
Abstract
Assessing feigning psychosis is extremely important in forensic psychological assessment. This pilot study investigated the utility of three multiscale personality inventories, namely, the Chinese Minnesota Multiphasic Personality Inventory (MMPI-2), the Ko Mental Health Questionnaire (KMHQ), and the Health-Personality-Habit Inventory (HPH), in the detection of feigning psychosis in Taiwan. It was hypothesized that the above three inventories were effective in the detection of feigning psychosis. The sample consisted of 70 participants (students and community members; with 19 men and 51 women), with mean age of 22.01 years (SD = 3.86), who were randomly assigned to two different groups: feigning psychosis and honestly responding. The KMHQ, the HPH, and the Chinese MMPI-2 were administered to each participant in this sequential order. Altogether 16 scales from these inventories were statistically analyzed using MANOVA, t test, Receiver Operating Characteristic (ROC) analysis, and discriminant analysis. Of these 16 scales, the scores of 14 scales differed significantly between the feigning psychosis and honestly responding groups. In addition to the exploration of the best discriminant variables, the effect size, best cutoff score, classification accuracy rate, sensitivity, and specificity of the scales of the above three inventories in discriminating participants between feigning psychosis and honestly responding were presented, respectively. The results of this study supported the utility of the Chinese MMPI-2, the KMHQ, and the HPH in the detection of feigning psychosis.
Introduction
In forensic psychiatric/psychological assessment, examinees may feign psychosis to escape culpability. Feigning psychosis is one of the main manifestations of malingering. According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013), malingering is defined as “the intentional production of false or grossly exaggerated physical or psychological symptoms, motivated by external incentives such as avoiding military duty, avoiding work, obtaining financial compensation, evading criminal prosecution, or obtaining drugs” (APA, 2013, p. 726). Malingering is different from factitious disorder in that the motivation for the former has an external incentive whereas for the latter external incentives are absent (APA, 2013). However, the distinction between malingering and factitious disorder is usually difficult and problematic in clinical work (Rogers, 2008b; Rogers, Bagby, & Vincent, 1994). Regardless of the differentiation of these, the first most important step is to detect feigning, which means “the deliberate fabrication or gross exaggeration of psychological or physical symptoms without any assumptions about its goals” (Rogers, 2008b, p. 6). As it is often difficult to determine individuals’ underlying motivations, psychological tests can be used to establish feigning, but not malingering (Rogers, 2008b).
Feigning is not rare. Surveys concerning forensic and nonforensic referrals yielded mean percentages of approximately 15% to 17%, respectively, and about 7% for feigning (Rogers, 2008b). In a study on the feigning of neuropsychological symptoms, 17% of criminal cases, 13% of personal injury cases, 13% of disability or workers compensation cases, and 4% of medical or psychiatric cases were found to have either symptom exaggeration or probable symptom exaggeration (Sullivan, Lange, & Dawes, 2005). Feigning has also been recognized in the military context (Malone & Lange, 2007). For instance, Chiang et al. (2006) found that in a draftee sample for psychiatric reevaluation, 9.1% were suspected to be feigners.
The phenomenon of feigning may create a range of serious problems. First, clinicians are trained with scientific knowledge and methods to find the psychiatric truth. Obviously, clinicians have not done their job well if they are fooled by their clients. Second, medical resources may be wasted on unwarranted care with clients with feigned illness. Third, when the reports of the assessment of clients’ conditions are used in judicial procedures, justice may be hindered if sentencing is based on incorrect evidence. Acceptance of incorrect evidence may affect individuals’ social standing, their property holdings, or even issues of life and death.
However, the detection of feigning is not easy. Both lay people and professionals are typically not very good at detecting lies (Vrij, 2008). Although there are individual differences in judging deception, few people can be identified as experts in deception detection (C. F. Bond & DePaulo, 2008; G. D. Bond, 2008). Scientific investigation on the detection of deception has pointed toward verbal and nonverbal behaviors that may be helpful cues in detecting deception. Yet, despite many years of research, the accuracy of all these suggestions is not high due to the enormous variation of human behavior while lying or telling the truth, both at the intrapersonal and interpersonal levels (Boyd, McLearen, Meyer, & Denney, 2007; Bradford & Goodman-Delahunty, 2008; Resnick, 2007; Sporer & Schwandt, 2007; Vrij, 2008). Some researchers focus on the physiological responses of liars and polygraph methods have been proposed for detecting deception. However, as is well known, generally speaking, the opinions of researchers on the accuracy of the polygraph fall on the negative side. In fact, the National Research Council of the United States National Academy of Sciences found that the validity of the polygraph has not been scientifically supported (Boyd et al., 2007; Iacono & Patrick, 2008; Vrij, 2008; Weiner & Hess, 2006; Wrightsman & Fulero, 2005).
On the contrary, the clinical assessment of response styles has made progress. Methods for the detection of feigning have evolved from case studies and group differences to detection strategies (Rogers & Correa, 2008). The Infrequency (F), Lie (L), and Correction (K) scales of the Minnesota Multiphasic Personality Inventory (MMPI) were regarded as the beginning of the assessment of response styles both systematically and empirically (Rogers, 2008a). There are four basic distinct response styles in clients within the psychiatric setting: reliable response style, irrelevant response style, defensiveness, and malingering (Rogers, Bagby, & Dickens, 1992). At present, the most commonly used multiscale personality inventories in clinical or forensic settings in the United States are the MMPI-2, the Personality Assessment Inventory (PAI), and the Millon Clinical Multiaxial Inventory–III (MCMI-III), and significant research has been devoted to assessing the validity of these measures for detecting specific response styles (Boyd et al., 2007; Greene, 2008; Sellbom & Bagby, 2008). With respect to the MMPI-2, some scales, such as the Infrequency Scale (F), the Back Infrequency Scale (Fb), the Infrequency-Psychopathology Scale (Fp), the Gough’s Dissimulation Index (F-K), and the Gough’s Dissimulation Scale (Ds), have been shown to be useful in detecting feigning (Gough, 1950, 1954; Greene, 2008; Meyers, Millis, & Volkert, 2002; Rogers, Sewell, Martin, & Vitacco, 2003). These are either validity scales or scales constructed for detecting feigning. According to the review by Rogers et al. (2003), the strategies used for the detection of feigned mental disorders in the MMPI-2 include the following: rare symptoms, symptom severity, comparison of obvious and subtle symptoms, and erroneous stereotypes. For example, the scales F, Fb, Fp, and F-K use the detection strategy of rare symptoms, while the scale Ds belongs to the strategy of erroneous stereotypes.
Despite the presence of various basic research designs in studying response styles, most research on feigning mental disorders relies on simulation designs using analog research method, in which nonclinical participants are randomly assigned to different experimental conditions (Rogers, 2008c). Then the experimental group is compared with the control group (i.e., honest or standard conditions). The strength of simulation designs is strong internal validity (Rogers, 2008b). In addition, coaching is considered to be an important variable in this kind of research (Bagby, Nicholson, Bacchiochi, Ryder, & Bury, 2002; Rogers, 2008c; Storm & Graham, 2000), as the assumption that the examinees in the forensic psychological assessment are uninformed of the purpose and method of testing is untenable (Rogers, Bagby, & Chakraborty, 1993). There are two kinds of coaching: symptom/disorder-based coaching and detection-based coaching (Rogers, 2008c). Research showed that the factors assisting feigners who succeeded to avoid detection on the MMPI-2 were greater intelligence, prior knowledge of the condition feigned, and prior information of the MMPI-2 (Pelfrey, 2004; Walters & Clopton, 2000). Moreover, Wetter and Corrigan (1995) reported that 50% of attorneys felt obliged to inform their clients about the MMPI-2. On the contrary, the effect of incentives on simulators is another issue in research on feigning mental disorders, and it appears that the desire for the award increases the motivation to feign (Rogers, 2008c). Some researchers attempted to provide higher incentives but made them available to only the top few performers in the simulating group (e.g., Bagby et al., 2002; Elhai et al., 2007).
The MMPI-2 has been translated into Chinese and published by the Chinese University of Hong Kong (Cheung, Zhang, & Song, 2003). Nevertheless, the Ko Mental Health Questionnaire (KMHQ) and the Health-Personality-Habit Inventory (HPH) are the two most frequently used multiscale personality inventories in clinical settings in Taiwan. They have also been used in forensic psychiatric/psychological assessment ordered by courts. However, there has been no research on the utility of the KMHQ or the HPH with respect to the detection of feigning psychosis.
Taken together, this pilot study investigated the utility of the Chinese MMPI-2, the KMHQ, and the HPH in the detection of feigning psychosis. The following hypotheses were made.
In addition, the effect size, best cutoff score, classification accuracy rate, sensitivity, and specificity of the scales of the above three inventories in discriminating participants between feigning psychosis and honestly responding were investigated, respectively. Furthermore, for each of these multiscale personality inventories, the best discriminative variables were also explored. This information is extremely important and useful for clinicians conducting forensic psychological assessment.
Method
Participants
The participants were recruited through advertisements posted on campus notice boards and the webpage of a university in northern Taiwan for 2 months. The inclusion criteria for participants were (a) at least 17 years old, (b) no history of psychiatric illness, and (c) not studying psychology or psychology-related courses. In total, 70 participants (19 men and 51 women) responded voluntarily to the advertisements and they all satisfied the inclusion criteria of the study. Their mean age was 22.01 years (SD = 3.86), ranging from 17 to 47 years old. The mean education level of the participants was 14.70 years (SD = 1.68), ranging from 12 to 19 years. With regard to occupation, 64 of the participants were students. In addition to the university’s institutional review board’s (IRB) approval of this research project and the signing of informed consent forms by all participants, the Declaration of Helsinki was strictly followed in the protection of participants’ rights.
Measures
MMPI-2
The MMPI-2 was first published in 1989 (Butcher, Dahlstrom, Graham, Tellegen, & Kaemmer, 1989). It is a self-report questionnaire comprising 567 items which can be answered “True” or “False,” and has seven validity scales. The MMPI-2 was standardized on an adult norm. There has already been accumulated a large amount of research on the reliability and validity of the MMPI-2 which supports its utilization (Butcher et al., 2001; Groth-Marnat, 2009). The Chinese MMPI-2 was first published in 2003 (Cheung, Zhang, & Song, 2003). Two norms have been reported: China norms and Hong Kong norms. Generally speaking, the psychometric properties of the Chinese MMPI-2 are similar to that of the English version (Cheung et al., 2003). Previous research indicated that Chinese respondents endorsed much more items of the MMPI F scale than American respondents, and thus a new Chinese Infrequency scale (ICH) was developed for the Chinese MMPI (Cheung, Song, & Butcher, 1991). This scale has also been used in the Chinese MMPI-2. As mentioned above, the scales F, Fb, Fp, F-K, and Ds have been shown to be useful in detecting feigning. In addition, as the ICH is the specific Infrequency scale for Chinese MMPI-2 respondents, the scales Fb, Fp, F-K, Ds, and ICH were used for statistical analysis in this study. The scales Fb, Fp, and ICH are in the standard scoring system of the Chinese MMPI-2 (Cheung et al., 2003) and consist of 40, 27, and 15 items, respectively. Gough (1950, 1954) constructed the Gough Dissimulation Index (F-K), which is the raw score difference between the F and K scales, and the Gough Dissimulation Scale (Ds), which has 58 items in the MMPI-2. The raw scores of these scales were used for computation.
KMHQ
The KMHQ is a Chinese multiscale personality inventory for assessing psychopathology and has been used in Taiwan for many years. The purpose of constructing this measure was to have an indigenous test similar to the MMPI. The items were empirically derived without adhering to any particular personality theory or psychiatric diagnostic system (Ko, 1998). The KMHQ’s first edition appeared in 1964 (Ko, 1964), and was revised in 1974 (Ko, 1977) and 1991 (Ko et al., 1992), respectively. The latest version was published in 1998 (Ko, 1998) and consisted of 300 items. Each item is responded to using 6-point rating scale, ranging from totally untrue to totally true. The KMHQ has 38 scales, in which six of them are validity scales, namely, Reliable Responding (S1): the degree which the respondent claims to respond honestly; Unreliable Responding (S2): the degree which the respondent claims to respond dishonestly; Maintaining Good Image (S3): looking good; Inconsistency (S4): discrepancy in responding to identical items; Opposite Response Consistency (S5): responding to items with similar meaning in a similar way; and Infrequency (S6): endorsing items that describe infrequent or odd behavior. There are three kinds of norms: junior-high students, senior-high students, and university students/adults, with each further classified into male and female norms. According to the manual of the KMHQ (Ko, 1998), most of the 38 scales (except three) had reliability coefficients (Cronbach’s αs) that ranged from .5 to .97. The author of the KMHQ explained that the low reliability coefficients of some scales were due to few items in each of these scales (Ko, 1998). The test–retest reliability coefficients (30-40 days) for most of the scales were above .6. The validity of the 1998 version of the KMHQ was investigated via differences between males and females, comparison of healthy versus unhealthy groups, and factor analysis. All these analyses supported the construct validity of the measure (Ko, 1998). Lin and Huang (1998) studied the validity of the KMHQ by using meta-analysis on 11 scales of the measure. The analysis comprised the data of 52 studies. They concluded that the extent of the KMHQ’s validity generalization was high and its discriminating capacity among the various mental disorders was good. The 1998 version of the KMHQ was used in the current study. As there has been no previous research on the utility of the validity scales of the KMHQ in the detection of feigning psychosis, the statistical analysis of this study focused on the six validity scales and the raw scores of these scales were used for computation.
HPH
The HPH is a Chinese multiscale personality inventory for assessing psychological health and personality characteristics in Taiwan. The HPH was first published in 1995 (Ko, 1995) and slightly revised in 1999 (Ko & Chang, 1999) and 2003 (Ko & Chang, 2003), respectively. The items were derived according to the clinical experience of the authors of the HPH and in reference to the diagnostic criteria of mental disorders described in the DSM system (Ko & Chang, 2003). The purpose of the HPH varies conceptually from the KMHQ. The items of the HPH are different from that of the KMHQ. In the HPH, there are 256 items in total. There are 27 clinical scales and five validity scales. The validity scales are labeled as Self-Rated Mentally Healthy (D5): I feel psychologically well; Self-Rated Mentally Unhealthy (D6): I feel psychologically poor; Self-Rated Reliable Responding (D7): I am responding honestly; Self-Rated Unreliable Responding (D8): I am responding dishonestly; and Infrequency (D9): I have uncommon behaviors different from the normal population. The response of each item is scored on a 6-point rating scale, ranging from totally untrue to totally true. There are five kinds of norms: junior-high students, senior-high students, junior college students, university students, and adults, with each further classified into male and female norms. According to the manual of the HPH (Ko & Chang, 2003), most of the scales had reliability coefficients (Cronbach’s αs) above .6. The measure possessed good stability (1-month test–retest). The validity of the 2003 version of the HPH was investigated via content analysis, differences between males and females, comparison of clinical versus normal groups, factor analysis, and correlations between the HPH with the KMHQ, the Edwards Personal Preference Schedule (EPPS), and the Interpersonal Behavior Survey (IBS). All these analyses supported the construct validity of this measure (Ko & Chang, 2003). The clinical validity of the HPH was further investigated on a sample of patients diagnosed with schizophrenia, bipolar I disorder, major depressive disorder, and anxiety disorders, respectively (Liu et al., 2015). The results found that the HPH displayed satisfactory discriminative power among the various mental disorders. The latest 2003 version was used in the current study. As there has been no previous research on the utility of the validity scales of the HPH in the detection of feigning psychosis, the statistical analysis of this study focused on the five validity scales and the Z scores of these scales were used for computation.
Procedure
When each participant arrived at the testing room, a coin was tossed to decide which of the two groups, feigning psychosis or honestly responding, to which the participants were assigned. In total, 40 participants (seven males and 33 females) belonged to the feigning psychosis group and 30 participants (12 males and 18 females) to the honestly responding group. The participants in the feigning psychosis group were coached by reading a two-page description of schizophrenic symptoms. To ensure that the participants understood and remembered the instructed symptoms, a 10-item quiz was administered; correctly responding on eight or more items was considered as satisfying the manipulation check requirements. The coaching procedure was repeated if the eight correct responses were not achieved. All the participants in the feigning psychosis group passed the manipulation check. The participants in the feigning psychosis group were instructed to imagine that they had killed someone and were eager to escape culpability by feigning psychosis. To enhance their motivation of feigning, they were told that the two best feigners would receive a monetary reward. The participants in the honestly responding group were asked to respond honestly according to their present feelings and thinking. Three multiscale personality inventories, that is, the KMHQ, the HPH, and the Chinese MMPI-2, were administered to each participant in this sequence. The participants completed the testing in two separate sessions on different days.
Statistical Analysis
Statistical analysis was implemented by using SPSS version 20 computer software. To examine the differences of the scores of the scales of the three inventories, respectively, between the two participant groups, MANOVA, t test, and Cohen’s d were computed. Receiver operating characteristic (ROC) analysis and discriminant analysis were also conducted to evaluate the accuracy of the scales of each inventory in differentiating feigning psychosis and honestly responding.
Results
To compare the means of the scores on the scales Fb, Fp, F-K, Ds, and ICH of the MMPI-2 of the feigning psychosis and honestly responding groups, MANOVA was first conducted. The Hotelling’s trace was 8.79, F(5, 64) = 112.47, p < .001. Accordingly, one-tailed t test was used on each of the scales. The means, standard deviations, t tests, and Cohen’s d of each of the scores of the scales of the Chinese MMPI-2 of the two participant groups are shown in Table 1. Similar procedures in statistical analysis were implemented for the validity scales of the KMHQ and the HPH. For MANOVA, the Hotelling’s trace for the KMHQ and the HPH were 1.73, F(6, 63) = 18.20, p < .001, and 1.62, F(5, 64) = 20.74, p < .001, respectively. The means, standard deviations, t tests, and Cohen’s d of each of the scores of the scales of the KMHQ and the HPH of the two participant groups are shown in Tables 2 and 3.
Results of t Test of Chinese MMPI-2 Scales.

Note. The scores are raw scores. MMPI-2 = Minnesota Multiphasic Personality Inventory–2; Fb = Back Infrequency; Fp = Infrequency-Psychopathology; F-K = Gough’s Dissimulation Index; Ds = Gough’s Dissimulation Scale; ICH = Chinese Infrequency Scale.
p < .001, one-tailed.
Results of t Test of KMHQ Validity Scales.

Note. The scores are raw scores. KMHQ = Ko Mental Health Questionnaire; S1 = Reliable Responding; S2 = Unreliable Responding; S3 = Maintaining Good Image; S4 = Inconsistency; S5 = Opposite Response Consistency; S6 = Infrequency.
p < .01. ***p < .001, one-tailed.
Results of t Test of HPH Validity Scales.

Note. The scores are Z scores. HPH = Health-Personality-Habit Inventory; D5 = Self-Rated Mentally Healthy; D6 = Self-Rated Mentally Unhealthy; D7 = Self-Rated Reliable Responding; D8 = Self-Rated Unreliable Responding; D9 = Infrequency.
p < .01. ***p < .001, one-tailed.
The utility of the scales with significant t-test results of each inventory in the detection of feigning psychosis was examined with ROC analysis. The results, including the area under curve (AUC), best cutoff scores, the percentages of the participants correctly classified, sensitivity, and specificity, are shown in Tables 4 to 6. In addition, discriminant analysis, with stepwise procedure, was conducted to explore the best discriminant variables of each of these inventories, respectively. For the Chinese MMPI-2, the Wilks’s lambda was .110, F(2, 67) = 272.33, p < .001. The best predictors were Fp and Fb, while the classification accuracy rate was 97.1%. For the KMHQ and HPH, the Wilks’s lambdas were .379, F(2, 67) = 54.93, p < .001, and .384, F(2, 67) = 53.70, p < .001, respectively. The best predictors were Infrequency (S6) and Inconsistency (S4) for the KMHQ, with a classification accuracy rate of 90.0%. With regard to the HPH, the best predictors were Infrequency (D9) and Self-Rated Mentally Unhealthy (D6), while the classification accuracy rate was 91.4%.
Results of ROC Analysis of Chinese MMPI-2 Scales.

Note. The best cutoff is raw score. ROC = Receiver Operating Characteristic; MMPI-2 = Minnesota Multiphasic Personality Inventory–2; AUC = area under curve; CI = confidence interval; Fb = Back Infrequency; Fp = Infrequency-Psychopathology; F-K = Gough’s Dissimulation Index; Ds = Gough’s Dissimulation Scale; ICH = Chinese Infrequency Scale.
Results of ROC Analysis of KMHQ Validity Scales.

Note. The best cutoff is raw score. ROC = receiver operating characteristic; KMHQ = Ko Mental Health Questionnaire; AUC = area under curve; CI = confidence interval; S2 = Unreliable Responding; S3 = Maintaining Good Image; S4 = Inconsistency; S6 = Infrequency.
Results of ROC Analysis of HPH Validity Scales.
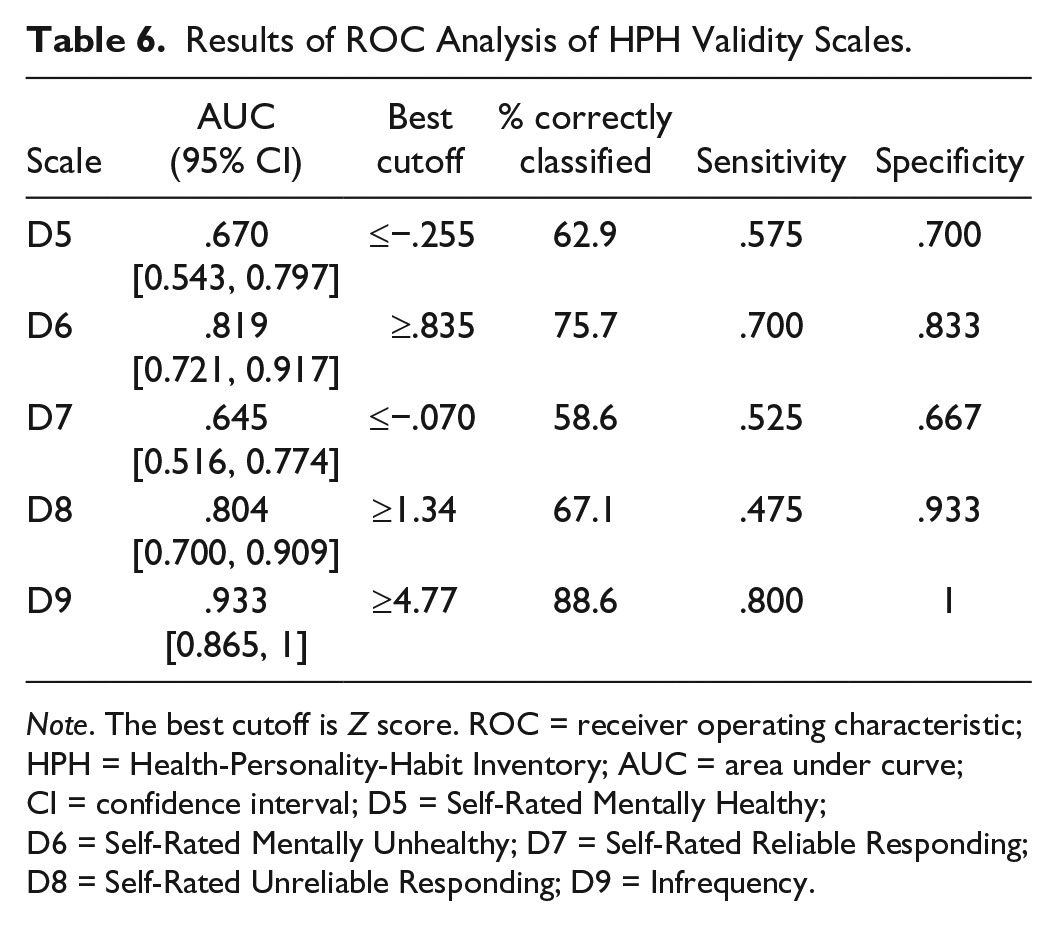
Note. The best cutoff is Z score. ROC = receiver operating characteristic; HPH = Health-Personality-Habit Inventory; AUC = area under curve; CI = confidence interval; D5 = Self-Rated Mentally Healthy; D6 = Self-Rated Mentally Unhealthy; D7 = Self-Rated Reliable Responding; D8 = Self-Rated Unreliable Responding; D9 = Infrequency.
Discussion
The results of this study supported the hypotheses that the three multiscale personality inventories, namely, the Chinese MMPI-2, the KMHQ, and the HPH, possessed effectiveness in the detection of feigning psychosis. In fact, of the 16 detection scales analyzed in the current study, only two had nonsignificant t-test results in comparing the means between the feigning psychosis and honestly responding groups.
As this study appeared to be the first in investigating the utility of the Chinese MMPI-2 in the detection of feigning psychosis, it may be informative to compare the results of this study with those using the English MMPI-2. To adhere to academic strictness and simplicity, meta-analyses of the MMPI-2 in the detection of feigned mental disorders were reviewed (Nelson, Hoelzle, Sweet, Arbisi, & Demakis, 2010; Nelson, Sweet, & Demakis, 2006; Rogers et al., 2003). Rogers et al. (2003) reported effect sizes for simulators versus nonclinical controls and the mean cutoff scores of various detection scales in the meta-analysis. Compared with the results of Rogers et al. (2003), the effect sizes and classification rates of the scales Fb, Fp, F-K, and Ds were higher in the present study using the Chinese MMPI-2, as shown in Table 7. However, these comparisons were made between a large sample (2,514 participants in the meta-analysis) and a small sample (70 participants in the current study). The differences in the statistical sample representation of the two samples might lead to the above differences in the effect sizes and classification rates of the Chinese versus English MMPI-2. One other possibility might be the effects of coaching the feigning psychosis group, which in turn enhanced the differences between the feigning psychosis and honestly responding groups. With regard to cutoff scores, all of them except for Ds were also higher in the Chinese MMPI-2 than those of the English MMPI-2. Previous studies have indicated that test takers in the Chinese society generally seemed to have higher MMPI-2 scores than those in the Western societies (Cheung et al., 1991). This implies that cultural differences would be one of the reasons for having higher cutoff scores for the Chinese MMPI-2 compared with the English MMPI-2. In other words, if clinicians conduct psychological assessment and use measures which are translated from other languages to Chinese, they should be familiar with research on cultural differences and do not interpret the scores of the measures only according to the studies in other cultures.
Effect Sizes, Cutoff Scores, and Classification Rates of Scales of the English and Chinese MMPI-2, Respectively, in Feigning Psychosis Detection.
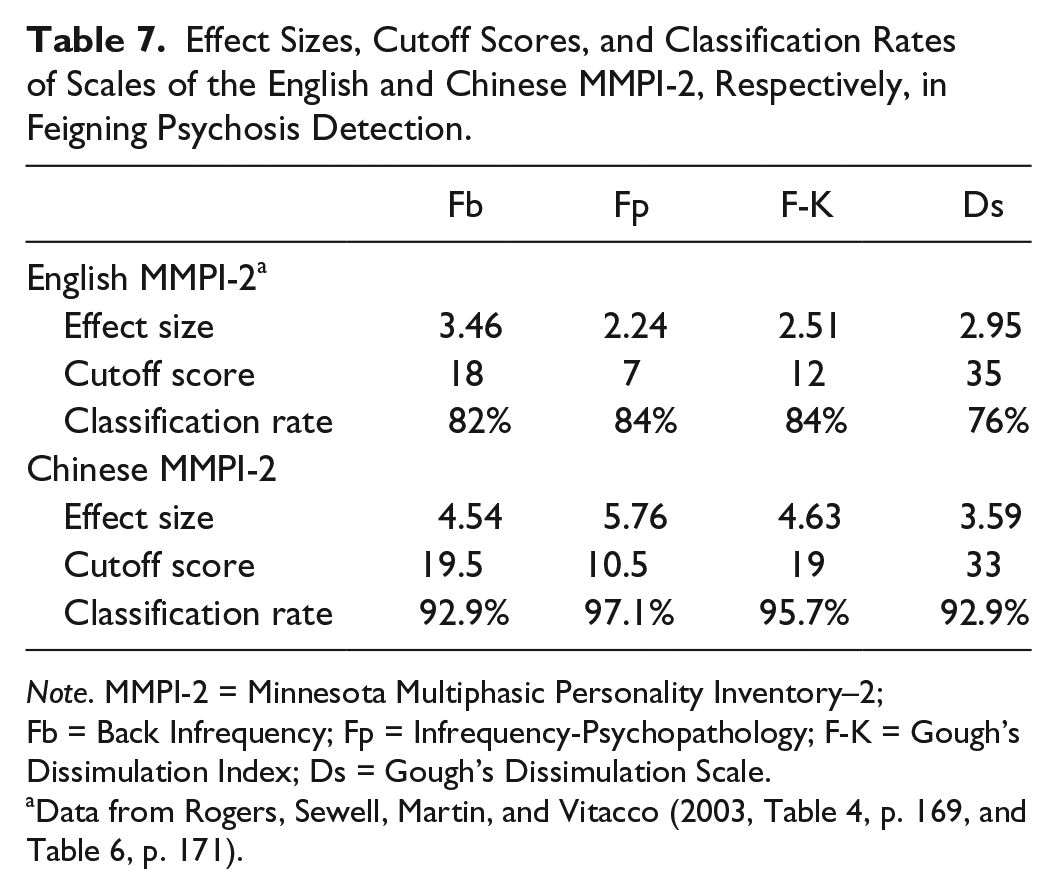
Note. MMPI-2 = Minnesota Multiphasic Personality Inventory–2; Fb = Back Infrequency; Fp = Infrequency-Psychopathology; F-K = Gough’s Dissimulation Index; Ds = Gough’s Dissimulation Scale.
Data from Rogers, Sewell, Martin, and Vitacco (2003, Table 4, p. 169, and Table 6, p. 171).
Another finding of this study was that, among the five scales of the Chinese MMPI-2 in the statistical analysis, the scales Fp and Fb appeared to be the best predictors in discriminating feigning psychosis from honestly responding. However, ICH was a new scale created especially for the Chinese MMPI and has also been used in the Chinese MMPI-2 (Cheung et al., 1991). This pilot study seemed to be the first research to investigate its utility in the detection of feigning psychosis. Results showed that, in addition to its high correlation with the Fb, Fp, D-K, and Ds scales (r = .925 ~ .970, p < .001), ICH possessed compatible discriminating ability, in terms of effect size and classification accuracy rate, with all these well-validated indices of the English MMPI-2. This implies that ICH is a valid scale for validity checking. Therefore, in addition to the scales of the MMPI-2 which have already been examined thoroughly in the detection of feigning psychosis, it is recommended that the utility of ICH of the Chinese MMPI-2 should also be carefully investigated in future research.
Despite that this is the first pilot study on the utility of the KMHQ and the HPH in the detection of feigning psychosis, the results of this study seemed to be very encouraging. For the KMHQ, the scales Infrequency (S6) and Inconsistency (S4) appeared to be the best predictors in discriminating feigning psychosis from honestly responding, using discriminant analysis. Moreover, the validity scale Maintaining Good Image (S3) also possessed good accuracy with regard to effect size and classification rate. For the HPH, the validity scales Infrequency (D9) and Self-Rated Mentally Unhealthy (D6) were good discriminant variables in discriminating feigning psychosis from honestly responding. However, besides relying on the validity scales of the KMHQ and the HPH for the detection of feigning psychosis, specific detection scales, such as Ds of the MMPI-2, should be developed in the future. Moreover, for the MMPI-2, detection models, which consisted of algorithms integrating individual indices, have been advocated to increase the accuracy of detecting feigned mental disorders (Meyers et al., 2002; Rosenfeld, Green, Pivovarova, & Dole, 2010; Steffan, Morgan, Lee, & Sellbom, 2010). The development of the detection models of the KMHQ and the HPH might be another future research direction.
From a clinical point of view, in this study on the detection of feigning psychosis, the scale with the largest effect size, classification accuracy rate, sensitivity, and specificity for the Chinese MMPI-2 was the Chinese Infrequency scale (ICH). Similarly, for the KMHQ, the scale with the greatest accuracy was the Infrequency scale (S6); for the HPH, it was also the Infrequency scale (D9). All these three scales use the detection strategy of rare symptoms. According to research, this rare-symptom strategy is the main technique for assessing feigned psychosis and has been shown to be a robust method (Rogers, 2008a; Rogers et al., 2003). Future research on the Chinese MMPI-2, the KMHQ, and the HPH may focus on the effectiveness of other detection strategies such as symptom severity, comparison of obvious and subtle symptoms, and erroneous stereotypes.
There were several limitations in this study. First, the sample size was small (N = 70). Second, the participants had generally high education levels (M = 14.7 years). Third, the comparison group consisted of healthy participants, instead of psychiatric patients, without psychopathology. Fourth, this was a simulation design study which lacked ecological validity. Fifth, the participants were not randomly selected from a base. Sixth, the incentives given to the simulators might be an issue of confounding variable. As a result, it should be cautious in the generalization of the results of this study to other populations and much further research is needed.
In conclusion, the results of this study supported the utility of the Chinese MMPI-2, the KMHQ, and the HPH in the detection of feigning psychosis in Taiwan. In addition, the scales which are particularly useful in the detection were also indicated for further study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.