
Abstract
This integrative review uses an ecological framework to examine research describing multilevel contributors to health inequities among Latina childbearing women in rural U.S. communities. Rurality exacerbates existing structural issues and makes the accumulation of both social capital and cultural competence in accessing and utilizing the health care system difficult. Four electronic databases were searched—Ovid/Medline, Web of Science, Google Scholar, and CINAHL—over the period of 2006 to 2018. Twenty-nine full-text articles met inclusion criteria. Findings were that a convoluted immigration policy, health care delivery and payment systems, geographic and economic barriers, discrimination, gender roles, and reproductive coercion all contribute to decreased utilization of health care, which in turn contributes to health inequities. More attention is required to situate Latina health inequities in rural communities within the context of other health-relevant aspects of discrimination and reproductive coercion, and to understand the contribution that the health care system itself has on these health inequities. Use of the ecological framework for this integrative review integrates well with inclusive vulnerable population research approaches such as community-based participatory research, because of its multilevel focus.
Keywords
Introduction
Hispanics have surpassed African Americans to become the largest minority group in rural settings and in small towns in the United States (U.S. Census Bureau, 2010). At a time when rural populations in general are declining, there is a 2% annual increase in the rural Hispanic population, growth that is driven in large part by births rather than migration (Stepler & Brown, 2016). Almost 10% (9.3%) of the population living in rural areas and small towns is Hispanic, much larger than the 6.5% present in the total U.S. population (Housing Assistance Council, 2012).
Available population-based surveys indicate that Latinas living in the United States have better health outcomes than many other ethnic groups, especially in the areas of cancer, heart disease, and adverse birth outcomes (Centers for Disease Control and Prevention, 2014). However, in comparison with non-Hispanic Whites, they are more likely to suffer from a variety of chronic illnesses, such as diabetes, kidney disease, and liver disease (Centers for Disease Control and Prevention, 2014) and have higher rates of maternal mortality (Mathews & Driscoll, 2017). In addition, Hispanics are less likely to have recently received health care (Centers for Disease Control and Prevention, 2014) and are less likely to have a regular health care provider (Mathews & Driscoll, 2017). Lack of access to care is an endemic problem in rural areas affecting people of all ethnicities (Rosenblatt, Andrilla, Curtin, & Hart, 2006).
Health inequities are quantified by disparities in health outcomes. Disparities related to health care access and health outcomes in rural populations include decreased access to women’s health care and higher rates of cardiovascular disease, self-reported fair or poor health status, smoking, obesity, and injury (The American College of Obstetricians and Gynecologists, 2014; Committee on Healthcare for Underserved Women, 2014; Douthit, Kiv, Dwolatzky, & Biswas, 2015; Hartley, 2004). The growing population of Latina childbearing-age women in rural communities brings unique cultural and logistical issues beyond those that create inequity for rural women in general. These women may lack extended family support networks that are common in rural areas, and they are likely to experience discrimination (Institute of Medicine [U.S.] Roundtable on Environmental Health Sciences, Research, and Medicine, 2006). Latina women experience more difficulty receiving both federal and state assistance such as supplemental nutrition program for Women, Infants, and Children (WIC) (Wiltz, 2015). In addition, an already fragmented health care delivery system is even more problematic in rural settings. As debates about how the United States will structure and fund health care continue on a national and state level, rural communities strive to maintain services and struggle to provide care for those on the margins. Shortages of health personnel as well as an overall lack of access to comprehensive care are more common in rural areas (Caldwell, Ford, Wallace, Wang, & Takahashi, 2016; Weinhold & Gurtner, 2014) while appropriate care with adequate Spanish (or other indigenous language) communication occurs disproportionately less frequently in rural areas. These language services are essential for many newly arrived Latina women. In these communities, ethnicity and economic position coalesce to make access even more difficult.
Understanding health care access and possible causes of disparities in this growing demographic group is important; it is incumbent to preserve and promote the health of Latinas not simply on humanitarian grounds but to protect the health and welfare of our nation. This review utilizes an ecological framework to look beyond a normative listing of disparities to how these inequities occur, to create testable strategies that can ameliorate these disparities to achieve equity (McLeroy, Bibeau, Steckler, & Glanz, 1988). Use of the ecological framework is important for this vulnerable population because it is a way through which to highlight the social determinants of health more clearly. We intend to demonstrate the relationships between issues at multiple levels of the spectrum that may affect health outcomes and to suggest possible interventions to mitigate these findings. Performing a literature review utilizing this framework is a natural complement to vulnerable population-focused research approaches such as community-based participatory research (CBPR) because of its emphasis on multiple levels of the ecological framework, particularly community and policy (Winterbauer, Bekemeier, VanRaemdonck, & Hoover, 2016). This article integrates published research on the health disparities that contribute to health inequities experienced by Hispanic women/Latinas of childbearing age living in rural settings in the United States.
Method
An integrative literature review was conducted utilizing the following electronic databases: CINAHL, Web of Science, Ovid Medline, and Google Scholar to search for articles pertinent to the topic. The search strategy, guided by the PRISMA statement, consisted of a thorough evaluation of the literature published between 2006 and 2018 (Figure 1). The Medical Subject Headings (MeSH) terms and subheadings employed in the search process included Hispanic Americans, Health Status Disparities, Healthcare Disparities, Health Status Indicators, Health Services Accessibility, Rural Population, and Rural Health Services, all of which were combined in various ways using “AND” and “OR” operators to generate variable results. Initially, Childbearing-age and pregnancy were also used as key words, yet adding these two search terms resulted in limited number of studies. Therefore, we removed these two key words to capture more research articles. An ancestry search strategy was utilized to generate more results. The terms Latina/Latino are embedded in the MeSH term Hispanic Americans.

PRISMA.
The terms Latina/Latino and Hispanic are often used interchangeably although they have different meanings. Latina refers to a woman of Latin American descent or origin, while Hispanic refers to Spanish speakers including those who are not from or descended from people living in Latin America (Austin & Johnson, 2012). It is important to note that many immigrants from Spanish-speaking countries do not primarily speak Spanish; rather, they speak indigenous languages other than Spanish as their first language. Literature on both Latina/Latino and Hispanic populations appeared in our searches and thus both terms are included in our review. For the purposes of this review, we will include both terms and use them broadly to refer to U.S. residents with Latin American roots.
Articles were initially included for review if they met the following five inclusion criteria: (a) written in English, (b) published within 12-year period of interest, (c) focused on Latina or Hispanic populations of childbearing age, (d) addressed health disparities, and (e) targeted rural communities in the United States. Studies identified by our search strategy that included a rural population but were not conducted in solely rural settings were included. Our search employed MeSH terms of Rural Population and Rural Health Services to generate articles. Many study authors do not define rural (Sawin, Sobel, Annan & Schminkey, 2017) and this trend was noted in the current review (e.g., Arcury et al., 2015; Branch, Harvey, Zukoski, & Warren, 2010; Cashman, Eng, Simán, & Rhodes, 2011) Furthermore, there is no clear consensus, even within the U.S. federal government, on how best to define rural areas. The U.S. Census Bureau defines rural as “non-urban” (U.S. Census Bureau, 2010, p. 1). More specifically, the U.S. Census Bureau defines areas as urban when they have more than 2,500 people living in an area, and rural when there are less than 2,500 people (U.S. Census Bureau, 2010). Similarly, the Office of Management and Budget defines rural as areas that do not meet the metropolitan statistical area definition (Health Resources & Services Administration, 2017). The Economic Research Service (ERS) of the U.S. Department of Agriculture classifies U.S. counties on an urban–rural continuum (ERS, U.S. Department of Agriculture, 2018). Furthermore, the ERS uses typology codes to further categorize counties based on economic indicators (e.g., farming dependent, mining, recreation) and policy types (e.g., housing stress, low education, child poverty; ERS, U.S. Department of Agriculture, 2017). Rurality exacerbates existing structural deficits and makes the accumulation of both the necessary social capital and the cultural competence to access and utilize the health care system difficult.
As the aim of our review was to examine barriers to health equity in Latinas of childbearing age, articles that failed to identify Latinas 15 to 49 years of age as their target populations or studies conducted outside the United States were excluded from this review. Due to the paucity of literature on this subject, we included articles that studied both genders if they included women of childbearing age. In addition, articles that were unable to be accessed in full-text were excluded.
Two researchers independently screened the titles, abstracts, and compared the results of study selection. When disagreement occurred, a third researcher assisted in resolving the discrepancy. Figure 1 shows that the initial search yielded a total of 204 articles. After applying the study criteria and examining the full-text of each article, 29 research studies were included. The articles were systematically analyzed for the following characteristics: demographics, ethnic/racial comparators, research site, study aim, type of study, as well as strengths and weakness experienced by Latinas in their lives (Table 1). With the guidance of the ecological framework (McLeroy et al., 1988), researchers assigned the study findings to either the individual, interpersonal, organizational, community, or policy level (Figure 2). Using this approach allowed researchers to better understand how the ecological domains dynamically interact with each other thereby obtaining a comprehensive perspective on the health disparities that describe health inequities in Latina/Hispanic women of childbearing age, one that allowed researchers to better understand the social determinants of health and health equity. This article aims to provide a review and critique of the empirical research on barriers to health equity among childbearing-age Latinas in rural Hispanic communities.
Summary of Research Studies.

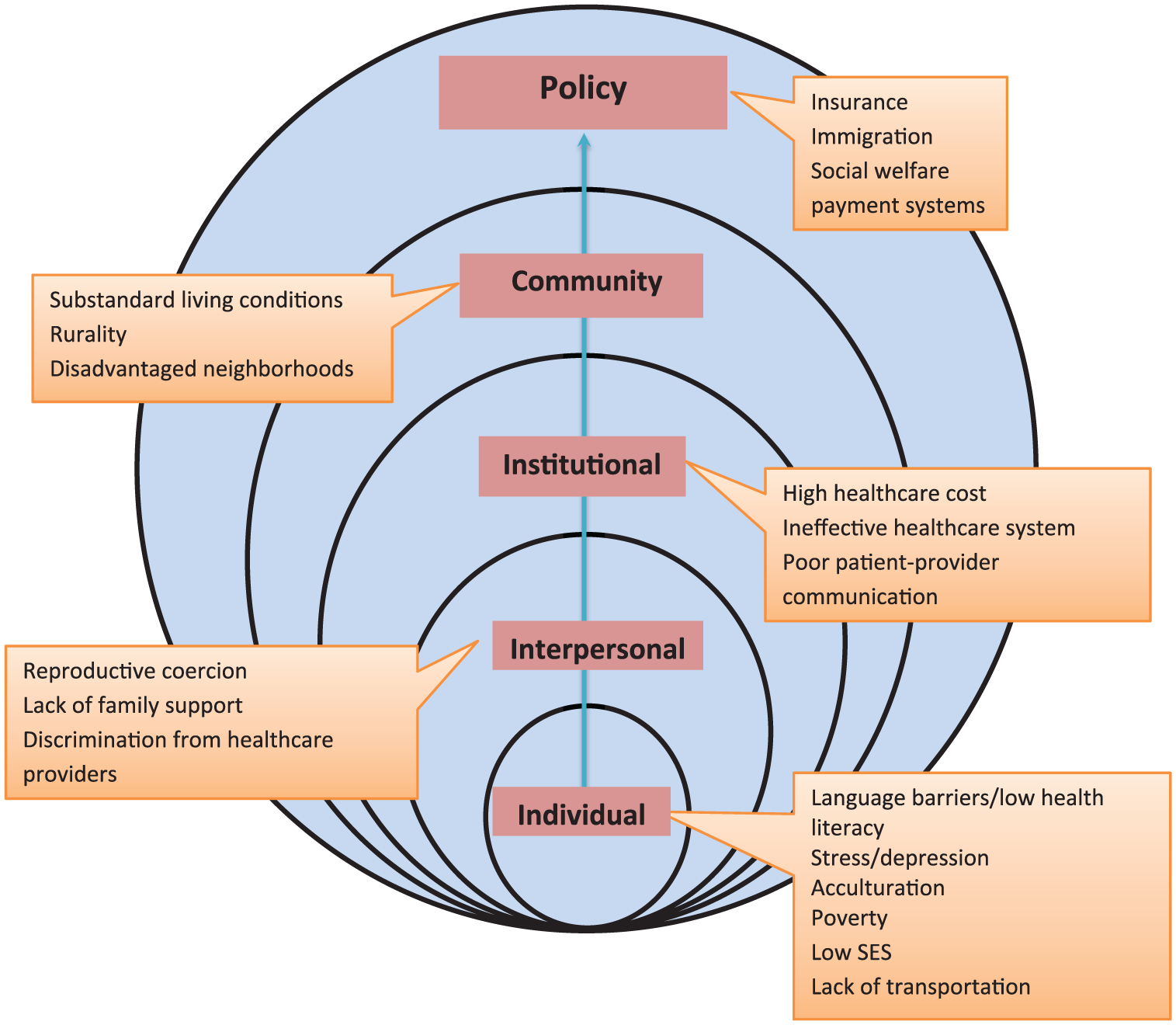
Ecological framework of health disparities in Latino populations.
Results
Sample Description
Among the identified research studies, 16 used quantitative methods, eight used qualitative methods, and two used mixed methods. In addition, seven studies utilized secondary data analysis to investigate health disparities. Study participants varied in age, race/ethnicity, and profession. Nine studies compared Latinas with women in other racial/ethnicity groups, seven studies solely focused on Latinas in rural communities, six studies examined Latinos of both genders, and four studies evaluated health disparities through the lens of health care professionals. The combination of various study designs and database analyses in this review provided a comprehensive presentation of the health status of rural Latinas of childbearing age in the United States.
The patterns of racial/ethnic disparities in health suggest that there are multiple avenues by which group membership can affect health. Table 1 illustrates the range of difficulties experienced by Latinas in rural America, including difficulties of health care utilization, sexual and mental health, pregnancy and childbirth outcomes, and living conditions that contribute to health inequities. The major identified barriers embedded in each level are specifically discussed below and displayed in Figure 3.

Frequency of issues identified as barriers to care.
Individual Level
Our findings reveal a number of barriers at the individual level that could influence well-being and health equity. The most consistently noted significant barrier was limited health care utilization. Several individual-level risk factors (acculturation, lack of health literacy, poverty, limited transportation, and mental health) were embedded within this issue, all of which limit the continuity of health care services for this population.
Acculturation
Cultural norms and health beliefs are essential in shaping health behaviors among women from Latin America. In fact, there were divided opinions regarding the effect of acculturation on people’s behaviors. First-generation immigrants preferred to preserve and use traditional health practices rather than seeking professional medical care in the first place (Butler, Kim-Godwin, & Fox, 2012; Doyle, Rager, Bates, & Cooper, 2006). Consequently, immigrants who are more acculturated have an increased likelihood of engaging with the health care system and accepting medical advice.
Conversely, some studies showed that acculturation sometimes leads to less desirable outcomes regarding health maintenance and health promotion among immigrant Latinas. For example, two studies (Harley, Stamm, & Eskenazi, 2007; Hohl, Thompson, Escareño, & Duggan, 2016) discovered that increased years of residence in the United States was associated with decreased rates of initiating breastfeeding and shorter duration of breastfeeding. In those studies, cultural beliefs, partner support, and infant feeding choices served as motivating factors of initiating breastfeeding, whereas obstacles included embarrassment about public breastfeeding, conflicts in cultural norms regarding the wide practice of formula feeding in the United States, worry about changes to breast shape, and work-related pressures.
Lack of health literacy
Low English proficiency and low levels of health literacy complicate the ability of some Latinas to understand and effectively utilize the U.S. health care system (Branch et al., 2010; Butler et al., 2012; Doyle et al., 2006). Malen, Knerr, Delgado, Fullerton, and Thompson (2016) interviewed a group of Latinos living in a rural agricultural community and found limited genetic literacy, which is the ability to acquire, understand, and use genetic information to make health decisions among this population. In addition, newly arrived immigrants frequently expressed difficulties of communicating with health care providers when an interpreter was not available. Latinas also voiced the need for more detailed explanations of diagnostic tests or treatments by providers because they often felt intimidated by the complex procedures (Butler et al., 2012). Moreover, lack of health education is a contributing factor that limits health literacy among rural Latinas. This population was frequently reported to underutilize prenatal care due to a lack of awareness and knowledge about relevant health preventive strategies as well as available health services (Cashman et al., 2011). When they were receiving prenatal care, there were widespread misconceptions about the causes of birth defects, and the usefulness, risks of and differences between screening and diagnostic tests (Griffiths & Kuppermann, 2008). Although the majority of Latinas expressed the importance of receiving health screenings and acquiring pregnancy prevention strategies, we observed a pattern of findings regarding knowledge gaps and misconceptions on these topics.
To improve health literacy, participants in Cashman et al.’s (2011) study recommended the development of a sexual health intervention that would equip Spanish and/or indigenous language speakers (if possible) with knowledge and skills about pregnancy, contraceptive use, and sexually transmitted infection prevention. By taking full advantage of the social networks within Latino communities and applying dynamic teaching strategies to meet various individual learning needs, Latinas believed that the intervention would assist them in overcoming the knowledge gaps and in establishing healthy sexual and reproductive behaviors.
Poverty
Poverty poses a significant barrier to accessing health care services for many Latinas living in rural areas. Several research studies found that financial constraint is a major obstacle that prevents Latinas from receiving standard quality of care (Branch et al., 2010; Butler et al., 2012; Cashman et al., 2011). Although some programs offer this population relatively inexpensive health care services (e.g., affordable contraceptive methods), nonetheless the costs were too high for some families. In addition, other Latinas were concerned about the quality of care they might receive from low-cost or free services (Branch et al., 2010; Cashman et al., 2011). In Butler et al.’s (2012) study, one barrier constantly faced by Latinas was their low-income status and inability to pay insurance. Given their financial constraints, many expressed the difficulties of affording a primary health care provider or follow-up for chronic-illness management, which seriously deterred them from gaining access to health resources and maintaining their well-being.
Limited transportation
Aside from poverty, the studies documented that a large number of Latinas expressed concerns regarding the available transportation resources. In fact, having appropriate means of transportation is especially vital for rural Latinas to access health care. The lack of independent transportation options, inability to drive, and high costs of gasoline were common barriers consistently mentioned in the identified studies (Branch et al., 2010; Butler et al., 2012; Cashman et al., 2011; Cristancho, Garces, Peters, & Mueller, 2008).
Mental health risks
Latinas were at high risk of suffering from mental health issues, especially during and after pregnancy. Ceballos, Wallace, and Goodwin (2016) reported that Latina mothers who lived in rural areas had 41% increased odds of experiencing postpartum depression than White mothers (odds ratio [OR] = 1.41, p < .01). Rural Latinas were reported to have a greater risk for depression if they experienced a high level of stress (OR = 14.8, 95% confidence interval [CI] = 4.03-54.06; Jesse & Swanson, 2007). But interestingly, researchers observed that self-esteem, social support, and spirituality were not significant predictors of developing depression. The same groups of researchers examined the association between biopsychosocial risk factors and preterm birth (PTB) in rural communities. Study findings indicated that Latinas had the lowest level of self-esteem, partner support, and the lowest rates of PTB in comparison with other racial/ethnic groups. Yet the hypothesis of Latinas obtaining adequate psychosocial resources was unsupported in this study (Jesse, Swanson, Newton, & Morrow, 2009). Although the high level of stress was consistently identified in the literature, mixed evidence was noted regarding Latinas’ mental health care seeking behaviors (Arcury et al., 2015; Doyle et al., 2006). One study observed immigrant Latinas to be more likely to seek mental health treatment than U.S.-born White women (OR = 2.17, p = .021). However, the authors further pointed out that the experience of stigma or other barriers may later intimidate them from receiving treatment (Nadeem et al., 2007). On the contrary, another study found that Latinas had increased odds of not seeking help for depression (adjusted odds ratio [aOR] = 3.2, 95% CI = [1.3, 8.1]) in comparison with other racial/ ethnic groups. Overall, what made the results distinct was that rural residents across all racial/ethnic groups were found to be active in seeking mental health treatment (aOR = 0.3; 95% CI = [0.2, 0.7]; McGarry, Kim, Sheng, Egger, & Baksh, 2009).
Interpersonal Level
The interpersonal level incorporates Latinas’ relationships with family members and health care providers. This review notes gender inequality and reproductive coercion within families, as well as discrimination in health care facilities, as interpersonal barriers.
Gender inequality and reproductive coercion in families
Reproductive coercion and health care access are closely related. Particularly, male partners play an indispensable role in decision making about health care service utilization among rural Latinas. One study argued that although Latino couples commonly identify equality as an important quality in relationships, in practice men retained more relative power than women (Zukoski, Harvey, Oakley, & Branch, 2011). Similar results were also documented in Butler et al.’s (2012) and Branch et al.’s (2010) studies. The decision to seek sexual health counseling may largely depend on a partner’s comfort level; some Latino male partners oppose male health care providers performing reproductive health examinations on their female partners (Cashman et al., 2011; Warren, Harvey, & Bovbjerg, 2011). In addition, a male partners’ unwillingness to use contraception, or their limited knowledge on HIV/STIs prevention, serves as constraints for women trying to obtain and use contraception (Branch et al., 2010). However, Zukoski et al.’s (2011) study posits that Latinas who migrate to the United States tended to play a more independent role and demand egalitarian relationships with their partners, which suggests a shift in cultural beliefs regarding gender roles and reproductive decision making among immigrant women, a shift that is not yet fully realized in practice.
Discrimination in health care settings
Not surprisingly, ineffective relationships with health care providers were noted by both Latinas and clinicians. In fact, the perceived discrimination from health care providers was commonly noted when asking Latinos their perceptions about the quality of health care. In Branch et al.’s (2010) study, a pre-focus group questionnaire with 66 health care providers and office staff revealed that 35% of the respondents voiced that discrimination from health care providers affected Latinos’ access to health care. This was echoed in the Cashman et al.’s (2011) article. The gaps between perceived health care quality and expectations further impaired Latinas’ abilities to build trust with providers. One study suggested that their dissatisfaction with the health care system partially results from their perceptions that chronic illnesses can receive apparent improvement through short-term treatment (Butler et al., 2012); however, there was also concern expressed by Latinas that their health problems were not correctly diagnosed (Trangmar & Diaz, 2008).
Institutional Level
Moving beyond the individual and interpersonal levels, the organizational level represents health system barriers, such as complexity, poor system-wide communication among providers, and poor accommodation of language barriers at the organizational level.
Health system barriers
One prominent gap identified in the literature was that few Latino populations were familiar with where to obtain the available health care resources and how to successfully navigate the health care system. At the individual level, Latinas identify their lack of health system literacy (Cashman et al., 2011) contributing to barriers at this level of the framework. This “cumbersome” system contained multiple and lengthy procedures for registration and payment, posing enormous challenges to immigrants with low English proficiency or little formal education (Branch et al., 2010). In addition, several studies demonstrated a strong association of high medical cost with health care underutilization among Latinas (Branch et al., 2010; Cristancho et al., 2008; Doyle et al., 2006; Sampson et al., 2009).
Lack of continuity, cooperation, and communication among health care providers additionally hampers the quality of health care services rural Latinas receive. Sampson and colleagues (2009) describe a lack of communication between physicians and pharmacists in the authorization of dispensing emergency contraceptives, which made the process complicated and hindered Latinas’ access to contraceptive methods. Although Park, Rodriguez, Hulett, Darney, and Thiel de Bocanegra (2012) found that long acting reversible contraceptive methods were generally more available in rural areas, when the predominant population being served was Latina, this trend was reversed. Two studies revealed the insufficiency of Spanish-language services in the health care system (Doyle et al., 2006; Sampson et al., 2009). Sampson et al. (2009) reported only half of the pharmacies within the study area offered interpretation services. Even in rural areas that offered Spanish-language services, Spanish speakers still were the least successful of all callers to receive contraceptives. Besides inadequate or nonexistent interpretation services, the inconvenient clinic hours, feeling of being rushed during doctor visits, and long waiting times were also highlighted as barriers to preventing Latinas from accessing health care services (Branch et al., 2010). Studies have described the development of lay-health navigator programs that successfully overcome health systems barriers in clinics serving breast, colorectal, and cervical cancer patients (Meade et al., 2014; Wells et al., 2012).
Community Level
The community level represents environmental barriers within the ecological perspective (McLeroy et al., 1988), namely substandard living conditions and geographical barriers due to rurality.
Substandard living conditions
The well-being of Latino families was strongly associated with living conditions. Arcury et al.’s (2015) study showed that the stress levels of Latina farmworkers were significantly associated with the characteristics of their housing and neighborhoods. A majority of the study participants lived in substandard rental housing and neighborhoods where traffic and community settings prevented them from easily getting access to public services and facilities. Consequently, the deficient living conditions led to the social isolation and diminished well-being of Latino immigrant families in rural communities. In addition, living conditions which lack sanitation and proper ventilation as well as hazardous work environment exposure (chemical toxin, injury-prone tasks, and health-threatening weather conditions, etc.) placed farm workers at increased risk of developing health problems (Doyle et al., 2006). Furthermore, findings presented by Torres-Aguilar, Teran-Garcia, Wiley, Raffaelli, and Morales (2016) revealed a high prevalence of food insecurity among Latino populations. The detailed analysis suggested that harmful dietary patterns were associated with household food insecurity, whereas getting access to food resources and information as well as language acculturation served as protective factors of promoting healthy dietary practices in Latino families. Thus, an inability to access nutritionally adequate food products with reasonable prices seems to be a major concern in rural Latino families.
Geographic barriers
In comparison with urban areas, rural Latinos and other minority groups constitute a smaller proportion of the population (Housing Assistance Council, 2012). Many Latinos reported the advantages and disadvantages of living in rural communities. Rurality can potentially contribute to the isolation of Latinas in communities. The long distance to amenities and the amount of time spent in traffic were major reasons that inhibited this population from engaging in social activities (Branch et al., 2010). Moreover, rurality affects women’s health. Lack of available conventional medical treatment led some to alternative therapies taught by family members to treat infections and digestive difficulties and for prenatal remedies (Trangmar & Diaz, 2008). Study findings indicated that rural Latina mothers, especially between the ages of 10 and 17, were more prone to develop potentially avoidable maternity complications than Caucasian mothers (OR = 3.29, p < .05), due to inadequate prenatal care and lack of obstetric care providers in communities (Laditka, Laditka, & Probst, 2006). Similarly, another study described rural residency to be associated with excessive pre-pregnancy weight gain (30.7% vs. 25.8%) as well as inadequate gestational weight gain (30% vs. 27.2%) in women when compared with those who lived in urban areas (Gallagher, Liu, Probst, Martin, & Hall, 2013).
In contrast, one research team illustrated that rural residence, if located in towns with populations in the 10,000-40,000 range, could have a potentially positive effect on Latinas’ health. These communities have reduced rates of PTB and low birth weight in comparison with those living in urban areas or relatively sparsely populated rural communities (Hillemeier, Weisman, Chase, & Dyer, 2007).
Public Policy Level
At the all-encompassing level of public policy, issues related to health insurance, national immigration policy, social welfare system, and the construction of the health system itself lie at the core of barriers to care for rural Latinas of childbearing age.
Insurance policy
Lack of health insurance emerged as a common factor contributing to inadequate access to health care services (Butler et al., 2012; Cashman et al., 2011; Cristancho et al., 2008; Doyle et al., 2006). With the high expenses of health care and limited financial resources, many Latinas were not able to afford regular clinical visits or follow-ups (Butler et al., 2012). Cristancho et al. (2008) identified three populations that were least likely to obtain health insurance: (a) new immigrants who had limited English proficiency; (b) immigrants who had incomplete documentation or could not afford health insurance; and (c) Latinas who do not qualify for public or private insurance coverage, or had limited knowledge about insurance.
Immigration policy
Aside from the barrier to accessing health insurance, policy has had a massive influence on rural Latinas’ daily lives. Since the 1970s, there has been a steady flow of migration across the U.S. southern border. This influx has resulted in a substantial number of undocumented persons illegally living in the United States. Several laws have been mandated to report any person without legal documentation (Gutierrez, 2016). Several authors (Cashman et al., 2011; Cristancho et al., 2008; Doyle et al., 2006) found that difficulties in obtaining legal immigration status and documentation serve as significant factors impeding adequate and appropriate health care services utilization among Latino populations. Latino focus-group participants reported their experiences as undocumented immigrants or non-U.S. citizens led to either restricted access to health care or receipt of low-quality care and services (Cashman et al., 2011). U.S. laws and policies restrict Latinos’ full participation in the workforce and access to benefits, such as social welfare and health insurance, and many are at risk of being deported from the United States (Gutierrez, 2016).
Social welfare policy and system design
Latina women expressed that there should be more local public assistance programs in the community that could help them acquire information or resources about public aid benefits (Cristancho et al., 2008). Furthermore, the interviews done by Cristancho et al. (2008) suggest that there are system design issues that need to be addressed. These issues surround health care payment, but also assumptions about when clinics should be open for appointments, where clinics are located, and the types of supports needed for people to be able to leave work and get to appointments. Cashman et al. (2011) noted uncertainty around a variety of systemic matters, ranging from the documentation necessary to access health and social services to physical examination procedures and recommendations for contraceptive use. Furthermore, Cashman et al.’s (2011) focus groups described the need for involvement of health care providers in the Latino community to advance health promotion and health education.
One of the barriers encountered when trying to understand and improve health disparities in rural areas is the lack of sufficient data. For example, the data that states provide to national data sets such as the Behavioral Risk Factor Surveillance System often undersample rural areas (Bopp et al., 2012). In contrast, some large data sets are able to identify disparities in specific disease outcomes (e.g., Keegan et al., 2015).
Another obstacle is presented by the siloed nature of federal funding schemes. Programs developed as pilot programs can receive research funds, but lack a source of ongoing funding, making it difficult to sustain capacity to meet community health needs (López-Cevallos, Dierwechter, Volkmann, & Patton-López, 2013).
The results generated from this review demonstrate that the combination of factors at individual, interpersonal, institutional, community, and policy levels interact and contribute to unique disparities in Latina women’s health. Use of these findings, organized in this way, can help researchers to more clearly understand the complexities of issues facing rural Latinas, and hopefully, ultimately, design more effective interventions.
Discussion
This review demonstrates factors that contribute to health disparities in access to care for rural Latinas that exist across the social ecological spectrum. The usefulness of employing an ecological framework in a discussion about issues affecting a group of individuals, in this case, rural Latina women of childbearing age, is threefold. First, it provides an opportunity to examine how a factor at one level could perhaps be approached and mitigated by action at another level. Second, it demonstrates opportunities to target both individuals and at least one other component of the social environment. Third, it is a method that demonstrates potential for integration with community-partnered research from a social justice perspective. Through use of the ecological framework, we examined the underlying issues identified in the literature that may contribute to our understanding of barriers and opportunities to achieving health equity for rural Latinas of childbearing age. This, along with a community based participatory research approach, will hopefully lead to more relevant research questions and effective and appropriate interventions.
Given the growing Latino populations in America, especially the influx of new immigrants in rural communities where available resources and supports are lacking, the study findings reveal multifaceted challenges facing this marginalized vulnerable population group. For example, many eligible Hispanics do not receive Supplemental Nutrition Assistance Program (SNAP) assistance, especially immigrant families or households consisting of U.S. and non-U.S. citizens (Delgado, Vargas Poppe, & Lopez, 2015). SNAP is intended to provide food resources to families who are at risk of food insecurity. Yet concerns about eligibility restrictions and immigration status deter many individuals from receiving benefits (Delgado et al., 2015). Correspondingly, data from the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) program (Thorn et al., 2015) show that a larger percentage of Latinos (70.7%) have incomes at or below the Federal poverty guideline than non-Latinos (65%). The gaps are more significant in women at the childbearing age, as the proportion of Latinas with no incomes at pregnancy (94.5%), breastfeeding (94.8%), and postpartum (92.6%) are relatively higher than women in other racial/ethnic groups (Thorn et al., 2015). Because many barriers are remediable through policy, initiatives are needed to narrow the health disparity gaps in the Latino population in comparison with non-Latino whites.
The difficulties addressed at each ecological level may provide guidance for researchers, practitioners, and policymakers who endeavor to improve access and equity in health care for rural Latinas. Furthermore, this is an opportunity for increased collaboration across health care specialties to address these inequalities at multiple levels.
Several articles in this integrative review demonstrate that CBPR is an effective approach to use with vulnerable populations. The CBPR approach was invaluable for Doyle et al. (2006), as the research team sought to form mutually beneficial community partnerships within the difficult-to-access migrant, seasonal farm worker population. The CBPR approach helped to establish stakeholder groups, which in turn informed and strengthened research (Doyle et al., 2006). The use of the CBPR approach helps researchers to assess the cultural and social contexts as well as the strengths and assets of the participant community, leading to inclusive collaborative research practice, essential for the establishment of trust within vulnerable populations (Cashman et al., 2011; Cristancho et al., 2008). This is especially important when researching sensitive topics such as mental health, violence, and sexual health, which are uncomfortable or even possibly shameful to discuss or disclose (Cashman et al., 2011).
Limitations
Our study is subject to the limitations of our search terms and strategy. The most significant limitation of the study is the small amount of research focused on rural Latinas of childbearing age. Limiting the review to Latinas of childbearing age focuses inordinately on issues related to maternal health rather than other (equally if not more important) chronic adult health conditions. Perhaps in the authors’ attempt to move beyond the rates that illustrate the health inequities of Latinas by focusing on the contributing barriers at the community and policy levels, we have unintentionally masked important inequities. A strength of the review is the broad nature of the literature reviewed. However, we cautiously urge readers to utilize studies of such broad groups of people as those that identify as Latina or Hispanic with the understanding that there will be variation in beliefs, values, practices, and past experiences. These variances can render quite different outcomes for an in-depth examination of a specific individual, family, or community.
Another limitation of this study is that an integrative review can only discuss what has been already published. For instance, poverty is generally recognized as a significant driver of negative health outcomes (Abdelsttar, Hendren, & Wong, 2017; U.S. Department of Health and Human Services, 2012). The findings identified in this review, however, suggest that individual-level utilization of and policy-level availability of health services are the main contributors to an individual’s’ overall health status. These findings are reflective of the search criteria we have focused on for this literature review.
Finally, we were unable to address all subgroups of the Latino population. For instance, the study authors did not differentiate differences among first- and second-generation immigrants, and how that affects health care access; therefore we were unable to explore what are likely significant differences. None of the study authors fully explored the vast differences among the many ethnicities from Latin American countries such as language, educational background, and socioeconomic status. In addition, people from Central America were underrepresented in study samples, whereas Mexican participants were overrepresented.
Implications for Research and Practice
This review identified 29 articles exploring health disparities among childbearing Latinas in rural Hispanic communities. Individual- and policy-level issues were the most frequently identified in these studies, followed by institutional level concerns. Given the barriers which have been documented at multiple levels for Latina women in the rural setting, a collaborative approach to providing health care between provider and community members would be a useful strategy.
Inadequate Spanish-language resources, for example, go beyond the lack of printed materials and extend to every facet of the system from receptionist to provider to bill collectors. However, nurses and other health care providers should make education of this population a priority, especially as related to efficacy of traditional health practices, breastfeeding, and health literacy (Branch et al., 2010; Butler et al., 2012; Doyle et al., 2006; Harley et al., 2007; Hohl et al., 2016).
Inequities that stem from language issues are in part due to an individuals’ language skills, but also reflect the discrepancy between the demographics of health care providers and that of the general population (Phillips & Malone, 2014; Valentine, Wynn, & McLean, 2016). Health care providers should be educated about barriers to care and their own role in the perception of discrimination and of inadequate health care. Further assessment is needed to evaluate risk for illness and disease sometimes overlooked in this population (Nadeem et al., 2007). A long-term strategy that will help remove some of the interpersonal and community-level barriers to health equity is to work toward achieving equity in health care professional training programs such as medical and nursing schools.
Past attempts at the policy level to ameliorate language barriers experienced by individuals (Chen, Youdelman, & Brooks, 2007) have not been entirely effective, as demonstrated by multiple studies in our review (Branch et al., 2010; Butler et al., 2012; Cashman et al., 2011; Doyle et al., 2006; Sampson et al., 2009; Torres-Aguilar, Teran-Garcia, Wiley, Raffaelli, & Morales, 2016). Unfortunately, there is still a gap between the intent of such policies and the execution of them to form a patient-friendly environment for Spanish speakers in rural areas. Indeed, this action at the policy level to intervene at an individual level has been employed in regard to issues affecting other marginalized populations (e.g., Poundstone, Strathdee, & Celentano, 2004), with equally unsatisfactory results. For these policies to effect change, they need to shape multiple levels of the socioeconomic spectrum to alter the environment and ameliorate issues.
Many of the issues that at first glance appear to be individual-level barriers arise from a lack of willingness to fund and support infrastructure at the policy and community level. For instance, the inability of a rural Latina to obtain transportation is not only a result of her not owning a car or a driver’s license, but also due to the lack of public transportation in her area. Immigration status is another circumstance that results from both individual or interpersonal choice but is informed by the labor workforce needs and networks that exist in institutions and communities (Hertz & Zahniser, 2013; Nelson, Trautman, & Nelson, 2015).
In comparison to their non-Hispanic counterparts, Hispanic women in the United States are disproportionately at risk for various health-related problems such as asthma (Hunninghake, Weiss, & Celedón, 2006) and obesity (Slattery et al., 2006), and they are less likely to use contraception (Dehlendorf et al., 2014). These disparities are best addressed through community and policy-level commitments to fund increased access to programs targeted at prevention in work environments, access to healthy foods, and early interventions.
It is worth mentioning that several new policies have been enacted to reduce health disparities in Latinas. For example, the Affordable Care Act has expanded health insurance coverage to 4.2 million Latinos. Nearly 8.8 million Latinos with private health insurance are able to utilize preventive services such as mammograms and cervical cancer screenings (Denys Reyes, 2015). Efforts to address health inequities at the policy level seem mainly concerned with payment for services. Access to health insurance is notably a key to reducing health disparities (Abdelsttar et al., 2017). Lack of Latino physicians is a barrier that policy directives and funding could ameliorate (Sánchez, Nevarez, Schink, & Hayes-Bautista, 2015). Because many barriers are remediable through policy, initiatives are needed to narrow the gaps in health equity in the Latino population in comparison with non-Latino whites.
These inequities in the health care experiences of rural Latinas, as a consequence of the current political climate in the United States, are likely to become even more fragmented before they will be fixed. The breakdown of the social contracts of private insurance, as evidenced by discussion of whether men should pay for prenatal care, attempts by the United States to defund Title X (Clerk of the U.S. House of Representatives, 2011), and the proposed “regressive redistribution” of wealth proposed by the 114th U.S. Congress (Oberlander, 2017) as part of the ongoing rhetoric and attempt to dismantle or repeal the Affordable Care Act (2010) lead us to believe that political maneuvering is trumping effective public policy at this juncture.
Finally, study findings noted that gender impacted health care for women. For instance, at the individual level cultural norms impacted breastfeeding. And at the interpersonal level a major contributor to contraception use access in the Latina population related to reproductive coercion, which at its’ core is a gendered issue. This was not named by Cashman et al. (2011), yet their findings support the prevalence of this phenomena within Latino families. Gender dynamics affecting the issue of reproductive decision making among Latino families need to be addressed through further research.
Conclusion
By 2025, Hispanics will be the largest minority group in the rural United States (Kandel, 2005). Approximately 30% of Hispanic women give birth before the age of 20 (Martin et al., 2011). And the birthrate for Latina teens in rural counties (47 per 1,000) is 50% greater than in urban counties (31.4 per 1,000; Hamilton, Rossen, & Branum, 2016).
Although many programs exist to address their needs, barriers to health care access remain. Solutions directed at dismantling these barriers cannot be swiftly implemented due to current political constraints. These constraints only emphasize the need to make drastic multilevel policy and programmatic changes to improve health equity for women of childbearing age and their families who live in rural areas. In the meantime, it will remain important to track individual-level barriers to health equity in Hispanic and non-Hispanic rural communities. However, it is also critical that we continue to identify higher level policy issues that contribute to health inequities in the rural Latina childbearing population.
Although resources and policy in the United States could be flexed to improve health care access and outcomes in rural areas for all who live there, the current unraveling of the social contract suggests we are entering an era void of any long-term commitment to fund and implement successful strategies to achieve health equity. Nonetheless for the sake of the well-being of rural childbearing Latino families who contribute to the food security and industry of our nation, health care and immigration policies should be reformed in the opposite direction from that being currently promoted in the U.S. Congress (Sessions, 2017). Fixing inequities experienced by this growing segment of our rural population, upon whom we depend as our labor base for our agricultural production, is vitally important for the welfare of our nation. Policies that promote access to health care, address poverty issues, and improve living conditions in rural areas, while attending to health and health system literacy in this population, should be advanced and implemented.
It is our responsibility to address health inequities for rural childbearing-age Latinas through funding the testing and implementation of multilevel interventions to eradicate barriers to health and health care access. The CBPR approach is essential because CBPR incorporates attention to social justice and human rights issues, which are at the core of the health inequities within this vulnerable rural Latina population, many of whom have experienced trauma. The participatory, partnering nature of CBPR allows researchers to utilize culturally sensitive, collaborative research techniques that can directly address power imbalances (Winterbauer et al., 2016). Engagement of community members as partners (not as research subjects) fosters, in theory, increased trustworthiness of the researchers and a high level of veracity of information from the community itself. This constant, open communication with the community about the research and the research process through the CBPR approach may lead to immediate benefit to the community itself, perhaps in the form of better health care or improved health care access. It is only by examining and designing interventions to address multiple structural and social practices, with thoughtful and careful incorporation of the community itself that there will be forward progress in assuring that rural childbearing Latinas achieve health equity in the United States.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.