
Abstract
So far, reablement is mainly developed in care for the elderly. This study adds knowledge about reablement in mental health care and the contribution of occupational therapists to this field. Qualitative interviews with 10 occupational therapists were conducted and analyzed using a qualitative content analysis. Reablement is built around everyday activities, used as systematic tools for stepwise improvement of mastery and bettered mental health. The findings support a greater emphasis on reablement and recovery in mental health care. Reablement demands multidisciplinary teams, where occupational therapists can bring important skills and perspectives. Occupational therapists can contribute substantially to further reablement. Their knowledge about—and therapeutic use of—everyday life activities seem to be a useful approach to helping people with mental illness. The occupational therapy foundations are highly related to the elements of recovery.
Introduction
The article presents a Norwegian study adding knowledge about reablement for people with mental illness, in addition to what the role of occupational therapists might be in this context. Reablement is a kind of rehabilitation where everyday life and mastery is seen as the basic point of departure (Ness et al., 2012). It has a preventive and rehabilitative focus central to user management and mastery, with an emphasis on the individual’s resources and participation.
The Norwegian health care system is based on the principle that everyone should have the same access to health services regardless of socioeconomic position and geographical location. The health service in Norway is structured on three levels; a national/state level, the four regional health authorities (RHF) and the municipal level (Spilker, 2015). The role of the state is to establish a national health policy, design and manage health legislation, and manage funding. The four RHF and the municipalities are responsible for the service itself. Reablement is provided by multidisciplinary teams organized by the municipalities.
Most of the projects on reablement undertaken in Scandinavia focus on elderly care and are, according to Laberg and Ness (2012), characterized by the following factors:
It takes place within the user’s arena, both at home and in the community.
Common everyday activities are used in rehabilitation.
It is an offer for elderly people, although there is no clearly defined minimum age.
It has a preventive perspective, because it maintains a mastery of everyday activities.
It has an early multidisciplinary assessment.
Intensive efforts are made at an early stage to intervene before the individual has lost significant functions.
While Cochrane and colleagues (2016) have come up with this description: Reablement [. . .] is frequently time-limited (usually six to 12 weeks) and aims to maximize independence by offering an intensive multidisciplinary, person-centered and goal-directed intervention. (p. 2)
There are several countries with similar rehabilitation interventions to those in Norway (Tuntland & Ness, 2014). In the United Kingdom, Ireland, and Denmark the term “reablement” is used for this kind of rehabilitation, while “restorative care” is used in the United States, Australia, and New Zealand (Tuntland, Aaslund, Espehaug, Førland, & Kjeken, 2015). They all address the same service users and emphasize an early, multidisciplinary, complex, and individualized reablement (Tuntland & Ness, 2014). In Norway, the occupational therapists and the physiotherapists take the lead role in the teams; while in the other countries it appears that nurses more commonly have a central role (Tuntland & Ness, 2014).
Tuntland and colleagues (2015) describes the reablement intervention as follows: The intervention is targeted, multicomponent and intensive, and takes place in the person’s home and local surroundings. The focus is on enhancing performance of daily activities defined as important by the person. The aim is to increase independence in daily activities, and enable people to age in place, be active and participate socially and in the society. (p. 1)
Recently, a report on follow-up research on reablement for the elderly and for people with intellectual disabilities was published in Norway (Langeland et al., 2016). The study shows that both groups benefit from reablement. For the elderly group the effect was significantly better compared to usual services/rehabilitation. In the group with intellectual disabilities the results showed a reduction in depression/anxiety and a general improvement of health measures. However, the report points out that people with mental health issues often are excluded from reablement and that more research on this field is required (Langeland et al., 2016). Reviews from other fields (see, for instance, Langeland et al., 2015; Tessier, Beaulieu, Mcginn, & Latulippe, 2016) show good results from reablement as well.
The foundation of occupational therapy is to support health and participation in life through engagement in occupations (T. Borg, 2007; Creek, 2005), as everyday activities affect our health and well-being, and give life meaning (Townsend & Polatajko, 2007). People with mental health problems may experience great difficulty when performing daily activities (Lindström, Lindberg, & Sjöström, 2013). Recovery from mental illness involves a process of development, in which people regain the power to influence and shape their own lives (Topor, 2006). The philosophical foundations of occupational therapy and the elements of recovery are highly correlated (Krupa, Fossey, Anthony, Brown, & Pitts, 2009). Through a client-centered approach, the occupational therapist sees a person’s participation and involvement as vital, and elements such as motivation, individual goals, and a sense of meaning are linked to the occupations to achieve a satisfactory result (Creek, 2005).
Aim of the Study
The aim of this study is to contribute to the knowledge on central topics in reablement in mental health care and on what occupational therapists can bring to this field. In particular, two topics are addressed:
What is meant by reablement in mental health care?
How can occupational therapists contribute to processes of reablement for people with mental health problems?
Method
To meet these aims, a qualitative and descriptive method was used (Silverman, 2000). Respondents expected to have comprehensive knowledge of reablement were interviewed. The empirical data was analyzed by qualitative content analysis (Graneheim & Lundman, 2004).
Respondents
A strategic sample (Malterud, 2011) of 10 respondents, 8 females and 2 males, was recruited by the first author’s professional network and professional organizations in the field of occupational therapy. The inclusion criteria were respondents who were educated occupational therapists, and who had experience of working within the field of mental health, and/or had knowledge of reablement. Nine out of 10 of the respondents had experience within different approaches to rehabilitation and mental health care, including reablement strategies, whereas one respondent had an expanded knowledge within reablement. The respondents worked within health care at different levels, or held positions related to the development of occupational therapy as both a profession and an academic field, and had working experiences from different geographical and socioeconomic settings.
Data Collection
Qualitative semi-structured interviews were used for the data collection, which allowed the respondents’ free descriptions (Kvale & Brinkmann, 2010). All respondents were informed about the study in a two-step process—when they were asked to participate in the first place, and immediately before the interview started. All interviewees gave their written consent to participate. The interviews were held in Norwegian. An interview guide with 12 open-ended questions was used covering topics on reablement (9) and the role of the occupational therapist (3). Positive aspects as well as potential difficulties and risks in connection with reablement were covered in the interviews. Most of the interviews lasted for more than 1 h, and took place at the respondents’ respective workplace. The number of interviews was regarded to cover the topics to a sufficient degree, as the last interviews added very little new information. One interview was conducted with two respondents present, a request proposed by the respondents themselves. All the interviews were conducted by the first author, with long-lasting experience as an occupational therapist. The second author, an experienced researcher within the field of mental health care, followed the data collection on a weekly basis. Methodological and practical issues were discussed and continuously decided upon. The interviews were recorded and transcribed verbatim.
Analysis
The data were, when the data collection was completed, analyzed by both authors, following Malterud’s (2011) description of the qualitative analytical process via four main steps. The overall aim of the analysis was to give voice to the respondents’ experiences from, knowledge of and reflections on reablement in regard to people with mental health problems.
Overall impression reading, when presumptions and theoretical frames of reference are set aside to focus on, and be open to, all sides that the data could convey (Kvale & Brinkmann, 2010). The entire data material was repeatedly read through. Significant themes, such as the importance of social network and everyday activities appeared already in this step.
Coding of significant units, when the transcripts were closely read through and significant units—parts of the text containing a meaning on its own—were identified, marked, and labeled. Significant unites ranged from one single word to a few sentences. Each unit was labeled with a short “name,” making it easy to recognize.
Condensation, when the significant units found in the previous step were read again, compared, and considered in relation to each other. In this step, the subcategories and—later—the categories described in the Result section emerged and became clearer in a process of ongoing questioning and testing of new combinations.
Synopsis when the subcategories and categories were written into a summarized text, including quotations from the interviews (Malterud, 2011).
During the process of analysis, both authors met continuously, discussed, and worked together.
Data Quality and Ethics
As all of the respondents were knowledgeable and experienced in the field of occupational therapy and mental health, the empirical data is regarded both valid and reliable. Being a qualitative study, resting on relatively few respondents, one cannot generalize the results to the entire field of reablement in mental health care. The study was based on voluntary participation and anonymity; the data material was treated with confidentiality, with access only for the two authors. The respondents participated in the study in their role as professionals, thus no private or personal matters were dealt with. The study was approved by the Norwegian Social Science Data Services (NSD, project no. 33422).
Results
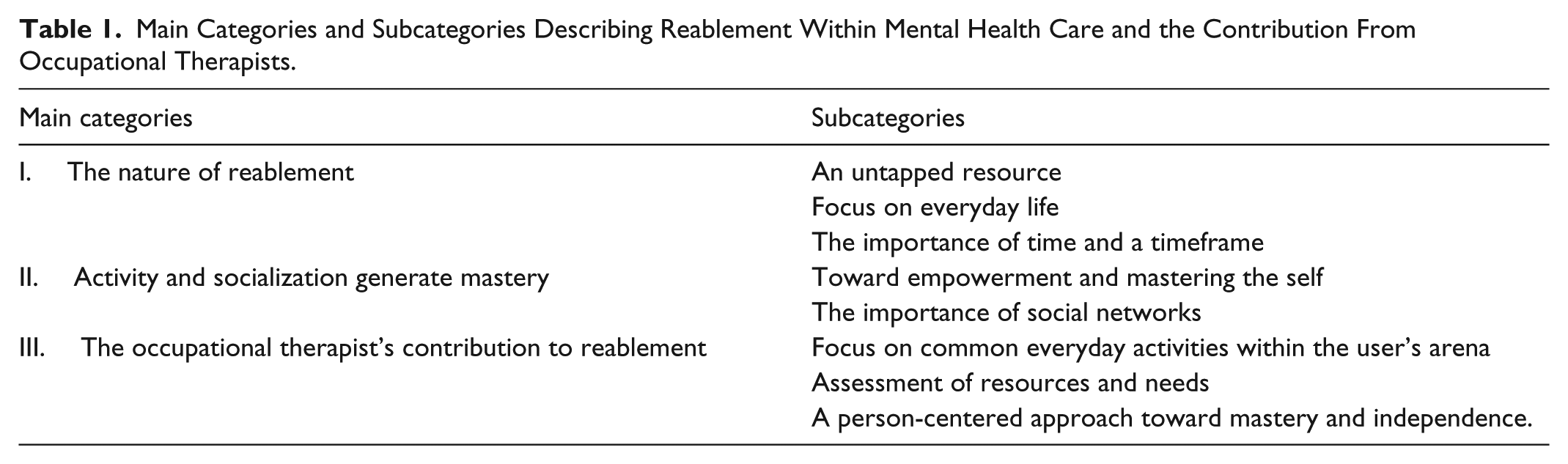
The analysis led to three main categories, each with subcategories, shown in Table 1. The categories and subcategories are described in detail below.
Main Categories and Subcategories Describing Reablement Within Mental Health Care and the Contribution From Occupational Therapists.
The Nature of Reablement
This category develops the concept of reablement in mental health care.
An untapped resource
A focus on rehabilitation within the municipalities’ mental health services is not a new dimension. A focus on everyday activities, everyday coping, and a reduction of services as users become more independent has to date been a central aspect and is relevant for all users, irrespective of the severity of their illness. Not least for those who suffer from a severe mental illness, the respondents underlined, successful rehabilitation can prevent worsening of the illness and episodes of hospitalization. However, specific models or concepts for this work have not yet been implemented. In the meantime, prevention and rehabilitation have often been overshadowed by a strong focus on nursing care in municipalities: “It’s a challenge to make health care think differently and get them into the groove of health promotion and prevention” (Respondent I).
Focus on everyday life
The main focus of reablement in mental health care should be on supporting each user to be as independent as possible and to take control of his or her life in the best way possible: It is obvious that when something happens, people must get help getting back on their feet. But it depends on how they get that help, if they get more help-reliant or if they actually get more independent. (Respondent I)
Reablement is about strengthening the user’s skills to cope with his or her everyday life with all its implications, so the person becomes self-reliant rather than needier. Sometimes, the result is clear: I led an empowerment project a while back, and there was a woman who had been receiving disability benefits for 30 years because of having a mental illness. After participation in the empowerment project, she started working fulltime at the age of 50. (Respondent G)
The most basic elements in users’ lives are to have a residence and to manage financially. When these two elements are safe, efforts can be targeted at participating in other occupations. For many, it is a challenge to manage activities such as getting up in the morning, getting out, go shopping at the store and participating in activities at a day-care center: That it perhaps primarily deals with coping in your own home and your everyday life, and it is not like training for a specific function, but here I think that you are going out into real life. (Respondent E)
It’s about helping users to learn/relearn skills they need to master the everyday life they want to live. And to be on the spot and assess together with the users’ what goals should be prioritized first for achieving their goals: And then there are people getting great job offers and internships, but if they fail to get out of bed, it somehow does not help. So, it’s about being where the problem actually is. (Respondent B)
The importance of time and a timeframe
The time dimension of the intervention is fundamental to reablement. One aspect of the time perspective highlighted by respondents is the need for enough time to develop a trustful relation with the users. They regarded a time frame of 1 to 2 years necessary for the users’ life situation to stabilize “We have a patient group who needs more time in the relationship building and it often takes a lot of time” (Respondent F).
The respondents concluded that sufficient time should be a main focus within reablement in mental health because the service users could use more time to achieve their goals. Their illness may affect their everyday life in a different way than those with physical impairments: The progress of the users varies and it can go up and down, and they must have the opportunity to try again and again. And then the question is how much time do we have . . . in the health service. (Respondent I)
If you go too fast and push too hard, it can lead to people becoming scared and refusing reablement. Therefore, the services need to be organized in such a way that they allow flexibility in the time dimension, and an ongoing adaption to the users’ situation. Several respondents related that they constantly experienced users who deteriorated when services came to a close, and they were adamant that it was important to avoid an abrupt ending.
Activity and Socializing Generate Mastery
The meaning of everyday activities is a central topic in reablement. Engagement in activity is a path toward increased coping skills, but more importantly it may mean the formation of a social network to achieve an independent and good everyday life.
Toward empowerment and mastering the self
It is usually not a lack of a physical function that keeps people with mental disorders from completing activities. It can be about the motivation and initiative to get started, as well as the belief in oneself and need for strengthening the self: It is about this drive to get started . . . to develop this drive with users, mastering experiences can be central. And in order to provide users with mastering experiences, it will be necessary to focus on the person’s resources. (Respondent D)
Many barriers and prejudices are related to living with a mental health problem. It may also involve a lot of self-stigma, with people losing their self-esteem and self-confidence. Some users need to strengthen their self-identity and improve/restore faith in themselves, whereas others may become passive when other people do things for them. By the experience of mastering different activities, they can get more motivated to develop their skills: There’s something about how you can create the motivation, the mastering experience, confidence and belief that it actually is possible. Being able to provide enough support and enough resistance, that’s the challenge. (Respondent F)
A prerequisite for mastering and personal growth is that there is a hope for positive changes. Therefore, part of the empowerment work sometimes is to convey hope to the user. “There are some people for whom you have to actually be their hope,” Respondent D said.
The importance of social networks
Many service users have access to a limited social network, and loneliness is often a part of their everyday lives. The respondents told that they often fulfilled the service users’ social needs, so they emphasized that it is important to help them find other social venues. “The reablement team must work to gradually redundant itself so they don’t become the user’s (only) network” (Respondent G).
The respondents highlighted that networking should be strongly prioritized. This calls for a network philosophy that exceeds family members and next of kin; every relationship may be included, be it the neighbor, a fellow student or an employer. Both the problems and the service users’ solutions are a shared responsibility. The next of kin may be a great resource and an important collaborative partner, and should be included in the reablement process from the start, if the service user wants it: It’s important to collaborate with next of kin to have a common understanding and common expectations for the user [. . .] so the next of kin knows what is important for the user and what promotes mastering and good health in the recovery process (Respondent F).
The Occupational Therapist’s Contribution to Reablement
This category highlights the resources of occupational therapists and how they can contribute toward helping people with mental illness through reablement.
Focus on common everyday activities within the users’ arena
Theories of occupations are a central part of occupational therapy, and everyday activities are used to assess, regain, improve, and maintain skills/functions. Moreover, occupations are considered a central part of people’s everyday lives, so there is an emphasis on the establishment of meaningful activities. An occupational therapist often starts the first conversation with questions like, “How is your everyday life?” and “Describe your typical day” (Respondent C).
All the respondents talked about how they meet the users at home or on other areas in the community. It is important to collaborate with the users where they live their lives and where they perform their everyday activities. The users’ arenas are both used in assessment of everyday activities and when everyday activities are performed to learn/relearn skills: I followed a lady to the post office one day to observe and she did everything perfectly well. This was a person I had been told had a very poor level of functioning. But I could say she had an overview of her finances. (Respondent F)
Assessment of resources and needs
A key element in occupational therapy assessment is to go into everyday activities together with the users, and to make an assessment of their resources and needs for facilitation. A central part of the assessment is observation of the user’s activity performance and here, as well, everyday activities are used: I remember I went with an older man with a walker to the grocery store and I felt everybody was watching me because I did not help him. He had to do everything by himself . . . if needed I would have assisted. But the aim was to see if he could go to the store and manage everything by himself or not. (Respondent F)
In this context, activity analysis is used to gain knowledge about skills needed for carrying out an activity. An analysis of data obtained from the initial assessment and the activity analysis is used to facilitate user performance: A part of the occupational therapist’s competence is to teach users techniques and develop plans for how users will master desired activities. I feel that a useful area, which is promoted by occupational therapists in particular, is to assess the user’s level of functioning and to motivate them to take action. (Respondent B)
The respondents have experienced that the occupational therapist is asked to make an assessment in cases where there is doubt about what potential the user has and what the user is capable of doing. A holistic assessment from an occupational therapist provides an important contribution for a multidisciplinary team to see the users’ skills and needs, and to know which activities users should be encouraged to perform themselves and what they possibly should not spend their energy on: When we come home to someone who cannot make their own breakfast, we ask ourselves; is that the optimal situation? Does the service user prefer this? Is it appropriate that the user get help with breakfast or has the home service/home nursing just started making breakfast, and continued? As occupational therapists we are questioning the intervention and try to make a holistic assessment. (Respondent H)
A person-centered approach toward mastery and independence
The occupational therapist’s competence is all about encouraging a person’s mastery and to make activity and environmental adaptations to help the users achieve participation and inclusion. In this context the occupational therapist plans for activities made to fit the users nearest zone of development, to facilitate mastery experiences. Occupational therapists place a greater emphasis on enabling the user’s functioning to his or her optimum level than on simply focusing on the disruption and deficits of a user’s skills: Another principle is often that one highlights the resources they have because there is too much focus on diagnoses. . .We want to bring out all the skills, and look for the resources. (Respondent E)
In some cases, the occupational therapist and the user may have slightly different intentions that should not always be discussed directly because they deal with vulnerable themes. The following example illustrates how an emphasis on interests, resources and experiences of mastery contributed to increased function and making the user independent in one area of her life: I worked with a lady with a serious mental illness when I found her hygiene a little suspect. This was a vulnerable subject for her; it was about her self-esteem and her intrinsic value in a way. However, she loved to swim so I encouraged her to join a group with swimming. I also encouraged her to ride her bike . . . Then by herself she got the idea that she could ride out to the beach and swim. (Respondent E)
Furthermore, the occupational therapists look at how the environment can be adapted and how this adaptation can contribute to an increase in functioning and independence in everyday occupations. Throughout the process, the focus on user involvement is significant. To achieve independence in activities, aids can be helpful. It might be cognitive aids or other aids that contribute positively to everyday life. Occupational therapists contribute with knowledge about aids and devices in the reablement team. “Some users have a good effect of weighted quilts, day boards and calendars. For others, the mobile phone can be a useful reminder aid to regain independence” (Respondent A).
Discussion
As shown in the Results section, there is a focus on rehabilitation in mental health care, although this is sometimes too unstructured and accidental. Everyday activities and user involvement permeate the entire reablement process, aspects that are well in line with the theoretical foundation of occupational therapy.
The results also show that, in practice, reablement, rehabilitation, and occupational therapy goes well together. This may not come as a surprise since the principles of reablement in Norway are based on a collaboration between the Norwegian Occupational Therapy Association, the Norwegian Nurses Organization, and the Norwegian Physiotherapy Association (Ness et al., 2012). And the Norwegian term for reablement is “hverdagsrehabilitering” which can be translated to “everyday rehabilitation.”
Reablement for Whom?
Reablement is potentially appropriate for every individual with mental health problems. Challenges in functioning and mastering an everyday life should be inclusion criteria for accessing this service (Tuntland & Ness, 2014). Respondents in this study regarded people with a severe mental illness as one of the target groups for reablement. An empirical study by Lindström, Hariz, and Bernspång (2012) showed that people with severe mental illnesses who received daily rehabilitation as home-based occupational therapy made important improvements in activities of daily living (ADLs). This is in line with the respondents’ view. However, as shown in several studies, reablement is an intervention that will suit anyone who seems to benefit from this approach, regardless of diagnosis (Langeland et al., 2015; Tessier et al., 2016; Tuntland et al., 2015).
Reablement focuses on means of prevention and health promotion (Ness et al., 2012). The respondents emphasize that one important goal for reablement in mental health should be prevention of hospital admissions. Once someone has developed a mental illness, it is not an issue of preventing it (Holte, 2012), but rather of trying to avoid new episodes (Hummelvoll, 2005). New episodes, the respondents underlined, often bring about dramatic changes in a person’s life with major loss of functions. Most reablement projects seems to focus on intervention before the individual has lost significant functions. Respondents in this study support this, but did not have it as a criterion, rather they meant that reablement can fit all.
Flexibility in Time and Availability
To avoid even more dramatic deterioration, many users prioritize getting help quickly when their condition worsens (Almvik & Borge, 2009). As a result, flexibility in the welfare system is necessary, as each individual has his or her own process with different needs for follow-up periods. This was strongly acknowledged by the respondents as well. In many cases, achieving flexibility could demand major changes in the services, meaning that they have to adapt to the user’s needs when it comes to methods, treatment arenas, and use of resources and time (Ulvestad, 2011). The reablement team must have the opportunity to follow the user’s recovery process, because their health conditions changes and will affect the need for care. Deegan (1988) emphasizes that we cannot force recovery to take place, but instead establish contexts and environments that nurture the process of recovery.
With regard to the time perspective in reablement for people with mental health problems, the respondents considered a period of 1 to 2 years as necessary for users to achieve a stable situation. We think that to help people in a process of recovery, it must be their need of time that governs the follow-up. For some users, increased flexibility will include a long-lasting follow-up. As such, it can be a preventive arrangement, thereby facilitating people’s efforts to master their everyday life. Flexibility, while avoiding administrative inertia, is also to be open-minded to the user’s own suggestions.
Everyday Life as the Point of Departure
When mental illness provokes a need for action from health and social services, it means that, in a way, everyday life collapses. In such situations, paradoxically, everyday life risks being in conflict with oneself, because it represents both the problem and the solution at the same time (Lorem, 2006). Reablement emphasize that rehabilitation should take place in the user’s arena (Laberg & Ness, 2012). Activity and participation in everyday life are the goals and means of occupational therapy intervention (T. Borg, 2007), focusing on the way in which mental illness can affect everyday life and daily occupation. For many users the days may consist of limited engagement in meaningful activities (Leufstadius & Eklund, 2008). “The primary role is to support the user to take part in meaningful occupations and to reshape a balance in everyday life” (T. Borg, 2007, p. 486). Deegan (1988) describes how recovery takes into account the entire person, not only symptoms or lack of functioning, which means that people can live with their impairments and no longer let them limit other facets of their life, but rather accept themselves and their situation.
The respondents agreed with Laberg and Ness (2012) that reablement is about taking the user’s wishes about activities in his or her everyday life as the point of departure. Such activities constitute our lives, and mastering these activities is crucial for our quality of life and well-being. The respondents regarded housing and economic circumstances as basic presumptions that must be in place before users could pay attention to other activities of everyday life. They related that most users wished to have “a normal life,” being able to master everyday ADLs on their own, which is also supported by several studies (M. Borg, 2009; M. Borg & Davidson, 2008; Deegan, 1988; Topor, 2006). To have your own home and economic security contributes toward the establishment of a frame for everyday life, as well as a place for one’s activities related to identity, personality, and personal values (Lindström, Lindberg, & Sjöström, 2011). All respondents described how occupational therapists support the service users to regain the everyday life they want. The mental illness can cause an imbalance in the users’ everyday life between the life they want and their current situation. A holistic perspective was emphasized by the respondents—to understand that people’s everyday lives are multi-faceted. This, in turn, lies well in line with the comprehensive assessment conducted by the occupational therapist.
Social Networks
The importance of social networking is well recognized both in our data set and in previous research (Almvik & Borge, 2009; Askheim & Starrin, 2010; M. Borg & Davidson, 2008; Bøe & Thomassen, 2009; T. Borg, 2007; Hummelvoll, 2005; Lindström et al., 2011). Hummelvoll (2005) points out that in social networks there are health-stimulating opportunities, and our ability to withstand and master life challenges increases if we have a good social network. M. Borg and Davidson (2008) found in their study that users also want to contribute and give something back to their network, and not only to receive help. Lindström (2011) describe how social settings create an arena for continuous learning and development of social skills. Users’ networks can be both good and bad. Good networks are characterized by the fact that they are an important source of support, sense of attachment, and self-esteem (Askheim & Starrin, 2010). A weak network may seem inhibitory and limit the person’s development capabilities.
Reablement emphasize that rehabilitation should take place in the user’s arena (Laberg & Ness, 2012). Respondents were concerned that they experienced many of the users as lonely and isolated. Loneliness and isolation can be harming in itself, but will as well mean that the possibility to acquire common-sense knowledge—by interacting with others—needed to master everyday life diminishes, according to Schütz (1970). If the individual becomes isolated and has little contact with the outside world, his or her development of everyday knowledge can be inadequate and thus affect the ability to master everyday life. In this context, respondents pointed out how occupational therapists often facilitate users to participate in activities in different social settings. Furthermore, the respondents highlighted the importance of collaboration with the next of kin. To help the service users reestablish contact with their social network can, as Hummelvoll (2005) describes, provide a good mental resistance and contribute to quality of life, for the service user.
User Participation in Assessment and Intervention
User participation is regarded as a core element in mental health care, reablement and occupational therapy (Almvik & Borge, 2009; Askheim & Starrin, 2010; Bøe & Thomassen, 2009). Askheim and Starrin (2010) emphasize that the welfare system must back out and relinquish part of the power that it has today if there is to be real user participation. Respondents related that users are anxious that the support system will enter and override their lives if they receive help. From this perspective, reablement could contribute to genuine user participation and maybe even user governance.
This study shows the importance of being respectful toward the users, taking their resources and limitations into account, and at the same time nurture the belief that change is possible. Hope is regarded an important precondition for people to be actors in their own lives (Lindström et al., 2013). For those who experience a lack of hope, it is of utmost importance that those around them can maintain that focus on hope (Deegan, 1988; Lindström et al., 2013; Spaniol, Wewiorski, Gagne, & Anthony, 2002; Topor, 2006), a notion also held by the respondents in this study.
A systematic assessment by the occupational therapist can be an appropriate way for both the therapist/reablement team and the user to discover realistic goals for the intervention. Respondents also point out that it is important to have sufficient time in the assessment because it may lead to other and more relevant goals and interventions that were not previously visible. Throughout the process it is the user’s perspective and wishes that are in focus. To have specific goals and to know which road leads forward can be of great help in a situation that otherwise seems hopeless and chaotic. Goal achievement can also give positive mental values in terms of providing self-confidence, hope and a sense of joy (Lindström et al., 2013).
The respondents underlined the importance of the occupational therapist’s role in the assessment phase as this provides the basis for the rest of the collaboration with the user. First and foremost, it could contribute to the user feeling recognized and respected because it is the user who tells about his or her life, wishes and needs. By being genuinely interested in listening to the user, the assessment phase can be an appropriate tool for the user to get a word of what one truly feels and thinks.
Lindström et al. (2013) conducted a study in which the results show that the participants were very satisfied with the occupational therapy intervention. They related that it was the first time that they had been offered rehabilitation, and that the occupational therapist played a major role in their change and development. The users described how the occupational therapists arranged for them to fulfill activities on their own, whereas they previously had got used to the municipality’s care-workers doing these things for them. The passive role and respect shown by the occupational therapists were appreciated, and made the users feel important and valued (Lindström et al., 2013).
Focus on Resources and Mastery
The focus on abilities, strengths, interests, and motivation within the user is highly relevant in the user’s recovery process. By supporting their resources, valuable experiences of mastery may arise, which in turn may strengthen the feeling of hope (Davidson, Harding, & Spaniol, 2005; Deegan, 1988; Lindström et al., 2012; Spaniol et al., 2002). People with mental health problems may have experienced numerous defeats and even small steps in the right direction can contribute to a feeling of mastery and improved self-image. The respondents underlined that people with mental health problems often have a negative self-image, therefore it is essential to emphasize challenges and activities that they have accomplished and can still master. Deegan (1988) describes how the feeling of hope can disappear when one develops a severe mental illness, also affecting the willingness and ambition to perform activities. The occupational therapist’s knowledge of how to adapt activities in relation to the nearest zone of development—activities that are partly mastered and partly challenging—is an essential contribution to this work. If the gap between the users functioning and expectations is too big, there will be no feelings of mastery. In this context, the respondents stressed that the occupational therapist, educated to make a systematic assessment and intervention, has a great potential to help people with mental health problems experience mastery in the recovery process.
Different aids/devices were also highlighted by the respondents as helpful for some service users. Furthermore, the respondents saw the occupational therapist’s knowledge and experience within this area as an important contribution in a reablement team. The literature brings out different examples of assistive devices useful in mental health rehabilitation, as, for instance, mobile devices (Briand et al., 2018), weighted blankets (Scanlan & Novak, 2015) and day boards (Røsand, 2009). Mobile phones can also be used as a reminder as it is something that everyone uses and does not stigmatize in terms of being seen as an aid. Wallis, Sutton, and Basset (2018) found that sensory modulation interventions could be a good supplement to treatment of anxiety, and that “its impact is amplified when used to support occupational engagement and participation in everyday life.” We believe this is transferable to other diagnoses, too.
Conclusion
Rehabilitation is an existing focus in a municipality’s mental health care, but it often appears to be overshadowed by nursing care. Therefore, more of an emphasis on preventive work and reablement is recommended, directed to people with mental health problems.
Currently, reablement is seen as an untapped resource, providing an opportunity for occupational therapists—but also a responsibility—to contribute to a health service where people with mental illness will be offered reablement interventions.
Reablement in mental health care will obviously benefit from the same principles as reablement for the elderly. However, some areas needing an extra focus seems to be flexibility in terms of time and availability, mastery experiences, social networks, and to follow the rhythm of the user’s needs.
Due to their knowledge about—and therapeutic use of—activities, occupational therapists can substantially contribute to reablement in relation to people with mental health problems, especially concerning activity analysis and a holistic view on the interaction between the person, the occupation, and environmental factors. The theoretical foundations of occupational therapy go well in line with the focus on activities, flexibility, gradual improvements, and increased self-esteem that characterizes reablement. As do nurturing hope for a better life as a motivating factor. Reablement in mental health care is a relatively new phenomenon, and this study only comprises a small group of respondents, hence further research in this area is highly needed, especially studies including service users.
Key Findings
Reablement in mental health care is seen as an untapped resource and as a highly relevant rehabilitation intervention reablement ought to be prioritized.
Occupational therapists can contribute to reablement teams as the core elements of reablement highly correlate with the foundations of occupational therapy.
What the Study has Added
This is the first Norwegian study to describe the contribution of occupational therapy within the combination of reablement and mental health care. Further studies, from reablement projects within mental health care, will help to define the interventions needed within this field.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.