
Abstract
The current study examined the impact of active duty service members’ symptoms following a combat deployment on child mental health symptoms. Soldiers from a brigade combat team (N = 974) participated in the study 2 months following return from a 15-month combat deployment to Afghanistan, of which 169 soldiers (17.3%) reported having at least one child living at home. Results supported two research hypotheses examining the interrelationship between parental posttraumatic stress disorder (PTSD) symptoms, general aggression, and marital distress on child mental health. First, the study documented a moderate association between parental PTSD symptoms and child mental health symptoms during the postdeployment reintegration period. This association was significant even after accounting for marital distress. Second, the study demonstrated that the impact of PTSD symptoms on child mental health symptoms may be explained by parental general aggression such that aggression mediated the PTSD symptoms–child mental health association.
Keywords
Deployment separation is one of the greatest demands of the military lifestyle on military families as it includes the risk of injury or death of the service member, as well as additional responsibilities for the at-home spouse who must adjust to the role of a single parent (Wright, Riviere, Merrill, & Cabrera, 2013). Aside from Vietnam, Operation Enduring Freedom (OEF) in Afghanistan has been the longest war the U.S. military has fought to date, and Operation Iraqi Freedom (OIF) the third longest (Hosek, 2011). More than 2.1 million service members have deployed in support of these missions. Approximately 100,000 (44%) of these service members are parents, with 48% of these deployed parents having deployed more than once (Department of Defense, 2010). In this time, nearly 2 million children experienced a parent’s absence due to deployment (Flake, Davis, Johnson, & Middleton, 2009).
Studies conducted with military families indicate that the psychological effects of a service member’s deployment extend to their children. For example, the Survey of Army Families (Orthner & Rose, 2005) reported that approximately 25% of school-age children were depressed because of deployment separation and 37% reported fear of harm to the deployed parent. Further evidence comes from a retrospective cohort study that linked health care visit records of children with parents’ deployment records (Gorman, Eide, & Hisle-Gorman, 2010), and found that for children aged 3 to 8 years old, behavioral disorders increased 19% and stress disorders increased 18% when the military parent was deployed.
Other studies of child psychological adjustment and parental deployment have found that children aged 3 to 5 years with a deployed parent had significantly higher externalizing behavior scores and clinically elevated internalizing behavior when compared with same-aged peers without a deployed parent (Chartrand, Frank, White, & Shope, 2008). Children with a deployed parent also experienced more emotional and behavioral difficulties than civilian samples, and these difficulties tended to increase with deployment length (Chandra et al., 2010). Child attachment behaviors also have been related to length of deployment and number of deployments (Barker & Berry, 2009), and cumulative length of parental deployment during the child’s lifetime predicted child depression and externalizing behaviors (White, de Burgh, Fear, & Iversen, 2011). In one of the few studies including the previously deployed service member (Lester et al., 2010), total number of months deployed and parental distress (both at-home spouse and returned soldier) independently predicted child adjustment problems. The returned soldier’s posttraumatic stress disorder (PTSD) symptoms predicted child depression as well as internalizing and externalizing behaviors. Although these studies support the relationship between child psychological adjustment and parental deployment, they do not explain the reasons why these effects occur. In addition, many studies focus on psychological effects on the family during the deployment separation time period rather than on the postdeployment reintegration period when the service member transitions back into the family.
To investigate the association between mental health symptoms in returning service members and the effects on their children, a targeted assessment to determine possible pathways and mediators is needed. To this end, the current study examined the interrelationship between the active duty service member’s PTSD symptoms, general aggression, and marital distress following a combat deployment on child mental health symptoms. Two research questions were examined:
PTSD and Child Outcomes
Much of the literature that explores psychological symptoms in returned war veterans and emotional and behavior consequences for their children has focused on PTSD symptoms as exacerbating risk for children (Dekel & Goldblatt, 2008). Several studies have examined parenting behaviors that may be affected by PTSD symptoms. For example, a longitudinal study of returned National Guard soldiers and reintegration effects on the family system (Gewirtz, Polusny, DeGarmo, Khaylis, & Erbes, 2010) found that PTSD symptoms during deployment influenced couple adjustment and parenting 1 year later. Positive parenting behaviors, child discipline and supervision, and involvement and interest in the child’s activities were affected by the soldier’s symptoms and resulted in impaired parent–child interactions.
A review of the literature (Galovski & Lyons, 2004) summarizing the effects of exposure to violence during combat concluded that PTSD symptoms resulting from such exposure affected family relationships and psychological adjustment. Numbing and arousal symptoms, as well as anger, were predictive of family distress and secondary traumatization. The arousal cluster of PTSD symptoms promoted anger and hostility toward both spouses and children, and disrupted marital and parental relationships (Wadsworth, 2010). Combat exposure, PTSD symptoms, and aggressive behavior have also been related to violence and hostility in the families of veterans as well as increased aggression in their children (Glenn et al., 2002). This research was conducted with an older cohort of children of Vietnam veterans and revealed a possible continuity of risk of behavioral problems into adolescence and early adulthood.
Additional support for the negative effects of PTSD on parenting comes from studies of spouses and partners of veterans (Manguno-Mire et al., 2007) who were secondarily traumatized by the service members’ PTSD, and reported negative consequences for parenting behaviors. Psychological effects have also included secondary traumatization for children (Rosenheck & Nathan, 1985) and higher risk of developing behavioral or psychiatric problems (Davidson, Smith, & Kudler, 1989). One study compared Vietnam combat veterans with and without PTSD, and found significantly more behavioral problems among those children of veterans with PTSD than among children of veterans without PTSD (Jordan et al., 1992). More specifically, research from the Veteran Center counselor survey (Matsakis, 1988) reported that the most common problems among children of veterans were low self-esteem, aggressiveness, developmental difficulties, impaired social relationships, and symptoms characteristic of secondary traumatization.
These findings suggest that PTSD symptoms in the returned service member contribute to negative mental health outcomes in their children; however, the link requires further explanation. One possibility is the association between PTSD and aggression (e.g., Taft et al., 2007). As there is evidence that aggression in a parent predicts child outcomes (Jouriles, Barling, & O’Leary, 1987; Margolin & Gordis, 2000), aggression could be a mediating factor explaining the PTSD–child outcome link.
PTSD, General Aggression, and Child Outcomes
Population-based cross-sectional studies of service members have documented anger and aggression as frequently reported problems for combat veterans returning from war in Iraq and Afghanistan (Jakupcak et al., 2007; Killgore et al., 2008; Thomas et al., 2010). Studies have also identified aggressive behaviors as comorbid with PTSD (Forbes, Creamer, Hawthorne, Allen, & McHugh, 2003; Thomas et al., 2010), and found that combat experiences such as exposure to human trauma, combat violence, and killing predicted verbal and physical aggression toward others (Killgore et al., 2008). Combat veterans with PTSD symptoms, but not meeting full diagnostic criteria for PTSD, also reported significantly higher aggressive behaviors when compared with the non-PTSD group, thus increasing the potential magnitude of postcombat adjustment problems for service members returning home to their families (Jakupcak et al., 2007). A meta-analysis examined the association between anger and PTSD (Orth & Wieland, 2006). The authors found larger effect sizes in samples with military war experiences compared with samples exposed to other types of trauma, suggesting that anger may be a more likely response for those exposed to combat.
Although very little research has explored the link between general aggression and child outcomes in families of returning service members, findings from the civilian literature indicate that parental aggression is a risk factor for child behavioral and emotional problems (Jouriles et al., 1987; Margolin & Gordis, 2000). Notably, general aggression may affect the child even if it is not directed at the child but at the spouse or other nonfamily members (Galovski & Lyons, 2004; Glenn et al., 2002; Hurt, Malmud, Brodsky, & Giannetta, 2001). A parent’s display of anger/aggressiveness may manifest in several ways that affect the child (e.g., verbal outbursts, marital conflicts, angry facial expressions, and other visible displays). Children who are exposed to angry interactions between their parents may become more sensitized to marital conflict and more vulnerable to its effects (Faircloth, 2012). This, in turn, may lead to the child having lower thresholds for exposure to aggression and experiencing increased arousal, distress, and fear which can affect their mental health. Anger and general aggression rather than more covert symptoms of PTSD may be important in understanding the impacts on children and families. Thus, one mechanism by which PTSD symptoms have an effect on a child’s mental health symptoms may be via increased aggression in the parent.
Marital Distress and Child Outcomes
From the civilian literature, there is substantial evidence that parental marital distress and conflict can increase risk of child mental health problems (Rhoades, 2008). Consequently, the impact of marital distress on children in military families is an important consideration as marital problems have been reported as significant, negative outcomes of combat deployment. An extensive review of research on readjustment needs for service members and their families (Committee on the Assessment of Readjustment Needs of Military Personnel, Veterans, and Their Families, 2013) identified several key studies documenting the impact of deployment on marital and family quality. For example, a population-based longitudinal study of service members returning from Iraq and Afghanistan (Milliken, Auchterlonie, & Hoge, 2007) found an increase in reported interpersonal problems (including those with family members) from the reintegration period up to 6 months later. Additional population-based assessments of family and marital problems were documented in the Army Gold Book Report (Department of the Army, 2012) where 19% of spouses were reported to be in counseling. Therefore, the consequences of marital distress and conflict should be considered in the assessment of child outcomes to determine whether parental relationship problems are the key mechanism affecting psychological adjustment in children of returning service members.
Marital Distress, General Aggression, and Child Outcomes
Marital distress is a robust predictor of anger and aggressive behaviors, particularly directed at the spouse (Stith, Green, Smith, & Ward, 2008; Stith, Rosen, McCollum, & Thompson, 2004). Marital conflict also has been identified as a strong predictor of adults seeking mental health services and of poor psychological adjustment for children, with severity of aggression linked to marital functioning for the couple and to depression, delinquency, aggression, and declines in psychosocial functioning for children (Faircloth, 2012). Research conducted with a nationally representative sample (Vissing, Straus, Gelles, & Harrop, 1991) found that children who witnessed verbally aggressive conflict between their parents had higher rates of interpersonal problems, aggression, and delinquency than other children. This finding suggests that an atmosphere of anger and conflict in the family can lead to mental health problems for children.
Marital distress also may increase risk of angry and aggressive behaviors toward children and aggression in general. As a result, chronic patterns of violence or an atmosphere of anger and aggression in the home may affect family relationships and the psychological adjustment of family members. For example, anger in postcombat veterans has been associated with family relationships marked by distress and emotional conflict, with the veteran’s anger directed at a variety of targets and not necessarily at their spouses and children (Galovski & Lyons, 2004). In a review of family risk and resilience in the context of war, Wadsworth (2010) reported that OIF/OEF veterans at postdeployment felt uncertain of their family roles and believed their family members were afraid of them, with many describing conflicts involving shouting, pushing, and shoving. Thus, not only abuse or aggression directed at the spouse but also other types of aggressive or angry behaviors may increase in response to marital distress. Taken as a whole, this literature suggests that parental aggression represents one of the possible causal mechanisms linking parental PTSD symptoms and marital distress to child mental health problems.
Current Study
The current study examined the interrelationship between parents’ PTSD symptoms, general aggression, marital distress, and military children’s mental health. While many studies have focused on the civilian spouse during the separation period, the current study examined the impact of the active duty service member’s symptoms following a combat deployment on child mental health symptoms (hyperactivity, conduct, and emotional problems). We hypothesized that the service member’s PTSD symptoms and marital distress would both predict child mental health symptoms. However, we expected general aggression of the parent would mediate the impact of PTSD symptoms and marital distress in returning service members on child mental health.
Method
Participants and Procedure
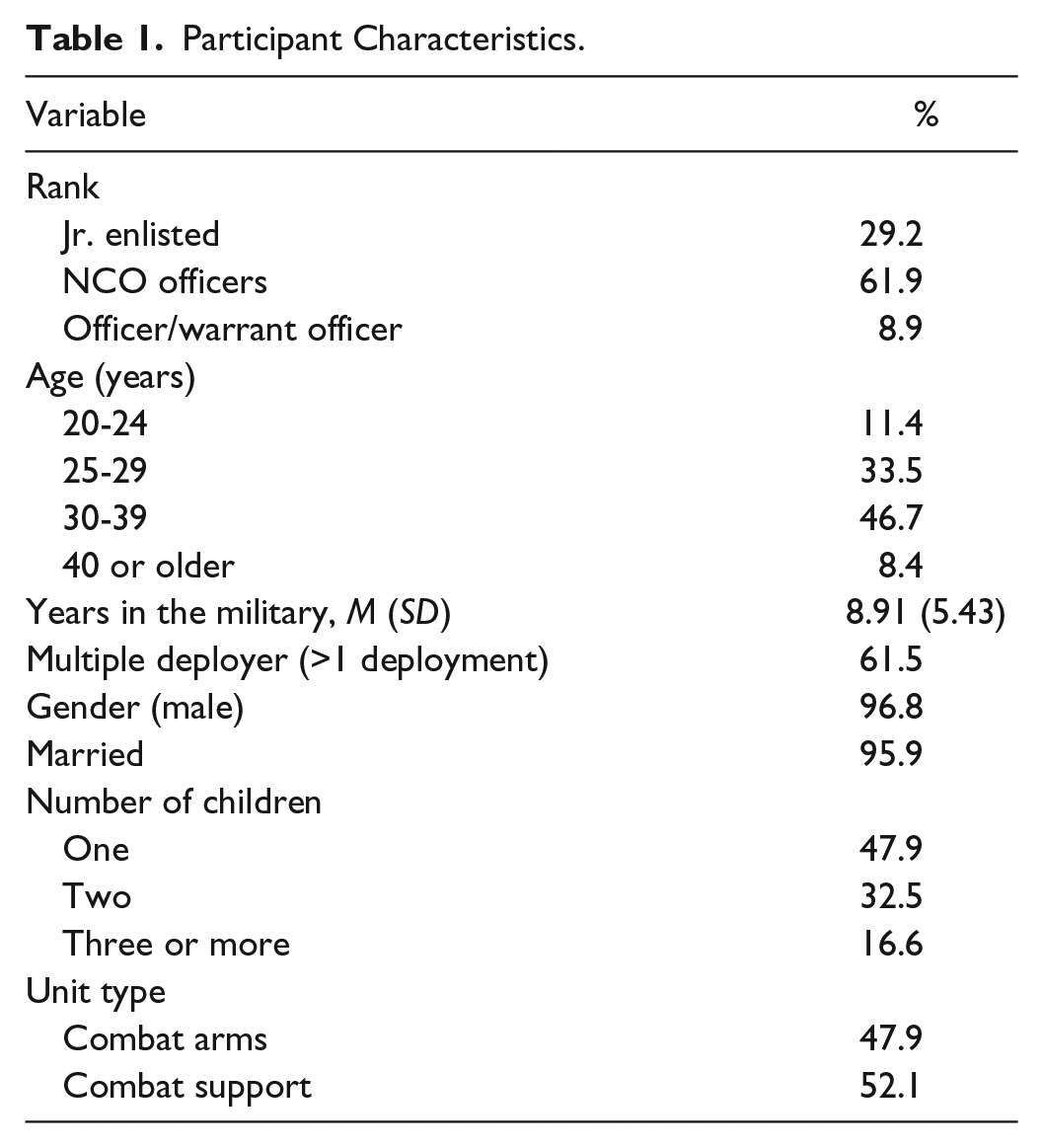
Active duty soldiers from a brigade combat team (N = 1,068) were invited to participate in the study 2 months following return from a 15-month combat deployment to Afghanistan. The study was approved by the local Institutional Review Board, and informed consent was obtained for all study participants, similar to other studies with active duty soldiers (e.g., Wright, Foran, Wood, Eckford, & McGurk, 2012). Surveys were administered to large groups of soldiers and required approximately 1 hr to complete. After being briefed on the purpose and procedure of the study, 91% consented to participate (N = 974) and were administered the anonymous paper-and-pencil survey. Participants in the current study included only those who reported having at least one child between the ages of 3 and 17 living at home (n = 169; 17.3% of the full sample). This rate is expected as this was a study of soldiers who served in a heavy combat deployment of which half of the overall sample was below 24. Sample demographics are presented in Table 1.
Participant Characteristics.
Measures
Parental PTSD symptoms
The widely used 17-item Post-Traumatic Stress Disorder Checklist (PCL; Blanchard, Jones-Alexander, Buckley, & Forneris, 1996) was used to assess PTSD symptoms. This measure has been validated with active duty military personnel (Bliese et al., 2008) and shown to have high internal consistency (e.g., Cronbach’s α = .96, current sample). Participants rated symptoms in the last month using a 5-point scale from 1 = not at all to 5 = extremely. Possible scores range from 17 to 85 with scores greater than 34 indicating a positive screen for PTSD symptoms among active duty military populations (Bliese et al., 2008).
Child mental health symptoms
The Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) was used to assess child behavioral difficulties in children aged 3 to 17. In addition to an overall score, the SDQ includes three subscales that assessed emotional problems (five items), conduct problems (five items), and hyperactivity/inattention (five items) rated on a dichotomous scale (0 = symptom absent, 1 = symptom present). This measure has good psychometric properties (Goodman, 2001; Tobia & Marzocchi, 2017), and has previously been used to assess child mental health symptoms among military samples (Chandra et al., 2010). Participants reported on symptoms for up to six children; symptoms scores were averaged across children. In addition, scores were computed using responses for the child with the highest scores reported within the family. Results were similar, so only average scores will be presented. In the current sample, the subscale alphas were .69 for hyperactivity/inattention, .58 for conduct problems, and .64 for emotional problems. These low to moderate alphas are not surprising, given that each subscale consists only of five items that are relatively broad in symptom content (Cortina, 1993). Cronbach’s α for the 15-item total scale was .77.
Marital distress
Marital distress was examined with three dichotomous items: “Are you having marital problems?” “Have you and your spouse gotten into frequent arguments or disagreements?” and the reverse-scored item, “Is your relationship strong?” This measure was developed based on item response theory analysis of commonly used marital distress items in military samples (Bliese, Wright, Adler, & Thomas, 2004; Ployhart, 2004). Items were rated on a scale from 1 to 2, with higher scores indicating more marital distress. These items have been used in other studies with military samples (Foran, Wright, & Wood, 2013). Internal consistency was .81.
General aggression
General aggression was assessed with eight items developed by the Walter Reed Army Institute of Research based on longer anger and aggression scales (Kulka et al., 1990; Spector & Jex, 1998; Spielberger, 1999) and used in previous studies with military populations (Cabrera, Bliese, Hoge, Castro, & Messer, 2010; Wilk et al., 2013). The items asked about angry feelings and aggressive behaviors during the past month (e.g., “threaten someone with physical violence,” “get into a fight with someone and hit the person,” “get angry at someone and yell or shout at them,” “boil inside with anger,” “feel like smashing something,” “get angry with someone and kick or smash something,” “slam the door,” and “punch the wall”). The items were rated on a 5-point Likert-type scale from 1 = never to 5 = five or more times. The internal consistency of the scale was .89. The aggressive behaviors may have been directed at the spouse, child, or nonfamily member. The scale was not meant to assess a specific type of aggression (i.e., spouse aggression) but rather aggression in general, which is a common presenting problem among combat veterans seeking mental health services (e.g., Taft et al., 2009). As expected, this measure was significantly but not perfectly correlated with a two-item measure of spouse aggression (r = .56, p < .001).
Results
Sample Descriptives and Bivariate Correlations
Almost one third of the sample reported PTSD symptoms above the cutoff of 34 or higher (31%). This high rate of PTSD symptoms is expected, given that there was a high level of combat exposure during the deployment. For example, 64% of the sample reported being attacked or ambushed, 79% reported that an improvised explosive device (IED) or booby trap exploding near them, and 51% reported a member of their own unit was killed in action.
In terms of child mental health symptoms, 50.9% of participants reported at least three hyperactivity symptoms for one of their children, 11.8% reported at least three emotional symptoms, and 9.3% reported at least three conduct symptoms. As shown in Table 2, parental PTSD symptoms, child mental health, marital quality, and general aggression of the parent were all significantly correlated as hypothesized.
Descriptive Statistics and Bivariate Correlations (n = 169).

Note. PTSD = posttraumatic stress disorder; MH = mental health.
p < .05. **p < .01. ***p < .001.
Model of Parental PTSD Symptoms, Marital Distress, and Child Mental Health
Structural equation modeling was used to test the multivariate model of parental PTSD symptoms, marital distress, and child mental health. Mplus 7.1 statistical software was used to conduct the analyses (Mplus, 2010). Model fit was evaluated with a variety of fit indices, including comparative fit index (CFI) > .95, Tucker–Lewis Index (TLI) > .95, root mean square error of approximation (RMSEA) < .08, and standardized root mean square residuals (SRMR) < .08 (Browne & Cudeck, 1993; Hu & Bentler, 1999).
First, we tested a model in which PTSD symptoms and marital distress predicted latent child mental health to determine whether they both accounted for unique variance in the context of each other. Because child mental health symptoms were strongly correlated, we analyzed them as a single latent construct in the model, treating each dimension as a separate indicator in the model. For latent child mental health, the factor variance was fixed to 1.0 and factor loadings were freely estimated. Analyses were conducted with full-maximum-likelihood estimation with robust statistics to adjust for potential bias due to multivariate nonnormality (Asparouhov & Muthén, 2005); notably, missing data on the various measures were minimal (<5%, n = 161-169). Parental PTSD symptoms and marital distress were free to covary. Results are presented in Figure 1. The model was a good fit to the data: χ2(4, N = 169) = 5.91, p = .21; CFI = .98; TLI = .95; RMSEA = .05, SRMR = .03. Both parental PTSD symptoms and marital distress uniquely predicted child mental health in the context of each other, and the size of the association was similar and of moderate magnitude; total variance accounted for in child mental health symptoms was 21%.

Parental PTSD symptoms, marital distress, and child mental health following deployment.
To test our hypothesis that general aggression may be a mediating factor that explains the association between parental PTSD symptoms and child mental health and between marital distress and child mental health, we tested a second model in which aggression was a mediating variable. Maximum likelihood with bootstrapped standard errors was used to test the model (1,000 draws). The model was a good fit to the data: χ2(6, N = 169) = 10.59, p = .10; CFI = .98; TLI = .95; RMSEA = .07, SRMR = .03. Results are presented in Figure 2. In Table 3, unstandardized estimates and confidence intervals for each path are reported. The direct paths from PTSD symptoms and marital distress to child mental health were no longer significant once parent general aggression was added to the model. Furthermore, when the direct paths from PTSD symptoms and marital distress to child mental health symptoms were removed from the model, χ2(8, N = 169) = 13.56, p = .06; CFI = .97; TLI = .95; RMSEA = .06, SRMR = .04, it did not significantly reduce model fit, Δχ2(2) = 2.97, p = .23. As shown in Table 3, the indirect paths from both PTSD symptoms and marital distress to child mental health via parent aggression were significant. The model accounted for 28% of the variance in child mental health. These results suggest that parental general aggression may be one mechanism through which parental PTSD symptoms and marital distress influence child outcomes.
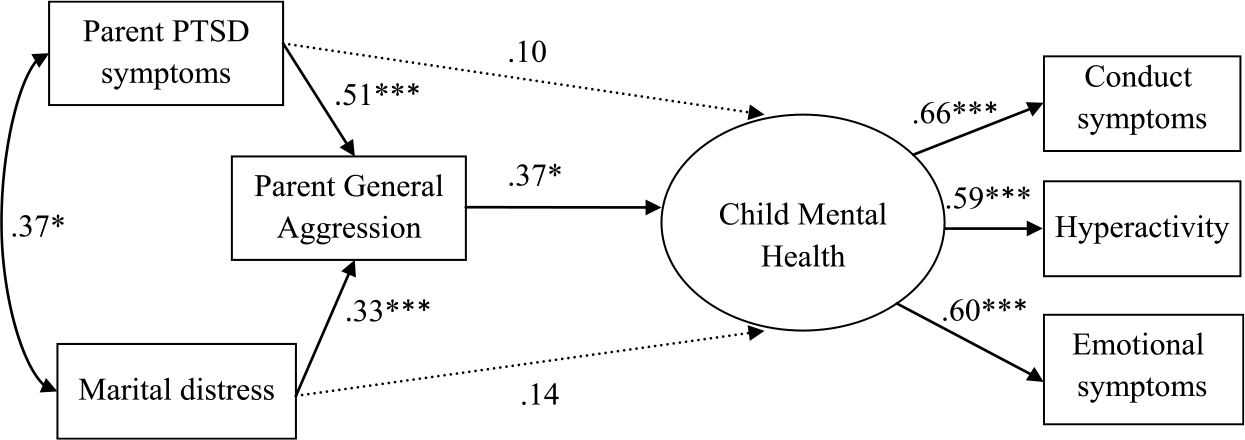
Mediation model of PTSD symptoms, aggression, marital distress, and child mental health.
Bootstrapped Parameter Estimates and 95% CIs for Model 2.

Note. Confidence intervals that include 0 are not statistically significant at p < .05. CI = confidence interval.
Discussion
Results from the current study supported the two research questions examining parental PTSD symptoms, general aggression, marital distress, and mental health of their children among active duty service members returning from a combat deployment. For the first research question, the study documented the association between parental PTSD symptoms and child mental health symptoms during the postdeployment reintegration period. This association was significant even after accounting for marital distress (see Table 2 and model depicted in Figure 1). For the second research question, the study demonstrated that the impact of PTSD symptoms on child mental health symptoms among returning military personnel may be explained by parental general aggression such that aggression mediated the PTSD symptoms–child mental health outcomes (see Figure 2).
This study extended the literature by focusing on the conditions for children in the military family during postdeployment as the returning veteran transitions home from combat. Combat-related trauma as expressed by PTSD symptoms, and the anger and general aggression found to mediate PTSD symptoms, may pose a significant problem for the psychological adjustment of children exposed to deployment transition challenges. The possibility of increased risk of negative mental health outcomes for these children suggests the need for early intervention, given the large numbers of veterans returning from combat deployment and the numbers of their children who may face exposure to reintegration adjustment problems. Future studies are recommended to address how the effects of combat trauma on family relationships can be reduced, and how children can be better protected during the adjustment period following return from deployment (Wadsworth, 2010). Some recently planned intervention projects designed to help military families through the deployment process are promising (Gewirtz, Erbes, Polusny, Forgatch, & DeGarmo, 2011) as they focus on intervention strategies to support at-risk families by improving parenting practices and child adjustment.
To build on the findings from the current study, research should be conducted to further explore the connections (pathways and mediating variables) between general aggression in the returning veteran and effects on their families. The importance of such research is illustrated by studies conducted with an older cohort of children of Vietnam veterans (Glenn et al., 2002) that revealed a possible continuity of risk of behavioral problems into adolescence and early adulthood for those families exposed to violent and hostile interpersonal interactions, suggesting the potential for long-term negative mental health outcomes.
There are some important limitations to our study that need to be acknowledged and that raise interesting questions for future research. Our sample was composed predominantly of fathers. The high proportion of men in the sample is consistent with known characteristics of service members with combat deployment experience who are mostly male. Nevertheless, it is possible that our results might not generalize to mothers, for whom the parent–child mental health relationship may differ. For example, in the Morris, Gabert-Quillen, and Delahanty, (2012) meta-analytic review of the relationship between adult PTSD and child PTSD symptoms among civilian families exposed to trauma concluded that this relationship was stronger for mothers than for fathers. Thus, our findings might underestimate the effects in a sample with greater proportions of mothers. The pathways linking PTSD and marital distress to child mental health symptoms also could differ by gender, such that aggression could be a more important factor for men than for women. These possibilities highlight the need for continued attention to how sample characteristics affect study findings in this research domain.
Another important issue concerns the fact that we only gathered data from the deployed spouse and not from the nondeployed spouse. Our study offers a unique perspective on child mental health as studies typically only obtain information from the nondeployed spouse. However, an assessment from both parents would provide a more complete picture of child outcomes. For example, the nondeployed spouse would have greater opportunities to observe their children’s mental health symptoms, whereas the deployed spouse may only hear about issues when they become problems. However, child mental health may be a more salient concern to the nondeployed spouse, leading them to be more aware of their children’s symptoms and/or more affected by them. Moreover, assessment of the nondeployed spouse to determine patterns of coping, stress level, and psychological symptoms during the deployment and following the service member’s return home would provide important information to better address risk and protective factors from a family systems perspective. These possible differences in reporting patterns between service members and nondeployed spouses raise several interesting questions for future research.
Furthermore, we assessed aggression broadly and did not include a distinct measure of anger or types of aggression (e.g., parent-to-child aggression, spouse aggression). There is substantial literature that indicates anger as a risk factor for aggressive behaviors (Anderson & Bushman, 2002), and both anger and aggression are more frequently experienced among combat-exposed veterans with PTSD symptoms (Orth & Wieland, 2006; Taft et al., 2007). In addition, our assessment of anger and aggression broadly maps onto treatment strategies in which both are typically addressed together (e.g., anger management programs for veterans). Nonetheless, there are also important differences between anger and subtypes of aggression, and these should be evaluated further in their relation to child mental health following deployments.
Another potential limitation concerns the cross-sectional study design. One important issue is that there may be bidirectional effects of adult and child mental health as well as marital distress and aggression. Both marital distress and general aggression may have been elevated prior to deployment. This may have in turn increased the risk of PTSD symptoms following return from deployment. We are, however, unable to demonstrate this in the current study, and cannot conclude whether there are long-term effects on family adjustment. Prospective, longitudinal studies with larger samples are recommended that would provide data on preexisting child behavior concerns, marital distress, aggression, and PTSD symptoms to identify either improvements or exacerbation of problems over the course of the deployment cycle.
Summary
A particular strength of the current study is that it included an assessment of redeploying service members during a unique time frame immediately following their 15-month combat deployment with data collected from the perspective of the returning service member. In addition, the study highlights the importance of parental general aggression as a potential mechanism of transmission of mental health symptoms from parent to child. There is evidence of an association between PTSD and general aggression in returning service members, and the study now demonstrates that the impact extends to child mental health outcomes. Future research should explore the possible bidirectional effects of child outcomes on the returning soldier and impacts on other family members from a family systems perspective (Minuchin, 1985).
Footnotes
Acknowledgements
We thank Steven Birchfield, Crystal Burnette, Edward Edens, Victor Martinez, Dennis McGurk, Angela Salvi, Steven Terry, and Michael Wood.
Authors’ Note
The findings described in this article were collected under a Walter Reed Army Institute of Research Protocol. The views expressed in this article are those of the authors and do not necessarily represent the official policy or position of the U.S. Army Medical Command or the Department of Defense.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.