
Abstract
The increasing prevalence of mental illness in the United States presents significant challenges for primary care providers particularly in low-income settings. Integrated Behavioral Health (IBH) programs have resulted in improved general health for low-income participants; however, managing appointment adherence, in which the patient attends appointment as scheduled, is particularly challenging. The purpose of this pilot project was to implement bundled interventions at a low-income primary care clinic in a Mid-Atlantic state to improve patient adherence to behavioral health treatment using a collaborative, community-based approach. Interventions were delivered in a bundle format and included patient education, warm patient handoffs, and follow-up phone calls by behavioral health counselors. In the 4-month postintervention time frame, the average number of patients who did not come to their appointment decreased by 60%, and the average number of patients who canceled decreased by 15%. These differences were significant (χ2 = 9.263, df = 2, p < .01). This pilot project showed that patients who became engaged as active participants in a bundle of interventions were more likely to keep their appointments.
Introduction
Mental health disorders are common, functionally impairing, and costly. In 2015, there were an estimated 43.4 million adults aged 18 years or older in the United States with mental illness. This number represented 17.9% of all U.S. adults (Center for Behavioral Health Statistics and Quality, 2016). Mental illness affects nearly 49% of patients in primary care settings serving low-income individuals (Wray, Dvorak, & Martin, 2013). Individuals benefit from evidence-based, collaborative Integrated Behavioral Health (IBH) care; however, many low-income adults and families do not receive beneficial mental health treatment (Santiago, Kaltman, & Miranda, 2013). Nationally, the unmet need for mental health services increased from 4.3 million in 1997 to 7.2 million in 2010 (Roll, Kennedy, Tran, & Howell, 2013).
Appointment adherence is particularly challenging in the long-term management of both chronic and episodic disorders, as individuals with serious mental illness are more likely to miss appointments and show poor adherence with the prescribed plan of care (DeFife, Conklin, Smith, & Poole, 2010). Using scales to determine the severity of mental disorder and level of social disorganization, Killaspy, Banerjee, King, and Lloyd (2000) found that those who miss psychiatric follow-up outpatient appointments are more unwell, more poorly socially functioning, and have a greater chance of dropout from clinic contact and subsequent hospital admission than those who attend. They concluded that appointment adherence is especially important for those with severe mental illness, as those who drop out after their first contact may experience significant deterioration in their mental state. Primary care patients who have a high propensity to miss appointments will have suboptimal clinical outcomes and higher rates of acute care utilization than those with a lower propensity to miss appointments (Hwang et al., 2015).
This pilot project incorporated community-based participatory research (CBPR) into a program aimed to improve mental health appointment adherence in a low-income clinic. CBPR empowers individuals, communities, and health care providers to become actively involved in solving their own health problems. According to the Agency for Healthcare Research and Quality (2018), CBPR is an approach to health and environmental research meant to increase the value of studies for both researchers and the communities participating in a study. It is particularly attractive for academics and public health professionals struggling to address the persistent problems of health care disparities in populations that the U.S. Department of Health and Human Services has designated as priority populations (including racial and ethnic minorities; low-income, rural, and inner city populations; women; and children). CBPR allows communities to collaborate and pull together resources. By involving people in identifying and defining their own health problems, this strategy is most likely to develop sustainable solutions that work for both individuals and communities (Thompson, Molina, Viswanath, Warnecke, & Prelip, 2016).
Accustomed to collaborating with various health care systems to meet the health needs of underserved clients, low-income clinics (free, low cost, and sliding scale) are well suited for collaborative, integrated programs that focus on providing patient-centered care. Patient-centered care is consistent with the values, needs, and desires of patients and is achieved when clinicians involve patients in health care discussions and decisions (Mead & Bower, 2000). The three main objectives of patient-centered care include effective communication, partnership, and health promotion (Little et al., 2001). Patient-centered, integrated care identifies that understanding patients holistically can be a means of achieving better health outcomes, greater patient satisfaction, and reduced health costs.
Literature shows that clinicians who use a bundle or combination of interventions that utilize available resources appear to have higher rates of success. Attendance improvement interventions such as transportation vouchers, early follow-up phone calls, warm handoffs, orientations, letters, home visits, patient contracts, and prizes were shown to be particularly effective when they employed multiple, combined intervention strategies. Bundles appeared to have a greater impact than single interventions but no research points to one particular bundle or specific combination of interventions that work well together (Lefforge, Donohue, & Strada, 2007).
Despite the apparent value of various interventions to improve adherence to appointments, literature is lacking regarding the application of patient-centered interventions in a low-income clinic. This pilot project was intended to determine whether a bundle of low-cost, patient-centered interventions would be successful in this setting. Results from this pilot can help facilitate the implementation of bundled interventions in a larger organization or inform the design of future research projects.
Problem/Aim and Objectives
In 2015, a community assessment was conducted in this Mid-Atlantic state to identify local needs and health concerns. The survey included results from local health departments, the school system, social services, community health centers, free clinics, local governments, and many others. The report also included findings from community focus groups and interviews on health issues and barriers to achieving good health. Data gathered from the community surveys identified the need for behavioral health services as a community concern. Behavioral health–related hospitalizations were acknowledged as an important indicator of community health status (Community Health Needs Assessment, 2015). In the assessment, 703 per 100,000 patients discharged from the local hospital had a behavioral health diagnosis as compared with 680 per 100,000 statewide. The leading diagnoses for these discharges were affective psychoses (55%), schizophrenic disorders (13%), and depressive disorders (6%; Community Health Needs Assessment, 2015).
Based on data obtained in the community survey and Healthy People 2020 (n.d.) goals, a low-income primary care clinic pooled community resources and brainstormed methods to decrease barriers to treatment for vulnerable, low-income individuals. Students in a doctoral counseling program along with community mental health volunteers and clinic staff developed an IBH program that allowed for the easy flow of communication between primary care and mental health specialists. After initiating the program, patients reported to counselors that they appreciated the programming and convenience of the co-located services.
One-year into programming data showed that the clinic had high rates of missed appointments with more than half of the patients counseled never returning for a second session. To promote the mental health of low-income individuals, new patient-centered interventions advocating holistic, integrated care were needed to improve behavioral health appointment adherence. The aim of this initiative was to demonstrate the effectiveness of bundled interventions. The project objectives were to
increase the number of patients receiving mental health treatment,
reduce the number of missed appointments from cancelations and no-shows, and
decrease patient dropout rates after the initial appointment.
Conceptual Framework
The Theory of Planned Behavior was utilized in this project to design interventions that target mental health program adherence. The theory provided a holistic approach for involving the patient and health care team in changing subjective norms, attitudes, and perceived behaviors toward mental health (Ajzen, 1991). In this project, brochures, posters, and discussions with clinic staff were designed to portray IBH care as a positive measure that contributes to overall well-being. Education and follow-up conversations with patients on the benefits of mental health services and integrated care promoted positive attitudes and improved motivation to pursue healthy behaviors. Awareness that subjective norms are favorable toward counseling was raised in the discussion that occurred during the provider/patient follow-up phone calls. The end goal is that the perceptions that mental health problems are a sign of weakness and that treatment is socially unacceptable will be negated and patients will fully engage by being an active participate in mental health sessions.
In addition, the plan–do–study–act (PDSA) was incorporated for evaluation of the interventions. It is derived from the Deming Quality Model and has been effectively applied in health care settings, including low-income clinics. It uses easily adaptable techniques to analyze data and measure compliance with expectations that have already supported improved patient outcomes (Baker et al., 2014). It was chosen as a framework for this project after proving to be successful with other collaborative, quality improvement approaches in this organization. Two cycles of the PDSA were completed in this pilot project (see Figure 1). The project was also added to the clinic’s ongoing quality improvement program for annual review.

Plan–do–study–act: Cycles 1 and 2.
Method
Setting
The setting of the project was a low-income clinic in a rural, Mid-Atlantic state with a patient census of just over 1,000 patients aged 18 years and above. Twenty-one percent of patients seen have a diagnosis of chronic depression and/or anxiety. In 2016, an IBH program was established based on the community need for mental health programming utilizing on-site counselors to provide mental health services to all who met clinic eligibility requirements. In the first 11 months of the program, 158 patients were served and 333 counseling sessions attended. Patients verbally reported to staff that the sessions were helpful; however, preliminary data gathered through the electronic health record (EHR) scheduling system revealed that 43% of appointments were missed from cancelations or simply not showing up (commonly referred to as no-shows), 52% of patients never returned for a second session, and 78% had three or fewer visits. This situation put a strain on IBH program, because valuable slots were wasted and counselors were left with nothing to do.
Participants
The population was low-income adults older than 18 but less than 65 years who met clinic income criteria and had mental health needs as determined during eligibility and clinic assessments by staff using screening tools (Patient Health Questionnaire–4 [PHQ-4]) and interviews. A retrospective chart review proposed to look at 6 months of information on all patients scheduled for one or more counseling sessions. The counseling session did not need to take place for the records to be included. Patients who spoke a language other than English or Spanish were excluded from the study, as the educational materials were only available in English and Spanish.
Data Collection Methods
A pre- and posttest measurement of data was chosen as the approach used to establish whether a relationship existed between improved adherence and the bundle of education, handoffs, and phone calls. Knowing it would not be possible to determine the effect of individual interventions, the study looked at the impact of intervention results collectively using chi-square for statistical analysis.
The researcher, with the assistance of clinic volunteers, was responsible for gathering and analyzing the data. A retrospective chart review (preintervention) provided baseline data and consisted of visit information on all clinic patients who were scheduled for one or more counseling sessions. The same data were collected post intervention. The clinic’s EHR was used to obtain data on the number of mental health counseling sessions, the number of patients receiving counseling, the number of missed appointments (canceled and noncanceled), and dropout rates (number of actual visits per patient).
To ensure quality of the analysis, as much information as possible was downloaded directly from the EHR. Data that were manually entered was cross-checked 3 times by the researcher. A quantitative data consultant reviewed data and the accuracy of analysis.
PDSA Cycle 1
The project was a longitudinal, descriptive, pilot project. A collaborative project team consisting of the researcher, clinic administrator, nurses, nurse practitioners, volunteer counselors, social work, and doctoral student faculty gathered and reviewed the data obtained from the retrospective chart review. They developed interventions based on (a) clinic data that showed deficiencies in the program (% missed appointments, no. of appointments/patients), (b) research on best methods for evidence-based practice, and (c) the collaborative team’s perception of the underlying problem and barriers based on observation and patient feedback.
Following institutional review board (IRB) approval, the team completed a worksheet for the first cycle of the PDSA and devised a procedure that incorporated the use of bundled interventions into new patient and follow-up visits. This procedure was updated after data analysis. Interventions were intended to increase participants’ motivation to adhere to treatment and included three elements:
Education: Brochures/visuals/materials portraying the components of the clinic’s integrated model of care and the benefits to holistic treatment were designed and made available to patients. Patients received brochures in the initial eligibility appointment on the benefits of multidisciplinary mental health/behavioral health treatment and were informed that their providers may determine that counseling will help improve overall health. Posters were displayed in clinic rooms, bathrooms, lobby, and the front desk. This education was intended to increase insight (knowledge of need and the integrated approach) and mental health literacy, hopefully decreasing fear and hesitation to seek and receive services.
Warm handoff: An introduction consisting of a warm handoff and tour of the mental health visitation rooms with Behavioral Health Counselors was done after the first medical visit. This was intended to increase the comfort level with counselors and improve understanding and awareness of the services offered.
Follow-up: Follow-up calls were initiated by behavioral health counselors for missed appointments. For this pilot project, the counselors called all patients who missed counseling appointments for follow-up on the reason for missing appointment, the motivation and intent to reschedule and continue with treatment and any concerns related to treatment and/or social stigma. This step was intended to explore personal stressors and increase motivation to adhere to a treatment plan.
Results
Over the course of the study, 72 patients who were seen in the IBH program met eligibility criteria. This exceeded the expected number of patients for the pilot (25) and resulted in 296 mental health visits scheduled during the 6-month initiative. Of 296 scheduled mental health appointments, 104 were in the preintervention group and 192 in postintervention group. Preintervention data consisted of 2 months of visits and postintervention consisted of 4 months of visits.
Descriptive Statistics
Pre- and postdata on the 72 patients and the number of visits were analyzed and compared for statistical significance. Data were entered in SPSS Statistics version 24 and Excel. Chi-square was used for statistical analysis. The average number of mental health sessions that were attended by a patient preintervention was 30 and postintervention 34. Patients were 13.3% more likely to adhere to the appointment after the bundle of interventions was introduced (see Figure 2).
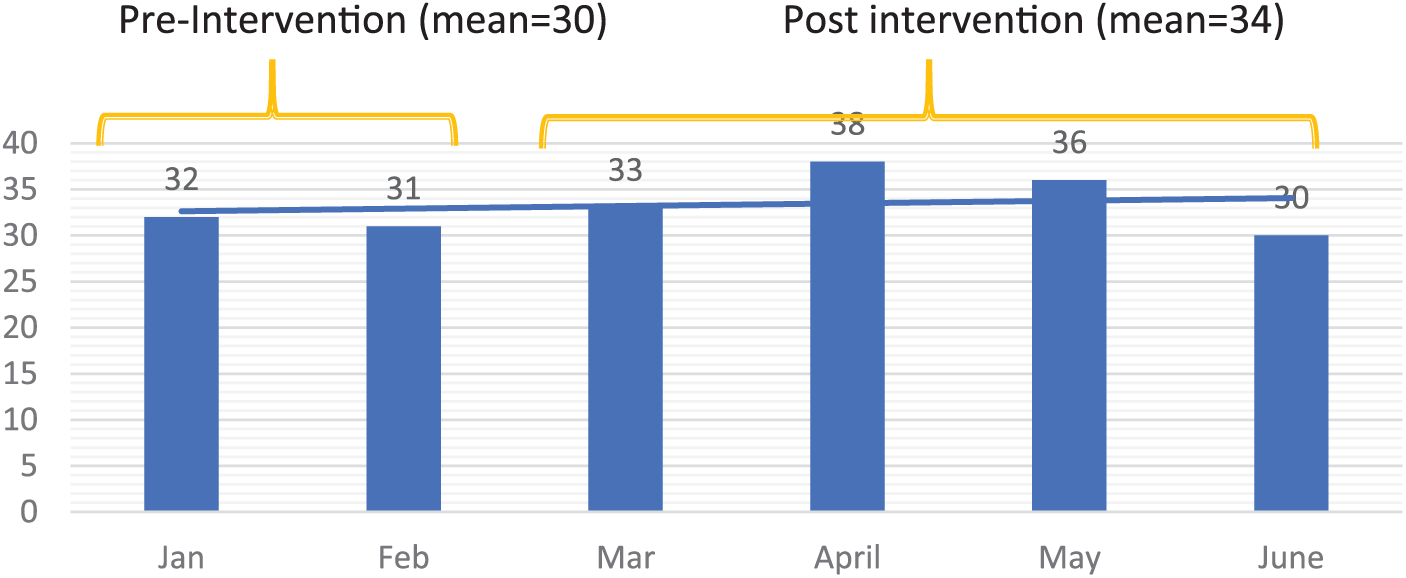
No. of patient sessions with a mental health counselor pre- and postintervention.
Of the 33 patients who were new to the clinic during the 6 months of data collection, two (15%) out of 13 in the preintervention group who received treatment with a counselor continued treatment after one to two sessions. Five (25%) out of 20 stayed in treatment in the postintervention group, showing a 66.6% increase for patients staying in treatment after the bundle was introduced.
To compare the appointment status of mental health visits pre- and postintervention (seen, no-show, canceled), the number for each was calculated (see Table 1). The mean for each group and percentage change was then determined (see Figure 3). After the introduction of the bundled interventions at the clinic, the average number of patients who kept their scheduled appointments and were seen by a mental health specialist increased by 22%. The average number of patients who no-showed for their appointment decreased by 60%, and the average number of patients who canceled decreased by 15%. These differences were significant (χ2 = 9.263, df = 2, p < .01). After the intervention, patients were more likely to keep their appointments and less likely to miss or cancel.
Total Number of Seen, No-Show, and Canceled Visits.

Note. χ2 = 9.263; df = 2.
p < .01.

Pre and postintervention means of “seen,” “no-show,” and “canceled” visits.
PDSA Cycle 2
After the project data were analyzed, the collaborative team met for the second PDSA cycle to review challenges, improve sustainability, and guide future practice. This was approximately 3 months after PDSA Cycle 1 commenced. Team discussion exposed the following barriers to the process for follow-up calls: (a) Counselors were calling only patients who no-showed for an unknown reason, not those who had notified the front office that they were going to be absent, (b) the procedure and form for documenting calls had been moved to a location distant from the counseling rooms, and (c) new counselors rotating into the clinic were not being updated on the purpose and procedure for follow-up calls. Barriers to the warm handoffs included (a) lack of an easy way to document the encounters, (b) patient privacy issues, and (c) lack of consistent personnel for process. A second PDSA worksheet for Cycle 2 was developed to meet the barriers and incorporate new methods to improve and sustain the process.
Discussion
Findings of the pilot project validated the benefit of using a bundle of interventions to improve mental health appointment adherence. Seventy-two patients participated in the IBH program during the study period and showed improved adherence with the 296 visits that were scheduled. Seventy-two percent of scheduled appointments were kept after being introduced to education, follow-up phone calls, and warm handoffs as opposed to 59% who were not exposed. Patients were also more likely to remain in treatment after one to two visits. This implies that patients felt more comfortable with counseling sessions and were more motivated to adhere to a behavioral health treatment plan.
The project had several strengths. First, the IBH program and procedures were already in place, providing an existing framework for improvement. Improving adherence enhanced the safety, efficiency, and effectiveness of the established program. Second, staff and volunteers were successful in other projects at the clinic and were open to evaluation and change. Third, the interventions were not costly to implement, requiring only minimal resources for the printing of brochures, flyers, and posters.
Data verified that there was a relationship between the status of appointments and bundle of interventions. Although research suggests that the individual interventions can have positive results, no research has used this combination of methods to address the problem of poor adherence. As a result of the bundle, patients were more likely to stay in treatment and the low-income clinic was able to fully utilize the counselors’ volunteered time by not having an appointment scheduled with no one to see.
Limitations
The clinic was aware that nonadherence was not always intentional or showed noncompliance. Child care issues, the lack of reliable transportation, and employment responsibilities were frequently cited by patients as contextual reasons for missing appointments. The clinic was limited in their ability to address these elements due to the scope and costs of underlying issues. Thus, the project was limited to interventions that were easily supported within the current infrastructure.
The primary challenge of the program was there was no way to determine whether one intervention was more effective than another. Although overall results were positive, it remains unknown whether the individual interventions of education, warm handoffs, or follow-up calls had greater impact within the bundle. This was complicated by the fact that an unknown number of participants received follow-up phone calls and handoffs. Although the health care providers acknowledged that these interventions took place, the imprecision in method collection resulted in an inaccurate count of those who participated. As a result, one could surmise that the education intervention was the most effective and the usefulness of handoffs and phone calls questionable.
A second challenge is a result of lack of access to data. Small, low-income clinics are seldom affiliated with larger hospital systems and therefore lack the ability to acquire “big” data needed for analysis of research. This dependence on others limits the extent for what is known regarding interventions and the improvement of health and cost savings associated with new processes.
Third, because small clinics are frequently limited in staff and resources, a challenge lies in their capacity (manpower needed) to enact multiple interventions. This potential barrier should be acknowledged and understood ahead of time. For this reason, the interventions of handoffs and phone calls underperformed. Additional research on utilizing the educational intervention alone would be useful.
Finally, the small size of the pilot design is a limitation because it cannot account for attribution. There was no way to control the possibility that the cause of behavior could have been due to additional internal or external characteristics, rather than to the planned interventions. A more robust research design and a larger sample are needed to prove the interventions effective.
A modification was made to data collection. Data collection was scheduled to cover 7 months; however, the first month was excluded because the clinic began an incentive program that allowed patients in all appointments (not just mental health) to obtain a month of free medication for one full year without a “no-show” visit. Excluding the first month prevented this contextual element from interacting with the intervention and kept the impact of the new incentive program element consistent throughout the entire project.
Implications
The CBPR approach is based on working with communities. This project utilized community data and collaboration to design and improve a program focused on meeting the needs of a vulnerable population. It united the interest of health professionals, academics, and the community and defined a research opportunity that gave the underserved population a voice. The project identified a community need, recognized the intensity of the problem, gathered partners, and responded in a way that positively impacted the community. This collaborative effort of individuals and agencies improved services and grew the number of counseling sessions to 200+ in a 6-month time period.
This project was useful because it piloted the implementation of an inexpensive bundle of interventions that could be well suited to low-income clinics and other settings where resources are limited. The bundle was easy to incorporate into practice, consisting of simple educational materials and noncomplex procedures for phone calls and handoffs. In this pilot, results were impressive. The occurrence of missed appointments dropped significantly and overall adherence improved by 22%. The challenge lies in the capacity of small numbers of staff and volunteers to enact multiple interventions. This challenge must be acknowledged and understood ahead of time. As the outcome was positive even when the handoffs and phone calls underperformed, additional research on the impact of the educational intervention alone would be useful.
Sustainability of the initiative was ensured by utilizing the PDSA model. In addition to the two completed cycles, the project was added to the clinic’s ongoing quality improvement program for annual review. Sustainability of the program will also depend on having an on-site leader or manager who is in charge of the process to continuously promote the interventions and to sustain excitement for the project. In this particular clinic, the Clinical Director who is responsible for ensuring clinic protocols are followed, took over this responsibility from the researcher, and will continue working with the collaborative team to improve outcomes.
Success of an IBH and Primary Care program depends on a well-planned model that identifies appropriate, attainable, and positive outcomes for the population. This pilot project highlighted the benefit of using multiple interventions to address adherence. Incorporating the use of education, follow-up phone calls, and warm handoffs was successful in improving attendance rates at mental health appointments. Low-income clinics with limited resources can easily replicate this program to improve mental health literacy, decrease stigma, and improve motivation, allowing vulnerable populations access to the needed behavioral health treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.