
Abstract
Experience-based co-design (EBCD) is a service design strategy that facilitates collaborative work between professional staff and service users toward common goals. There is a lack of published examples of it in relation to family carer engagement within a mental health context, and little research exploring the mechanisms behind successful implementation. The aim of this study was to explore the processes that facilitated EBCD with carer involvement. The study adopted a grounded theory–informed approach involving interviews with 16 participants of an existing EBCD project in an English National Health Service (NHS) trust, reflecting multiple stakeholders. EBCD can be thrown off track in two ways: conflict and getting “bogged down.” Leadership by project and design-group leaders could return group cohesion and maintain project momentum. The developed model reflects key processes. Future research should examine EBCD projects with similar ranges of stakeholders and in contexts with different levels of organizational change.
Keywords
Introduction
Policy documents mandate the involvement of service users and carers in English National Health Service (NHS) service design (Cree et al., 2015; Department of Health [DoH], 2001, 2004, 2008; Wilkinson & McAndrew, 2008), but tend to be short on guidelines for implementation (Rutter, Manley, Weaver, Crawford, & Fulop, 2004) resulting in user involvement remaining poorly defined (Millar, Chambers, & Giles, 2015) and under-utilized (Lewis, 2014). Common means of eliciting user views have been satisfaction surveys, one-off consultation, and complaints procedures (Crawford et al., 2002). This information has rarely been translated into service improvement (Coulter, Locock, Ziebland, & Calabrese, 2014). Barriers to involvement in service design have included prioritizing organizational needs over service user and carer need (Horrocks, Lyons, & Hopley, 2010), use of technical language, and professional attitudes toward involvement (Hitchen et al., 2011).
Experience-based co-design (EBCD) engages those who use services and staff at “every stage within the design process, from problem diagnosis to solution generation and implementation” (Bate & Robert, 2007b, p. 41). The idea of “co” in co-design refers to moving service users to a position where they are actively contributing to designing care. EBCD follows a six-stage process (The King’s Fund, 2013; Robert et al., 2015) displayed in Figure 1. The first stage involves gathering service user, carer, and staff experiences of the service via interviews and observations. Touchpoints are identified, critical moments with emotional tone within an individual’s experience of a service (Bate & Robert, 2006). The touchpoints are fed back to service users, carers, and staff at a joint event, using edited films of user interviews. During the joint event, small co-design groups are developed to collaboratively design quality improvement outcomes. A celebration event is held at the end to allow all involved to review progress.

Diagram representing EBCD process based on Donetto, Tsianakas, and Robert (2014).
Donetto, Tsianakas, and Robert (2014) conducted a survey identifying the practices and developments made within EBCD from its conception in 2005. They identified 59 completed projects internationally, with 70% evaluated, usually available in the form of an internal report, and less frequently as a peer-reviewed journal paper. Projects have ranged across diverse settings, including cancer care, diabetes, intensive care (Donetto et al., 2014), and, less commonly, mental health (Cooper, Gillmore, & Hogg, 2016; Larkin, Boden, & Newton, 2015; Springham & Robert, 2015).
There is less reporting of carer involvement than user involvement. Indeed, the King’s Fund’s (2013) toolkit subsumes carers within the term “user.” However, one project has explicitly focused on informal carers of patients receiving treatment for cancers (Tsianakas et al., 2012), and a later project tested the impact of an intervention previously co-designed between informal carers and health care staff, and reported improved carer understanding of symptoms and side effects compared with non-intervention control condition in a chemotherapy setting (Tsianakas et al., 2015). Wright, Lowton, Robert, Grudzen, and Grocott (2017) included both service users and carers in a project in palliative care.
The available data suggest EBCD has successfully led to implementing small-scale improvements such as training manuals and information packs (Donetto et al., 2014). Secondary benefits include increased understanding of each other’s perspectives; increased sense of community (Tsianakas et al., 2012); promotion of mutual accountability between service users, carers, and staff (Boaz et al., 2016); and enabling staff to reconnect with personal values around care (Tollyfield, 2014).
EBCD success may be dependent on a receptive environment for change, high level support, and co-design improvements that are specific to a service, as difficulties can be met when improvements require involvement of other internal but separate teams (Tsianakas et al., 2012). Sustainability of improvements relied upon staff ownership of outcomes. This can be limited by high staff turnover (Wright et al., 2017).
Adaptations are required for implementation in mental health settings. Larkin et al. (2015) reflected on ethical considerations, including consent, anonymity, confidentiality, and data ownership; mental health stigma; and the potential for re-traumatization following retelling or reliving difficult experiences. They instigated safety procedures such as providing service users with contact information for the named facilitators. Springham and Robert (2015) raised the issue of power as a particular difficulty within mental health, where professionals can impact upon an individual’s civil liberties (Springham & Robert, 2015).
EBCD was developed from participatory action research, learning theory, and narrative-based approaches to change (Robert, 2013). Its aim is to afford service users and carers a stronger voice. This stance challenges the status quo and requires service users, carers, and staff to renegotiate their roles and reconfigure the balance of power held within the traditional structures in quality improvement work and, more broadly, within the NHS (Donetto et al., 2014). Allport’s (1954) contact hypothesis seems helpful here. It proposed that enabling contact between conflicting groups, and giving them equal status in pursuing common goals, fosters mutual understanding and collaboration. Corrigan and Shapiro’s (2010) literature review of the impact of anti-stigma programs supported this view.
Study Rationale
Further research is required to ensure reliable effectiveness of EBCD. This can only be facilitated by “understanding the social processes and mechanisms that produced the outcomes” (Dixon-Woods, Bosk, Aveling, Goeschel, & Pronovost, 2011, p. 1). This is particularly apparent within the mental health context, where EBCD is still in its infancy. While a ward-based EBCD project appeared to produce a dramatic reduction in complaints (Springham & Robert, 2015), EBCD as a methodology has not previously been applied within the complex context of improving family and carer involvement within a community mental health team (CMHT). The current study aimed to explore and develop a theory of the perceived mechanisms that might facilitate the EBCD process with carer and family involvement.
The following questions were addressed:
How do participants in an EBCD project perceive the project and their participation in it?
What factors do participants see as helping and hindering progress?
Method
An NHS Research Ethics Committee reviewed and approved the research. All documents were reviewed by a service user group to ensure readability. Informed consent was gained from participants, in line with the British Psychological Society (BPS, 2009) Code of Ethics and Conduct. Participants were made aware that the third author was directly involved in the EBCD project. They were informed that this person would not read interview transcripts. Quotes in this article are anonymized. As a participant observer, the first author identified herself and explained her role at the start of every meeting to further ensure informed consent for data collection.
Context
The study was conducted within a CMHT in outer London. The Trust had identified carer involvement as a key area for change. The family and carer EBCD project was initiated in 2014, and was still ongoing in 2017. The project leader had been integral to the instigation of EBCD within the Trust, and had been involved in a previous successful project.
Design
The study adopted a grounded theory–informed approach within a social constructionist framework (Charmaz, 2006). This methodology enables exploration of social action, consistent with EBCD. Grounded theory is often used to approach underexplored areas of research (Corbin & Strauss, 2015). The EBCD project with families and carers in a mental health context was the first of its kind. A social constructionist standpoint acknowledges the researcher’s own viewpoint in the interpretation of data (Charmaz, 2006). The first author’s role was to document the EBCD project’s work and theorize about its perceived processes.
Participants
Participants were recruited from the existing EBCD project, aiming to sample for diversity of perspectives. Participants from all stakeholder groups were included. Two service users and two carers were interviewed, which meant that members of two out of the original five families in the EBCD project were included in the present study. A greater number of staff was involved in the EBCD project, and 12 staff members were interviewed to include the different professions. Professions included psychology, occupational therapy, art therapy, family therapy, community psychiatric nursing, and carer support. Table 1 shows participant demographics.
Participant Demographic Information.

Data Collection and Analysis
A semistructured interview was developed and initial interviews lasted 45 to 90 min and took place within the community team site between July and September 2016. Open questions enabled the first author to be responsive to individuals’ unique experiences (Smith, 1995). Data collection and analysis ran concurrently. The focus of the questions was on participants’ experience of participating in the EBCD project, beginning with how people came to be involved and experiences of different phases and events. As is usual in grounded theory research, the first author added new questions as the research proceeded and in discussion with the other authors, to explore emerging themes and assist theoretical development (Charmaz, 2006), for example, eliciting further perceptions of a conference that appeared to have had a re-energizing impact part-way through the EBCD project (discussed in the “Results” section). Other than this exploration of new issues as they arose (theoretical sampling within interviews), theoretical sampling of new participants was not possible within the scope of the project, hence the description of the method used as grounded theory–informed.
One service user and one staff member completed a follow-up interview in February 2017 to explore later developments in the project. These participants were chosen as they were part of the remaining EBCD team. As major organizational change unconnected with the project (see “Results” section) resulted in it being moved to a different team, original staff members could no longer be involved. As can happen in EBCD, the joint event with staff, service users, and carers led to suggestions for improving more than service issue, and four co-design work-streams were created with different aims, each planning to meet regularly to do the co-design work. The first author attended meetings as a participant observer in one of these co-design streams. Field notes were used for triangulation (Bryman, 2015). These are only reported upon where they add something to the quotations from interviews.
Data analysis followed Charmaz (2006) and Urquhart (2013): initial, focused, and theoretical coding. Line-by-line coding of transcripts enabled the first author to stay “close to the data” (Charmaz, 2006, p. 51). This was then refined through focused coding, comparing between transcripts and between codes and data, known as constant comparison (Glaser & Strauss, 1967). The final phase of theoretical coding involved establishing the relationships between concepts, facilitating theory development (Charmaz, 2006). Diagramming and memo writing aided this process (Charmaz, 2006). The final theory was shared with the remaining EBCD participants for respondent validation.
Quality Assurance
Good practice guidelines were followed (Henwood & Pidgeon, 2003). Yardley (2000) specified the following characteristics: (a) sensitivity to context, including, in this case, participants’ perspectives and ethical issues; (b) approaching the topic with commitment and rigor; (c) transparency and coherence; and (d) recognition of researcher impact.
Analysis was completed by the first author and a sample of transcripts were also coded by the second. Discussion between all three authors, respondent validation, and reflective memos of category development and personal responses to the data were used to enhance methodological rigor (Strauss & Corbin, 2008), especially as the first author had previously belonged to the service and might share some assumptions made by participants.
Reflexivity
The first author carried out the research as part of clinical psychology doctorate training, and had earlier worked alongside members of the CMHT on placement. This placement coincided with the instigation of the EBCD project. The first author attended the joint event but had little further involvement at that time. At co-design meetings during her subsequent research, group consent was gained at each meeting.
The researcher’s relationship with the team may have influenced the project: Staff may have felt comfortable through knowing her or have limited their disclosures due to her changed role. Carers and service users may have seen the author as a staff member, possibly impacting their openness. The author differentiated her role from that of an active clinician in discussions with service users and carers. The first author kept a reflective diary to examine and remain aware of possible bias. She had an interest in service user and carer involvement, was aware of previous work in the trust involving service users, and viewed this favorably. She was mindful of the potential for service user and carer involvement to be tokenistic if not implemented meaningfully.
Results
The EBCD Project
Carers had made complaints against the CMHT prior to the EBCD project, and carer involvement had become a priority at trust level, leading to willingness to try EBCD. The carers and family project followed the EBCD process outlined by the King’s Fund (2013). Carers were recruited from a carer’s group run in a community-based charitable organization external to the trust, which had 30 families attending. Five families were willing to participate in a process mapping exercise where they used post-it notes on a giant roll of paper to display the team admission process. Carers in five families were interviewed for films, and then, the five edited films were played back to these families to test that the films presented the touchpoints the families had identified. These edited videos were shown at the joint event. Four carers, three service users, and 22 staff members attended this event.
Four design streams were collaboratively generated from the touchpoints: psychoeducation for carers, first meeting between service users (with carers) and the team, confidentiality, and service users’ advanced directives. Each co-design group comprised service users, carers, and staff. Two groups did not develop solutions and two were merged due to staff dropout (Table 2). Through using role-plays to develop prototype versions of potential staff–carer interactions (Bate & Robert, 2007a), a number of outcomes were planned, namely, a training manual for staff delivered by carers and service users, a psychoeducation group for carers, and a mapping tool to elicit from service users who were in their social network and who they wanted involved in their care.
The Four Design Streams of the EBCD Project and Their Progress.
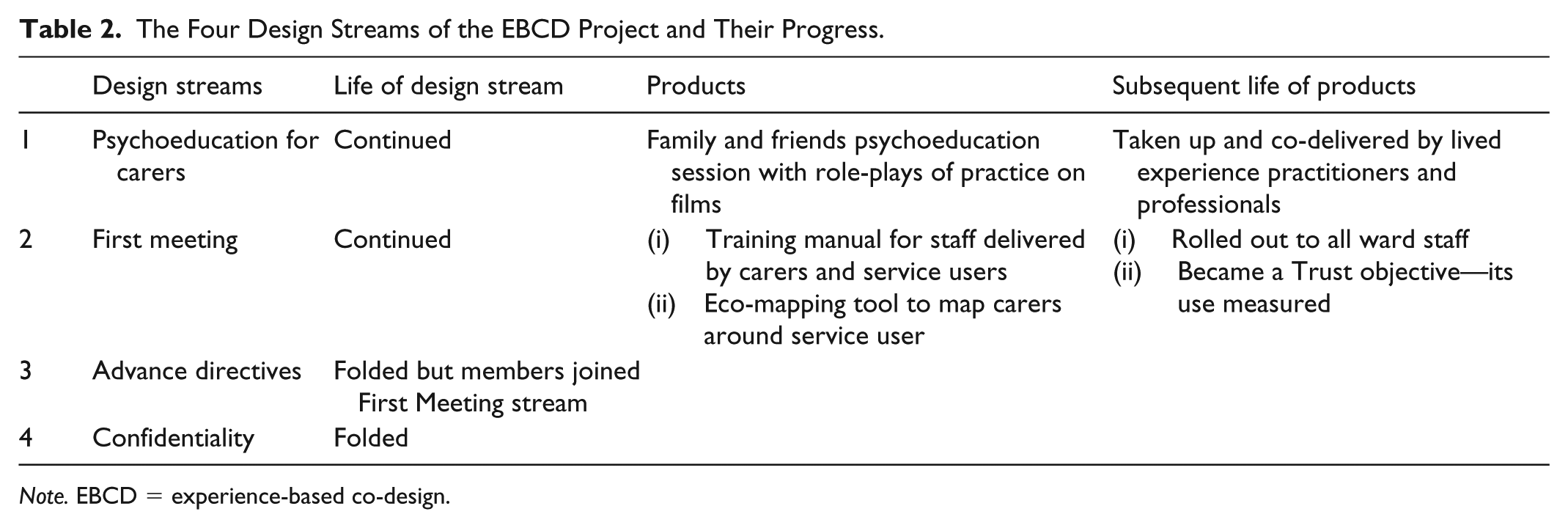
Note. EBCD = experience-based co-design.
Throughout the project, organizational changes occurred, including a service re-design, which resulted in changes to staff’s team membership, location, and management. Furthermore, the team underwent a Care Quality Commission review, and had to address some areas of need. The process and the corresponding contextual changes are illustrated in Figure 2.

The contextual factors that took place during the EBCD project and at what stage within the project they occurred.
Figure 3 shows the theory derived from the data. This is a constructivist grounded theory, and that is to say, the authors recognize that its precise form and content depend on the sense that the participants made of the various events they experienced within the specific health care context of the EBCD project, and also the sense that the researchers made of participants’ perceptions and their own direct experiences of the context (Charmaz, 2014). With these provisos, the figure depicts the main processes that seemed to be required for the successful implementation of the family and carer project, in addition to those hampering progress. It is an explanation of some psychological, social, and contextual processes that appeared to influence how a particular project proceeded, some of which may operate (or be perceived or experienced as operating) in similar health care contexts and with similar projects. Within a critical realist epistemological framework (Gorski, 2013; Marchal et al., 2013), it is acknowledged that real world processes happen but that we are operating in an open system that is only partially controllable. The theory indicates some of the processes that may be influenced and in what ways, in complex situations that bear similarity to the specific context in which this research was conducted. This section outlines and illustrates with participant quotations each constructed category, with corresponding subcategories. Field notes concurred with interview data.

Grounded theory of facilitators and barriers to EBCD.
Planets Align
Participants reflected upon multiple factors impacting the implementation of EBCD, described as planets aligning (Table 3). First, EBCD was reported to have developed a reputation within the NHS trust for tackling areas of difficulty: prior success. It was recognized as an “agent for change” (Staff 5).
Very compelling evidence that the methodology of EBCD can be a really good change you know, agent for change. (Staff 12)
Respondents reported that EBCD had to fit with organizational and personal values to be supported and to motivate individual engagement. The organization had to recognize the need for service user and carer involvement, as supported by local and national policies.
[Senior staff member] was charged with, of bringing, of developing a new carers’ strategy that had just run out. . . . so all the planets aligned and at the top level. Complaints, “must do’s,” carers expressing huge amounts of anger. So there was a massive need. (Staff 1)
Many participants also drew on personal experiences of service user and carer involvement to describe their motivation. Involvement was valued as a common-sense approach to improving services.
If I come up with a good idea, and I think, oh this is what they should use but ultimately the people who use it are the staff and the service users aren’t able to invest in it then it will fail, whatever, however, good the idea may be. So I always try to involve everyone with that set of things. (Staff 7)
Staff members saw service user and carer involvement as compatible with their ways of working.
I’ve come to learn to work with individuals but also had a systemic view . . . so when [project leader] told me about this I thought this is what I do all the time, . . . my bread and butter therapeutically is to bring about change by enquiring, by working with the system therapeutically. (Staff 2)
Finally, it was acknowledged that for a project to be implemented, all stakeholders needed to be invested in it, multiple stakeholder commitment.
The Trust had kind of put their hands up and said, we’ve made mistakes. And we want to see if we can change. . . I was hoping that it would bring together everybody within the Trust service, . . . and to try to talk things through and yeah I was interested then to see where it was going to go. (Carer 2)
List of Categories and Subcategories for Planets Align.

Implement EBCD Process
Participants stated that showing the carer and service user videos and providing space to share experiences was memorable. Participants reported that these narratives enabled staff to recognize a need for change in practices. Hearing others’ perspectives enabled them to place themselves more readily in another’s position. The joint event facilitated mutual understanding (Table 4), which appeared to lessen the divide between service users, carers, and staff.
The videos that are being shown are the individuals saying this is how I feel, this is how it felt, this is how I was looked after, this is what I think could have gone well. . . . It tugs at people’s heart strings . . . You could see people’s enthusiasm and eagerness to change develop within that room. You could see people thinking about, “What can we do differently.” (Staff 7) I am much more understanding about what situation faced by clinicians after that training. Because previously I could only see things from my point of view, and thought “how could they not—be so unsympathetic to my situation?” but obviously they didn’t know what went on before my [relative] had the breakdown. (Staff 6, with carer experience)
List of Categories and Subcategories for Imlement EBCD Process.
Note. EBCD = experience-based co-design.
It was reported that all stakeholders within the group were given the opportunity to voice their opinions and experiences, with diverse perspectives valued, and that this helped the co-design group to move forward: group cohesion.
I think once we moved on from that initial stage where everyone is airing what they needed to air and started talking about plans going forward, I thought there was space to talk, I hope, and I found it really helpful to have such a range of people in the room, who had ideas, lots of ideas. (Staff 10)
Following the formation of a cohesive group, stakeholders were then able to focus on collaborative action to develop solutions, with staff membership ensuring that these were realistic for clinical practice.
We can all come at something from a different perspective. But before the day is out, we have all agreed what is going forward. So it’s not been any one person saying “oh actually, we’re going to be doing this.” (Service User 2)
It is proposed that for solutions to be sustainable, they needed to be simple and fit within clinical practice.
Of course what we come out with is obvious and simple, but it’s not being done, so there’s something not obvious about that. (Staff 1)
Planets Misalign
Participants highlighted factors that one described as when the planets misalign (Table 5). These seemed to contain two categories: conflict and bogged down. Many participants acknowledged initial conflict within co-design groups, with one suggesting it was the meeting of “two warring factions” (Staff 1): Carers initially used meetings to share further difficult experiences, leaving staff feeling attacked. There was acknowledgment of the need for these stories to be heard to identify potential solutions, but it became overwhelming for some staff.
The meeting would turn less about co-production and more about some way to, as a space to kick the service as the staff were sat there, which must have been awful for them to hear. (Service user 2)
List of Categories and Subcategories for Planets Misalign.

Service users and carers did report feeling respected and heard, but carers also reported concerns about power, stating that group cohesion was terminated at the end of each session, which may reflect the legacy of carer and service user involvement. Carers reported a history of being excluded and disempowered.
You are very aware that the minute you leave that room, they will go back into their role and they will go back into their job that they are doing, and you don’t know what they are going to say to your care co-ordinator. (Carer 2)
There was sometimes a sense of all stakeholders feeling unsupported at points of emotional intensity. Involving carers from an existing external carer’s group was meant to address this by providing a supportive forum; however, it appears not to have been sufficient. This was different from the situation with service users, who gained support through their existing membership of a trust-run group.
The carers, we don’t have debriefing, we don’t have colleagues that we can turn to and say, could we just run over this with me or I felt like this. It was kind of like, at the end of the meetings . . . you know, really we had nothing. (Carer 2) It’s really important, obviously not to be defensive in any way. . . . That might be easier for some members of staff than others, and it may be something people need a bit of support with. (Staff 10)
Participants described the project sometimes becoming bogged down. First, the project was implemented during major organizational change, in which the host team was divided into two separate teams, alongside a change in manager and site. This is often the reality of “designing in the real world” (memo following conversation with the project leader).
It was a big change, they [staff] were trying to get their heads around that, . . ., it possibly didn’t create the right circumstances to enable people to get involved. (Staff 12)
This change seemed to impact staff morale and engagement.
If it’s happening around the time you’ve got enormous change and challenge for a team, it’s inevitable that some people just can’t prioritise it. (Staff 10)
Although numerous desired outcomes were identified, this did not always progress to solutions. Two co-design streams folded (see Table 2), and it is proposed that this was due to the tasks being seen as unfeasible due to relying upon wider structures within the trust. Other potential solutions were limited by insufficient resources and reflected a need for greater backing from the trust.
They [advanced directives] are quite a tricky area, in terms of confidentiality and advanced agreements, it’s like, well where do you begin to tackle this. (Service User 2)
One participant stated that it is “counterintuitive” (Staff 12) for stakeholders to work with prototypes and discard unhelpful solutions: suggesting a lack of design experience–hindered progress. This may be a product of anxiety and that flexibility in thought and perceived agency for a solution is required and may not fit with the norm of NHS service design.
There’s the actual doing, the actual, “Okay, so this is the issue, we’ve heard all these different voices now what are we going to do about it?” And my sense was that just, that was really where it started to get bogged down. (Staff 12)
Many participants reflected on resistance to change. A number of ideas were raised to explain this, including prioritizing demands on staff time, lack of belief in the need for change, and perception that some staff were “volunteered” to participate rather than volunteering. Each could result in disengagement.
Sometimes it’s easier to go along the way you have been doing than to do any change . . . That’s what I think is difficult about the whole of the project. (Carer 1) So we’ve taken the project away from the community teams and we’re piloting it on the wards. . . . Maybe we’re doing that because the planets align there, because the management is engaged through that. (Staff 1, Interview 2)
Leadership
Participants suggested that senior and local leadership (Table 6) was necessary for supporting staff to be fully engaged with the project, sustaining solutions in the future, and providing credibility.
So I think I’ve learned that if the managers don’t engage there’s no way round that. (Staff 1, Interview 2) For clinicians, . . ., there was a recognition that this was taken seriously, . . . And for service users and carers . . . they felt they were taken seriously. That really this is something the whole trust, with its hierarchy and authority, really want this to happen. (Staff 2)
List of Categories and Subcategories for Leadership.

The project leader and group facilitators were instrumental in the smooth running of the project.
We want to be responsive and work with whatever comes up. Because it’s not just the solutions that are emerging and coming up, it’s also the blockages, the barriers that are coming up and to deal with that takes time and space. (Staff 2)
Group and project leaders could move things forward when groups were striving for cohesion. Participants stated that the process of “airing what needs to be said” could become circular, resulting in no collaborative action. It was helpful when leaders acknowledged past experiences and drove the group forward by reminding participants “Everybody is working to the same ends” (Carer 1).
I’m often quite surprised by how much of a therapist part of myself that I have to use in that, as a kind of peace negotiator, . . . both for staff and service users, especially when both sides go into attack mode and don’t want to come together because they are feeling injured. (Staff 1)
Furthermore, the project leader needed to support movement from inaction to action, by sifting through group ideas to fix a plan. This approach may have limited co-production, but actions were collaboratively sanctioned.
I think, just having [project leader] there made it possible to sit down and write some stuff down and start to plan . . . And I think that was really important. (Staff 10)
The project leader helped people focus on outcomes that could be produced quickly. This approach was taken to maintain motivation and engagement.
Why would you go for the longest projects and hardest projects first, when . . . it’s a quicker process for the other two, so let’s get those two done and dusted, get them working? And then revisit the ones that are going to be a much longer process. . . . More about policy and HR. (Service User 2)
Maintain Momentum
Many participants reported that the project was a long process. Participants noted that momentum ebbed and flowed, and suggested means of maintaining momentum (Table 7) to “keep the project alive” (Staff 12). Participants felt that changes happened and those not directly involved were not informed, suggesting a need for increasing communication. Lack of information could limit co-creation, but it was re-kindled by opportunities to showcase outcomes of the work at a trust-based conference. This gained recognition from outside the project.
It’s sometimes you know, important to remind people, to update people, refocus, . . . keeping an awareness going. (Staff 3) We presented some of our work. . . . After it all, some other staff members from the trust came up and said this sounds amazing. And they said it in front of the families and carers, and for the first time they felt like they were really doing something, and they were all so pleased and really buzzing. (Service User 2)
List of Categories and Subcategories for Maintain Momentum.
Momentum was also maintained by highlighting benefit for all stakeholders, and viewing outcomes as “not doing more, but doing differently” (Staff 9).
The methodology . . . it enables us to see that this is kind of, it’s not an added extra, it should be integral, it’s fundamental rather than this, “I’ve got to do a carer’s assessment and I’ve got to do that.” (Staff 12)
Discussion
The preliminary grounded theory of facilitators and barriers to EBCD (Figure 3) proposes that certain conditions need to be met prior to project initiation, namely commitment from multiple stakeholders, facilitated by the approach being consistent with organizational and personal values and previous successes, captured by the concept planets aligning. This has been recognized in previous EBCD projects (Larkin et al., 2015). Once these conditions are met, a joint event facilitates sharing personal stories, enabling the development of mutual understanding around project aims. The emotionally charged stories on film, which can “tug at people’s heart strings” (Staff participant 7), help staff to reconnect to their personal values. In our theory, we hypothesize that this contributes to group cohesion and collaborative action. This is in keeping with recent theorizing by Palmer et al. (2018) relating to the way that people telling their stories assists staff, service users, and carers in moving from focusing on their individual experience or collective discontent, to a sense of mutual understanding and togetherness, and working for a common goal.
The joint event in which films are shown to convey service user experience, and also the experiences of staff are heard, is also consistent with the much older contact hypothesis (Allport, 1954), which held that certain conditions need to be present for the reduction of stigma. These included each member having equal status in pursuit of a mutually valued goal supported by the institution. The EBCD process appeared to facilitate these conditions. The EBCD projects of Tsianakas et al. (2012) reported increased understanding of the “other” perspective and creation of shared identity. Stakeholders mainly felt respected for their expertise and knowledge, as suggested by Bate and Robert (2007b).
All this notwithstanding, we also hypothesize the need for particular skills in a project leader, to steer it through the potential for derailment by existing power imbalances, as reported in other projects (Larkin et al., 2015) and present in the model of EBCD for mental health services by Palmer et al. (2018). Tuckman’s (1965) established model of group work can be used to explain some of the challenge inherent in EBCD co-design groups. Tuckman’s model encompassed four stages: (a) Forming, orientating the group around the task; (b) Storming, the group responds to conflict; (c) Norming, a cohesive group is formed, opening up freedom for personal opinion; and (d) Performing, the group channels its energies into the task. In relation to our preliminary grounded theory of EBCD, the sharing of experiences may have facilitated the formation of the groups and highlighted the importance of the task and joint goal. However, some conflict was experienced in relation to “airing what needed to said” (Staff 10), where staff felt “attacked” and service users and carers experienced a repetition of previously unhelpful power dynamics. Support is required at this point for all stakeholders, and should be offered by project leaders and local management.
Stains (2012) suggested ways of assisting participants of dialogue who may slip back easily into patterns of conflict to become and remain more reflective and curious before, during, and after coming together. Lessons from the field of conflict resolution may be particularly helpful for EBCD in mental health services where there can be large power differentials (Springham & Robert, 2015), as experienced by some in this project. Blackwell et al. (2017) found it helpful to set up regular staff forums “to review problems and share successes” (p. 89). Such structures are also suggested by a recent review of facilitators and barriers to service user engagement in co-design (Bombard et al., 2018).
While service users in the current project had a regular group where they could discuss the project, neither staff nor carers had a dedicated regular forum. Nevertheless, two co-design groups were able to move beyond conflict and described the openness and value of multiple perspectives in developing solutions, and began performing.
At the collaborative action stage, multiple perspectives are used to generate simple, sustainable solutions. In the current project, groups found it difficult to move to a point of action and needed group leader support in selecting solutions. If actions are based on group-generated ideas and endorsed by the group, this remains close to co-design. Bate and Robert (2006) stated that “users” were co-partners not co-leaders. At times, the group’s task can require too much from structures and teams outside the co-design group. This can lead to disengagement, consistent with the findings of Tsianakas et al. (2012). Future projects should focus on simple solutions that can provide quick outcomes and maintain motivation for those involved. Staff can feel less burdened when small but significant solutions can be readily implemented (Blackwell et al., 2017). As found in the literature, participants of the current project reported secondary outcomes, namely some service user and carer empowerment and a staff re-connection with their values (Cooper et al., 2016).
The current study highlights important factors that can hamper projects. The EBCD project coincided with a time of major organizational change, which appeared to impact staff morale but also changed the structure of their team. There was a loss of local management, leading to reduced commitment at that level. It seems likely that this, together with staff overstretch due to the reorganization and thus difficulty prioritizing the project, explains staff dropout from the project when things were difficult. Some initial conflict is inevitable, as is illustrated in the model diagram, and when surrounding organizational factors (planets misalign) are also present, it is likely to be even more difficult, though perhaps not impossible with good project leadership and efforts to maintain momentum. This can allow at least some participants, perhaps having built cohesion within their co-design groups, to sustain commitment and continue fruitful work. These findings are consistent with process research by Leamy et al. (2014) on implementing change in the NHS, and with other EBCD projects within physical health settings (Bate & Robert, 2007b).
Our findings are also consistent with the review by Bombard et al. (2018) on what helps maintain service user engagement in health care co-design. Factors they emphasize include leadership (high level commitment and local champions), a receptive context (efforts to reduce power disparity between staff and patients), and preparation of all stakeholder groups, which may entail joint training and makes clear everyone’s roles and responsibilities. The new theory presented here is based on only one context as opposed to reviews that encompass many studies. However, the aim was to capture the dynamic processes of an EBCD project, and to represent how a project as a whole may be impacted by and its participants negotiate inherent challenges along the way. Our grounded theory suggests ways to maintain momentum in the face of these challenges and when “planets misalign,” and these include leadership, communication, promotion of the benefits, and showcasing outcomes.
Leadership was reported to be fundamental, from both project and group leaders and senior and local management. Future projects need responsive leadership to smooth conflict and energize participants to sustain effort. This approach fits within Bass’s (1990) transformational leadership model. The current project’s leader focused on simple solutions and presenting goals and outcomes clearly, while addressing obstacles. The main role was perhaps holding hope in times of uncertainty (NHS Leadership Academy, 2013). However, the leader could not progress the project without the support of senior and local management, which provided credibility and resources.
Limitations
The first author maintained a role as participant observer. Although field notes were used to triangulate the interview data, participation may have influenced the data collected and its interpretation. This author’s earlier clinical role may have enhanced or limited participants’ responses at interview. These factors were mitigated by researcher reflexivity, independent audit, and respondent validation. Field observations did not contradict the interview data. Given the third author’s significant involvement within the project, measures were taken to limit his influence on the data. For example, he was not involved in data analysis. It was also recognized that participants may recognize each other within the data. However, only quotes relevant to the developing theory, selected sensitively, are included in this article.
Attempts were made to ensure diversity in perspectives, though it is possible that some key stakeholders were missed: for example, those not directly involved in the project but part of the staff team or service user and carer population served by the team. In particular, rather more staff than family members were involved in our interviews. However, there were more staff involved in the EBCD project itself, with only five families having been willing or feeling able to take part. Service users and carers from two of these five families took part in our study. While this small number undoubtedly limited the potential range of experience we could explore, the study did capture multiple perspectives and illustrated both successes and setbacks, potentially enhancing the theory’s helpfulness to others in future EBCD projects of this type.
The EBCD project had not reached completion when the first author had to disengage due to it being her doctoral thesis as part of time-limited clinical psychology training. Therefore, potentially important processes that occurred toward the end may not have been captured. The EBCD project was also conducted, and studied, at a time of major organizational change. Therefore, this theory may be more helpful in relation to difficulties that arise at a time of instability and be less transferable to EBCD projects conducted under more stable circumstances.
Considerations for Clinical Practice
Limited research has explored the processes that help and hinder the implementation of EBCD, especially in mental health and with carers, although the review by Bombard et al. (2018) examined the slightly narrower question of facilitators and barriers to service user engagement in co-design. Therefore, the theory presented here may support future projects to achieve their potential by highlighting key processes for consideration. In the United Kingdom, clinical psychologists could play a helpful role in EBCD. The U.K.’s Division of Clinical Psychology (2010), within the BPS, has outlined the role of clinical psychologists as leaders, highlighting their skills in engagement and collaboration, which appeared to be important in the EBCD project. The project leader needed to bring in multiple stakeholders, hold onto a vision, and sometimes act as “peace negotiator.” Clinical psychologists and other mental health professionals with relevant training understand group dynamics and have leadership and communication skills for supporting co-design groups. Skill in promoting psychological well-being (e.g., BPS, 2008) could help ensure all stakeholders, including staff, are supported throughout the process.
Perhaps, however, mental health professionals may wish to seek those with skills or experience in design to aid the conversion of ideas into simple and workable solutions. Langley, Wolstenholme, and Cooke (2018) suggested that “a designer’s skills and experience” (p. 5) have been removed from EBCD, and they discuss, among other things, how designers can enable tacit knowledge to become explicit and usable. It is worth noting that the EBCD project studied here was led by an art therapist. Arts therapists have skills in enabling their clients to express confusing mental material and thereby understand and use it to overcome difficulties, a process which perhaps corresponds most closely to Gabel and Robb’s (2017) concepts of symbolic expression and embodiment from their review of literature on group art therapy. As is also apparent from Gabel and Robb (2017) and literature on arts therapies more generally (e.g., All-Party Parliamentary Group on Arts, Health and Wellbeing, 2017), many arts therapists are also experienced in working with groups. In addition, working with creativity and playfulness, which requires openness to experience and flexibility, is their modus vivendi.
Future Research
The proposed theory is preliminary. Further research needs to test its validity. In particular, future research should examine an EBCD project with a similar number of stakeholders in a more stable context. The model of EBCD presented here may have applications for other kinds of change projects. The issue of outsourced support groups for carers or service users is something that could be investigated, as such groups may not have sufficient focus on members’ co-design work. Furthermore, complex projects involving a large number of stakeholders in scattered parts of large NHS trusts may be particularly difficult in relation to maintaining lines of communication, and it may require research into innovative ways of tackling this. Finally, research could examine different ways of inducting all stakeholder groups and staff at different organizational levels into the work of EBCD so that they do not unwittingly undermine it or have expectations that cannot be met.
Conclusion
This study presents a preliminary theory of the processes involved in an EBCD project with family carers in community mental health. For a project to be successfully implemented, it needs to fit with both organizational and personal values and attain multiple stakeholder commitment. A mutual understanding of the problem needs to be acquired, supporting the diverse groups to collaborate with a joint aim. Project leaders and co-design group facilitators need to be alert to re-emergence of conflict, and to power dynamics, and provide support to all stakeholders. Projects cannot be sustained if there is not sufficient local leadership, if project aims are perceived as unfeasible, and if the solutions are not simple and readily integrated into clinical practice. EBCD projects can be lengthy, and require motivation to be sustained through communication and perhaps showcasing interim outcomes. Further research is required to assess the broader applicability of the theory presented and to ascertain any difference that arises when conducting a project in a more stable context.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.