
Abstract
Medications are the most common treatment modality for diabetes; however, medications may lead to inadvertent injury. Reducing adverse events in patients with diabetes is an important health care goal. Using pooled data from the 2011-2013 National Ambulatory Medical Care Survey, this cross-sectional, observational study explored univariate associations between patient safety for patients with diabetes as measured by adverse events and practice characteristics, including health information technology capabilities. This study found that the overall rate of adverse events among adults with diabetes is 7%, inclusive of injury, poisoning, or adverse effect of medical/surgical care or medicinal drug. We find evidence that e-prescribing, seeing a primary care provider, and being an established patient are associated with less adverse events.
Background
In 2015, an estimated 30.3 million Americans had diabetes (Centers for Disease Control and Prevention, 2016). In addition, diabetes was the seventh leading cause of the death in the United States, and medical expenditures for people with diabetes were over 2 times higher than nondiabetics (American Diabetes Association, 2013). Medications are the most common treatment modality for diabetes; however, medications may lead to inadvertent injury (Sakuma, Kanemoto, Furuse, Bates, & Morimoto, 2015). The risk is particularly important among people who take anti-diabetic medications, which are in the top five causes of drug-related adverse events. Adverse effects from anti-diabetic medications may occur due to illegible handwriting, including the improper use of abbreviations or poor communication between patient and provider (Cox & Ferner, 2009).
Improving the prescription process is among the potential benefits of the widespread adoption of electronic health records (EHRs) and the ability to find, send, receive, and integrate electronic health information (Buntin, Burke, Hoaglin, & Blumenthal, 2011; Zuckerman, 2017). In addition, electronic prescribing (e-prescribing) can help providers send accurate and legible prescriptions directly to pharmacies. E-prescribing has been shown to reduce adverse events among patients with diabetes in the ambulatory care setting (Powers, 2015). Given the potential of these types of health information technology interventions to improve care and decrease adverse events, we explore the relationship between (a) EHRs, (b) health information exchange, and (c) e-prescribing and adverse events in patients with diabetes.
Diabetes racial/ethnic disparities have been well documented in the literature (Beach et al., 2006). In addition, racial/ethnic disparities in diabetes agents–related adverse health events have been found in previous studies (Baehr, Pena, & Hu, 2015; Gabriel, Powers, Encinosa, & Bynum, 2017). As the U.S. population continues to age and become more diverse over time, it will be essential to understand racial differences in factors that mitigate or contribute to adverse health events in patients with diabetes.
Furthermore, individuals with diabetes may have limited access to care with a specialist. In the United States, there is a dearth of endocrinologists, and patient demand has outpaced the availability of these specialists (Vigersky et al., 2014). Therefore, most patients with diabetes (85%) turn to primary care physicians for their diabetes care (Vigersky et al., 2014). Consequently, it is important to explore characteristics of practices that promote patient safety. The literature around adverse events among patients with diabetes is predominately focused on events that result in either emergency department (ED) visits or inpatient admissions (Budnitz, Lovegrove, Shehab, & Richards, 2011; Classen, Pestotnik, Evans, Lloyd, & Burke, 1997; Donihi, DiNardo, DeVita, & Korytkowski, 2006; Forster et al., 2004; Kaushal et al., 2001; Lazarou, Pomeranz, & Corey, 1998; Leape et al., 1991; McDonnell & Jacobs, 2002; Nebeker, Hoffman, Weir, Bennett, & Hurdle, 2005; Taché, Sönnichsen, & Ashcroft, 2011). However, less research has been conducted on the prevalence and correlates of adverse events in primary care settings (Gandhi et al., 2000; Gandhi et al., 2003; Gurwitz et al., 2003; Hanlon et al., 1997; Hutchinson, Flegel, Kramer, Leduc, & Kong, 1986; Royal, Smeaton, Avery, Hurwitz, & Sheikh, 2006; Taché et al., 2011), even though most medications are prescribed in the outpatient setting. Given the lack of research on primary care practice characteristics and adverse events, we also explore the relationship between practice characteristics and adverse events in patients with diabetes. More specifically, we study the relationship between (a) whether the patient has been seen before, (b) solo practice, and (c) if the patient identifies the doctor as their primary care provider and the likelihood of an adverse event for patients with diabetes.
Method
Data
Using pooled data from the National Ambulatory Medical Care Survey (NAMCS) conducted by the National Center for Health Statistics (NCHS) from 2011 to 2013, this cross-sectional, observational study explored univariate associations between patient safety for patients with diabetes as measured by adverse events and practice characteristics. The NAMCS is an annual survey composed of probability samples of outpatient visits to non-Federal office-based physician practices in the United States. The data are weighted to represent all ambulatory care visits to physicians across the United States. A thoughtful explanation of NAMCS methodology are available elsewhere (NAMCS, 2017).
Sample
We limited our sample to adult patients (18 years of age and older) with diabetes. To determine patients with diabetes, we considered diabetes to be present when the response box to “Does this patient have diabetes?” was checked on the Patient Record Form. In the NAMCS, the measure for diabetes in 2011-2013 survey years includes both type 1 diabetes mellitus (insulin dependent or IDDM) and type 2 diabetes mellitus (non-insulin dependent or NIDDM). It excludes diabetes insipidus and gestational diabetes. Covariates of interest used to age and race/ethnicity subsamples included sex, race/ethnicity, and age. Age was measured as a continuous variable in years; race/ethnicity was defined as a set of dichotomous indicator variables representing White, Black, or Hispanic race based on NCHS’s imputed race/ethnicity recoded variable (Mafi, 2017). Patients who were “other” based on the race/ethnicity recoded variable were excluded from the analysis due to small sample size. We excluded outpatient surgical practices from the sample. The final sample included 17,587 observations.
Dependent and Independent Variables
The outcome of interest was whether or not the patient’s record indicated an adverse event. Adverse events were based on a variable in the NAMCS indicating if the reason for the visit was related to any of the following: unintentional injury/poisoning; intentional injury/poisoning; injury/poisoning—unknown intent; or adverse effect of medical/surgical care or adverse effect of medicinal drug. The adverse event variable was coded as 1 if any of these reasons were listed and 0 otherwise. The independent variables of interest included measures of health IT and practice characteristics. Health IT measures included whether the practice had electronic prescribing abilities in their practice, 1 if they exchanged health information electronically, 2 and if they had an EHR. 3 Practice characteristics included whether or not the physician was the patient’s primary care provider, 4 whether the physician was a solo practitioner, 5 whether the practice was in a non-MSA area based on the Office of Management and Budget’s definition, and whether the patient had seen that particular physician before. 6
Analysis
We hypothesize that adverse events will differ by practice and patient characteristics as well as by race/ethnicity and age.
We performed difference of means tests to determine if the probability of an adverse event differs by (a) e-prescribing, (b) EHR, (c) ability to exchange health information, (d) solo practitioner, (e) whether the patient has been seen at the practice before, (f) whether the patient lists the provider as their primary care doctor, and (g) whether the practice is located in a non Metropolitan Statistitical Area (MSA). We performed these tests for the full sample, for subsamples by race/ethnicity, for subsamples by age, and for subsamples by race/ethnicity and age.
As previous research on adverse events among patients with diabetes found evidence of racial and ethnic differences in adverse events (Gabriel, Powers, Encinosa, & Bynum, 2017), we performed our analysis on the full sample of adults with diabetes and subsamples by race/ethnicity (Black, White, and Hispanic). Evidence of a relationship between e-prescribing and adverse events for patients with diabetes has been found in the Medicare population. We extend this research by testing whether these relationships persist in younger samples as well by performing the analysis on the full sample, 18- to 64-year-olds, and patients ages 65 years and older. We also explore the relationships between practice characteristics and adverse events by age and race subsamples.
All analyses accounted for the complex survey design using the STATA design variables provided in the NAMCS public-use datasets. STATA was used for all analyses (StataCorp, 2017).
Results
Table 1 presents descriptive statistics of individuals with diabetes (N = 156,344,072 nationally representative, weighted observations). In all, 6% of the sample experienced an adverse event. The average age of individuals with diabetes was 64 years old and more than half were female. Whites accounted for the majority of the sample (68%), while Blacks and Hispanics represented 13% and 14%, respectively. The majority of individuals with diabetes had a physician who electronically prescribed and used EHRs, but an average of 45% of patients had a physician who exchanged health information electronically. Most patients were seen previously in the ambulatory care practice, but only 53% of individuals with diabetes visited their primary care doctor.
Weighted Means for Sample, Adults With Diabetes in the United States (Ages 18 and Older).
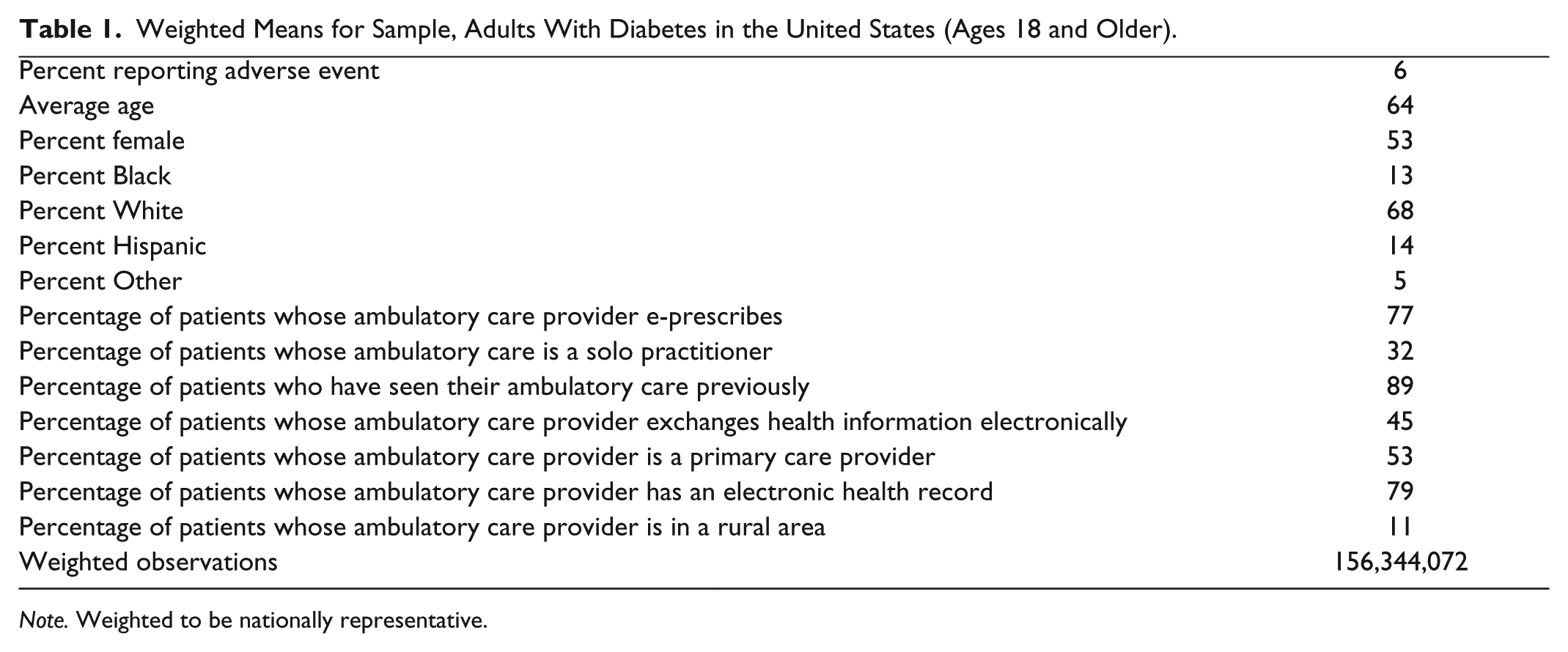
Note. Weighted to be nationally representative.
Table 2 shows the results for the difference of means test for the full sample and by age. These results indicate that e-prescribing was associated with less adverse events for the full sample. Being on insulin, compared with other antidiabetic agents, was associated with a lower risk of adverse event for the 64+ subpopulation. Being an established patient was also associated with less adverse events but was concentrated among the subsample of 18- to 64-year-olds. Finally, seeing a primary care provider was associated with less adverse events, and this relationship was evident for the full sample and both age subsamples.
Means of Adverse Events Occurring in Adults With Diabetes, by Explanatory Variables by Age Categories.

p < .10. **p < .05. ***p < .01.
Table 3 describes adverse events by the independent variables for different racial/ethnic subgroups. Whites who were seen previously in a practice on average had less adverse events (M = 6.2) compared with Whites not seen previously in a practice (M = 9.1). Having a primary care provider was associated with a less adverse events for Whites and Hispanics with diabetes but not for Blacks. Among Hispanics, having a physician who exchanged health information electronically was associated with less adverse events (M = 4.2) compared with Hispanics (M = 9.6).
Means of Adverse Events Among Adults With Diabetes, by Explanatory Variables by Race.

p < .10. **p < .05. ***p < .01.
Table 4 depicts adverse events for patients, aged 18 to 64 years, with diabetes by race/ethnicity. Similar to the results in Table 3, seeing your primary care physician for treatment was associated with fewer adverse events for Whites and Hispanics with diabetes but not for Blacks. The relationship between being seen before and adverse events persisted for Whites. In addition, Hispanics and Blacks age 18 to 64 years with a physician who exchanged health information electronically less adverse events compared to those whose physician’s practices did not. In addition, for non-elderly, adult Hispanics, living in a rural area was associated with fewer adverse events. For the White subpopulation, taking insulin, compared with other antidiabetic agents, was associated with higher rates of adverse events.
Means of Adverse Events by Explanatory Variables by Race, Among Adults With Diabetes, Ages 18 to 64.

p < .10. **p < .05. ***p < .01.
Finally, Table 5 shows adverse events for patients aged 65 years and older with diabetes by race/ethnicity. For these subsamples, e-prescribing was associated with less adverse events for the White and Hispanic subsamples but not the Black subsample. Seeing a patient’s own primary care physician was associated with fewer adverse events for the White and Black subsamples of patients with diabetes aged 65 years and older. For the White subpopulation, taking insulin, compared with other antidiabetic agents, was associated with higher rates of adverse events. Health information exchange was associated with less risk of adverse event for elderly Hispanics.
Means of Adverse Events in Older Adults Aged 65+ Years With Diabetes, by Explanatory Variables by Race.

p < .10. **p < .05. ***p < .01.
Discussion
This study found that the rate of adverse events among adults with diabetes is 6%. This is inclusive of injury, poisoning, or adverse effect of medical/surgical care or adverse effect of medicinal drug. This is comparable with more conservative definitions in the literature. One cohort study found that 0.4% of an older population with diabetes had hypoglycemia that was associated with hospitalization (Majumdar et al., 2013). An ambulatory care–based study focused on adverse events that resulted in hospitalization or an ED visit (Gabriel, Powers, Encinosa, & Bynum, 2017). This study found an adverse event that ranged from 39 to 41 per 1,000 Medicare beneficiaries with diabetes. These studies use a more conservative approach to measure adverse events than this study and tend to focus on the 65 and older population.
This study found significant negative associations between e-prescribing and adverse events. Adverse events were significantly lower for White patients 65 years and older whose physicians e-prescribed compared with those patients whose physician did not e-prescribe. A recent study found that e-prescribing significantly reduced rates of adverse events among patients 65 years and older with diabetes (Powers, 2015). While another study of adverse events in ambulatory care by Gandhi and coauthors (2003) did not find a relationship between e-prescribing and adverse events, they did find that the majority of preventable adverse events were due to prescribing errors and one third could have been avoided using e-prescribing. Interestingly, e-prescribing significantly reduced adverse drug events among older Whites and Hispanics, but not Blacks. The literature is not in agreement. Several studies support this finding (Gabriel, 2017; Powers, 2015), while another found that being Hispanic or Black was associated with a lower likelihood of an adverse event (Bhavsar, Probst, Bennett, Hardin, & Qureshi, 2017).
Our results suggest being an established patient plays an important role in adverse events among adults. To our knowledge, ours is the first study to find evidence of this relationship. Gandhi et al. (2003) did not find a relationship between duration of care and the likelihood of an adverse event. Our study found that, relative to new patients, being seen before was associated with a lower likelihood of adverse events. Other research has found that the majority of ameliorable adverse events in ambulatory care settings were ascribed to unsuccessful communication between doctor and patient (Gandhi et al., 2003). Perhaps being an established patient fosters more effective communication thereby decreasing adverse event risk.
Patients of primary care doctors (vs. non-primary care) have significantly lower numbers of adverse events. Other literature has not demonstrated a reduction in adverse events in primary care settings (Gurwitz et al., 2008; Steele et al., 2005). Patients seeing their primary care physician were less likely to report an adverse event. The relationship was evident for all age groups, Whites, and Hispanics, but not for Blacks. The literature supports the benefit of primary care specialties in terms of hospitalizations. It has been found that ongoing monitoring with a general practitioner does have a protective effect against unforeseen hospitalizations. Unplanned hospital admissions associated with potentially inappropriate medications is decreased in elderly people who have higher levels of general practitioner coverage (Price, Holman, Sanfilippo, & Emery, 2014). This is a positive finding, as the United States is currently experiencing a dearth in endocrinologists, many patients with diabetes are seeking care from primary care physicians (Vigersky et al., 2014). This study, along with others, provides evidence that the use of primary care physicians in the management of diabetes is appropriate.
Overarchingly, solo practitioners, those in non-MSA areas, those with EHRs, and those that exchanged health information electronically did not have significant associations with adverse events. Exchanging information electronically was associated with a lower rate of adverse events for some subsamples of Hispanic and Black patient populations.
This study provides evidence that e-prescribing, seeing a primary care physician, and having an established doctor–patient relationship were all associated with lower numbers of adverse events in patients with diabetes. Given the high incidence of diabetes, it is important to understand what types of interventions can improve health outcomes. Importantly, our study cannot indicate causality. Further research should explore the relationship between these characteristics and adverse events in patients with diabetes using multivariate regressions. However, our study is the first to explore these relationships using a nationally representative sample in the ambulatory care setting.
Conclusion
Reducing adverse events in patients with diabetes is an important health care goal. Given that in the United States there is a dearth of endocrinologists and patient demand has outpaced the availability of these specialists, ambulatory care providers are an increasingly common source of care for patients with diabetes. The relationship between adverse events and health information technology and the relationship between adverse events in patients with diabetes and practice characteristics points toward evidence that e-prescribing, seeing a primary care provider, and being an established patient are associated with less adverse events in adult patients with diabetes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.