
Abstract
Research is vague regarding the influence of media exposure on HIV testing among youth in sub-Saharan Africa (SSA). Using three rounds of Demographic and Health Surveys (DHS) from three selected countries in SSA (Kenya, Nigeria, and Zambia), this article investigates the relationship between mass media exposure and HIV testing among youth in SSA. Logistic regression was used to examine these associations. SSA has witnessed some growth in the percentage of youth who are tested and an increasing trend was evident. There was a significant relationship between exposure to mass media and HIV testing during the mid-2000 among youth in Kenya and Nigeria, but not in Zambia. The findings highlight an increase in the number of youth testing for HIV who were exposed to mass media messages. We suggest that continuous and proactive media movements may lead to diffusion of ideas among youth that may ultimately promote HIV testing.
Introduction
The Millennium Development Goal 6 (MDG 6), which targeted the reduction of the spread of HIV/AIDS by 2015 (World Health Organization, 2014), was not achieved but new infections have been gradually declining (Ki-Moon, 2013). Despite this, there is still a window of opportunity to meet the Sustainable Development Goal 3 (SDG 3), which is focussed on guaranteeing health and wellness for all ages (United Nations, 2018). HIV testing is a crucial prevention strategy in the reduction of HIV/AIDS. Despite the gains recorded in the reducing new cases of HIV/AIDS worldwide, some countries in sub-Saharan Africa (SSA) still have the highest incidence. For instance, about 1,600 new infections occur daily in South Africa, while one out of four adults have HIV in Namibia, Botswana, Zimbabwe, and Swaziland (Engel, 2017). This differs from the rates of infection in the North and West of Africa, where prevalence ranges between 0.5% and 5% among adults (Poku, 2017).
While studies have asserted that no singular approach will be enough to curb the HIV endemic (Kurth, Celum, Baeten, Vermund, & Wasserheit, 2011), HIV testing has shown promising results in reducing prevalence in various settings (Kharsany, Karim, & Abdool Karim, 2010). This is because of the opportunity testing provides for people to know their HIV status, complemented by counseling and education support. HIV testing is also a prevention intervention and related to behavioral change. A drawback of low HIV testing among populations who are assumed to be “not at risk” is that it may result in missed chances to identify and link infected persons to care (Ansa, White, Chung, & Smith, 2016; Kurth, Lally, Choko, Inwani, & Fortenberry, 2015).
Protective factors have been documented to increase the likelihood of positive outcomes in the lives of youth and reduce the odds of negative consequences because of exposure to risk (Garmezy, 1991; Somefun & Odimegwu, 2018). However, this remains a growing area of research. Although young people have been previously associated with risky behaviors, recent studies are showing that some young people engage in positive behaviors despite the obstacles they face. Some of these behaviors include abstaining, consistent use of condoms, single sexual partnerships, and HIV testing (Kabiru & Ezeh, 2007; Odimegwu, Somefun, & Chisumpa, 2018). For example, it has been recently found that HIV testing among youth ranged from 77.5% in Uganda, 45.3% in Mozambique, 31.4% in Congo, to 24.7% in Nigeria (Asaolu et al., 2016).
Remarkable progress with HIV testing has been made, but differentials by age have been established wherein testing increases between the ages 20 to 34 years (Center, Gunn, Asaolu, Gibson, & Ehiri, 2016; Staveteig, Wang, Head, Bradley, & Nybro, 2013). For instance, young males aged 20 to 29 years were 2 times more likely to test than adolescent males aged 15 to 19 years in Zambia (Hensen et al., 2015). This has also been established among females in Kenya (Achia & Obayo, 2013).
Young people make up a significant proportion of people living with HIV globally (Kharsany & Karim, 2016; United Nations Children’s Fund [UNICEF], 2018), and if current trends in low testing among youth continue, there would be a higher number of HIV-positive young people, which could be detrimental for human capital and development. While low testing has been reported among adolescents (Asaolu et al., 2016; Wilson et al., 2017), some other studies have reported an increased interest among young people in being tested for HIV in SSA (Sam-Agudu, Folayan, & Ezeanolue, 2016).
For instance, demographic factors such as region of residence and sex have been linked with HIV testing, with some studies showing a higher likelihood of testing among females compared with males; this has been ascribed to the earlier age of sexual activity among females compared with their male counterparts (Sanga, Kapanda, Msuya, & Mwangi, 2015). The relationship between socioeconomic status and HIV testing has also been established, where educated youth have a higher likelihood of testing (Ziraba et al., 2011). HIV risk behavior and perceived HIV risk are some other variables that have been linked with HIV testing (Kabiru, Beguy, Crichton, & Zulu, 2011).
As part of this growing body of literature, the effect of mass media on HIV testing has also been studied (Do, Figueroa, & Kincaid, 2016; Gyasi & Abass, 2018; Hutchinson, Mahlalela, & Yukich, 2007; Peltzer et al., 2012). This is partly because of the documented influence mass media has on youth behaviors, especially sexual behaviors, which has increasingly become of interest to policy makers and program planners (Collins, Martino, & Shaw, 2010). In addition, mass media has recently emerged as a significant tool used to influence various health behaviors in mass populations, where HIV testing is no exception. For example, increased HIV knowledge, information about testing areas, and understanding the benefits of HIV testing have been linked with mass media exposure (Onsomu, Moore, Abuya, Valentine, & Duren-Winfield, 2013).
One reason for the significance of mass media exposure lies in its capacity to reach out to the public by equipping them with information that influences their understanding of various concerns. For instance, mass media campaigns have been associated with behavioral adjustments such as condom use (Jung, Arya, & Viswanath, 2013) and reduction of HIV-related stigma (Bekalu, Eggermont, Ramanadhan, & Viswanath, 2014) in SSA. They have also been associated with increased odds of being faithful in Zambia (Kraft et al., 2012). Studies have established that young people are excessive users of media including Television (TV; Chandra et al., 2008; Strasburger, Jordan, & Donnerstein, 2010), print media and, lately, the Internet (Andreassen, Pallesen, & Griffiths, 2017).
The use of role models to change traditional norms and influence policy makers regarding important health issues has been seen in televised campaigns (Scheier & Grenard, 2010; Wakefield, Loken, & Hornik, 2010). A notable televised campaign is the “Shuga” program, sponsored by MTN and Presidential Emergency Plan For Aids Relief (PEPFAR) in Africa, which is a multimedia campaign aimed at spreading the message about responsible sexual behavior (Booker, Miller, & Ngure, 2016; Borzekowski, 2010). Other forms of media campaign such as condom promotion though social marketing have also been used in Uganda and Tanzania (Coates, Richter, & Caceres, 2008). In South Africa, Khomani, meaning “caring together,” Love Life, and Soul City are other HIV/AIDS televised programs that have been used to influence positive behavioral change (Peltzer et al., 2012).
Despite the positive relationship between mass media and protective behaviors shown by a number of studies, some studies have documented that exposure to sexually explicit material in media leads to early sexual activity among youth by influencing their perception of sexual activities (Bleakley, Hennessy, Fishbein, & Jordan, 2011; Brown et al., 2006).
We can infer from this background that the available literature shows the relevance of mass media exposure on youth sexual behavior, albeit with mixed results. What is missing in the literature is evidence of the changes that have occurred in youth sexual behavior, such as HIV testing, because of exposure to media in SSA. The available literature also does not examine whether gender differentials exist in these changes. This is an important question, because globalization has also influenced the different types of media available to youth. This can be linked with easy access to media with increased sensual messages and low representation of protective sexual attitudes.
This article is timely and contributes to the literature because the available media existing today are different from those that existed in the early years of the HIV pandemic. It is therefore important to document the changes that have occurred in HIV testing among youth because of media exposure. The main question this article seeks to address is as follows: What are the changes that have occurred in HIV-testing behavior of youth because of exposure to mass media in Kenya, Nigeria, and Zambia between the early 2000s, mid 2000s, and a decade after?
Theoretical Framework
The study adopted cultivation theory by Gerbner, Gross, Morgan, and Signorielli (1980) and the protective factor model of the resilience theory (Fergus & Zimmerman, 2005). Cultivation theory proposes that massive exposure to mass media messages can foster opinions about reality, media as a medium of conservative socialization (it reinforces norms and practices). The basic tenet underlying this theory is that higher exposure to media messages is more likely to result in a higher likelihood of message being viewed as reality. This theory identifies how the communication of messages through various media outlets can reinforce youth perceptions of reality and change their behaviors. This relationship may not be as straightforward as we would imagine. This is because of the different types of media messages currently available for young people. For instance, if watching health-promoting messages encourage positive sexual behaviors, would watching other types of sexual messages encourage risky behaviors?
Studies on mass media exposure and various behavioral outcomes have gone beyond Gerbner et al. (1980) seminal work. For instance, exploring the linkages between media exposure to information on HIV/AIDS prevention and condom-use related attitudes among females in Beijing, Xiao, Li, Lin, and Tam (2015) reported a significant association between online information and condom use self-efficacy. Mass media promotions have also been used to reduce disparities in HIV/AIDS based on their influence and efficacy. This has been established in a meta-analysis targeted at assessing the usefulness of media campaigns in improving condom use and HIV-related knowledge (Lacroix, Snyder, Huedo-Medina, & Johnson, 2014).
In SSA, Sano et al. (2016) examined the association between exposure to mass media and HIV testing among married men and women in Ghana using national data. Their results showed that HIV testing was associated with higher levels of exposure to radio for women and higher levels of exposure to print media and television for men. This gender differential in the type of media that influences HIV testing has also been documented in Kenya, where women who read newspapers had higher odds of being tested compared with men, while men who watched television almost every day had higher odds of being tested (Onsomu et al., 2013).
The protective factor model proposes that assets or resources buffer the negative effects of adversity on youths’ development (Zimmerman, 2013). This implies that protective factors work together to shield an individual from the negative effects of risk exposure. We hypothesize that media exposure could be a protective factor in the lives of youth regarding their HIV-testing behavior and could also act as a risk factor depending on the type of media message. We believe that focusing on HIV testing reflects strengths, assets present in the lives of youth, and media exposure emphasizes the different ways in which youth react to their external environment.
Data and Method
The present study uses Demographic and Health Surveys (DHS) data of three sub-Saharan African countries, purposefully selected on the basis of geographical difference, with Kenya (2003, 2008, and 2014) representing East Africa, Nigeria (2003, 2008, and 2013) representing West Africa, and Zambia (2001, 2007, and 2014) representing Southern Africa. The use of three survey years was to document changes that have occurred in HIV testing and also examine the changes in HIV testing associated with media exposure. This selection was also based on the differentials in their levels of HIV prevalence. The study includes youth who are male and female aged 15 to 24 years. We also made sure they had three rounds of DHS from the year 2000. The total sample size of the three countries has been presented for the three survey years in Supplemental Appendix 1.
Ethical Considerations
Permission to use data was obtained from the DHS program (https://dhsprogram.com/data/available-datasets.cfm). A request was made on the website and access was granted for the study countries. There were no ethical considerations on the part of the researchers as the data are completely anonymized and the DHS program has handled ethical issues before and during the survey.
Variables Measurement
The dependent variable HIV testing was deduced from the question “ever been tested for HIV.” Youth were coded “1” if they reported ever being tested for HIV and “0” otherwise.
Independent Variables
The key independent variable is media exposure. This was measured from three variables on the frequency of exposure to media: frequencies of reading print media, listening to the radio, and watching television (0 = not at all, 1 = less than once a week, 2 = at least once a week). These variables were merged together using principal component analysis to form a scale ranging from 0 to 9 and categorized as 1 “low,” 2 “medium,” and 3 “high” which has been used in other studies (Achia & Obayo, 2013).
Based on the literature, we have identified some other variables that have been linked with HIV testing. They include age, place of residence, wealth status, educational attainment, work status, condom use at last sex, multiple sexual partnership, and family structure measured by sex of household head.
Older adolescents have been established to engage more in protective behaviors compared with younger adolescents, thus age has been dichotomized as “15-17” and “18-24.” We included components of sexual behaviors in the model because the association between sexual behaviors and HIV testing has been inconclusive.
Statistical Analysis
We performed separate analyses for males and females. Univariate analysis was conducted to show the percentage distribution of youth who had HIV testing in each year. The independent effect of media exposure, each control variable, and HIV testing by survey year was analyzed at the bivariate level. At the multivariate level, the combined effect of media exposure, control variables, and HIV testing was modeled. Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs) and alpha level set at .05. Analysis was conducted using STATA (Version 14.2). Sample weights were used to adjust for disproportionate sampling and nonresponse in the date.
Results
Descriptive Statistics
Figure 1 shows HIV testing uptake among male and female youth increased in Kenya, Zambia, and Nigeria. HIV testing was seen to be highest among males and females in Kenya, with the highest percentage increase. Although about 15% of male youth tested for HIV in the early 2000s, less than a quarter tested a decade after compared with the other countries. Similar results were seen for female youths in Nigeria.

Trends in HIV testing by country.
Being exposed to media showed an increase in HIV testing among female youth in the three countries. For instance, HIV testing increased in Nigeria from about 11% in the early 2000s for females who were exposed to high levels of media to about 33% a decade after. In Zambia, HIV testing increased from 16% to 64% among female youth with high exposure to media. Similar results were seen for males. For instance, HIV testing increased from 13% to 70% for males youth with high exposure to media messages. Other descriptive statistics have been presented in Supplemental Appendices 2 to 7.
Association Between Exposure to Media and HIV Testing
The bivariate results have been presented in the Supplemental Appendix. Supplemental Appendices 8 to 13 show results of the association between media exposure and HIV testing for females for the 3 years studied. In Kenya, media exposure was significantly associated with HIV testing among youth in the early 2000s, OR = 3.60, CI = [2.65, 4.89], mid 2000s (OR = 1.78, CI = [1.51, 2.11]), and a decade after (OR = 1.53, CI = [1.36, 1.72]). These results were similar to results in Nigeria among youth in the early 2000s (OR = 4.06, CI = [2.57, 6.41]), mid 2000s (OR = 4.81, CI = [4.14, 5.58]), and a decade after (OR = 3.11, CI = [2.77, 3.48]). On the contrary, in Zambia media exposure was positively associated with HIV testing among female youth in the early (OR = 2.84, CI = [2.16, 3.74]) and mid 2000s (OR = 1.058, CI = [1.33, 1.888]), but youth who reported high media exposure a decade after were less likely to test for HIV (OR = 0.84, CI = [0.75, 0.94]). For males, media exposure was associated with increased odds of HIV testing in all the countries studied and for all the survey years.
Demographic variables such as age, religion, place of residence, and age at first sex were also associated with HIV testing in the countries studied although significance varied by country and gender.
By socioeconomic status, male and female youth who were working were more likely to have ever tested for HIV in the mid 2000s and a decade after in all the countries studied. Similar results were seen for wealth status.
By sexual behaviors, condom use was associated with HIV testing among female youth for all the three survey years, but in Kenya and Zambia, condom use was positively associated with HIV testing in the early 2000s and negatively associated with HIV testing a decade after. Different results were seen for males, where condom use was significantly associated with HIV testing for the three survey years. Male and female youth who reported having multiple sexual partners were significantly more likely to test for HIV for all the three rounds studied.
Multivariate Results
In the multivariate analysis, which has been presented in Tables 1 to 6, age at first sex and sexual activity were dropped as they were correlated with condom use at last sex. After controlling for other covariates, the influence of media exposure on HIV testing among youth differed by survey year. Among female youth in Kenya, there was a positive relationship between media exposure and HIV testing in the early 2000s (OR = 2.49, CI = [1.65, 3.75]) and mid 2000s (OR = 1.87, CI = [1.31, 2.68]). In Kenya, high media exposure was not significantly associated with lower odds of HIV testing a decade after. Among females in Nigeria, media exposure was not significantly associated with HIV testing in the early 2000s, but there was a positive relationship between media exposure and HIV testing in the mid 2000s (OR = 1.33, CI = [1.06, 1.67]) and a decade after (OR = 1.32, CI = [1.15, 1.52]). In Zambia, there was no significant relationship between media exposure and HIV testing among female youth except in the early 2000s where females exposed to media had higher odds of testing for HIV (OR = 1.71, CI = [1.12, 2.62]).
Adjusted Association Between Media Exposure and HIV Testing Among Female Youth in Kenya.

Note. OR = odds ratio; CI = confidence interval.
Adjusted Association Between Media Exposure and HIV Testing Among Female Youth in Nigeria.

Note. OR = odds ratio; CI = confidence interval.
Adjusted Association Between Media Exposure and HIV Testing Among Female Youth in Zambia.
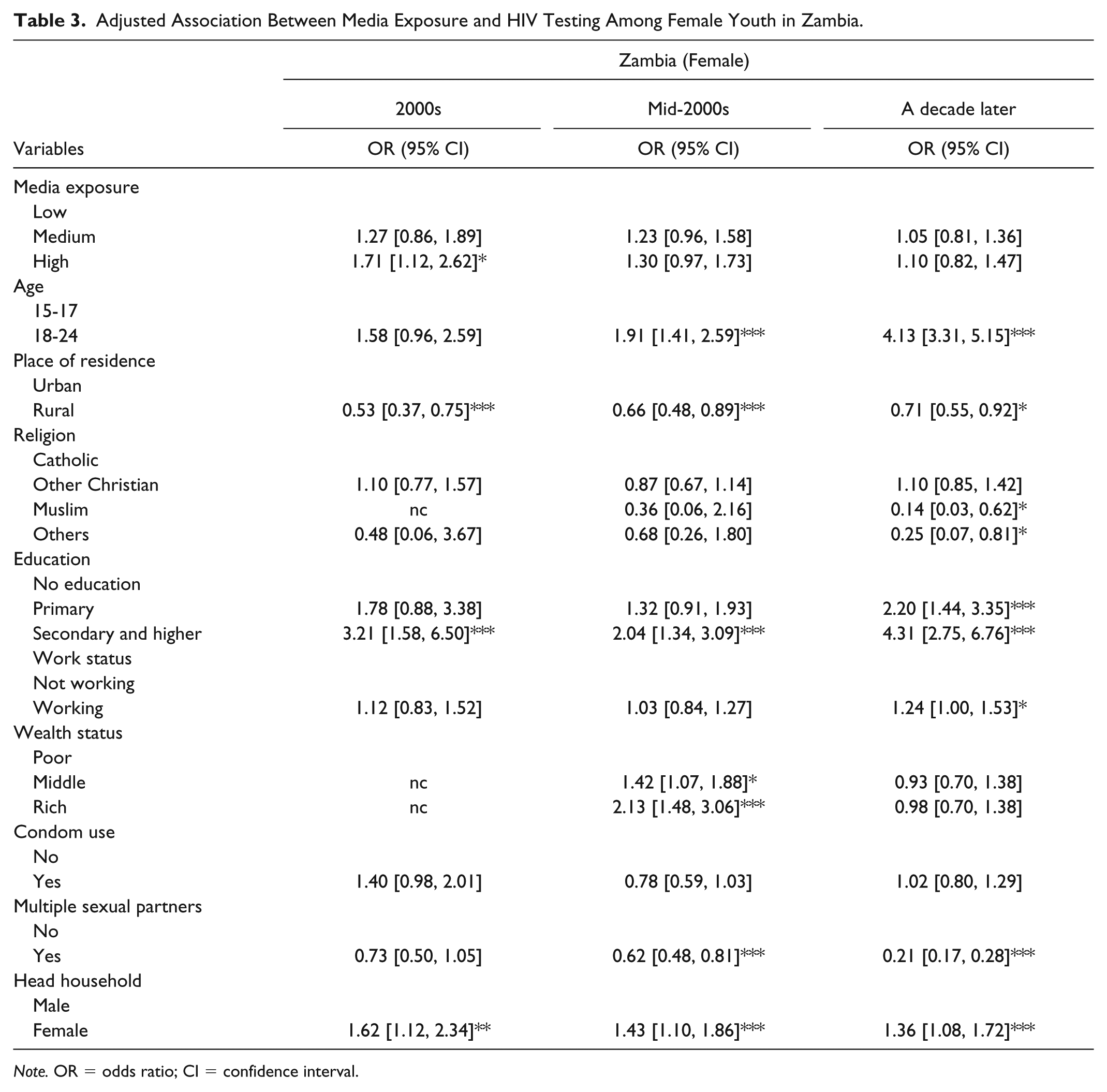
Note. OR = odds ratio; CI = confidence interval.
Adjusted Association Between Media Exposure and HIV Testing Among Male Youth in Kenya.

Note. OR = odds ratio; CI = confidence interval.
Adjusted Association Between Media Exposure and HIV Testing Among Male Youth in Nigeria.

Note. OR = odds ratio; CI = confidence interval.
Adjusted Association Between Media Exposure and HIV Testing Among Male Youth in Zambia.

Note. OR = odds ratio; CI = confidence interval.
p < .1 (Significant at 10%). **p < .05 (Significant at 5%). ***p < .01 (Significant at 1%).
Results for males showed that media exposure was not associated with HIV testing in the early and mid 2000s in Kenya, but youth who were exposed to media a decade after (OR = 2.12, CI = [1.57, 2.87]) were significantly more likely to test for HIV. Similar results were seen in Nigeria, where male youth were significantly more likely to test for HIV a decade after (OR = 1.50, CI = [1.07, 2.11]). There was no significant association between media exposure and HIV testing among male youth in Zambia for the three study years.
By demographic characteristics, female older youth aged 18 to 24 years were more likely to have been tested for HIV in each of Kenya (OR = 3.50, CI = [2.46, 4.97]), Nigeria (OR = 2.63, CI = [2.12, 3.27]), and Zambia (OR = 4.13, CI = [3.31, 5.15]) compared with youth aged 15 to 17. Similar results were seen for older males in Kenya (OR = 1.91, CI = [1.43, 2.56]), Nigeria (OR = 1.95, CI = [1.10, 3.44]), and Zambia (OR = 2.22, CI = [1.79, 2.77]). Rural residence was associated with lower odds of HIV testing among females in Kenya (OR = 0.64, CI = [0.44, 0.93]), Nigeria (OR = 0.71, CI = [0.62, 0.81]), and Zambia (OR = 0.71, CI = [0.55, 0.92]). These results are comparable with the results for males in Kenya (OR = 0.76, CI = [0.59, 0.97]), Nigeria (OR = 0.72, CI = [0.55, 0.95]), and Zambia (OR = 0.77, CI = [0.62, 0.96]). In Kenya (OR = 0.62, CI = [0.38, 0.99]), Nigeria (OR = 0.43, CI = [0.35, 0.54]), and Zambia (OR = 0.14, CI = [0.03, 0.62]), Muslim women had lower odds of HIV testing. This result was only similar for male Muslims in Nigeria (OR = 0.56, CI = [0.38, 0.82]).
The results on socioeconomic status show that secondary and higher education was associated with HIV testing among female youth in Kenya (OR = 11.02, CI = [6.34, 19.16]), Nigeria (OR = 4.35, CI = [3.54, 5.35]), and Zambia (OR = 4.31, CI = [2.75, 6.76]). Male youth who had secondary and higher education in Kenya (OR = 3.58, CI = [1.96, 6.54]), Nigeria (OR = 6.48, CI = [2.72, 15.41]), and Zambia (OR = 3.05, CI = [1.69, 5.48]) were also likely to have ever been tested for HIV. Female youth who were working were also more likely to get tested for HIV in the three countries, but work status was not significantly associated with HIV testing among male youth in Nigeria and Zambia.
By sexual behavior, multiple sexual partnerships, which was associated with higher odds of being tested for HIV in the unadjusted model, became negatively associated with HIV testing in the adjusted model for female youth in Kenya (OR = 0.18, CI = [0.12, 0.27]), Nigeria (OR = 0.29, CI = [0.24, 0.34]), and Zambia (OR = 0.21, CI = [0.17, 0.28]). This relationship was the same for male youth in Kenya (OR = 0.37, CI = [0.26, 0.52]), Nigeria (OR = 0.56, CI = [0.37, 0.85]), and Zambia (OR = 0.26, CI = [0.20, 0.34]).
By familial characteristics, female household headship was associated with increased odds of HIV testing for females in Nigeria (OR = 1.39, CI = [1.19, 1.61]) and Zambia (OR = 1.36, CI = [1.08, 1.72]).
Discussion
This study examined the association between media exposure and HIV testing among youth and sought to examine the changes in HIV testing associated with exposure to media in three selected countries in SSA. The results show that there were changes associated with media exposure and these changes differed by country.
The findings show that there has been an increase in HIV testing over the past decade among the three surveys in the selected countries, although it remained quite low in Nigeria among both male and female youth. Among females in Kenya, HIV testing increased from about 13% in the early 2000s to about 72% a decade after. This increase was similar to the increase witnessed for female youth in Zambia. However, in Nigeria the percentage of female youth being tested was not as high as the other two countries. HIV testing among youth increased from 6% in the early 2000s to 19% a decade after. These results are similar to the results for males in Nigeria. This is quite low compared with other countries in the region. This low percentage of testing among youth in Nigeria has also been found in other studies (Nwachukwu & Odimegwu, 2011; Ogbo et al., 2017) and has been linked to a lack of awareness (Iyaniwura & Oloyede, 2006). It is also possible that testing is low in Nigeria compared with the other countries studied as a result of HIV stigma in Nigeria. A review by Odimegwu, Akinyemi, and Alabi (2017) has recently documented that stigma and discrimination are key barriers to testing in Nigeria. Although a recent study (Odo, Samuel, Nwagu, Nnamani, & Atama, 2018) conducted in Enugu Nigeria among adolescents revealed that sexual and reproductive health public facilities were accessible, it is possible that the staffs were not friendly to youth which may influence HIV testing among this population.
Our results also confirmed that there was an association between mass media exposure and HIV testing for both males and females in the study countries. Among males in Zambia and Kenya, the number of youth who were exposed to a high level of media messages and who tested for HIV increased from about 10% to about 70%. Males testing for HIV/AIDS also increased in Nigeria, although not as much as in the other two countries. These levels of increase were also seen in female youth. This result underlines the possible importance of media exposure for behavioral change among youth in SSA. The results also highlight the importance of context, because of the different results evident in Nigeria. The differences in the association of media exposure and HIV testing could be due to the differences in HIV prevalence in the countries studied. In addition, this could also be to the types of messages included in the media in these countries. Another possible reason for the result could be access to media messages. A study exploring the effect of mass media and the Internet on sexual behavior of adolescents in Southwestern Nigeria found that only one fifth of the students had ready access to radio and television (Asekun-Olarinmoye, Asekun-Olarinmoye, Adebimpe, & Omisore, 2014). In Kenya, entertainment education and distribution of HIV/AIDS printed materials are other strategies that have been used to influence behavior (Onsomu et al., 2013).
The results on the associations between media exposure and HIV testing also differed by country and survey year. For females in Kenya, media exposure was associated with HIV testing in the early and mid 2000s, but no association was seen a decade after. We suggest that this result may be as a result of the decline in the HIV prevalence rate in Kenya (Kimanga, Ogola, & Umuro, 2014) which has been reported to have almost reached the national target (Ng’ang’a et al., 2014). This decline may have influenced mass media strategies that previously promoted HIV testing among youth. The results were different for females in Nigeria, where media exposure was not associated with HIV testing in the early 2000s, but became significantly associated in the late 2000s and a decade after. It is possible that global initiatives such as the U.S. PEPFAR program have helped in encouraging youth to test in the later years. In Zambia, media exposure was only significantly associated with HIV testing in the early 2000s. Results for males also differed: media exposure was not significantly associated with HIV testing in the earlier years for the countries studied. However, in Kenya and Nigeria, media exposure later became positively associated with HIV testing among male youth.
However, other characteristics like education and work status were consistently significantly associated with HIV testing among females in Kenya across the three survey years: educated youth and youth who were employed were likely to get tested. This is consistent with the literature on socioeconomic status and HIV testing. Risky sexual behavior such as having multiple sexual partners also consistently predicted HIV testing in all the countries for the last survey years. This is expected, as youth who engage in such risky behaviors may be aware of the risk and thus get tested compared with counterparts who are monogamous.
Limitations
Our results are limited to statistical associations based on the cross-sectional nature of the data set. HIV testing may be underreported based on the sensitivity and stigma that may be attached in some settings. The dependent variable, HIV testing, is a self-reported measure which could also be subjected to errors. Our study is also limited to three countries and three survey years which may not be so generalizable. The study created a dichotomized, synthesized measure of “media exposure” that combines TV, radio, and print media, so finer-grained information on the effect of different levels of exposure to different media types was lost in the analysis.
Policy Implications
This study provides information on the changing role of media exposure in HIV testing among youth, which is significant for programs and policies in government and media industries. Program planners should continue with the use of different forms of media such as Facebook and Twitter to encourage protective sexual behaviors among youth. Diverse and new types of media that are appealing and accessible to youth such as Internet, billboards should also be considered in promoting these messages. The study also highlighted other predictors of HIV testing that will be useful for policy. For instance, in Nigeria, religion was a significant predictor of HIV testing among youth for the three survey years. Programs that work with religious organizations should also be considered for sustainable results.
Supplemental Material
Online_Appendix – Supplemental material for Media Exposure and HIV Testing Among Youth in Sub-Saharan Africa: Evidence From Demographic and Health Surveys (DHS)
Supplemental material, Online_Appendix for Media Exposure and HIV Testing Among Youth in Sub-Saharan Africa: Evidence From Demographic and Health Surveys (DHS) by Oluwaseyi Dolapo Somefun, Stephen Ojiambo Wandera and Clifford Odimegwu in SAGE Open
Footnotes
Acknowledgements
We acknowledge Matt Hodgkinson of AuthorAid for his editorial input which helped in improving the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Consortium for Advanced Research Training in Africa (CARTA). CARTA is jointly led by the African Population and Health Research Center and the University of the Witwatersrand and funded by the Carnegie Corporation of New York (Grant No: B 8606.R02), Sida (Grant No: 54100113), the DELTAS Africa Initiative (Grant No: 107768/Z/15/Z) and Deutscher Akademischer Austauschdienst (DAAD). The DELTAS Africa Initiative is an independent funding scheme of the African Academy of Sciences (AAS)’s Alliance for Accelerating Excellence in Science in Africa (AESA) and supported by the New Partnership for Africa’s Development Planning and Coordinating Agency (NEPAD Agency) with funding from the Wellcome Trust (UK) and the UK government. The statements made and views expressed are solely the responsibility of the Fellow. We also acknowledge National Research Foundation (NRF), South Africa for supporting Oluwaseyi’s doctoral study.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.