
Abstract
The South African health care system, despite recording some significant improvements since independence, still faces a number of health challenges. Mobile technologies application in health care, also known as mHealth, has been shown as feasible in helping alleviate some of South Africa’s disease burden and cause improvements in health care outcomes. Although some feasibility studies have shown the potentials of mHealth, there is a paucity of literature establishing clear outcomes of mHealth interventions in South Africa. This study, therefore, is a systematic review of literature that was carried out to evaluate empirical evidence on the effect of mHealth interventions on health outcomes in South Africa. Academic databases such as PubMed, ScienceDirect, EBSCOhost, and Scopus were searched for empirical studies relating to mHealth interventions in South Africa carried out between 2011 and March 2016. The search, after the screening, yielded 40 papers, of which six randomized controlled studies were eligible for review by the PRISMA guideline. Findings revealed that mHealth interventions using mobile phones and text messages had been targeted at improving treatment adherence and eliciting behavioral actions in patients. However, while mHealth portends the potential to improve health outcomes and possibly transform the health system, there was no sufficient evidence to confirm the effect of the mHealth interventions on improved health outcomes. The study concludes that there is a need for more intervention studies to show evidence of the impact of mHealth interventions on health outcomes and health care delivery processes in South Africa.
Introduction
The health care system of a country is arguably the driver of every other sector, and hence, optimum functionality must be maintained. The health care system in South Africa is reported to have witnessed significant improvements since the end of apartheid in 1994. These improvements have been geared at reducing inequalities in health care access, increased primary health care facilities, enactment of enabling policies and regulatory frameworks, and implementation of priority health programs (Odine, 2015; Rispel, 2016). The World Health Organization (WHO) country profile on South Africa also notes an increase in life expectancy caused by innovative practices, especially the proportional increase in the treatment and care afforded to patients with HIV/AIDs and tuberculosis (TB), and improved access to immunizations (World Health Organization [WHO], 2016). Even with these improvements, the health care system is still beleaguered with a number of challenges. In fact, as noted by Rispel (2016), the national response to the country’s disease burden has not been sufficient, thus, compromising many of the earlier gains and improvements. This is evidenced in health care inequalities and poor health outcomes that abound, as the country is still burdened with diseases such as HIV/AIDs, TB (South Africa contributes about 73% of the burden in the African Region), and high neonatal and maternal mortality ratios (Rispel, 2016; WHO, 2016).
The adoption and application of information and communications technology (ICT) tools have been seen as a sort of silver lining through which health systems in various countries can be improved. Notably, the prevalence and penetration of mobile technologies, especially mobile phones in developing countries, have proven to be a major ingredient needed to improve health care service delivery. According to Gupta (2014), the epidemic of mobile technology is pervading the African region, and it is being used to tackle health problems. Statistics from the International Telecommunications Union (ITU) shows a steady increase in mobile phone subscription in South Africa. Evidently, South Africa has one of the highest mobile phone penetrations in the world, as about 149 per 100 inhabitants are subscribed to a mobile phone network (International Telecommunications Union, 2014). The increasing rate of mobile phone penetration has garnered considerable interest among governments, world bodies such as the United Nations, WHO, and World Bank, and researchers alike regarding its application in improving health care delivery systems. This has led to the term mHealth.
Background
The Global Observatory for e-health of the WHO defined mHealth as the “medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants and other wireless devices” (WHO, 2011). Considering the proliferation of mobile phones even in remote areas, and their affordability and wireless access, they are increasingly seen as the technology of choice for improving health outcomes in developing countries. Studies have reported that mHealth offers opportunities in the areas of strengthening health systems, and causing an improvement in health outcomes and health care service delivery in general (Curioso & Mechael, 2010; Free et al., 2013; Ojo, 2017). Furthermore, to characterize mHealth, Labrique, Vasudevan, Kochi, Fabricant, and Mehl (2013), outlined 12 areas of mHealth applications in their review. These are applications targeted at educating clients and communicating a behavioral change, enhancing decision support, enabling communication between care providers, tracking vital events, collecting and reporting health-related data, and the management of human resources. Other areas of mHealth applications are electronic health records, supply chain management, point-of-care testing for patients, education for care providers, work planning, and financial management.
mHealth in South Africa
The mHealth application landscape in South Africa is also burgeoning. A report by GSMA, a body that represents the interests of mobile operators worldwide, indicates there are 83 existing mHealth services in South Africa, with the majority focusing on HIV/AIDs and women and children (Cargo, 2013). Also, the GSMA mHealth tracker, a web page that curates mHealth products and services all over the world, shows there are 98 mHealth initiatives in South Africa, making it the highest in Africa (GSMA, n.d.). This is further corroborated by Ojo (2017) who notes that about 47% of mHealth applications in Africa are implemented in Southern Africa. Worthy of mention are mHealth applications in the country that have received international acclamations due to their potentials to improve health outcomes. These applications include Cell-Life MAMA SMS (a text messaging solution targeting women who are pregnant and those with babies aged up to 3 months), Project Masiluleke (a specialized text messaging aimed at combating HIV/AIDS), SIMPill (a medication adherence solution), and MomConnect which is a mobile phone application that makes it possible for pregnant women to receive messages based on the stage of their pregnancy to help them improve their health and that of their babies (Akter & Ray, 2010; Cargo, 2013; Curioso & Mechael, 2010; Odine, 2015; Rivett & Tapson, 2009; Seebregts, Tanna, Fogwill, Barron, & Benjamin, 2016; Waldman & Stevens, 2015; WHO, 2013). Also, some feasibility studies have been carried out in the South African context. The use of mobile phones is feasible for clinic reminders and adherence messages (Crankshaw et al., 2010; Georgette et al., 2016; Nachega et al., 2016), cost-effective learning opportunities for health workers (Woods, Attwell, Ross, & Theron, 2012), data collection by health workers (Tomlinson et al., 2009; van Heerden, Norris, Tollman, Richter, & Rotheram-Borus, 2013), monitoring and evaluation by community health workers (Neupane et al., 2014), reliable and sustainable injury severity scoring in a high-volume trauma center (Spence, Zargaran, Hameed, Navsaria, & Nicol, 2016), data for injury surveillance (Zargaran et al., 2014), supporting the malnutrition management of children under the age of 5 (Nyumbeka & Wesson, 2014), cardiovascular screening (Gaziano et al., 2015), and mapping indoor residual spraying (IRS) spray events in relation to malaria cases (Eskenazi et al., 2014). However, studies evaluating the effectiveness of these interventions are limited.
It is evident from the foregoing that mHealth is a potential tool for alleviating some of the health care challenges in South Africa. However, there is a paucity of literature on systematic reviews that have assessed evidence on the extent to which mHealth interventions have generally improved health outcomes in South Africa. In addition, a study describing the state of mHealth implementation in South Africa reports that most initiatives are donor-funded, with no clear evidence of a business model that can ensure sustainability (Botha & Booi, 2016). The authors concluded that there is a need to explore the effectiveness of mHealth strategies in the South African context. This is only expedient, considering that previous similar studies have either focused on a specific technology against a specific disease (Mukund Bahadur & Murrayb, 2010) or now requires to be up to date in the face of the rapid advances in technology (Aranda-Jan, Mohutsiwa-Dibe, & Loukanova, 2014; Betjeman, Soghoian, & Foran, 2013; Free et al., 2013; Krishna, Austin Boren, & Balas, 2009). Therefore, this study aims to fill this gap by attempting to assess via a systematic review of literature, the effectiveness of mHealth interventions in improving health care outcomes in the context of South Africa.
Method
A literature search for peer-reviewed publications was conducted using four databases: PubMed, ScienceDirect, EBSCOhost, and Scopus. Considering the rapid advances in mobile technology, the search was limited to articles published between 2011 and March 2016. A combination of MeSH terms, mHealth and South Africa, was first used as keywords for the search. Second, a combination of free-text words, mobile phone/cell phone and health and South Africa, was also used.
A total number of 395 records were retrieved from the search. Subsequently, the Endnote reference management software (version X7) was used to check for and remove duplicated articles. A manual verification was also carried out. From the search results, all potential articles for full-text review were screened using the titles and abstracts (N = 243). The full text of articles was retrieved and reviewed (N = 40). Also, a systematic search of the reference lists of the full texts was conducted to identify studies that may have been missed. For the selection of articles to be included in the review, the inclusion criteria were studies that were peer-reviewed and utilized a form of randomized control trials (RCTs) or such having a control group that evaluated a mobile health intervention in South Africa. This study focused on articles that have adopted RCTs because RCTs still remain the gold standard in assessing the outcome of medical interventions (Barton, 2000). Studies not entirely carried out in South Africa, without a control group, and without a mobile device intervention, and evaluative or pilot studies were excluded.
Results
After a careful examination taking into consideration the inclusion and exclusion criteria, six studies were found eligible for review. The PRISMA flow diagram as shown in Figure 1 presents the inclusion and exclusion process. The full text of the six studies included for review was retrieved, and information regarding study design, the objective of the study, the mobile technology used, location, intervention, and outcome were extracted. Table 1 shows the characteristics of the included studies.
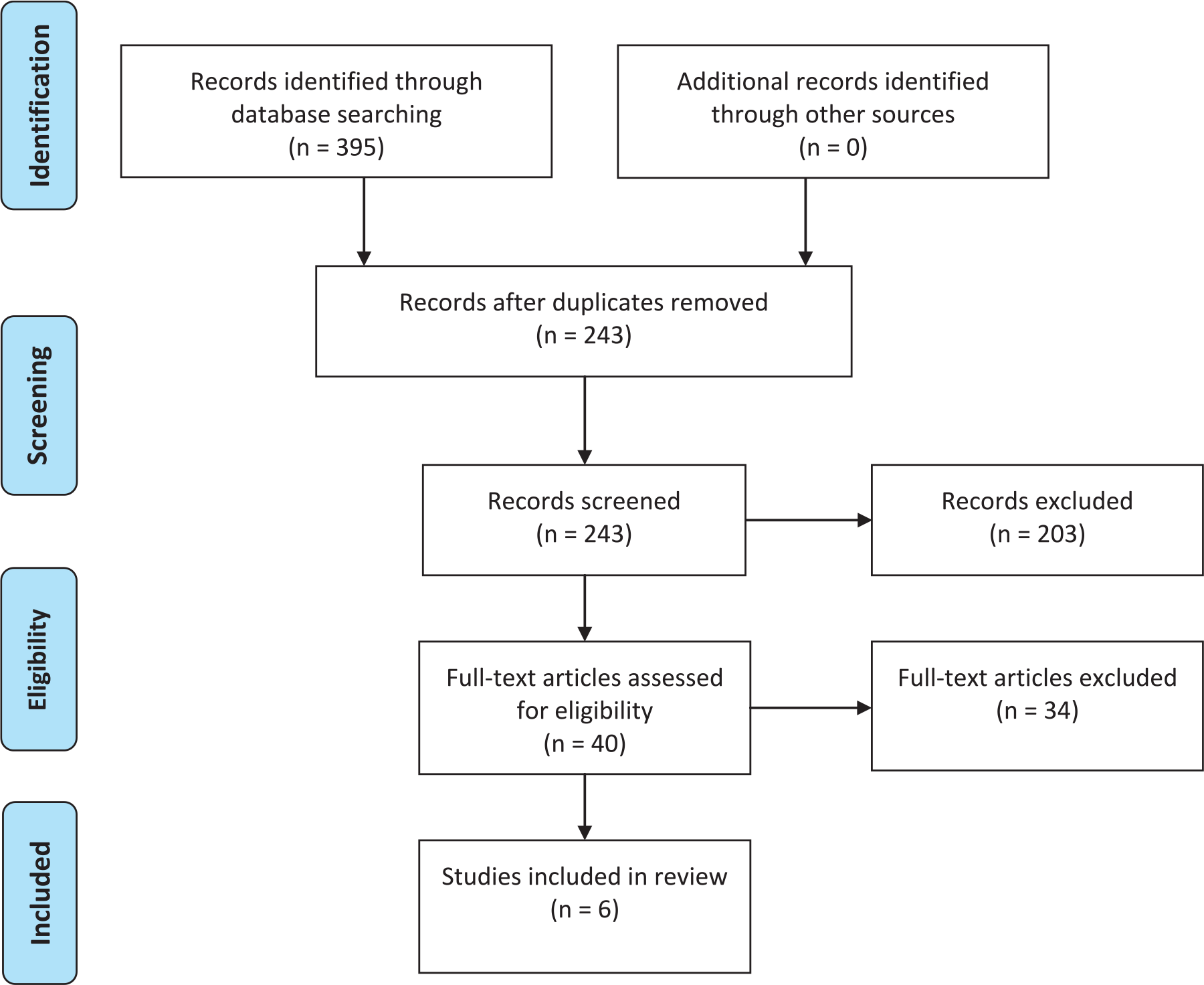
PRISMA flow diagram.
Characteristics of Included Studies.
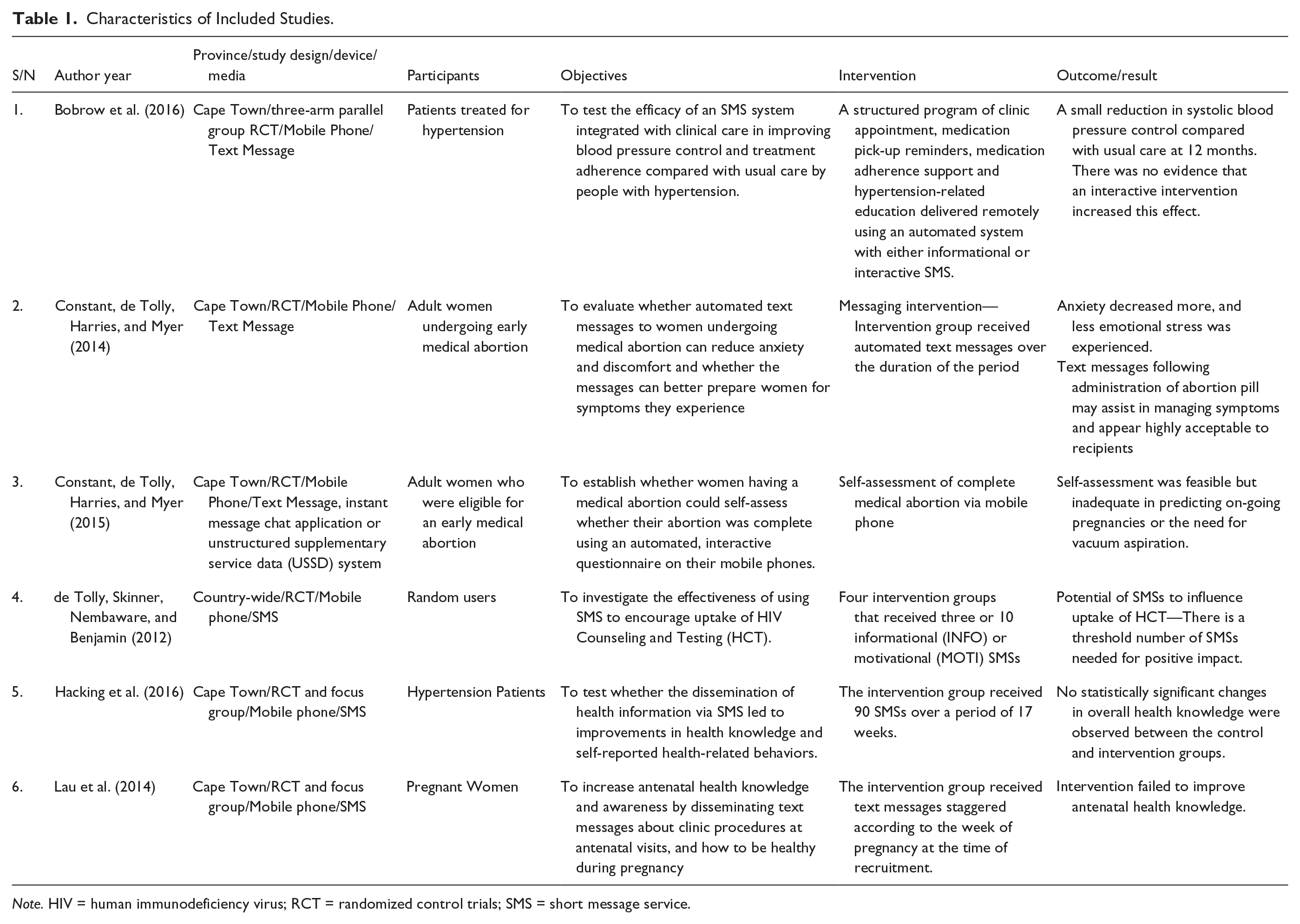
Note. HIV = human immunodeficiency virus; RCT = randomized control trials; SMS = short message service.
Four studies included in the review were solely RCTs, while the other two were mixed studies that utilized RCTs and focus groups. Furthermore, all of the interventions described in the reviewed studies were mobile phone based. While the mobile phone interventions were driven by adopting text messaging platforms in five of the reviewed studies, it was based on the text messaging platform, instant message chat application, and unstructured supplementary service data (USSD) system in one study. Thematically and in line with the categorization of mHealth interventions provided by Labrique et al. (2013), all of the studies under review could generally be characterized as interventions aimed at client education and behavior change communication. This is further discussed in the following.
Treatment Adherence
An RCT assessed the effect of automated treatment adherence support text messages on blood pressure of hypertensive patients (Bobrow et al., 2016). The study had three groups: a usual care control group, a support group whose members received only text messages aimed at motivating them to collect and take their medicines while providing educational contents about hypertension and its treatment, and a group who in addition to the text messages could respond to some messages via a free “please call me” request. The text messages were automatically sent to the patients over a period of 1 year. These text messages were enabled by an open-source web-based medical record system. The message was said to be tied to the patients’ clinic appointments. Their findings revealed that the text message intervention had only small impact on blood pressure of the intervention groups compared with the usual care group—This was in the form of a small reduction in their systolic blood pressure. They concluded that although their text messages could support adherence to hypertension treatment, their study did not provide sufficient evidence to suggest the text message intervention had a significant effect on adherence or blood pressure.
Health Education and Information
A study assessed whether health information disseminated via text messages caused an improvement in the knowledge and behavior of hypertensive patients as related to their state of health (Hacking et al., 2016). The experimental group received 90 text messages spanning 19 weeks. Their study revealed that, overall, there was no statistically significant change in the knowledge of those who received the text messages compared with those who did not. However, those who received text messages had positive increases in self-reported behavior changes. They concluded that text messages were effective in causing positive self-reported behavior change among hypertensive patients.
Similarly, another study sought to assess the effect of text messages relating to antenatal visits, clinical procedures, and maintaining a healthy lifestyle during pregnancy on the knowledge and awareness of pregnant women about antenatal health (Lau et al., 2014). The study included pregnant women in various stages of their pregnancy. The experimental group were sent text messages tailored to their stage of pregnancy as and when recruited into the study. Findings from the study revealed no statistically significant effect of the text messages on the women’s antenatal health knowledge. However, the authors further conducted a focus group discussion with the pregnant women with which they concluded that text messages could encourage health-seeking behavior.
In a similar behavioral intervention RCT involving the use of mobile phones and automated text messages, the authors assessed the effect of automated text messages on reducing anxiety and discomfort among women undergoing medical abortion, and preparing them for the symptoms they would experience (Constant, de Tolly, Harries, & Myer, 2014). They reported that the text message intervention caused a decrease in anxiety in the women, as they also experienced less emotional stress. Thus, they concluded that text messages following the administration of abortion pills might assist in managing symptoms experienced by women undergoing a medical abortion.
The study by Constant, de Tolly, Harries, and Myer (2015) was part of a larger RCT described in the preceding paragraph in which the benefits of sending information via text messages to strengthen and simplify medical abortion was investigated. In the randomized trial, they sought to find out whether women undergoing medical abortion could assess themselves on the completeness of the abortion and whether the assessment was accurate enough in predicting provider’s assessment of the need for follow-up. The device used was the mobile phone owned by the respondents who were women aged 18 years and above, and eligible for medical abortion. The self-assessment was achieved through an instant message application or a USSD system. They concluded that while the mobile self-assessment was feasible, it was not enough to predict a need for follow-up. A finding of interest to this review is the respondents’ preference for USSD over the instant messaging application. It was recommended in the study that combining other technologies such as telemedicine and provision of informational text messages could improve the use of mobile phones for self-assessment in the context of medical abortion.
Also, an RCT investigated the effectiveness of text messages in encouraging HIV counseling and testing (HCT) among participants who were randomly recruited via text messages (de Tolly, Skinner, Nembaware, & Benjamin, 2012). There were four intervention groups and a control group. The four intervention groups received either three or 10 informational or motivational styled text messages accordingly. Findings from the study revealed that while those that received 10 motivational styled text messages were more likely to go for HCT, the interventions when taken together did not have a statistically significant effect on encouraging people to get tested for HIV. They, however, concluded that text messages have the potential to be used as interventions encouraging people to take health-related actions.
Discussion
Six studies that were RCTs were included in this review. The review focused on RCTs rather than pilot projects or feasibility studies to draw clear inferences about the effect of mHealth interventions on health outcomes or health care delivery processes in the South African health system. Of the six studies reviewed, only one (Constant et al., 2014) emphatically reported a significant effect as a result of the mHealth intervention. Others, while not reporting statistically significant effect, only confirmed the feasibility of mHealth interventions. Findings from this study are similar to other reviews that revealed that although mHealth has the potential to improve health outcomes in Africa, the evidence base is not enough to warrant large-scale interventions (Aranda-Jan et al., 2014; Betjeman et al., 2013). It is also pertinent to note that the major mobile technology in use is text messaging or short message service (SMS) made possible by the mobile phone owned by respondents. This result is not unexpected, considering that almost every individual in the country owns a mobile phone and can access their text messages. Studies reviewed focused more on interventions targeted at causing a health action or behavioral change in patients and consumers of health care—specifically adherence support, emotional support, and health behavior. It is also not surprising that majority of the studies under review focused on some of the disease burdens eminent in the country—HIV/AIDS, hypertension, and maternal mortality. Evidently, it also seems researchers are more interested in health outcomes, at the expense of health care delivery process, going by the fact that the studies reviewed focused only on patients, and none focused on health care practitioners.
Limitation
This article is not without some limitations. The study is limited in time and design scope, as it focused only on RCTs and studies published within a 5-year span. Also, the gray literature that may have yielded some valuable publications were not consulted. Oversight on the part of the author in selecting studies for inclusion in this study is also not improbable. However, a more elaborate and collaborative study reviewing the mHealth landscape in the country is underway.
Conclusion
Conclusively, this study does not provide sufficient evidence to affirm mHealth interventions as causing significant improvements in health outcomes or health care processes in South Africa. No doubt, many mHealth projects are going on and being implemented in the country. However, these projects are likely to remain pilot projects that continue to confirm the potential of mobile technologies in health care but with unclear evidence of outcomes and benefits. There is a need for more intervention studies to ascertain the effect of mHealth interventions on health outcomes and health care delivery processes.
Footnotes
Acknowledgements
I would like to acknowledge the contribution of the Southern African Systems Analysis Center, the National Research Foundation, and the Department of Science and Technology in South Africa, as well as the International Institute of Applied Systems Analysis in Austria.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.