
Abstract
Research evidence is incompletely translated into clinical practice. This study aimed to explore research needs from clinicians’ perspectives in the field of bipolar disorder and their reflections on patients’ research needs as well as to unravel the potential role of researcher-clinicians, to narrow the research practice gap. Using focus group discussions (FGDs) and interviews, research needs according to psychiatrists, psychologists, and nurses working with bipolar disorder were explored. Subsequently, we interviewed researcher-clinicians to gain insights into their views on patients’ research needs. The clinicians’ research needs were clustered as: causes, diagnosis, pharmacotherapy, nonpharmacological treatment, recovery, and care system, and overlapped with the research needs formulated by patients. Researcher-clinicians were able to translate patients’ needs into feasible research questions. Researcher-clinicians can serve as intermediaries between research and practice and can both integrate their practical experience into research and their research experience into practice.
Keywords
Introduction
Bipolar disorder (BD) is a complex psychiatric disorder, characterized by recurrent episodes of (hypo)mania and depression alternating with euthymic intervals. It affects more than 1% of the population worldwide (Grande, Berk, Birmaher, & Vieta, 2016). In the Netherlands, the estimated lifetime prevalence is 1.3% (de Graaf, ten Have, van Gool, & van Dorsselaer, 2012). BD is disabling due to its early onset, severity, and chronicity (Ferrari et al., 2016) and the functional impairment even in euthymic phases. Moreover, BD leads to a reduced quality of life for patients and their caregivers (Granek, Danan, Bersudsky, & Osher, 2016). These consequences could be partly overcome by treatment, which is considered to reduce symptoms and improve functioning and the quality of life (IsHak et al., 2012; Sylvia et al., 2017). However, it remains challenging to diagnose and treat BD (Henry et al., 2013), due to the complex course and the heterogeneity of the disorder.
In modern mental health care, care is often provided according to the prevailing paradigm of evidence-based medicine (EBM). The cornerstone of EBM is practicing health care based on the best available research evidence (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996) to “de-emphasize intuition” and “unsystematic clinical experience” (Guyatt et al., 1992, p. 2420). In this paradigm, randomized controlled trials (RCTs) are central in acquiring this evidence (Darlenski, Neykov, Vlahov, & Tsankov, 2010) and are, along with meta-analysis and systematic reviews, considered the gold standard of research (Rycroft-Malone et al., 2004). These research findings are often translated into treatment guidelines, which are a tool to support clinical decision making based on research evidence (Hay et al., 2008; Weaver, 2015). Research has resulted in a greater understanding of the disorder. However, the effect of this understanding on the effectiveness of mental health care is considered questionable (e.g., Henry et al., 2011), and the evidence is not always easily translated into clinical practice (Green, 2009; Kazdin, 2008; Rosner, 2012), leading to a gap between research and practice (Henry et al., 2011).
It is increasingly acknowledged that to bridge the gap between research and practice, it is beneficial for several reasons to include patients in research as end users—as “someone who will consume, use or work in the specific health field under research” (Elberse et al., 2012, p. 232). First, it improves the clinical relevance of research and the acceptance of the research outcomes (Abma & Broerse, 2010; Elberse et al., 2012), and second, it contributes substantive new knowledge, owing to patients’ experience of living with the illness and their need for care (Broerse, Zweekhorst, van Rensen, & de Haan, 2010; Tait, 2005). In a previous study, we explored the research needs of patients with BD (Maassen, Regeer, Bunders, Regeer, & Kupka, 2018). As clinicians are also end users of the research, the same argument can be made to include them in the research process. Involving clinicians would be advantageous for numerous reasons. They could complement the patients’ experiential knowledge with their clinical expertise by adding relevant research topics and by indicating which research results are (un)likely to be used in clinical practice (Newnham & Page, 2010). Therefore, we argue that one step into bridging the research–practice gap is to unravel relevant research needs according to clinicians and the overlap with patients’ research needs. Moreover, clinicians, and in particular researcher-clinicians, could play an intermediary role between research and practice and potentially narrow the gap between the two (Kluijtmans, de Haan, Akkerman, & van Tartwijk, 2017). They are close to patients and hence in a good position to understand patients’ needs and preferences. In their role as clinicians, they use the results of research in clinical practice by applying guidelines, while being actively involved in research processes. Many clinicians are involved in research projects, whether through collecting data about their patients or through setting up and conducting entire research projects. Thus, to contribute to bridging the research–practice gap, our study seeks to explore research needs from clinicians’ perspective in the field of BD and their reflections on the research needs of patients.
Method
A qualitative research approach was used to gain insights into clinicians’ perspective (Green & Thorogood, 2009) on research needs and to elaborate on topics (Gray, 2014) to deepen the understanding of their motivations and views. Our study consists of two phases.
Phase 1: Research Needs From Clinicians’ Perspectives
This phase aimed to gain insights into the research needs according to clinicians. For this purpose, we recruited clinicians from three teams specialized in treatment of BD at two Dutch outpatient clinics. In each team, separate focus group discussions (FGDs) were conducted with psychiatrists, psychologists, and nurses to derive a broad range of research needs. In two teams, there was only one psychologist. We therefore conducted interviews instead of FGDs. In total, 18 clinicians participated: seven psychiatrists, seven nurses, and four psychologists. The FGDs and interviews were based on a preliminary guide, comprising three parts: trends in health care, hopes for the future, and associated research needs. The sessions took 60 to 90 min. The FGDs and interviews were audiotaped and transcribed verbatim. A framework for thematic analysis (“identifying, analyzing and reporting patterns and themes within data”) by Braun and Clarke (2006) was used for the analysis, supported by the qualitative software program Atlas.ti. Open coding was used to derive all research needs formulated by clinicians. Subsequently, we sought patterns to cluster these codes into themes, after which these themes were named. In addition, the research needs of clinicians were compared with the research agenda according to patients with BD.
Phase 2: Reflections of Researcher-Clinicians on Patients’ Research Needs
As previously explained, including end users in setting a research agenda has been shown to contribute to narrowing the gap between research and practice. In addition, narrowing this gap could benefit from the potential intermediary role researcher-clinicians could play, as they use research in their clinical practice, are actively involved in research, and are in a position to understand patients’ needs and preferences. We therefore conducted a pilot study to gain insights into the views of researcher-clinicians on patients’ research needs. In this study, a researcher-clinician is defined as a psychiatrist, psychologist, or nurse, who in addition to their clinical work spends time on research in the field of BD. As a discussion tool, 23 research needs according to patients with BD were used. These research needs were formulated by patients with BD in a previous study by the authors, which aimed to set a research agenda from the perspective of patients with BD (Maassen et al., 2018). First, two pilot interviews were conducted with two researcher-psychiatrists to fine-tune the interview guide. Before the start of the interview, participants were asked to reflect on each of the 23 topics formulated by patients, considering if and in which phase of research they see a role for their discipline to contribute to the research topic. Four phases of research were distinguished: (a) formulating a problem statement, (b) conducting the research, (c) interpretation of the results, and (d) implementation of the results in clinical practice. In total, six interviews were conducted, two with psychiatrists, two with psychologists, and two with nurses. Participants were included in this phase of the study if they had experience with treating patients with BD and if they were conducting research in this field. The interviews took approximately 45 min. The interviews were audiotaped and transcribed verbatim. The first step in the analysis was to familiarize ourselves with the data. Second, open coding was used to code all segments that described factors that play a role in the view of researcher-clinicians on the research needs of patients. Third, all codes were listed and comparable codes were merged into the same code. Subsequently, we looked for patterns throughout all codes, using the Atlas.ti qualitative software program.
Ethical Considerations
According to the Medical Ethical Committee of the VU University Medical Center, the Medical Research Involving Human Subjects Act does not apply to the first part of this study. Given the noninvasive character of the second part of the study, formal approval from a medical ethical committee was not required, according to Dutch law. All participants gave verbal consent before the start of the FGD or interview for audiotaping, transcribing, and analyzing the FGDs and interviews. Anonymity of all participants was ensured. Participants were informed that they could withdraw from the study at any time.
Results
Research Needs From Clinicians’ Perspectives
The research needs formulated by clinicians could be clustered into six themes: causes of BD, diagnosis, pharmacological treatment, nonpharmacological treatment, recovery, and care system. In the following section, these research themes are further explained.
Causes of BD: including the psychological perspectives
Clinicians formulated research needs on the etiology and the triggers for a mood episode. They called for more research on genetic influences and neurobiological processes, but also indicated the relevance of a psychological explanation for the manifestation of BD. This would include research on the influence of personality traits on the onset of BD, the psychological explanation for the symptoms, and the question of whether certain personality traits could be more frequently recognized in patients with BD. This research need is explained by a psychologist: But also if people with BD have different premorbid characteristics . . . That they are different than people who are not diagnosed with BD.
Research on these fundamental questions would provide health professionals with a better understanding of (the causes of) the disorder.
Diagnosis: detection and distinction
According to clinicians, diagnosing BD is challenging. This is expressed by one psychiatrist: There is an average ten-year gap, between the early signs and the moment the patient is diagnosed with BD. If we would find more [information] on that, we would win the Nobel prize! So early detection, that is what it is about.
Clinicians set out a diverse set of research needs involving the diagnostic process, aiming to increase the early detection of BD and enable the distinction between BD and other psychiatric disorders. According to clinicians, this requires research on the early warning signs of BD, greater knowledge among general practitioners (GPs) about BD, the validity of diagnostic tools, and the distinction between BD and personality disorders. In addition, there is a need for more research on the role of psychologists in the diagnostic process.
Pharmacological treatment: increasing efficacy
Clinicians stressed challenges in the process of finding effective and acceptable pharmacological treatment and being able to predict which medication will be most effective. The following quote from a psychiatrist addressed this challenge: Sometimes, people are stabilized by the medication, but they experience side-effects. And sometimes persistent side-effects. With lithium, kidney failure. Then you have found a treatment that is effective, but at the same time harmful.
These challenges featured a focus on research on increasing the efficacy of medication, while also developing medication with fewer side effects and improving the ability to predict which pharmacotherapy will be most effective for an individual patient, for example, by research on biomarkers. In line with these research needs, clinicians recognized the relevance of improving the treatment of BD, as this is more difficult to treat than a manic episode.
Nonpharmacological treatment: broadening the treatment options
A variety of research needs in the theme nonpharmacological treatment were highlighted and were aimed at broadening the options for treatment. Clinicians formulated needs for research on the efficacy of nonpharmacological treatments and the development of eHealth. The former includes research on the efficacy of nonpharmacological biological treatment options, for example, light therapy, but also entails research on psychological treatment. The need for more research on the role of psychological treatment in treating BD has been highlighted, to gain insight into effective psychological treatments and when and in what circumstances these are appropriate. Research on the efficacy of treatments could also include studying the effectiveness of treatments that are currently used in other disorders for treatment of BD. Within broadening the treatment options, the improvement of nonpharmacological treatment for bipolar depression was particularly stressed. In addition, clinicians would appreciate research on which elements of a treatment might influence effectiveness. As one psychologist explained, Look, we now start a cognitive behavioral therapy group, but also from this therapy it is not exactly clear what the effectiveness is and for whom it would be effective, because that is depending on the mood.
Recovery: reducing the impairments
Clinicians called for more research to contribute to reducing impairments in a variety of life domains caused by BD. They formulated the need for research on the nature of functional impairments due to BD, such as cognitive impairments or overstimulation, and on the influence of these impairments on occupational functioning. In addition, research needs on increasing knowledge in society and decreasing stigma to reduce social impairments were formulated. One nurse explained why this is important, Increasing the understanding by society. We often notice, that when patients tell others they have a manic-depressive disorder, automatically they are branded as crazy. People think these patients always suffer from psychosis or have multiple personality disorder [. . . ]. And the term bipolar disorder is often unknown. If you say manic depressive disorder, they know, but then a negative result comes in.
Another research need to contribute to reducing impairments was to gain knowledge on effective self-management strategies. Overall, clinicians advocated research on factors influencing the patients’ quality of life.
Care system: toward a dynamic system
Clinicians expressed research needs that would contribute to establishing a dynamic care system. These needs include research on improving the continuity of care, the question on how to use everyone’s expertise in clinical practice to improve efficiency, and collaboration systems among a variety of clinicians. One psychiatrist explained, Look, as a bipolar care team, you cannot offer everything, but since it is a disorder that often deals with comorbid disorders . . . it is about improved collaboration within the mental health institution but also child welfare and family therapists [. . . ], but also in the field of physical health, including neurologists, doctors of internal medicine [. . . ]. To find an efficient way of collaborating.
In addition, clinicians expressed interests in research on how science and practice could be better integrated, to be able to use scientific results and conduct research that is relevant for clinical practice. Furthermore, they would appreciate research on the quality of care from a patient’s perspective.
Reflecting on the research-practice gap, it is important to focus on the overlap and differences between the research needs formulated by patients and clinicians. There is a considerable overlap between the clinicians’ research needs, as identified above, and the research agenda formulated by patients with BD (see Table 1; Maassen et al., 2018). Both end-user groups call for research aiming to provide a clearer understanding of the underlying cause of the disorder, with a focus on the etiology and triggers of BD. Both patients and clinicians formulate the need to study the effectiveness of pharmacological treatment and the development of effective new medication, as well as for the need for research on the effectiveness of nonpharmacological therapies, early warning signs, (the validity of) diagnostic tools, and the improvement of GPs’ knowledge of BD. Moreover, both end-user groups formulated the need for research on enhancing social acceptance and knowledge, effective self-management strategies, and the improvement of the care system to provide continuity, flexible care, and an adequate collaboration system among clinicians. Overall, clinicians’ and patients’ research needs address the same research themes, but their specification varies slightly, with patients and clinicians emphasizing both overlapping and distinct topics within the themes. For instance, clinicians did not mention the needs formulated by patients related to recovery, for example, positive aspects of BD, the impact of BD on patients and caregivers, and strategies for social reintegration. Therefore, it would be interesting to understand the view of researcher-clinicians on research topics mentioned by patients, if they see potential in these topics and if they consider them eligible for research.
Research Agenda for Bipolar Disorder According to Patients, in Order of Prioritization (Maassen et al., 2018).

Note. BD = bipolar disorder; GP = general practitioner.
Reflections of Researcher-Clinicians on Patients’ Research Needs
From the interviews, it became clear that researcher-clinicians saw potential in, and understood, all the research topics formulated by patients, including those not formulated by clinicians. This finding was strengthened by the fact that the researcher-clinicians not only affirmed they could contribute in (phases of) research on these topics but also made concrete suggestions for research approaches.
These suggestions provided a better insights into the role of interpretative frames of researcher-clinicians in translating patients’ research needs into research they could conduct and the conditions in which they would be able to conduct the research.
Interpretative frames
From the findings, it became clear that researcher-clinicians used an interpretative frame to interpret the research needs of patients and translate these into research. This interpretative frame is formed by their role in clinical practice, their disciplinary background, and the multidisciplinary nature of clinical practice.
The first aspect that plays a role in the interpretation and translation is the reasoning from a clinical viewpoint by researcher-clinicians. The research topics were approached from a clinical perspective rather than from a solely scientific perspective. These approaches reflected the clinical actions of the researcher-clinicians and the problems they experienced in clinical practice. One psychologist explained how a research question can be derived from clinical practice, For me it [reason why I would conduct research] is way more clinical when I am treating patients and I think: for this I would want a solution, because I run into a problem in the treatment and it would be nice if we would have something to offer or that we can do something about it.
A nurse illustrated why a research topic would be suitable for their research domain, based on their role in clinical practice, Well, I think triggers for a new episode. The triggers, that are just the things you try to capture in for example an alert plan, so I think research in that area would really fit nurses.
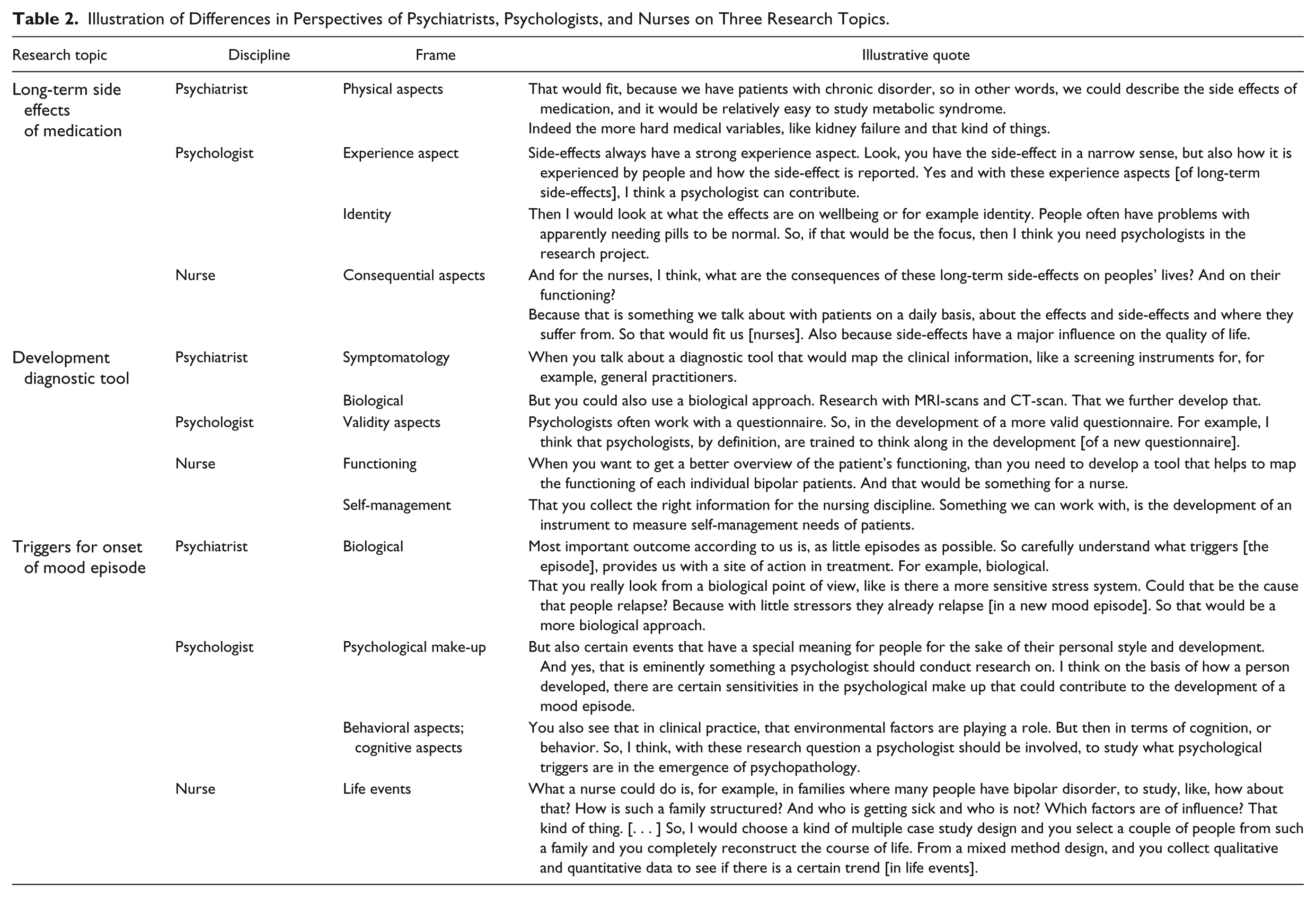
A second aspect is the specific disciplinary background of the researcher-clinicians. Nurses would focus primarily on the consequences for the patient, the influence on functioning, and the impact. Psychiatrists would approach the research topics from a medical frame, focusing on physical aspects, biological aspects, medication, and symptomatology and the psychologists from a psychological frame, which entails a focus on psychological mechanisms, behavior, cognition, and experiences. Table 2 illustrates the differences in perspectives between disciplines on the basis of three research topics that clearly address these differences.
Illustration of Differences in Perspectives of Psychiatrists, Psychologists, and Nurses on Three Research Topics.
The third aspect is the interdisciplinary nature of clinical practice. Researcher-clinicians recognized their role as member of a multidisciplinary team, which was considered relevant both in addressing patients’ needs in clinical practice and in research. They emphasized the importance of an interdisciplinary approach to benefit from all the available knowledge and expertise and to do justice to the complexity of the research topics. They were able to recognize and appreciate the research needs of patients that were not directly related to their own discipline and should primarily be studied by another discipline. However, even when participants attributed the research need of patients to another discipline, they recognized a role for themselves in one of the research phases, for example, in formulating the problem statement or implementing the results.
Moreover, they mentioned that some research could be conducted within a team of researcher-clinicians, but other research requires collaboration with experts from other fields (e.g., public administrators, pharmacologists). In the latter, researcher-clinicians could function as a source of knowledge, while other experts take the lead in the research. According to the participants, an interdisciplinary approach would prevent a narrow approach to the research topics: I think, by definition, everything should be interdisciplinary. [. . .] Yes, because I think otherwise, by definition, you conduct bad research, because you already steer it [the research] in a certain direction.
Research conditions
As mentioned earlier, researcher-clinicians expressed an interest in the research needs formulated by patients and even formulated practical conditions under which they would conduct the research with the resources at their disposal. Based on the findings, three important aspects related to resources can be distinguished.
The first aspect mentioned by participants is the research setting, for example, academic setting or mental health clinics. This influences the available techniques (e.g., laboratories, magnetic resonance imaging [MRI] scans) that are necessary to, and expertise (e.g., neuroscientists, pharmacologists) that could be supportive in, conducting research and therefore shapes the research approach. One psychiatrist illustrated the relevance of the research setting, Biological [triggers] are of course also very important, but then you need large institutions. That is not very practical from a general institution. [. . . ] We can join, but academic centers will be leading.
The second aspect mentioned is patient population. For some research topics, a certain patient population is required, which does not exist in every setting, for example, a certain age group or population that could be followed up over time. This could mean that the research topic is either completely incompatible or would require a different approach, focused on the available patient population. For example, early warning signs could be studied in a group of young children who are not being treated at an adult outpatient clinic. To study early warning signs in a distinct setting would require a different approach.
The third aspect mentioned is population size. Some research topics, for example, the genetic influences on the disorder, require a population size that transcends the borders of the institutions and even countries, which makes this type of research incompatible with the research environment of researcher-clinicians: That [genetic research] really must be done from the NIMH [The National Institute of Mental Health] and otherwise it is less than a drop in the ocean.
To conclude, based on this pilot study, researcher-clinicians can play an intermediary role between research and practice. They are able to understand the research needs of patients based on their clinical experience and at the same time offer concrete suggestions on how to conduct the research based on these needs, including the conditions in which this could be done.
Discussion
The importance of involving end users’ perspectives in formulating research agendas to improve the clinical relevance and increase acceptance of the research, and thus narrow the research-practice gap, is increasingly acknowledged (e.g., Elberse et al., 2012; Newnham & Page, 2010). Therefore, this study aimed to explore the research needs from clinicians’ perspectives and to complement it with a comparison with previously studied patients’ needs as well as to unravel the potential intermediary role of researcher-clinicians. Research needs as perceived by patients largely overlap with clinicians’ research needs. Clinicians view patients’ research needs as relevant and researchable and suggest concrete ways of doing the research. In this way they can act as intermediaries.
In the first phase of this study, six categories of research needs were derived: causes, diagnosis, pharmacological treatment, nonpharmacological treatment, recovery, and care system. Even though clinicians’ research needs regarding BD had not yet been systematically studied, several studies have included clinicians’ perspectives on research priorities for mental health in general (Forsman et al., 2015; Griffiths, Jorm, Christensen, Medway, & Dear, 2002; Michalak et al., 2016; Owens, Ley, & Aitken, 2008), and in mental health, justice and safety issues (Crocker et al., 2015). The findings of these initiatives partly overlap with our findings, such as research on pharmacological treatments (Forsman et al., 2015; Griffiths et al., 2002), (genetic) causes (Forsman et al., 2015; Griffiths et al., 2002), cognitive processes (Griffiths et al., 2002), and improving society’s mental health literacy (Crocker et al., 2015; Fiorillo et al., 2013; Griffiths et al., 2002). In addition, clinicians’ research needs on helpful components of psychological interventions (Fiorillo et al., 2013; Forsman et al., 2015; Michalak et al., 2016; Owens et al., 2008), the quality of services (Fiorillo et al., 2013), early detection, and the social impact and stigma (Fiorillo et al., 2013; Michalak et al., 2016) were also found in other initiatives on mental health in general. This overlap suggests that these research topics are not only relevant for BD, but for other psychiatric disorders as well.
Some scholars argue that a patient-informed research agenda contains research topics that have been researched and therefore reflects an implementation gap instead of a research gap (Banfield, Barney, Griffiths, & Christensen, 2014; Owens et al., 2008). Subsequently, it could be argued that a clinician-informed research agenda reflects an implementation gap as well. However, we argue that in addition to this possible implementation gap, the fact that clinicians formulate these research needs suggests that current research does not completely address their needs, but instead focusses on a different angle. The latter is supported by Phase 2 of this study, where it became clear that different disciplines use their own frame to interpret the research needs of patients and to formulate a research approach. This illustrates that there are a variety of research approaches that could be used for one specific research topic. To this end, we argue that some topics on the research agenda might already be researched, but the used approach may not match the specific need clinicians have.
Interestingly, the clinicians’ research needs can be positioned between the research needs according to patients and the current European research agenda formulated by the European Network of Bipolar Research Expert Center (ENBREC; Henry et al., 2013; Maassen et al., 2018). Patients’ research topics relating to recovery and recovery-oriented care were underrepresented in this European agenda. Clinicians and researcher-clinicians not only formulated topics relating to recovery and recovery-oriented care but were also able to translate these topics into research questions. By recognizing the relevance of these topics and formulating research approaches to address them, the underrepresentation of this theme could be reduced with the support of researcher-clinicians. Hence, clinicians (and researcher-clinicians) can play a role in developing meaningful research based on their experiences in practice (and in research).
In the past decades, there have been many efforts to bridge the gap between research and practice under labels such as transdisciplinary research (Darbellay, 2015; Enengel et al., 2012; Klein, 2015), implementation sciences (Damschroder et al., 2009; Proctor et al., 2009), and translational medicine (Drolet & Lorenzi, 2011; Woolf, 2008). A core feature of these approaches is that they emphasize the role of actors being part of several contexts. These actors, labeled, for example, as brokers or boundary spanners, and familiar with settings on the ground and research or policy contexts, are regarded as promising in narrowing the research–practice gap. According to recent literature, researcher-clinicians can play this intermediary role for several reasons. First, they have the ability to translate research findings into clinical practice (Gunasekaran, Krishnadevarajan, & Barry Lawrence, 2017; Kluijtmans et al., 2017; Roberts, Fischhoff, Sakowski, & Feldman, 2012; van Oostveen, Goedhart, Francke, & Vermeulen, 2017). In this role, one could argue that researcher-clinicians could also play a role in educating clinicians about current research, to decrease an implementation gap. Second, they are directly confronted with patients’ reactions and can thus lead information from practice into research by creating new hypotheses (Roberts et al., 2012). This resonates with our study, where we found that clinicians understand patients’ needs and can translate them into research questions. They showed that patients’ clinically relevant questions could be translated into a research question that fit their setting. In this study, it emerged that the interpretative frame and the research conditions of the researcher-clinicians play an important role in this translation process. For example, respondents indicated that research topics that could be approached by studying a patient population would fit their perspective, whereas research topics that could be approached with studies that required a laboratory would not. This finding is confirmed by Cleary, Hunt, Walter, and Jackson (2010), who stated that academic researchers often have scientific projects “ready to go,” but need clinicians to investigate the effectiveness of treatments. Third, they have the ability to both conduct research and disseminate their results to other researchers and clinicians, thereby bridging a gap in perspective between researchers and clinicians (Smith & Wilkins, 2018). Fourth, researcher-clinicians can play an intermediary role between research and practice because they have a broader perspective on care than either researchers or clinicians. Kluijtmans et al. (2017) found that clinicians who became skilled as scientists “evoked reflection with regard to their clinical profession as they developed broader perspectives on patient care and the organization of care” (p. 651). Our study also found that researcher-clinicians had a broad perspective on patient care. They were not only able to translate the research needs of patients into research questions that would fit their own interpretative frame but could also recognize research questions that would fit other disciplines.
Limitations and Recommendations for Future Research
Our study has some limitations. First, this study explored research needs from the perspectives of clinicians by means of FGDs. A limitation of this method is that the research needs could not easily be prioritized. Future research could focus on the prioritization by means of a quantitative study design. Second, to generalize the findings of our study, research needs from the perspective of clinicians should be verified by a larger group. Third, we studied the views on the research needs of patients in a small group of researcher-clinicians. To further understanding of the potential intermediary role of researcher-clinicians, this study needs to be extended.
Conclusion
In conclusion, our study contributes to the field of research agenda setting by studying the research needs of clinicians in the field of BD. The research needs formulated by clinicians largely overlapped with those of patients with BD, but in addition both clinicians and patients raised specific topics. Research topics formulated by patients could be translated by researcher-clinicians into study approaches that fit existing research domains. Therefore, researcher-clinicians could play an intermediary role between clinical practice and research to narrow the research–practice gap.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.