
Abstract
This article details an account of a young female with congenial aglossia. Because of the low incidence of this anatomical and physiological presentation, this narrative review includes a brief historical review of the disorder and a detailed description of: (1) reports in the literature of congenital hypoglossia and aglossia, (2) characteristics of speech in children with congenital aglossia below the age of 18 years, and (3) the medical history, speech acquisition, and course of intervention of a 5-year-old girl with congenital aglossia currently in speech treatment.
Introduction
This article introduces the reader to the condition of congenital aglossia (CA), in which individuals are born without a tongue. There are few documented cases of CA from the literature because the majority of infants born with aglossia do not survive without medical intervention, due primarily to complications with the airway and/or feeding. The authors will detail a narrative review and case description of KG, a now 5-year-old female born with the condition of CA. Complicating factors in KG’s history include an inability to feed orally at birth with a resultant gastronomy tube, and a tracheostomy due to the presence of excessive pharyngeal tissue causing airway insufficiency. This CA case study is unique as the information was gathered through record review, parental interview, and 30 days of direct intervention with KG from two speech-language pathologists (SLPs) with expertise in this syndrome. The client’s medical history and current path toward speech sound acquisition will be discussed in hopes of assisting other professionals and families working with a child or client with CA.
Background Literature on CA and Hypoglossia
CA is a rare syndrome in which an individual is born without a tongue. It was first documented in 1718 by de Jussieu. According to Salles et al. (2008), the condition of CA is caused by a failed embryogenesis of the lateral lingual swellings and tuberculum impar that occurs during the fourth to eighth gestational weeks. The term aglossia refers to the congenital absence of the entire tongue. The related terms, microglossia and hypoglossia, refer to an abnormally small tongue and an incompletely developed tongue, respectively (Salles et al., 2008). A review of the literature reveals reports of aglossia and hypoglossia associated with limb deformities (Alexander, Friedman, Eichen, & Buchbinder, 1992; Christian, Goldberg, Sturman, & Ingersoll, 1984; Coşkunfirat, Velidedeoğiu, Demir, & Kurtay, 1999; Grippaudo & Kennedy, 1998; Gupta, 2012; Hall, 1971; Howard & Hurt, 1976; Johnson & Robinow, 1978; Kettner, 1907; Knoll, Karas, Persing, & Shin, 2000; Lustmann, Lurie, Struthers, & Garwood, 1981; Mishima, Sughara, Mori, & Sakuda, 1996; Nevin, Burrows, Allen, & Kernohan, 1975; Rosenthal, 1932; Simpson & Meinhold, 2007; Tüysüz, Erginel, Unutmaz, & Cenani, 1994; Wada et al., 1980; Wadhwani, Mohammed, & Salm, 2007; Yamada, Konno, Yoshimichi, Saitou, & Kochi, 2000), deafness (Higashi & Edo, 1996), situs inversus (Amor & Craig, 2001; Dunham & Austin, 1989; Jang, Lee, Choung, Son, & Tockgo, 1997), thyroid dysfunction (Kantaputra & Tanpaiboon, 2003), and several associated craniofacial syndromes (Kuroda & Ohyama, 1981; Neidlich et al., 1988). Another common condition accompanying both CA and hypoglossia is micrognathia (Roth, Sommer, & Strafford, 1972). See Figure 1 for images on CA (Allison et al., 1987).

An image of the PwCA from cineradiographic data collected by Allison et al. (1987).
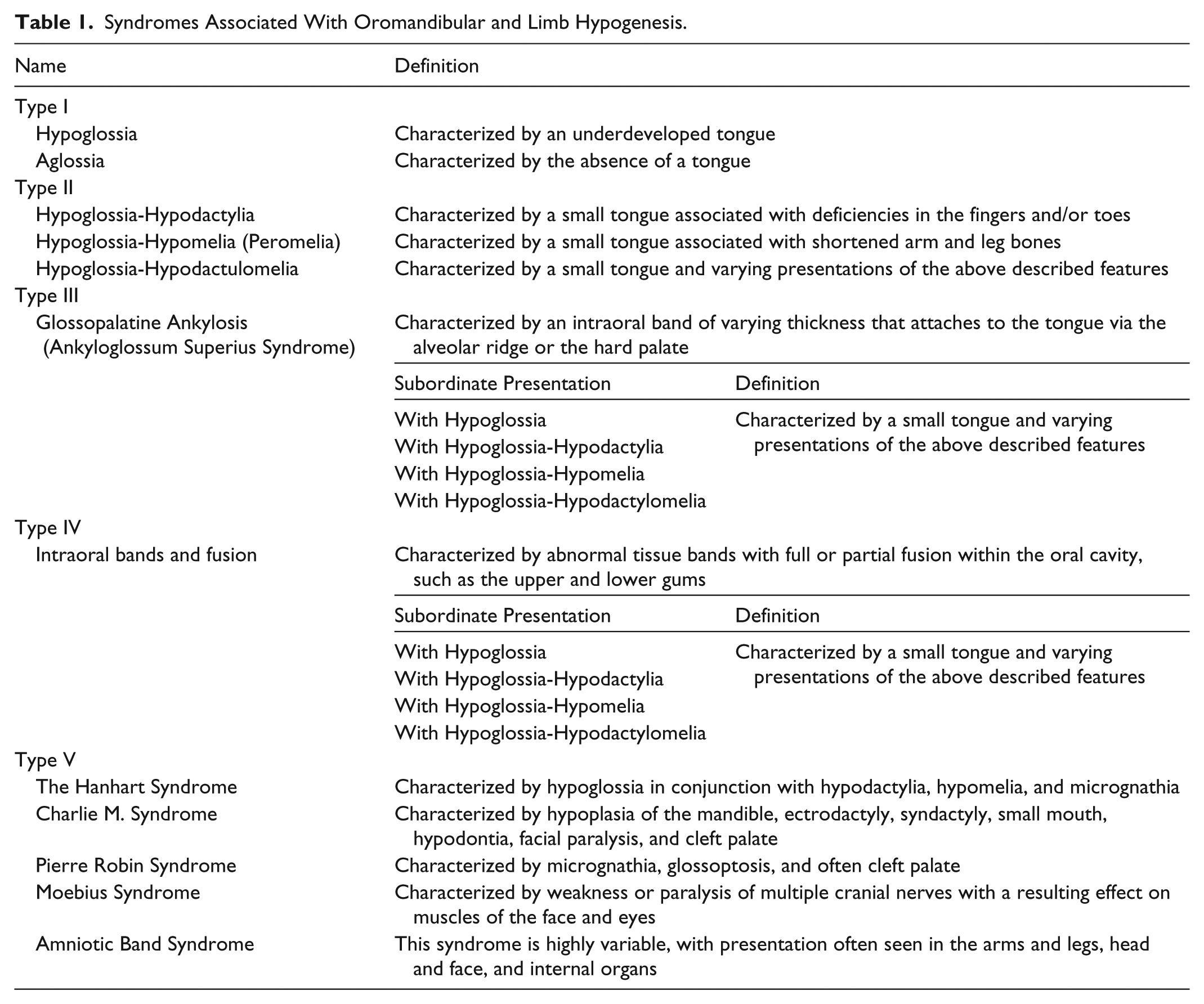
The above syndromes are collectively referred to as oromandibular-limb hypogenesis syndromes (OLHS) (Grippaudo & Kennedy, 1998) and occur only rarely across populations. In 1971, Hall conducted an overall classification of OLHS, as seen in Table 1.
Syndromes Associated With Oromandibular and Limb Hypogenesis.
The terms microglossia and hypoglossia are often used interchangeably in the literature to describe aglossia. However, true isolated CA, in absence of other syndromes or symptoms, has been described in only 13 reports (Allison et al., 1987; de Jussieu, 1718; Eskew & Shepard, 1949; Farrington, 1947; Goto, Tanaka, & Iizuka, 1991; Higashi & Edo, 1996; Khalil, Dayal, Gopakumar, & Prashanth, 1995; Kumar & Chaubey, 2007; Kuroda & Ohyama, 1981; Pettersson, 1961; Rasool et al., 2009; Salles et al., 2008; Watkin, 1925). Cineradiographic and audio-visual materials from the 16-year-old female cited in Allison et al. (1987) have been studied extensively (McMicken et al., 2014; McMicken, Vento-Wilson, Von Berg, & Rogers, 2015; McMicken, Von Berg, & Iskarous, 2012). Additional studies have been conducted using electropalatography, videoflourography, and real-time magnetic resonance imaging (MRI) with the person with CA (PwCA) in her 40s (McMicken, Von Berg, Wang, Kunihiro, Vento-Wilson, & Rogers, 2015; McMicken, Kunihiro, Wang, Von Berg, & Rogers, 2014; McMicken et al., 2017; McMicken, Vento-Wilson, Wang, & Rogers, 2015). In addition, taste testing was conducted with the female as an adult (Mahood, Wang, McMicken, & Rock, 2017; McMicken, Wang, & Vento-Wilson, 2014).
Description of Speech in Pediatric Cases of CA
There are only six accounts in the literature of speech in a child with CA (CwCA). The earliest account in the literature is found in de Jussieu (1718), which was translated by Twisleton (1873) when he described the speech of a 16-year-old Portuguese girl as . . .speaking is performed by her so distinctly and so easily that one could not believe that the organ of speech is wanting to her, if one were not told of it beforehand; for she pronounced in my hearing not only all the letters of the alphabet, and several syllables separately, but even a series of words forming complete sentences. I remarked, nonetheless, that among the consonants there are some in particular which she pronounces with greater difficulty than others, such as C, F, G, L, N, R, S, T, X, and Z; and when she is obliged to pronounce them slowly or separately, the trouble which she takes to sound them is manifested by a stoop of the head, in which she draws in her chin towards the throat or larynx, as if to raise the latter, and pressing it, to make it come near the teeth, and to bring it to their level. (pp. 62-63)
In 1907, Kettner cited a case of a 4-year-old male CwCA, and concomitant syndromes (i.e., cleft and limb deformities), that was later described by Rosenthal (1932), Fulford, Ardran, and Kemp (1956), and Ardran, Beckett, and Kemp (1964). This case and others are described in Table 2.
Characteristics of CA Speech With Comorbidities.

Note. CA = congenital aglossia; CwCA = child with CA.
This case was originally documented in 1925 by Watkin; however, that manuscript was not available to the authors at this time.
In 2008, Salles et al. described the speech of a female CwCA who had undergone mandibular surgery and speech therapy: Our patient had a neutral voice quality and moderate impairment of nasal resonance. She also had severe articulation problems, with more marked distortions in the articulation of the phonemes /t/, /d/, /n/, /s/, /z/, /s/, /f/ and omission of the phonemes /l/ and /r/. She tried to make the lower lip touch the maxillary incisors to articulate linguodental phonemes, but had marked difficulties because of lack of muscle tone, which made her speech sound imprecise and slurred. Speech and hearing therapy improved this pattern, and after 10 months of exercises, the plosive phonemes /t/ and /d/ and the nasal phoneme /n/ became clearer and better articulated. The fricative phonemes /s/ and /z/ also became clearer, but distortions in the articulation of the phonemes /f/ remained. (p. 46)
The next example of a CwCA is found in Rasool et al. (2009) with a brief description of the speech of a 6-year-old male who, according to the article, demonstrated difficulty pronouncing lingual consonants.
Medical History of 5-Year-Old KG
The present article focuses on the case history of KG, a female CwCA, which was obtained through record review and parent interview. KG was born at 37 weeks gestation to a healthy 26-year-old primigravida woman. Antenatal testing and morphology scans conducted throughout the pregnancy were reported as normal. KG had a birth weight of 2.29 kg and was delivered vaginally with forceps assistance secondary to prolonged fetal tachycardia. KG was hypoxic at birth, requiring continuous positive airway pressure and suction for resuscitation. KG was diagnosed with CA, and an ultrasound of the neck at 6 months showed incomplete thyroid gland formation with an absent left lobe and isthmus. These results were supported by a thyroid scan conducted at a nuclear medicine facility. Magnetic resonance imaging conducted in the same time period showed a large anterior pituitary gland. See Appendices A and B for detailed speech-language therapy notes, and goals and objectives.
Clinically, KG presents with severe micro- and retrognathia and congenital atrophy of the anterior tongue. KG has an abnormally v-shaped lower alveolar margin and a high arched palate; however, there is no evidence of cleft palate. KG was determined to have a normal karyotype. The presenting factors of (a) micrognathia and (b) upper airway and oropharyngeal obstruction, secondary to hypertropic wall-of-mouth, with ptosis of rudimentary posterior tongue intruding into the pharynx, contributed to an obstructive respiratory deterioration. Because KG was not intubatable, an emergency tracheostomy was performed at 3 weeks of age. Under general anesthetic, KG appeared to have grossly normal laryngeal anatomy and epiglottis. KG spent her first 2 months and 2 days in a tertiary hospital before being discharged to the family.
A key challenge in this case was KG’s severe vomiting (on average 16 times per day) up until the age of 2;5, which required admission to a hospital on at least two occasions for dehydration. Different diets, including prescription elemental diets and medications (i.e., domperidone, omeprazole), were trialed throughout this period without clear effect. Although an investigation under general anesthetic appeared normal, pathology showed evidence of intestinal inflammation. Issues with constipation were managed via daily doses of macrogol. KG also had difficulty managing her oral secretions up until the age of 3;9. This manifestation was controlled to a degree using the medication glycopyrrolate, which was gradually decreased by age 4;5. Other challenges included management of the tracheostomy and percutaneous endoscopic gastrostomy (PEG) in terms of risk aversion, suctioning, tube changes, and assistance with dressing, bathing, and stoma care.
The complex medical needs of KG required a 24-hr commitment for her care by the family, and sometimes up to a dozen appointments per month with multiple disciplinary teams at a tertiary hospital. Initially, the required commitments presented significant financial and social burdens upon the family. KG was otherwise developing cognitively and physically fairly typically. Audiology assessments were conducted intermittently, and at age 3;6 KG was discharged from a healthy hearing program after both ears showed normal middle ear pressure and mobility, and hearing within normal limits. Earlier, tympanometry showed eustachian tube dysfunction bilaterally and partial transient evoked otoaccoustic emissions bilaterally.
In addition to the emergency tracheostomy performed at 3 weeks of age, at 8 months of age, KG underwent an advanced glossopexy to pull the hypotrophic tongue anteriorly. Until 8 months of age, KG received nutrition and fluids via a nasogastric tube until a PEG was placed. While reducing the frequency of vomiting, this resulted in the deciduous teeth becoming retroclined. As such, at age 4;3, a partial release of the glossopexy was performed, and uvulectomy of the bifid uvula with scarification of the palate was performed. KG’s first teeth emerged at 9 months of age, and she lost her first tooth at age 4;10. In the same year, a sleep study was performed with the tracheostomy tube capped, and normal sleep architecture was recorded. Oxygen saturations were well maintained with baseline saturations in the high 90s and carbon dioxide did not increase above 45 mmHg. An investigation under anesthetic by multiple teams determined unfortunately that KG remained unable to be intubated at this stage and so a decision was made to leave the tracheostomy in situ. The tongue-base remnant was visible at the oropharynx level and only the floor of the mouth was visible in the oral cavity. The oropharyngeal isthmus was described as extremely narrow.
Socialization, Language, and Swallowing
The parents have attempted to provide KG with as typical an upbringing as possible, despite the significant challenges associated with the tracheostomy in unfamiliar settings. Toward this end, KG attended an early childhood development program 1 day a week from age 3;0 and a day care facility for 10 hr per week. KG attended kindergarten from age 4;0, initially for 3 days a week, and progressing to 5 days a week for the second half of the school year.
In an effort to support the linguistic development of their child, KG’s parents attended classes in Auslan, the signed language of the Australian Deaf community, and taught this language to their daughter. This early reliance on signed language resulted in KG signing the single word “hello” at 8½ months of age, and combining signs at around 16 months of age. A series of signed words were used by 18 months and complete sentences by 20 months. By age 3;0, KG’s signed language vocabulary was approximately 200 words. By age 4;0, KG could write and type her name and other basic words, and recognize approximately a dozen sight words. Per parent report and observation by the primary investigator, KG demonstrates complex and extensive signed language. KG has also experimented with augmentative and alternative communication (AAC) in the form of a graphic symbol–based AAC system, Pragmatic Organization Dynamic Display (PODD) books, from age 1;9. However, KG was reported to preferentially opt for signed language. High-tech AAC systems such as computer applications on an iPad (i.e., Proloquo2go, Words for Life–LAMP) have been used as well. KG demonstrated some interest in the Word for Life application for several years. KG always has and continues to demonstrate age-appropriate receptive language abilities.
The road to oral language has been long and challenging for KG. At 6 months of age, she produced only very soft squeaky sounds. It was not until age 2;8 that KG was able to tolerate the Passy Muir Valve (PMV) for any length of time. Despite struggling to manage oral secretions in the early years of life, KG began to swallow small volumes of water at age 4;0. At age 4;2, KG produced her first oral word, “mum” /mʌm/. This production correlated with her ability to swallow larger volumes of water and being able to coordinate blowing some air out of her mouth. At age 4;5, KG could approximate a short basic phrase, although it was normally produced in imitation. Examples of attempts at early spoken phrases include “Mum no” /mʌm no/, “More mum” /mo mʌm/, and “I want more” /ʌ wa mo/.
Speech-Language Intervention Program
The development of the intervention program for KG involved careful analysis of the anatomical and physiological characteristics of KG’s oral structures within the following hierarchy: (a) establishing a longer duration in her use of the PMV, (b) establishing the air flow required for phonation (see Appendix B for the full description), (c) establishing oral structure movement that had never been used for speech or swallowing, and (d) establishing coordination between lip and jaw movement. Once these motoric patterns were stable, the focus of intervention shifted to a phonetic approach and the production of vowels and consonants in isolation and in combination. The initial vowels selected were based on vocal tract shapes and involved the neutral vowel (e.g., /
Subsequent targets were identified and introduced in the following hierarchy:
/a/ as in “ha ha”
/e/ as in “hay”
/æ/ as in “ham”
/ε/ as in “head” (KG uses this vowel as an approximation for /i/)
/o/ as in “home”
/u/ as in “who”
After the establishment of the various vowels, consonants were targeted in the following hierarchy, as seen in Table 3 (Edwards, 2003). It should be noted that KG would need to use other structures as substitutions for tongue placement.
Hierarchy of Targeted Consonants.

With consistent production of these phonemes, the intervention shifted to a phonological focus and the sounds were combined initially into simple contrasting vowel pairs with the syllable shapes of (a) Consonant–Vowel/Consonant–Vowel (C1V1—C1V1), as in the production of “ha ha” /ha ha/ and (b) Consonant–Vowel/Consonant–Vowel (C1V1—C1V2), as in the production of “puppy” /pʌpi/. At this point in the intervention, the consonant was being targeted in the initial position only. Because the goals of this intervention program included the spontaneous generation of novel utterances and the development of oral language, a focus was maintained on the progression from imitative tasks to independent production.
As KG moved through the hierarchy from a phonetic approach by producing sounds in isolation to a phonological approach by combining sounds into words, it was a logical step to shift to a semantic focus and superimpose her newly acquired speech sound production abilities onto functional and meaningful vocabulary.
Summary
KG is a bright 5;4 girl who demonstrated strong motivation in this phase of direct therapy. KG was faced with not only the deficits that CA itself presented, but also the inherent challenges due the Class II severe dental malocclusion, atypical excess tissue in the oral pharynx, and the presence of the tracheostomy, which, when not occluded, significantly impaired her ability to achieve adequate intraoral air pressure needed for most speech sound productions. In the beginning, an additional problem encountered with establishing oral airflow was KG’s lack of tolerance of the PMV, related to her inability to coordinate respiration and oral airflow. Despite these obstacles, KG achieved sufficient oral airflow and accurate production of the phonemes /m, w, h, p, b/ and a emergence of /f/. KG has selected words with /y/, such as “yeah “ /jæ/, and /n/, such as “no” /no/ and “now” /nau/. KG demonstrated a few episodes of the coloring of /l/, but replication of the production remained challenging. Future online and direct therapy will focus on increasing KG’s functional vocabulary within her existing phonemic inventory, while probing strategies for compensatory placements for other phonemes in initial, medial, and final positions, such as /n, l, t, d, s, z/. Once she demonstrates a more consistent production of /f/, the phoneme /v/ will be targeted as well.
Currently, KG tolerates the PMV for extended periods and demonstrates adequate vocal intensity and vocal quality. KG continues to practice the motor planning and sequencing required for respiration, phonation, and articulation. Because of KG’s reduced range of motion in the mandible and the severe Class II dental occlusion, she had previously struggled in earlier phases of direct therapy to exhibit little, if any, oral excursions or labial movements. In recent therapy, KG demonstrated significant improvements in the range of motion of the lips and mandible. She continues to exhibit difficulty in coordinating movements for retracted vowels in the presence of the small mandible and severe Class II dental occlusion. KG continues to exhibit difficulty controlling oral secretions and still needs to periodically pause and tilt her head back to swallow secretions more completely.
McMicken et al. (2017, 2015) discussed the compensatory articulations evident on real-time MRI studies of speech in a highly intelligible PwCA and the importance of bilabial substitutions for normally produced lingual sounds such as /t,d/. While this was a successful compensatory articulatory pattern for the adult, KG has not yet demonstrated the ability to attempt to coordinate movement similar to the PwCA.
Based on her progress to date, there is potential for KG to continue to progress in oral speech production and increase her communicative competence as a speaker. The use of Auslan and AAC devices support further language development and communication, but continue to limit the number of communicative partners. KG’s parents are an integral part of their child’s success and actively work with her, as well as her schoolteachers, to support a multimodal system of communication across partners and contexts. An ongoing therapy program is highly recommended to support KG’s continued success. In addition, KG is scheduled for a mandibular distraction, which has the potential to improve her communication abilities and create the potential of decanaualization. This surgery would widen the pharyngeal area and therefore increase oral airflow. It may also assist her ability to swallow, and therefore the potential of eating orally.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.