewpoints about how the MOH should address these challenges in service delivery. One hundred and sixty-five FRHWs, of whom 48 were recruited for extensive follow-up, participated in our study. Key findings include distrust in the MOH is prevalent among FRHWs, there is a lack of trust in the organization’s coordination role in service delivery and this affects health care delivery to patients, interrelations, and provider cooperation. Therefore, restoring trust in government hospitals will require a truthful non-violent response by the MOH in its contractual agreement with FRHWs. In our analysis, we employ Habermas’s Theory of Communicative Action.
Introduction
There is an ongoing debate about the role of trust and distrust in organizational performance, in particular, how trust influences access, retention, and performance within health care systems, as well as epidemic response and preparedness. Trust, or the lack thereof, influenced the preparedness for and response to the West African Ebola virus epidemic of 2015–2016. Distrust was reinforced by resentment toward governments and manifested itself in a denial [by the people at high risk] of the epidemic and resistance to disease control programs (Spencer, 2015). It has also been suggested that trust in the doctor–patient relationship mediates the likelihood of adhering to treatment, increases the probability of patient satisfaction, and improves patient health status while decreasing the likelihood of the patient leaving the physician’s practice or withdrawing from a health plan (Hall et al., 2001; Park & Akello, 2017; Pearson & Raeke, 2000). Further studies show how trust facilitates collective action and the cooperation of people to achieve goals. In other words, secure communication and dialogue builds the legitimacy and capacity of public systems (Coleman, 1990; Gilson, 2003; Putman, 1993). Trust enhances employee morale and motivation, and in turn, organizational performance (Gilson, 2003). When a patient trusts a provider, there can be a direct therapeutic effect, because trust facilitates disclosure and the patient may have greater autonomy and decision-making power (Mechanic, 1998).
The above-mentioned studies were conducted in high-income settings, which are characterized by relatively functional medical systems with efficient diagnostics and staffing. However, many anthropological studies outline the ineffectiveness, fragmentedness, and inefficiency of health care systems in developing countries. For example, Camaroff and Camaroff (2008) argue that health systems in contemporary African contexts lack legitimacy and need to identify new and creative solutions to improve health service delivery. Sjaak van der Geest and others have examined how weak health systems characterized by minimal state health sector spending lead physicians to over-prescribe and patients to self-medicate and/or over-medicate, including with antibiotics and sleep medicines (Akello et al., 2010; Hardon et al., 2004; Mulemi, 2008; Van der Geest, 1991; Van der Geest & Finkler, 2004; Van der Geest & Hardon, 1996). This can pose serious problems, such as the development of bacterial resistance as a result of the over-use of antibiotics at sub-optimal dosages (Hardon et al., 2004) and dependence on psychotropic medicines for everyday stressors (Akello et al., 2010). In Uganda, the informal uncontrolled distribution of pharmaceuticals is prolific due to poor service delivery in the public health sector and the continuous shortage of essential drugs in government hospitals. Furthermore, while it is the Ministry of Health’s (MOH, 2000, 2001) responsibility to recruit health workers and make them accessible to the entire population, many health centers in Uganda are understaffed (Uganda Demographic and Health Survey [UDHS], 2011). In effect, this makes it impossible to obtain an official prescription (van der Geest, 1991, p. 78).
To compound the problem, in many low-income countries, profits from sales of pharmaceuticals have become an important part of health workers’ incomes (Akello, 2010; Akello et al., 2010; van der Geest, 1991; van der Geest et al., 1996; Whitehead et al., 2001; Wolffers, 1995), and many frontline health workers (FRHWs) employed in government health centers run private clinics on the side. In this public medical sector, drug stores and peddlers also prescribe medicines for patients, who might receive prescriptions from hospitals but cannot obtain the medicines from them due to chronic stockouts (van der Geest et al., 1996). Whitehead et al. (2001) describe how a medical poverty gap is created, whereby there is an increasing poverty of those who are already poor due to increasing health spending.
Birungi (1998), while analyzing the breakdown of interpersonal and system-level trust within the Ugandan public medical sector, suggests that political and economic crises undermine the government health system. Popular distrust in the system of health care provision and funding thus influences trust in individual providers as well as personal health practices (Birungi, 1998; Gilson, 2003). While Birungi (1998) proposes a system-strengthening approach to restore trust, for instance, through openly sterilizing syringes, our article addresses relational, behavioral, and social approaches to restoring trust. If trust is a relational notion, in this case between FRHWs and the MOH, one urgent question is how to address the distrust in the public medical sector while focusing on public health approaches such as system strengthening and medical improvisation. Put differently, how can this public medical sector be transformed to improve health service delivery, while taking into consideration “the trustee demands” presented in Table 1; demands that are not egocentric calculations of success but which rather need acts of reaching (an) understanding (Habermas, 1984, p. 286)? By “reaching an understanding,” we mean participants in communication coming to an agreement with one another about something in the world without reservation (Habermas, 1984, p. 294). Furthermore, Habermas (1984), in The Theory of Communicative Action, argues that “what counts as fundamental is not the interpersonal relation between the at least two speaking and acting subjects” (p. 279). Rather, emphasis is placed on understanding language as the medium of coordinating action at the fore point of interest.
FRHWs’ Determinants of Trust in the MOH (N = 165).
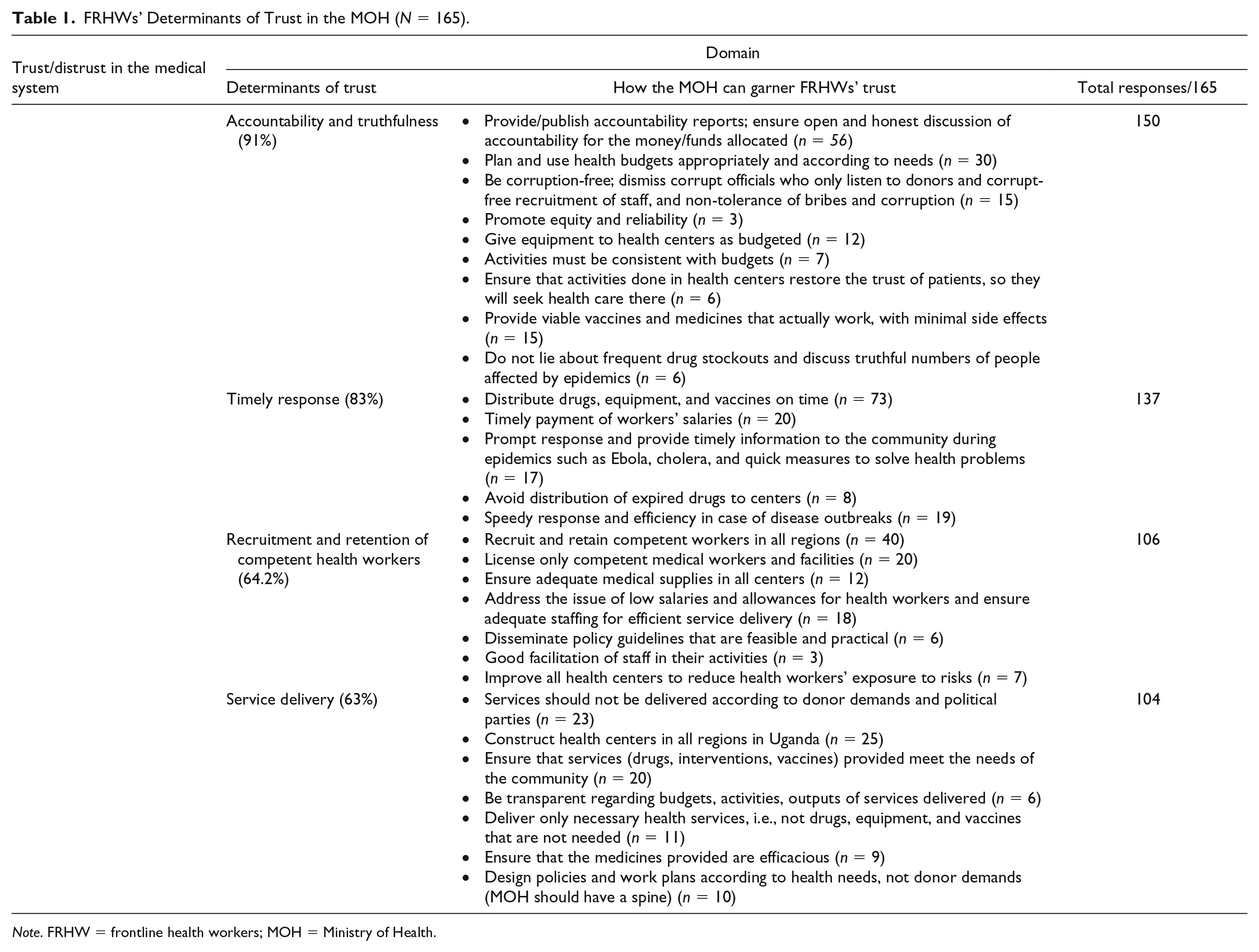
Note. FRHW = frontline health workers; MOH = Ministry of Health.
We will return to this theoretical argument in the discussion to suggest that addressing the factors identified by FRHWs would be an effective way of dealing with their distrust in the MOH and the government health sector. That is, when we analyze how to restore trust (i.e., achieve a transformation), we deliberately present the viewpoints of the weaker side (FRHWs), which are directed to the stronger side (the MOH), to align our arguments with Habermas’s (1984) analysis that a change—or more specifically a transformation—in asymmetric relationships happens only when it is publicly identified in the subjective language of the weaker side.
Conceptualizing Trust and Distrust
We conceptualize trust in a relational spectrum, whereby on one end of the spectrum is the notion of a moralistic or altruistic behavior rooted in explanations about how people should behave (Mansbridge, 1999; Ulsaner, 2001). In this regard, there can only be trust or distrust (Ulsaner, 2001). We perceive that altruistic trust mediates the dynamic in the patient–FRHW relationship. Although we will discuss altruistic trust in another article, restoring altruistic trust can be facilitated by FRHWs’ responding honestly and “non-violently” to patients’ frustrations and criticisms. By presenting a non-violent account to patients, FRHWs could garner their trust, deal with distrust, and ultimately achieve organizational legitimacy. This then would be a way of restoring order in the public health sector through an affective, emotional basis of trust. Altruistic trust is therefore derived from the belief that most people share fundamental moral values and that trusting behavior is morally worthy (Ulsaner, 2001). The expected outcome of FRHWs making an honest and responsible account to their patients would be affective trust, redistributive action and solidarity, sociability, and a vibrant and tolerant social community (Kramer, 1999; Rothstein, 1998; Ulsaner, 2001).
At the other end of the trust spectrum—which is our principal focus herein, we use the term “calculative, cognitive trust” to explain a more contractual, organizational type of relationship: in this case, trust between FRHWs and the MOH. Cognitive trust is expressed or can be met through the common values and norms of obligation for an organization (Lane, 1998). We therefore aim to analyze how trust could facilitate collective action and cooperation between key stakeholders in health care to achieve organizational goals. If the MOH’s role falls in the realm of service delivery, then as the trustor, its contractual agreement with the trustee (the FRHWs) should ensure that the FRHWs take into account its interests in service delivery (Warren, 2001). It is the role of the MOH to ensure what Giddens (1990) calls “faceless commitment,” and to monitor, discipline, and promote consistent behavior among its trustees. Analysts mention truthfulness as a way of promoting consistent behavior (Ulsaner, 2001; Warren, 2001). The outcomes of the MOH’s actions would be to reinforce its legitimacy and authority (Camaroff & Camaroff, 2008; Gilson, 2003). We will engage with the concepts of trust and distrust, and more specifically how the MOH can address FRHWs’ demands, in the discussion. But first, we will present the methodology.
Method
Study Design
We conducted a 9-month ethnographic and analytical study in northern Uganda from December 2016 to September 2017.
Study Setting and Participants
We recruited a purposively selected sample of 165 FRHWs between the ages of 26 and 67, with varying levels of experience, working in government health centers, missionary hospitals, and in private for-profit clinics in northern Uganda. Out of a total sample of 165 FRHWs, 48 were purposively selected for extensive follow-up through participant observation in health centers and multiple in-depth interviews, to verify the determinants of trust that FRHWs proposed, and which the MOH would need to address to garner FRHWs’ trust.
Of the 165 FRHWs (N = 165, n = 87 men, n = 78 women), this included clinical officers (n = 26), nurses (n = 57), laboratory assistants (n = 22), nursing assistants (n = 23), and midwives (n = 37). The rationale for the purposive selection of FRHWs was our interest in a variety of experiences in service delivery. Although a substantial proportion of the interviewed workers had resigned from their appointments citing appalling work conditions and low remuneration by the MOH, many FRHWs remained committed to service delivery under these very conditions.
Data Collection
We conducted individual interviews, asking open-ended questions including, What are the key challenges FRHWs face in service provision? And given the challenges in their everyday practice, what are the key determinants for their trust in the MOH? We then conducted multiple interviews, participant observations, and hospital visits with FRHWs who were willing to discuss their experiences with us in more depth, until we reached a saturation point with consistent and similar responses. In essence, this ethnographic study over a 9-month period followed what Biehl (2013) describes as “conducting ethnography” as a way of staying connected to open-ended and even mysterious social processes and uncertainties, and to counterbalance the generation of certainties, as well as foreclosures, by other disciplines (p. 590). Doing ethnography was an opportunity to explore knowledge through an intersubjective process of sharing experiences and finding common ground (Jackson, 1996). We wrote fieldnotes depicting FRHWs’ challenges in service delivery, and recorded interviews where the respondents gave permission for us to do so.
Participant Observation
We conducted 5-day participant observation exercises in each of the eight purposively selected health centers. Participant observation is a strategy that provides richer and more thorough data than other data collection techniques when conducting research (Carnevale, 2013; Carnevale et al., 2008). In this dynamic, the researcher is both a participant and an observer, who is engaged in the activities in the setting and has informal conversations with the participants that contribute to data collection that is more contextualized (Morse, 2016; Phillippii & Lauderdale, 2018). Although Becker (1967) argues that a social scientist is on the side of the subordinate, we did not choose the side of the FRHWs, and neither the superordinate (MOH); instead in this ethnographic study, we positioned ourselves to observe what happened during the encounters between the FRHWs and the MOH including those encounters published in the MOH website, National Newspapers including, The New Vision (see Fassin, 2013). In this article, we then relate findings to the larger picture of communicative action within a public health sector. Generally, we reached a saturation point in our observations, as the patterns remained similar over the days during which we observed activities in the selected centers. In seven health centers, we observed how clinical officers, nurses, and nursing assistants interacted with patients in the outpatients’ units. In one hospital, we observed midwives and nurses offering care and support in the antenatal and general medicine wards. Key areas in our observation checklist included time of staff reporting to work; time of closing the health center; how FRHWs responded to patients’ inquiries; how they expressed their frustrations in offering care in the government hospitals, for instance, in an over-crowded maternity ward; and how they addressed the issue of drug stockouts. We then engaged in a discussion with the FRHWs concerning how the MOH could address challenges in the public health sector to garner their trust. Through observing and reviewing the MOH’s media responses to FRHWs’ demands, we were able to see how the power dynamic between the two parties needs to be redressed.
Data analysis
Fieldnotes and digitally recorded information were manually transcribed and organized according to recurring thematic categories (Bernard, 2006). We categorized recurring themes in the FRHWs’ narratives depicting their distrust in the MOH into what we call “determinants of trust,” as presented in Table 1.
Ethical considerations
This study’s protocol was presented to, and approved by, St. Mary’s Hospital Lacor (LHIREC 016/07/16). St Mary’s Hospital Lacor is accredited by the Uganda National Council of Science and Technology to review and approve studies conducted in northern Uganda. Prior to conducting interviews with FRHWs, additional permission was sought from St. Mary’s Hospital Lacor, Gulu Regional Referral Hospital, the District Health Office and Gulu Municipal Offices to fulfill all of the requirements for conducting studies in the selected health centers. The FRHWs we approached for interviews consented to the study and were willing to be observed and interviewed a multiple number of times.
Findings
We will first present a summary of the qualitative data obtained through the interviews with FRHWs working in government, missionary, and private for-profit health centers. We asked open-ended questions, yielding multiple responses about the challenges that FRHWs experience, how these challenges influence their trust in the MOH, and given these challenges, what the MOH could do to garner their trust. We will also present verbatim some of the FRHWs’ narratives as well as descriptions of the data obtained through participant observations.
The data in Table 1 show that there are numerous challenges that FRHWs face within the government medical sector, which account for low health worker morale, irresponsibility, and inaction in terms of achieving the organizational goals of health service delivery.
Challenges in the Government Medical Sector
As seen in Table 1, the key determinants of trust/distrust in the MOH that the FRHWs identified were accountability
1
and truthfulness (150/165 = 91%), timely response (137/165 = 83%), recruitment and retention of competent staff in various health centers (106/165 = 64%), and service delivery (104/165 = 63%). In the FRHWs’ narratives, the MOH is depicted as having limited focus to address both internal and organizational/system issues as well as the needs of the people it aims to serve. Indeed, we observed frequent drug stockouts in health clinics, one example of such a limitation. In addition, 36 FRHWs mentioned that the MOH frequently supplies drugs and equipment that are not needed. We too observed vaccines and medicines that were about to expire in the eight health centers where we conducted participant observations. One clinical officer
2
in a government hospital, upon being asked why he always prescribed an expensive antimalarial to resource-poor patients, expressed his dismay at policy guidelines drafted in 2005 (MOH, 2005) recommending that Coartem be prescribed as the first-line drug for uncomplicated malaria, which the MOH then distributed to hospitals in early 2006, in the following terms: . . . Just one morning, we were called for a meeting in which the medical superintendent explained new guidelines for prescribing in case of uncomplicated malaria. In this meeting, it was shocking to us how we were going to start telling people to buy Coartem for their [uncomplicated] malaria. Here in Gulu, many people were living in camps, and they could not even raise money for the usual chloroquine and fansidar we were prescribing, which at that time was only six hundred shillings [approx. 0.02 USD]. But the MOH designed guidelines that we will start prescribing Coartem, which was about twenty thousand shillings then [approx. 8 USD]. Since that day, I find it difficult to trust the MOH.
One nurse also discussed her experiences of waste in the system, explaining how the MOH frequently delivers unnecessary drugs and supplies that are not in line with local needs: Sometimes it is difficult to trust the information which the Ministry of Health disseminates. I have been working in this hospital for many years, and I am about to retire, but for the past few years it is becoming very common to receive vaccines and medical supplies which are remaining with two months to expire. When you raise a question, they say you can at least use the medicines until four months later [after the expiry date]. Some of the batches received are of drugs which we do not need, yet we submitted the exact items which we frequently use. Maybe that is why many people are not getting well, even for simple diseases like malaria. But the next thing you hear . . . Oh there is this malaria which does not respond to all types of medicines. It is now an epidemic in northern Uganda. Very many children are dying . . .
During interviews, two nurses mentioned how they were surprised to hear the MOH reporting that only three people had been affected by cholera during the previous rainy season, yet they had treated over 26 people in the emergency care unit for cholera. “How can one trust the MOH ever again if we keep on reading about those false figures?” one of the nurses questioned.
Another nurse discussed her frustration in service delivery as follows: . . . in this hospital it is now just normal to have very many plans to take the vaccines to communities through our outreach program, which never materialize. If you are lucky to have the vaccines, the car will not have fuel, the team members will be complaining of the so many activities they participated in and they have never been paid, and one time, the vehicle allocated for this outreach could not even start. So we had to unpack everything we had prepared and abandon the entire mission. Remember, we were trying to make sure the community receives the vaccines before it expires.
In the antenatal ward, where there has been rigorous training and advocacy for mothers to stop dangerous home delivery practices, and the option of consulting with traditional birth attendants is discouraged, one midwife explained the situation: . . . I think more women are exposed to infections in this hospital during deliveries compared to if they had gone somewhere else or even given birth in their homes. See for yourself. The cleanliness of this ward has always been an issue. Even cleaners complain that there are no detergents and they have to work without them for weeks. How can one expect to do an efficient job with such conditions? Sometimes we are allowed to see budgets in this hospital, but it is rare that that money is received on time. Many activities are affected because the MOH does not release funds on time.
Participant Observation in Health Centers
By observation, in selected government health centers, nurses, nursing assistants, midwives, clinical officers, and laboratory assistants have to attend to patients under dire circumstances characterized by dilapidated hospitals and health centers, a lack of equipment, and frequent stockouts of vaccines and medicines. In their everyday practice, they must account to the higher decision-making body—the MOH—whom, as their narratives show, is donor-driven, disorganized, and needs revamping and major transformation.
Apart from the maternity ward in one hospital, all of the FRHWs observed reported late to duty, and we observed seven in-charges open the health center after 11 a.m., despite the fact that we had been waiting from 8 a.m. Two nurses argued that they did not see the reason to open early when they had none of the medicines or vaccines that their clients needed. Three nurses were observed beating and yelling at women in labor. They expressed their frustration at women who were unaware of the dirtiness of the floors in the antenatal wards. 3 Although the women patients reasoned that such behavior was a way of ensuring that no mistakes were made on the ward, they nevertheless discussed extensively how the nurses in that ward were rude and violent and uttered all sorts of abuse at them, not only during labor but also when they reported for regular check-ups.
In more than 10 observation exercises in outpatients units, clinical officers did not send their clients for laboratory tests to verify or confirm their illnesses. Three clinical officers gave diagnoses for malaria based only on symptoms of fever and headache. They argued that the health centers had not had the reagents needed in the laboratory for many months. In two health centers, the laboratories remained closed during the 3 days that we conducted a participant observation exercise. Some clinical officers referred patients to other hospitals and clinics with functional laboratories. Four laboratory assistants sent patients home, after they had waited for the entire day for their results, because they did not have all of the required reagents. To one patient, a laboratory assistant only screamed back in frustration: “I told you your results are not ready. Come back tomorrow!”
Responses From the MOH to FRHWs’ Demands
The MOH in Uganda is not unused to challenges ravaging its health sector as well as frequent strikes by health workers demanding improved working conditions and salary increments. For example, the MOH released a press statement on its website (www.moh.co.ug) on November 7, 2017, informing how “the Minister of Health declared Uganda Medical Workers’ industrial action illegal. She also issued an ultimatum for the medical personnel [to] resume their duties.” There were no attempts to address the health workers’ demands, which were cited as “poor work conditions in facilities and low pay.” In the recent past, the MOH has responded to such actions with promises to address FRHWs’ demands, but it did not act, leading FRHWs to doubt the truthfulness of its response. In many FRHWs’ meetings with the MOH, in which their challenges have been shared, the MOH has also identified the leaders and subsequently threatened them with dismissal. In summary and as shown in Table 1, the MOH exhibits indifference to FRHWs’ needs, lacks particularity in attending to patients’ needs, discourages freedom of speech by threatening FRHWs who strike with dismissal, and supplies vaccines that are expired and drugs that are not needed. These actions all suggest that the MOH is detached from its local, social, moral, and ethical obligations in service delivery.
In another incident in November 2017, MOH press reports showed images of the MOH preparing to build a new medical store in Kampala, after it had received many complaints about the distribution of expired and near-expired medicines and vaccines (see www.newvision.co.ug, November 7, 2017), yet the problem of expired drugs is also experienced in Kampala. And then in February 2018, the MOH also had a stand-off with the NTV media group in Nakaseke district when it persistently denied that people were being affected by a DRC strain of Crimean fever, even when local media were broadcasting all of the experiences in the affected health centers and how medical workers had fled the district. Later, the MOH reluctantly admitted that up to 8 people had died of the DRC strain of Crimean fever and ordered the medical workers to report back to work.
Generally, the way in which the MOH responds to FRHWs’ demands has fueled distrust and ultimately has a negative impact on service delivery. In the next section, we employ Habermas’s (1984, p. 286) Theory of Communicative Action to enable us to gain insights concerning the possibility of reaching an understanding in this medical system and working toward transformation, as the FRHWs’ demands are not primarily oriented toward their own individual success, nor are they pursuing their own individual goals.
Discussion
Trust is an important parameter in health service delivery, because like all corporate institutions, there must be confidence and mutual understanding to meet the organization’s objectives. This mutual understanding is contractual in nature, with pre-conditions to achieve the organizational objectives as identified by the leadership/contractor (the MOH) for the led/trustee (FRHWs). In a biomedical system, trust or distrust is mediated by the extent to which contractual conditions for improved service delivery are met; such conditions address infrastructural issues (i.e., hospitals, equipment, medicines, vaccines), processes/guidelines, and health workers’ needs, including working conditions, remuneration, and skills development. The MOH recruits health workers with a promise that it will ensure that the conditions necessary for this task exist. Any deviation from this contractual agreement creates distrust among FRHWs, and significantly affects the MOH’s legitimacy and credibility. In turn, the health workers deployed in these appalling conditions cannot trust the MOH, as the contractual conditions have been breached. Trust in this case may imply confidence in the individual or the MOH as an organization, but its absence implies an urgent call or demand for the MOH to conduct itself in a manner that will restore its legitimacy and authority.
We argue that as FRHWs’ demands are not “oriented to their own individual success, and individual goals, but instead a focus to harmonize their plans of action suggesting a common understanding” (Habermas, 1984, p. 287), distrust in the biomedical system can be mitigated through an effort whereby the powerful side—the contractor (MOH)—listens and addresses the demands raised by the weaker side (FRHWs). In our findings, we see what Habermas (1984) describes as follows: “With imperatives the speaker [the FRHWs] refers to a desired state in the objective world, and in such a way that he would like to get H [the Hearer/MOH] to bring about this state” (p. 325, original emphasis). In our case, we have the MOH and FRHWs as the two speaking and acting subjects, whom we presume will understand a linguistic expression in the same way. To understand what a speaker wants to say with a speech act, the hearer has to know the conditions (moral, material, interpersonal) under which it can be accepted. When a speaker accepts a speech act, then an agreement comes out between at least two acting and speaking subjects (Habermas, 1984, p. 307).
Our findings suggest that distrust in the MOH is prevalent among FRHWs (Table 1). FRHWs’ arguments in relation to the MOH relate to what Habermas (1984) calls “a claim to power vis-a-vis the addressee in order to get him to act in such a way that the intended state of affairs comes into existence” (p. 286). FRHWs’ narratives also reflect a lack of trust in the organization’s coordination role in service delivery. This severed social relationship consequently affects health care delivery and patient–provider cooperation and interactions (Cahn, 1997; Gilson, 2003). In light of our findings, we will also anchor our analysis on Judith Butler’s (2005) concept of giving an account of oneself, to argue that restoring trust in government hospitals in northern Uganda will require a truthful non-violent response by the MOH in its contractual agreement with FRHWs. In this regard, the powerful party (the MOH) accounts to the powerless (FRHWs) in an experiment to transform and restore organizational legitimacy in service delivery. In effect, we argue that restoring trust in the public health sector will be achieved through a responsible, truthful, non-violent account made by the powerful to the weaker side (Habermas, 1984).
In proposing that the MOH should address the demands of the weaker side (Habermas, 1984)—as they themselves identify—we suggest that the MOH offer transparent accountability and ensure improved service delivery. According to Habermas, listening to the weaker side will enable the MOH to transform, as the focus will shift to addressing its internal qualities and contractual conditions, and to exploring how to modify recommendations in the trustees’ (FRHWs’) narratives. For example, it is possible for the MOH to report truthfully when epidemics occur, regarding both the numbers of those affected and how to control them. This would help to restore health workers’ trust in the organization.
Put another way, without the MOH addressing its own internal system and organizational challenges, as couched in FRHWs’ viewpoints and expressed in experiential subjective language, organizational transformation will not be possible. This argument resonates with Laverach and Manoncourt’s (2016) assertion that in a context of fear, mistrust, and resistance due to experiences of poor-quality health care, utilizing bottom-up approaches to communication that respect local knowledge would be more effective than those that are top-down and experience-distant. Similarly, Richards et al. (2015) argue for continuous consultation with the community, rather than viewing local customs and cultures as barriers. To be sure, we recommend that although FRHWs’ ideas (Table 1) represent uncomfortable knowledge (cf. Rayner, 2012), these ideas can no longer be excluded from current health policy debates, especially when addressing challenges within the Ugandan state-run biomedical system.
FRHWs’ narratives show that they expect the MOH in its leadership role to engage in the provision of health services in a timely, transparent, and context-sensitive manner. In the case of one of the interview excerpts above, the FRHW states that the national policy shift toward Coartem lacks an understanding of the economic conditions and possibilities of the country, and therefore demonstrates a neglect by the MOH of its responsibility of care toward patients. If health services are a collective good, which the government of Uganda provides through the MOH, then health workers’ lack of confidence—and lack of trust—calls for a transformation in the MOH’s approach to service delivery.
Judith Butler’s (2005) argument about “experimenting otherwise” further enables us to approach in a different way the task of gaining an understanding in this asymmetrical power bind between the MOH and FRHWs. Butler describes transformation as an “experiment in living otherwise.” The experiment takes the form of practicing non-violence in an emphatically non-reciprocal response, of refusing, in the face of violence, to return it (Butler, 2005, pp. 99–100). Thus, there is a sense in which this responsibility is said to refuse violence, to practice non-violence in the face of violence. Our central argument is therefore that both FRHWs and the MOH can transform through acting differently when providing care and delivering services in Uganda’s medical sector.
The MOH Attending to FRHWs’ Demands
Our theoretical contribution lies in how to restore trust in spite of the defectiveness of the biomedical sector in northern Uganda. In particular, our starting point is the various factors that FRHWs identify which affect their trust in their contractor, the MOH. When we propose that the MOH should address FRHWs’ demands in a bid to transform the medical system and reach an understanding in terms of how to improve service delivery, our discussion resonates with Habermas’ (1984) approach to finding concrete ways of transforming organizations through listening to the weaker side. In effect, the powerful, voluntarily and without being fearful and intimidated, addresses the contractual demands of the powerless. By implication, the MOH will take into serious consideration FRHWs’ demands and address the challenges that health workers experience in everyday practice. Doing so will enable the MOH to garner legitimacy, trust, and credibility as a contracting organization.
Evidence from this study suggests that the MOH tends to give a “violent response” when addressing its organizational challenges and has neglected and ignored the plight of FRHWs. Despite this, because FRHWs find it very difficult to work within this inefficient organization (in terms of policy, leadership, decision making, structures), they nevertheless suggest ways of transforming the organization. The determinants, namely, accountability and truthfulness, timely response, service delivery, and transparent recruitment and retention of health workers (Table 1), are further operationalized to specifics and activities that the MOH can implement. For instance, the MOH could ensure that drugs and vaccines that are delivered to health centers are not close to or past their expiration date, that the drugs that are procured and distributed are consistent with local needs, and that they are effective and produce minimal side effects. Furthermore, when there is an epidemic such as cholera or Ebola, the MOH’s response should be prompt and people at risk, as well as the general public, should be alerted. As long as the dimensions of trust are understood not as a demand that the MOH makes an account of itself to “outsiders” (i.e., “foreign” donors or interests), but that it should engage in internal reflection and report to the powerless side that it leads and coordinates, then we presume that organizational transformation will be a continuous process, whereby the MOH strives to be accountable to itself in its prime role in health service delivery. This then is the essence of organizational responsibility.
Accountability, as discussed, will be understood as a continuous process of reflectivity. This will imply that useful and new parameters, such as prompt drug supply to health centers, improving work conditions, and salary increments, will provide the premises for an evaluation by the MOH of its own performance, each time assessing whether its performance is consistent with the needs of the weaker side, that is, the FRHWs in government hospitals.
Connectedly, in the press statement quoted above, the MOH’s response to a strike by doctors and FRHWs over low pay and poor working conditions was one of “violence”: They contacted a lawyer and issued a threatening statement about their employees’ so-called “illegal activity” (and even suggested impending dismissal of those workers involved). By reversing this form of irresponsibility, we suggest, the MOH can choose to approach the addressee in the spirit of transforming itself as an organization.
Recommendations for Addressing Organizational Challenges
In this view, the MOH will craft a response in a “deliberate acting otherwise or in another way” (cf. Butler, 2005), with the main objective of achieving organizational goals and transforming the organization itself. What is more, a crafted response could entail what FRHWs themselves can do to make a contribution to transforming Uganda’s biomedical sector. There will be mutual trust—a restoration of trust even—in this mutual act of self-making or self-crafting by both the MOH and FRHWs. Mutual trust attained through dialogue and a non-violent response will ultimately lead to what Camaroff and Camaroff (2008) describe as an identification and creation of innovative solutions experienced by a health system which has lost its legitimacy.
Herein, the MOH should give an account specifically explaining how the system is weakened, and what it can and cannot do to resolve the pertinent issues raised by FRHWs. For instance, the MOH as a contractor could decide to raise FRHWs’ salaries, albeit gradually, to improve employee morale. The MOH could also decide to address the trustees’ demand for equipment in government hospitals that is needed in everyday care. That the MOH would be able to account to the FRHWs would signify responsibility, because regardless of whether all issues would be resolved or not, the health system would be strengthened, and its ability to perform tasks and “experiment with service delivery” would be appreciated by all stakeholders. Our expectation is that this way of working would restore trust in care and caregiving in Uganda’s public health sector.
In line with the responsibility toward the key goal of transformation, whereby the powerful works toward self-improvement, the MOH needs to see FRHWs’ narratives as suggested guidelines or premises that it can adapt to improve its performance and strengthen the weakened biomedical system. The key contractual conditions identified by FRHWs include accountability and truth telling, timely response, service delivery, and transparent recruitment of competent staff. These contractual conditions are not static, and by implication, the MOH will exhibit flexibility and adapt to the changing demands in a non-violent and responsible way. Thus, although it appears that the MOH, in its organizational leadership capacity, is presently engaged in what Rayner (2012) describes as addressing unknown known challenges in the public health sector, it is now time for the MOH to define concrete (rather than clumsy) solutions for the serious problem of poor performance within its biomedical sector by giving an account to the FRHWs, with the objective of transforming the system. For example, where FRHWs demand for increased pay and improved working conditions, the MOH will not threaten them with dismissal, but will instead honestly explain its current capabilities or lack thereof in terms of meeting FRHWs’ demands.
Conclusion
We aimed to analyze how trust could facilitate collective action and cooperation between key stakeholders in Uganda’s public health sector to achieve organizational goals. Key stakeholders represented here are FRHWs and the MOH. In this dynamic, the MOH is the contractor and the FRHWs are trustees. Findings show how FRHWs did distrust the MOH because of their everyday challenges in service provision within the government biomedical sector. We argue that the MOH can restore FRHW trust by meeting its contractual obligations and offering the addressee/trustee a non-violent response, particularly when the addressee objects to the current state of things in the organization. In this vein, the MOH could offer consistent explanations about the defectiveness of the biomedical sector, improve FRHW morale through salary increments, and attend to the reported challenges that hinder effective health care delivery. This is what we call transformation in performing organized health service delivery. We frame our analysis within the Habermas (1984) theory of communicative action to suggest that real organizational transformation of this public health sector will occur only when FRHWs’ demands are considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded under the German Research Foundation Program “Infectious Diseases in Africa” with the grant numbers BE5682 4-1 and PA2647/2-1. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.