
Abstract
Discussions and studies on Ghana’s pluralistic health care system usually ignore or downplay self-care as a crucial sector in this system of care. In view of this, this study uses a triple sector approach of the pluralistic health care system as advocated by Kleinman to assess care-seeking behaviors of residents in the Asikuma-Odoben-Brakwa District (Ghana). The results of cross-tabulation analysis demonstrate that respondents’ general care–seeking behavior is different from the type of care sought for last illness before the study. Data for the study were obtained from 227 urban and rural respondents in the study district in 2013. The findings indicate that factors such as geographic location, health insurance, and perception of the cost of professional care had a bearing on residents’ general care–seeking behavior. However, age, sex, relationship status, economic status, and proximity to nearest biomedical care service influenced the type of treatment sought for last illness. The approach use of the study demonstrates that self-care remains a general avenue of care for residents, whereas in times of severe illness, respondents often rely on professional biomedical care. The use of professional indigenous care services is generally low due to the financial burden associated with its use.
Introduction
The concept of medical or health pluralism is applied loosely in social science research. The concept of pluralistic health environment often differs from studies and research on the subject based on place or location of studies (Amegbor, 2014). Studies in western industrialized societies often use the concept in reference to the parallel existence of a biomedical health care system and other forms of natural and scientific health care (postmodern scientific health care) such as chiropractic, naturopathy, homoeopathy, and aromatherapy (Raffaetà, 2013; Stevenson, Britten, Barry, Bradley, & Barber, 2003; Unschuld, 1980). This conception most often ignores the indigenous health care system of natives such the Aboriginal people of North America, Europe, and Australia. Similarly, in most developing countries, especially sub-Saharan Africa, the concept of medical/health pluralism frequently refers to the existence of western biomedical therapies, and indigenous healing practices and traditions (Digby & Sweet, 2012; Hampshire & Owusu, 2013; Pantelic et al., 2015; Ribera, 2007; Twumasi, 1979). The conception of which healing practices constitute a pluralistic health environment is confined to professional care therapies. However, studies increasingly point to the predominance of self-care and/or home care as the major health care management option for most people in both the developed and developing worlds (Asenso-Okyere, Anum, Osei-Akoto, & Adukonu, 1998; Chenge et al., 2014; Cocks & Dold, 2000; Stevenson et al., 2003). Thus, self-care is not given its due diligence as a vital health care sector, in the discourse on health care systems and medical/health pluralism.
Research and literature on the phenomenon of medical/health pluralism in Ghana usually acknowledge two systems of care—a dual approach (Barimah, 2013; Sato, 2012a; Tabi, Powell, & Hodnicki, 2006; Twumasi, 1979). This dual approach to medical/health pluralism—biomedicine versus the others—shrouds the reality of the health care system of most contemporary societies, as well as treatment-seeking behavior of patients. As indicated earlier, the dual approach downplays the vital role and the predominance of self-care as a major treatment system in any pluralistic health society (Asenso-Okyere et al., 1998; Chipwaza et al., 2014; Danso-Appiah et al., 2010; Kleinman, 1978; Stevenson et al., 2003). Whereas some studies have acknowledged and explored the critical role of self-care in treatment-seeking behavior of patients in Ghana and sub-Saharan Africa, such studies usually do not emphasize this treatment avenue as part of the health care structure. In addition, the use of the dual approach skews reality about patients’ preference and choice of treatment in favor of the alternative and/or traditional medicine (Amoah, Sandjo, Bazzo, Leite, & Biavatti, 2014; Anyinam, 1987a; Dahlberg & Trygger, 2009; Rutebemberwa et al., 2013). This misrepresentation is largely due to confinement of biomedical care to professional and institutional-based care, whereas indigenous/traditional medicine is loosely applied care in professional setting and self-care setting. To tackle these shortfalls and the conceptual challenges associated with the use of dual systems approach, this study adopts a modified version of Kleinman’s model of health care system (Kleinman, 1978) to assess treatment-seeking behaviors of people in the Asikuma-Odoben-Brakwa district of Ghana. In view of this, I use a modified version of Kleinman’s model to assess preference and actual use of professional biomedical, professional indigenous, and self-care forms of health care in addressing acute illness in the Asikuma-Odoben-Brakwa district of Ghana. Furthermore, I synchronize this new modified model of health care system with the existing behavioral model of access and use of health care services to enhance the discourse and knowledge on exiting studies.
The remainder of the study is five substantive sections. The section “A Triple-Systems Model Approach to Medical/Health Pluralism in Ghana” covers the adopted pluralistic health system models and the behavioral model of access to health care. It further discusses the logic in blending the two models into a new model of access and use of health care services with a pluralistic outlook. The section “Study Context” gives the context of the study area and rational for choosing it. The section “Method and Data Analysis” explains the methods of data collections, techniques of sampling, measures of study variables, and statistical analyses used. The section “Results” presents a summary of the results of the descriptive, bivariate (cross-tabulation), and the multinomial logistic regression models generated from the study data. The section “Discussion” critical discusses the findings in relation to the conceptual framework and existing literature on the subject. It further delves into the limitations of the study. The “Conclusion” section discusses the implication of the study and the model for future research and discourse on health-seeking behavior in pluralistic health environment
A Triple-Systems Model Approach to Medical/Health Pluralism in Ghana
The Ghana health care system such as many contemporary systems of care is usually described as pluralistic in practice and approach (Abel, Busia, & Med, 2005; Aikins, 2002; Aikins, Boynton, & Atanga, 2010; Tenkorang, 2016). As a whole, the health care system is characterized by a diversity of health knowledge, beliefs, and practices. Ghanaians use a plethora of cures and remedies to treat and meet their everyday health care needs (Amegbor, 2014; Gyasi et al., 2016). Nonetheless, these remedies for treating acute illnesses and complex health conditions are drawn from two main medical traditions: biomedical and traditional (indigenous). Whereas the former system of care was introduced into the country through Christian missionary activities and colonialism, the latter is embedded in the socioculture orientation of Ghanaian societies (Hampshire & Owusu, 2013; Twumasi, 1979, 1981). Researchers are often been intrigued by the parallel traditions of these medical systems, yet their integration by patients in addressing health problems (Aikins, 2003; Kroeger, 1983; Moshabela, Schneider, Silal, & Cleary, 2012; Sato, 2012b). The phenomenon is termed as “healer shopping” (Aikins, 2005; Kroeger, 1983). A large volume of literature exists on the predominant use of the indigenous medical system and its remedies (Albertyn, Berg, Numanoglu, & Rode, 2015; Anyinam, 1987a; de Wet, Ramulondi, & Ngcobo, 2016; Good, 1987; Pouliot, 2011; Tabi et al., 2006; Twumasi, 1979). However, the biomedical health care system has a monopolistic hold as the official and legally sanctioned medical system in Ghana and many other sub-Saharan Africa countries (Amegbor, 2014).
Reports estimate that more than 60% to 80% of Ghanaians and residents of other sub-Saharan Africa countries use indigenous medical remedies in meeting their everyday health care needs (McFarlane, 2015; Thorsen & Pouliot, 2016; Vadi, 2007; WHO, 2002). It is widely acknowledged that access to biomedical health care remains elusive to many patients, especially the poor and rural dwellers in Ghana and the subregion (Aikins & Marks, 2007; Helmchen & Lo Sasso, 2010; Powell-Jackson, Hanson, Whitty, & Ansah, 2014). Scholars and researchers criticize the structure of biomedical care, and opine its inability to reach the mass is due to social distance, economic and financial constraints, and the uneven distribution of health and medical resources in this part of the world (Haddad, Makin, Pattinson, & Forsyth, 2015; Harris et al., 2011; Jørgensen, 2008; Kissah-Korsah, 2008; Mills et al., 2012). For instance, research in the 1980s and early 1990s observed a drastic fall in the use of biomedical care among Ghanaians due to the introduction of user fees during the structural adjustment era (Anyinam, 1994; Asenso-Okyere et al., 1998; Nyonator & Kutzin, 1999). Interestingly, this period coincided with global acknowledgment of indigenous medical practices and their role in promoting access primary health care, as well as, improving overall health (Gilbert & Gilbert, 2004; Green & Makhubu, 1984; Ndhlala, Stafford, Finnie, & Van Staden, 2011). During this period, Ghana passed several decrees and laws aimed at regulating and ensuring the safety of indigenous medical practices (Romero-Daza, 2002). These legislations, as well as efforts to integrate the indigenous healing system into the national health care system, contributed to the transformations of the indigenous medical practices (Anyinam, 1987b; Romero-Daza, 2002). Hitherto, the indigenous medical practices were usually noncommercial communal-based healing systems, and hence were described as affordable, culturally acceptable, and physically close to it users (Ae-Ngibise et al., 2010; Anyinam, 1987a; Muela, Mushi, & Ribera, 2000). For instance, some studies assert that in some communities, money or paying for health destroys the potency of the medicine (Bierlich, 1999; van der Geest, 1992). These policies and licensing of indigenous medical practitioners coupled with direct out-of-pocket payment for biomedical care provided an ideal incentive for professionalization of healers through setting of standards (Janes, 1999). The end result was the commodification of some aspects of the indigenous healing practices, particularly herbal and plant medicine (Flint, 2001; Han, 2001; Hsu, 2009).
The commodification of indigenous medical care systems created a professional body of healers whose activities are highly formal and commercially oriented. Thus, the current indigenous medical care system is not as that purported by early researchers, such as Anyinam (1987a), Good (1987), and Twumasi (1975). In addition, certain key policies such as the introduction of a national risk-pooling health insurance scheme and community health posts (CHPs) in deprived rural areas have changed the landscape of access to biomedical health care (Aryeetey et al., 2013; Fenenga et al., 2015; Jehu-Appiah et al., 2011). For instance, the National Health Insurance Scheme (NHIS) aims to mitigate direct out-of-pocket payment for biomedical health care, thus reducing the financial burden and constraints of Ghanaians especially the poor and vulnerable (Gobah & Zhang, 2011; Witter & Garshong, 2009). Likewise, the introduction of community-based health planning and services (CHPS) seeks to reduce geographical distance between people in deprived communities and biomedical care services, as well as, foster an inclusive program of community-based health services (Akazili, Garshong, Aikins, Gyapong, & McIntyre, 2012; Fenny, Asante, Enemark, & Hansen, 2015; Kuuire, Bisung, Rishworth, Dixon, & Luginaah, 2015). The CHPS health centers in these deprived communities are crucial for primary health care needs while district- and regional-based hospitals and clinics provide secondary services to residents in times of urgent need (Fenny et al., 2015; Tawiah et al., 2016). Studies have explored how these transformations are improving or affecting access to health care, albeit this has not been done as a pluralistic health system perspective. The continued use of a dual health care systems approach to analyze treatment-seeking behaviors of Ghanaians (Jørgensen, 2008; Kissah-Korsah, 2008; Sato, 2012a), as well as a mono-care systems approach (either biomedical or indigenous care; Gyasi, Mensah, & Siaw, 2015), shrouds the current reality of the health scape in Ghana.
To mitigate these challenges while acknowledging the transformations that have characterized both the biomedical and indigenous health care systems in Ghana, this study adopts a modified version of Kleinman’s (1978) model of health care systems in a pluralistic society. In his model, Kleinman argues that the health care system in a pluralistic environment comprises of three overlapping parts: the popular, the professional, and the folk sectors (Kleinman, 1978; Stevenson et al., 2003). The popular sector refers to informal care and treatment in the family or home context, including social network and community activities (Kleinman, 1978). The professional sector comprises professional healers in the scientific (biomedical) and indigenous healing traditions, while the folk sector is a nonprofessional healing specialist often classified into secular and sacred groups (Kleinman, 1978). In his work, he acknowledges those studies that overemphasize the folk sector while playing down the popular sector. This assertion highlights the neglect of the popular sector in pluralistic health care system discourse. Although this model is more than three decades old, compared with the dual model (posited by Good, Hunter, Katz, & Katz, 1979, & Twumasi, 1979), it accurately and adequately reflects the current Ghanaian health care system.
In this study’s model (Figure 1), the popular sector is conceptualized as the self-care sector of the Ghanaian health care system. Like Kleinman’s popular sector, the self-care is a nonspecialist popular arena of the Ghanaian health care system, where disease and illness are first identified, defined, and decision on treatments is made. The use of self-medication or self-treatment as the first health care option for patients is not only peculiar to Ghanaians or residents of sub-Saharan Africa (SSA) (Bussing, Koro-Ljungberg, Williamson, Gary, & Wilson Garvan, 2006; Chung et al., 2011; Ramdas, 2012; Stevenson et al., 2003). A large volume of literature points to the large proportion of patient’s in western industrialized nations and other parts of the global south who depend on this sector for their basic health care need (Paterson et al., 2012; Stevenson et al., 2003). In Ghana, studies indicate that a large section of the Ghanaian population heavily rely on this form of treatment for common illness such as malaria, fever, pains, and aches. The treatment of diseases and illness in this sector involves the use remedies, drugs, and treatment resources from both the biomedical and indigenous medical systems (Beiersmann et al., 2007; Chipwaza et al., 2014; Tabi et al., 2006). Existing literature on health-seeking behavior in Ghana and other parts of SSA reports the use of biomedical drugs for self-medication, especially pain killers purchased from “chemical/drug stores” (Asenso-Okyere et al., 1998; Dzator & Asafu-Adjaye, 2004; Febir et al., 2016; Goodman et al., 2007; Goodman, Kachur, Abdulla, Bloland, & Mills, 2009; Kassam, Collins, Liow, & Rasool, 2015). For instance, a recent study by Febir et al. (2016) reveals that members in the study community purchased drugs they deemed appropriate from drug stores for their perceived health condition or alternatively relied on the advice of the vendor. The study similarly noticed the use of herbal preparation or left over pharmaceutical drugs from previous illness for treatment.

Study’s conceptual framework.
Furthermore, the study’s model distinguishes between professional care in a biomedical care and indigenous care settings. This distinction is appropriate given the health care system in Ghana has not formally integrated healers from biomedical and indigenous health care system. The system of integration in Ghana is what Stepan (1983) terms the tolerate system. This system of integration gives legal recognition to scientific-based indigenous medical practices or remedies such as herbal medicine, while the nonscientific aspects are tolerated by the law. However, the Chinese health care system, which was the context of Kleinman’s study, has a formal integration of traditional Chinese medicine and biomedical treatment—that is an inclusive system of pluralistic health care integration (Kleinman, 1978; Stepan, 1983). Thus, the professional biomedical health care sector in this model refers to the official legally backed health care system in Ghana. Care and treatment in this sector are provided by professionals such as physicians, nurses, midwives, and surgeons who are trained in formal education systems. In addition, care and treatment are provided in hospitals, clinics, or CHPs (Fenny et al., 2015). The professional indigenous care sector as used in this model refers to both licensed and communally recognized indigenous healers including faith healers whose activities are generally commercially oriented. As noted earlier, although some indigenous healers and their practices are licensed and recognized by law, they are not part of the formal health care structure, and hence their separation from biomedical professionals.
In furthering current understanding on care-seeking behaviors in a pluralistic health environment, the study synchronizes the triple systems approach of Kleinman and Buor’s behavioral model of health care access and utilization. Buor’s (2003) behavioral model of health care utilization (Buor, 2003) is an improvement of Andersen’s behavioral model. Andersen’s model generally recognizes three group factors (predisposing, enabling, and need) that influence patient’s access and use of health service (Aday & Andersen, 1974; Andersen, 2008). In addition to these three broad factors, Buor’s model incorporates spatial characteristics, provider characteristics, and restrictive factors (combination of government policy that determines service, location, and distance of coverage) to the list of factors that influence and determine user’s behavior (Buor, 2003, 2004). The model opines that the use of health care services is dependent on broad socioeconomic, spatial, health, and provider characteristics operating in an organized user environment (Buor, 2003). The model used in this study does not exhaustively include all factors identified by Andersen and Buor as influences of patient’s health-seeking behavior. Nevertheless, the model includes key geographical, sociodemographic, economic, and restrictive factors (health financing and cost of care).
Study Context
The study district, Asikuma-Odoben-Brakwa, is located in the north-central portion of the Central Region of Ghana. With a total land cover area of 884.84 km2, it lies between latitude 5° 51″ and 5° 52″, and longitude 1° 50″ and 1° 5″ West. The district lies in the moist semideciduous rainforest vegetation cover of Ghana; hence, agriculture is the predominant occupation. It is currently estimated that agriculture employs for 65% of the district’s labor force (Ghana Statistical Service [GSS], 2014a). In addition, about 52% of the population engaged in other economic activities engage in agriculture as a secondary occupation (GSS, 2014a). The study district has an estimated population of 112,706 per Ghana’s 2010 Population and Housing Census (GSS, 2012), of which 48.2% are males and 51.8% are female. Like most rural Akan communities, household units in the district are still traditional; that is, extended family members often live in the same housing units (popularly termed compound houses). Individual family dwelling or nuclear family household systems account for a third (33.4%) of the total household number in the district (GSS, 2014a). In addition, there are more females per household than males.
The district is characterized as the most deprived district in the Central Region according to the 2006 Ghana Health Service regional report (Ghana Health Service, 2007). Current national and regional public health policy planning coupled with the distribution of health care facilities in Ghana are largely urban biased and hence neglect or do not favor most rural communities including Asikuma-Odoben-Brakwa district. The entire district is served by one hospital, two clinics, and 10 CHPs. These facilities are manned by nine medical officers, six medical assistants, with the help of 23 midwives, 18 staffed nurses, 12 enrolled nurses (student nurses), and eight public health nurses. Furthermore, the main hospital—Our Lady of Grace Hospital—also serves surrounding communities and districts, which places an undue burden on the limited human resources in the facility, resulting in long waiting hours for most patients (Amegbor, 2014). For instance, the ophthalmology clinic in the district hospital (Our Lady of Grace) is the main eye care facility serving the district and more than five surrounding and nearby districts such as Assin North and South districts, Agona East and West districts, Ajumako-Enyan-Essiam district, and the Gomoa districts (Abokyi, Koffuor, Abu, Kyei, & Abraham, 2012).
Coupled with these health care provision challenges, the district has one of the highest major population growth indicators as well as mortality cases in the region (GSS, 2014b). For instance, the total fertility rate is 4.68 (the highest in the region), whereas deaths in household and crude death rates are 1,114 and 9.88, respectively (GSS, 2012, 2014a). In addition, borehole, pump, and tube well constitute major sources of drinking water (37.8%), with an additional estimated 18.2% of households resorting to rivers and streams for their water consumption supply (GSS, 2014a). These health and development challenges make the district an ideal location to assess health care usage behavior in a pluralistic framework that incorporates self-care/home-care (nonprofessional administered care).
Method and Data Analysis
The primary data used in this study are from a cross-sectional survey conducted in the Asikuma-Odoben-Brakwa district of Ghana between June and July 2013. The survey was conducted in relation to an MPhil thesis on health-seeking behavior in a pluralistic health care environment. The survey solicited the views and responses of 227 respondents in three communities—Asikuma, Bedum, and Fosuansa—in the district. These communities were selected through a cluster area and lottery sampling techniques. Recognizing intraregional differences in the study district in terms of population size and social amenities allocations, that is, the degree of urbanity, I grouped the communities in the district into three settlement categories—urban areas, semiurban or semiurban areas, and rural areas. The list of the communities in the district was obtained from the district assembly planning office, and the help of the planning officer was sought in determining which communities fit the set categories based on the district planning agenda. This was also complemented with the criteria for rural–urban classification used by GSS—population size and predominant occupation. Thus, communities with a population size of 10,000 or more were placed in an urban category, while those with a population of 6,000 and below were placed in the rural category. I proceeded with using lottery sampling technique to draw one potential data collection site from the urban category (there were only three communities in this category), and two potential data collection sites from the rural category. The target population for the study was all persons aged 18 years or above in the three selected communities—Asikuma (urban community), and Bedum and Fosuansa (rural communities). In each cluster, an adult aged 18 or older in a randomly selected household or workplace was sampled to answer a face-to-face survey administered.
Ethical approval for this study was obtained from the Department of Sociology and Human Geography, University of Oslo, and the supervisor for the MPhil project. With the help of the district coordinator and the district planning officer, a daylong training session on the survey administration and research ethics was conducted for the two research assistants on the premises of the district assembly office. Data gathering at each site was done concurrently between me and one research assistant to ensure adherence to ethical standards and sampling techniques. In the data collection site, a household was randomly selected and an adult aged 18 years or above was sampled for a face-to-face survey administration. In Asikuma, household sampling was interlaced with offices and trading posts, given the administrative function of the location as the district capital and the major market hub. That is, some potential respondents for the survey on this site were mostly likely to be in their offices or trading sites during the time of administering the survey. The purpose of the survey was explained to each respondent, and their right to withdraw from the survey (including any information divulged) before, during, and after the survey was made known to them.
Measures
The focus of this study was on the health-seeking behavior of respondents in a pluralistic health care environment, modeling self-care or home-care as a health care alternative. The search for respondents’ health-seeking behavior was not confined to last illness, as a health care option used for a recent episode of illness may not be a true reflection of normal health care–seeking behavior. Thus, respondents were asked to identify the predominant form of care they use in addressing their health care needs, as well as, the treatment used for last illness. The former allows for an assessment of the general health care–seeking behavior of the respondent, whereas the latter assesses recent health care–seeking behavior, which may or may not be similar to the general behavior. The dependent variables for this study were obtained from two prime questions: What is the preferred or usual choice of treatment for your health care needs? and What type of care was sought for the last episode of ailment? Both questions had three response categories: professional biomedical care, professional indigenous medical care, and self-care. These responses were created from an original response list: hospital, clinic, CHP compound, drug store, traditional healer, prayer camp, herbal clinic, and self-medication. Care sought in hospitals, clinics, and CHP compounds was coded as professional biomedical care; care sought from a traditional healer, prayer camps, and herbal clinics was coded as professional indigenous medical care; and care sought by the use of drug store and self-medication was coded as self-care. The term professional is attached to biomedical and indigenous care to distinguish them from the use of biomedical or indigenous remedies in a self-care context. Thus, professional care as used in this study refers to licensed and legally sanctioned biomedical and indigenous medical care services. However, in the case of the latter (indigenous medical care), the term is loosely applied to embrace “professional care” provided by faith healers, spiritualists, and diviners whose activities may or may not be legally sanctioned. These indigenous professional healers charge patients for their services either in cash or kind. These responses represent the conceptualized systems of care in a pluralistic health care environment.
The choice of independent variables for this study was informed by an adopted behavioral model of health care utilization. This model was adopted due to its acknowledgment of geographical (spatial setting), socioeconomic, and health policy dynamics (such as the distribution of health resources, health insurance, and cost of services) as vital factors that determine the use of health care services. Thus, basic sociodemographic characteristics, place of residency, perception on distance to nearest professional care facilities, as well as respondents’ perceptions of their economic status, and the relative cost of professional care, were used as independent variables. Sociodemographic variables such as age, sex, highest level of education, and relationship status were selected as independent variables for statistical analysis. Economic indicators such as the type of employment and perceived economic status were also used as independent variables. The question on type of employment had two categories: formal sector and informal sector. Similarly, respondents’ perception of their economic status had two categories: okay and not okay. Respondents were asked about their NHIS status and they were to choose either yes (for registered member) or no (for nonregistered member). Respondents were also asked about their perception of which professional care was relatively costly based on their personal experience or that of a close social relation: professional biomedical care and professional indigenous care. Whereas respondents were not asked for their place of residence, the questionnaires distributed in each sampled data site were coded as Asikuma = 001, Bedum = 002, and Fosuansa = 002. The coding 001 signifies an urban location while 002 signifies a rural location, thus, helping to determine whether the respondent was an urban or a rural dweller.
Data Analysis
The study used three levels of statistical analysis—descriptive, bivariate, and multivariate—to assess the relationship between general and last illness care–seeking behaviors, and relevant independent variables identified above. The data were analyzed using STATA statistical software (version 13). A chi-square test of independence was used to determine the association between the study’s dependent variables and independent variables. The strength of this relationship was then determined using Cramer’s V test. Furthermore, a multinomial logistic regression model was used to examine the influence of the selected independent variables on the choice and the use of professional biomedical care, professional indigenous medical care, or self-care as general care–seeking behavior and last illness care–seeking behavior. This analytic technique was selected for computing because both dependent variables and their responses are categorical with no inherent order.
The first multivariate logistic test (Model 1) used respondents’ general care–seeking behavior as the dependent variable, whereas the second test (Model 2) used the type of treatment sought for in the last episode of illness as the dependent variable. The models report the relative risk ratio (RRR) and the standard error.
Results
A general summary of the study is presented in Table 1. A significant proportion of the study’s respondents were female rural residents aged between 18 and 50 years (56.8%, 55.1%, and 66.1%, respectively). In addition, a relatively high proportion of this study’s respondents were either married or in a form of a union and had no formal education or only basic education (59.0% and 67.0%). Most respondents also indicated being employed in the informal sector (75.8%) and viewed their economic status as being okay (72.7%). In terms of health insurance coverage, a highly significant number (72.7%) of this study’s respondents were registered members of the national risk-pooling insurance scheme (the NHIS). This nation-wide health insurance scheme is limited to only hospital or biomedical based care. Notwithstanding, a sizable proportion of the respondents still viewed professional biomedical care (i.e., care sought in established health care facilities) as being costly (40.5%). However, the majority (59.5%) were of the view that professional indigenous care is relatively costlier than biomedical-based care. Furthermore, a relatively higher proportion of respondents surveyed (75.8%) were of the view they were in close proximity to the nearest professional biomedical care services compared with professional indigenous care services (55.5%). The result for care-seeking behavior of this study’s respondents reveals a sharp contrast between the general health care behavior and the care-seeking behavior for the last episode of illness suffered by the respondent. In the case of the former, a little above half (52.9%) of respondents indicate the use of self-care as the general health care behavior. However, in terms of the type of care sought for their last illness, most respondents (61.2%) indicated seeking professional biomedical-based care either in the hospital, the clinic, or from a CHP compound. Interestingly, the proportions of respondents using professional indigenous care as both general care–seeking behavior and last illness care–seeking behavior were significantly low (4.8% and 18.1%, respectively)
Descriptive Summary of Study Variables (n = 227).

Note. PBC = professional biomedical care; PIC = professional indigenous care; NHIS = National Health Insurance Scheme (Ghana).
Findings of Bivariate Analysis
In determining the relationship between respondents’ health care–seeking behaviors on one hand and their sociodemographic, economic, geographic, and health financing and cost on the other, I compute a series of cross-tabulation tests (Table 2). These tests set the premise for the multinomial logistic regression models that follow. A relatively higher proportion of respondents in urban and rural areas (55.9% in the urban location and 50.4% in the rural locations) generally indicate self-care as their general care–seeking behavior as compared with professional biomedical care and professional indigenous care. Interestingly, in the two geographical locations, professional indigenous care as the general care option is significantly low (1.0% and 8.0% of urban and rural respondents, respectively). There is a weak statistically significant relationship between respondents’ place of residence (urban and rural) and the type of treatment they indicate as their general care–seeking behavior (p < .05, V = .163). In addition, a higher proportion of the respondents, who perceived both professional biomedical and indigenous care services as being close, indicate self-care as their general care–seeking behavior (55.2% and 56.3%, respectively). Respondents in all sociodemographic categories, except those who have attained secondary education or higher, indicate self-care as their general care–seeking behavior. A higher proportion of respondents who have attained secondary education or higher (50.7%) indicate professional biomedical care as their general care–seeking behavior compared with self-care and professional indigenous care (45.3% and 4.0%, respectively). None of the variables in the sociodemographic category had a statistically significant relationship with general care–seeking behavior.
Cross Tabulation of Independent Variables and Care-Seeking Behaviors (Row %).

Note. PBC = professional biomedical care; PIC = professional indigenous care; NHIS = National Health Insurance Scheme (Ghana).
p < .05.
Similarly, a higher proportion of respondents employed in the formal sector indicate professional biomedical care (50.9%) as their general care–seeking behavior compared with those in the informal sector who indicate self-care (54.1%). Overall, respondents irrespective of their perceived economic status indicate self-care as their general care–seeking behavior. Both economic variables did not have a statistically significant relationship with general care–seeking behavior. Membership in the NHIS and perception of the cost of professional care on one hand, and general health–seeking behavior on the other had statistically significant relationships (p < .05). A little above half (50.3%) of the respondents who are registered and active members of the NHIS indicate professional biomedical care as their general care–seeking behavior. Interestingly, respondents who indicate professional biomedical care and professional indigenous care as being costly indicate self-care as their general care–seeking behavior (51.1% and 54.1%, respectively). The test of the strength of an association indicates that there is a strong level of association between NHIS membership and general care–seeking behavior (V = .350), whereas that between respondents’ perception of the cost of professional care– and general care–seeking behavior is weak (V = .191). In general, the percent of respondents who indicate the use professional indigenous care as their general care–seeking behavior is significantly small, ranging between 1.0% and 14.5% (in all independent variables)
A cross-tabulation computation between respondents’ last illness care–seeking behavior and the independent variables shows that, in all categories, a higher proportion of respondents used professional biomedical care. Nevertheless, a chi-square test of association reveals only perceived proximity to nearest professional biomedical care service, age, and sex had statistically significant relationships with last illness care–seeking behavior. Both proximity to nearest professional biomedical care and sex had a weak statistically significant association with respondents’ last illness care–seeking behavior (V = .163 and V = .183, respectively; p < .05). Age as an independent variable had a moderate statistically significant relationship with the type of care sought for last illness (p < .05, V = .253). In contrast to general care–seeking behavior, the use of professional traditional care varies across all the responses for the independent variables (Table 2).
Findings of Multinomial Regression Models
Two models were built to assess the relationship between respondents’ socioeconomic, geographical, and health care cost and financing characteristics on one hand, and their health care–seeking behaviors on the other. As stated previously, the results of the cross-tabulation test informed these multinomial regression models. The two models (Table 3) strengthen the bivariate cross-tabulation findings in predicting the health care–seeking behaviors of respondents in different socioeconomic, geographic, and health care cost and financing. The interpretations of the RRR for the multinomial logistic regression models are in reference to the base outcome of using or selecting self-care as the general and last illness care–seeking behavior. The first model (Model 1) examines the relationship between general care–seeking behavior and the socioeconomic, geographical, and national policy characteristics. In Model 1, NHIS members as compared with nonmembers were three times more likely to select professional biomedical care as general care–seeking behavior rather than self-care (RRR = 3.336, p < .01), controlling for all other factors. In addition, urban residents as compared with their rural counterparts were less likely to select professional indigenous care as their general care–seeking behavior (RRR = 0.079, p < .1). Residents who were of the opinion professional biomedical care was relatively expensive compared with professional indigenous care were nearly six times more likely to indicate professional indigenous care as their general care–seeking behavior rather than self-care (RRR = 5.844, p < .05), controlling for all other factors. Overall, the model was statistically significant and the predictor variables used in the model accounts for 25% of the variance in the general care–seeking behavior.
Relative Risk Ratio of Using Self-Care in General Care–Seeking Behavior in AOB District.
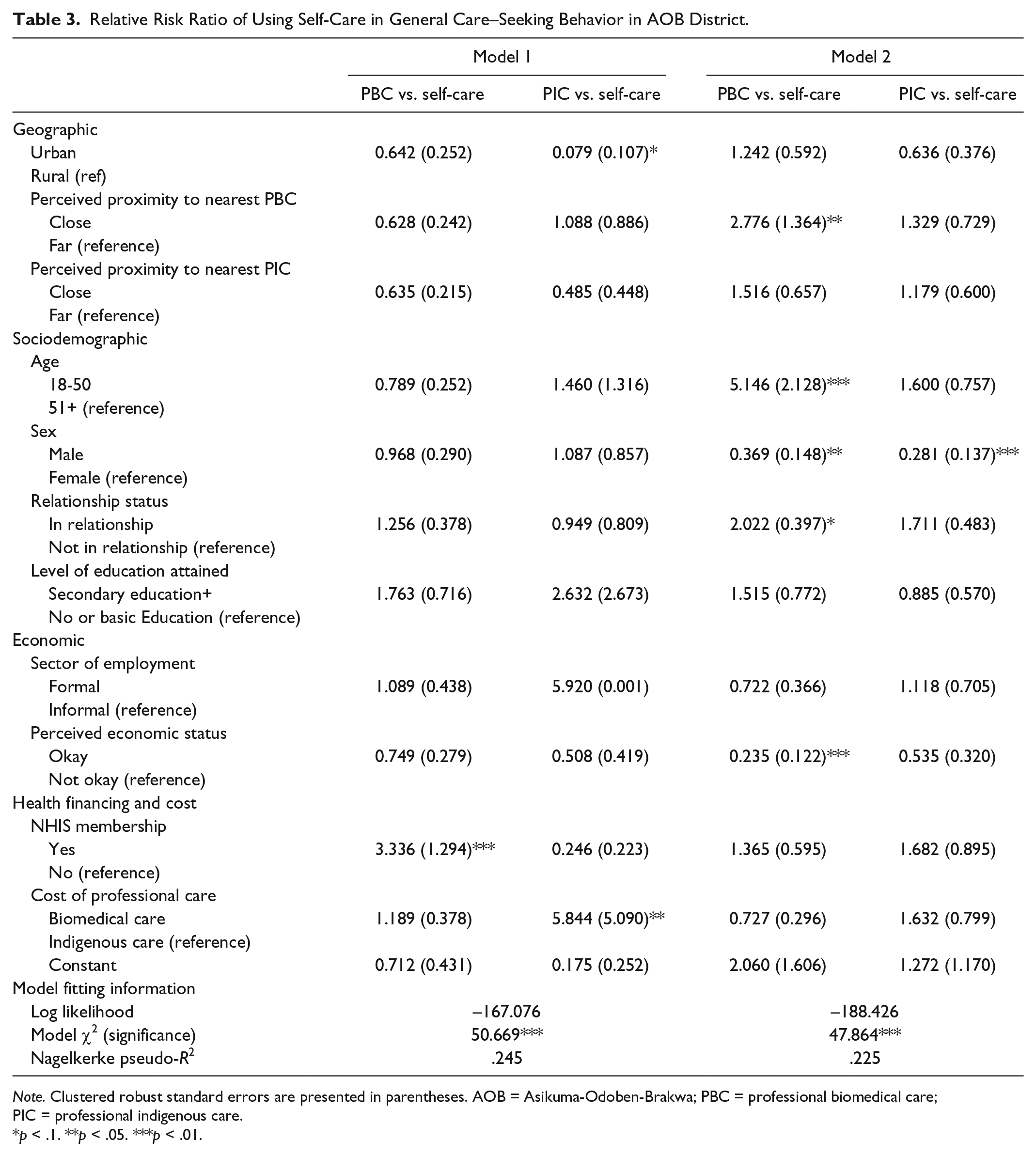
Note. Clustered robust standard errors are presented in parentheses. AOB = Asikuma-Odoben-Brakwa; PBC = professional biomedical care; PIC = professional indigenous care.
p < .1. **p < .05. ***p < .01.
Model 2 examines the relationship between the type of treatment sought for last illness (last illness care–seeking behavior), and socioeconomic, geographic, and health care and financing characteristics. The results of the test show that residents who perceive professional biomedical care being close, as compared with those who view it as far, are nearly three times more likely to have used professional biomedical care rather than self-care for the last illness they experienced prior to the study (RRR = 2.776, p < .05). In addition, residents aged 18 to 50 years (compared with those aged 51 years and above) are five times more likely to have used professional biomedical care rather than self-care for the last illness experienced (RRR = 5.146, p < .01). Males compared with females are almost 63% less likely to have used professional biomedical care rather than self-care for the last illness experienced prior to the study (RRR = 0.369, p < .05). However, individuals in a relationship as compared with those not in a relationship are twice more likely to have used professional biomedical care rather than self-care in treating the last illness they experienced prior to this study (RRR = 2.022, p < .1). People who perceive their economic status as okay compared with those who viewed their status as not okay were 76% less likely to have used professional biomedical care rather than self-care for the last illness suffered before the study (RRR = 0.235, p < .01). Comparing the use of professional indigenous care to self-care, males in relation to females were almost 70% less likely to have used the former care option (RRR = 0.281, p < .01)
Discussion
The goal of this study was to examine health-seeking behavior of residents in Asikuma-Odoben-Brakwa district of Ghana from the context of a pluralistic health care system. Generally, the findings of this study demonstrate that the general care–seeking behavior of residents in the study district contradicts their treatment-seeking behavior for the last illness they experienced prior to this study. Whereas residents usually tend to self-medicate, most of the residents sought care from a professional biomedical care center for their last illness. The difference in general health–seeking behavior and the type of treatment sought for last illness can be understood from both health and socioeconomic perspectives. In the case of the former, numerous studies in Ghana indicate that patients mainly delay in seeking treatment from professional healers for their bad health (Ahorlu, Koram, Ahorlu, De Savigny, & Weiss, 2006; Asenso-Okyere et al., 1998; Getahun, Deribe, & Deribew, 2010). Patients tend to self-care for illness they perceive less chronic; remedies used in the self-care context include both biomedical drugs and traditional herbal medicine. For instance, numerous studies on malaria care–seeking behavior in Ghana indicate that the poor and vulnerable usually delay in seeking treatment for this prevalent disease (Ahorlu et al., 2006; Amexo, Tolhurst, Barnish, & Bates, 2004; Tolhurst & Nyonator, 2006). The delay in seeking professional care results in high mortality cases attributed to the disease (Dzator & Asafu-Adjaye, 2004; McCombie, 2002). Whereas access to biomedical care and patient’s perception on the severity are noted as contributing to delay in seeking treatment, cost of care and inability to pay for professional health care are the major reasons for patients’ delay in seeking professional care (Asenso-Okyere & Dzator, 1997; Kolling, Winkley, & von Deden, 2010; Russell, 1996).
The influence of economic and financial factors on residents’ care–seeking behavior is evident from the findings of this study. Cross-tabulation computation of the study variables shows that residents with secondary education or higher, employed in the formal sector, and active members of the NHIS tend to use professional biomedical care as their general care seeking option (50.7%, 50.9%, and 50.3%, respectively). The inability of the poor and marginally poor to pay for treatment contributes to their delay in seeking cure for acute health conditions, hence the use of self-medication (Ahorlu et al., 2006; Ansah et al., 2009; Carrillo et al., 2011). The decision to seek professional care is made when the disease or illness deteriorates (Ansah et al., 2009; Kiwuwa, Charles, & Harriet, 2005; Mugisha, Kouyate, Gbangou, & Sauerborn, 2002) and, even in such situation, they usually borrow money or pawn their goods to pay for care (Aikins, 2005; Amexo et al., 2004; Asenso-Okyere & Dzator, 1997). In addition, the findings of these studies such as many others reveal that policy interventions in the biomedical health care system such as the NHIS has improved access and use of professional care in this sector of Ghana’s health system (Blanchet, Fink, & Osei-Akoto, 2012; Fenny et al., 2015; Tawiah et al., 2016). Notwithstanding, registered members of the NHIS still face fiscal burden in their use of biomedical services. The heavy financial burden on registered members mainly emanates from payment for prescribed drugs (Dalinjong & Laar, 2012; Witter & Garshong, 2009). Whereas physician consultation may be free or less expensive for members under the scheme, the drug coverage of the scheme is highly inadequate (Dalinjong & Laar, 2012). Existing studies on Ghana’s NHIS as well as other’s in the subregion indicate that registered members complain about the need to pay for most of their prescription drugs (Abdou Illou, Haddad, Agier, & Ridde, 2015; Beogo, Huang, Drabo, & Yé, 2016). This contributes to the significant number (48.5%) of registered members who selected self-care as their general care behavior. In view of such challenges, it is acknowledged that it is difficult to isolate health insurance as the key factor influencing the use of biomedical services (Fenny et al., 2015).
Although the indigenous health care system is becoming increasingly commercialized, currently there is no existing policy that relieves its users of the financial burden they face. The NHIS does not cover indigenous medical care; hence, patients using this professional system of care pay directly out of pocket (Barimah, 2013; Sato, 2012a). This heavy financial burden may have contributed to the lower proportions of respondents who indicate its use as a general care–seeking behavior and as care sought for last illness (Table 2). Likewise, the financial burden of using professional indigenous medical care may account for the low RRR of residents in an urban settlement, indicating this treatment option as their general care–seeking option compared with self-care (RRR = 0.079, p < .1). It is generally recognized that the cost of treatment in urban areas tends to be higher than rural areas (Romay-Barja et al., 2015). In addition, professional indigenous healers in the rural areas may be less commercially oriented due to high levels of close social relations among rural residents compared with the anonymity of urban life (Bierlich, 1999; Muela et al., 2000; Stromberg, 1975). In view of the heavy financial burdens Ghanaians face using the professional indigenous health care sector, some researchers advocate for the need to include traditional healers (especially licensed or registered healers) as service providers in the country’s NHIS (Barimah, 2013). The commodification of some aspects of the indigenous health care system through professionalization of healers (licensing) and regulations has saddled patients and nonpatients with the financial burden that once inhibited a large number of Ghanaians from using biomedical care (Asenso-Okyere et al., 1998; Asenso-Okyere & Dzator, 1997; Dzator & Asafu-Adjaye, 2004; Nyonator & Kutzin, 1999).
Whereas self-care or self-medication remains a popular treatment-seeking avenue for general care behavior, the use of professional biomedical care for severe or chronic, as well as, other acute illness remains popular among residents in the study district. This finding challenges long-held assertion that biomedical care remains highly unpopular among Ghanaians and people in sub-Saharan Africa (Ae-Ngibise et al., 2010; Good et al., 1979; Leslie, 1980; Tsey, 1997). It is worth noting that other studies have similarly acknowledged the popularity of biomedical remedies and therapeutic drugs among younger people (Asenso-Okyere et al., 1998). The second model (Model 2) of this study confirms this intergenerational gap in the use of biomedical care. The relative risk of the young (18-50 years) seeking professional biomedical care for their last illness as compared with self-care is more likely by a factor of 5.146 (p < .01), all else being equal (Table 3). There is the gendered aspect in the use of professional biomedical care, as males are less likely than females (RRR = 0.369, p < .05) to have sought professional biomedical care rather than use self-care for the last illness experienced prior to this study. Likewise, males are less likely to have sought professional indigenous care for the last illness they experienced before this study (RRR = 0.281, p < .01). Studies by de-Graft Aikins and Sato demonstrate the preference for biomedical care in the initial stages of professional care (Aikins, 2005; Sato, 2012b). For instance, in the case of the latter’s study, the use of indigenous medicine was relatively low at the first recourse of treatment, while it doubles or triples in the second stage (Sato, 2012b). Thus, professional biomedical care, contrary to popular belief, is widely accepted by Ghanaians. However, patients often seek professional indigenous care for diseases and illness that could not be treated with biomedicine (Aikins, 2002, 2005; Aikins et al., 2010; Sato, 2012b).
In addition, the changing socioeconomic structure of Ghana influences the use of biomedicine and indigenous medicine. In his study on the role of socioeconomic status on the use of biomedicine and indigenous medicine, Sato (2012a) notes that rising income is associated with the increasing use of the former and the decreasing use of the latter (indigenous medicine). From the study’s model, the relative risk of using professional biomedical for the last illness experienced by residents who perceive their economic status as okay compared with the poor, is less likely by a factor 0.235 (p < .01), all else being equal. This finding is counterintuitive to Sato’s assertion. However, factors such as time spent seeking for care and existing social security program for the poor may explain the difference. Individuals who are economically active are less likely to trade off their economic activity for professional care in acute health conditions (Buor, 2004). In addition, the NHIS provides exemptions for individuals without adequate financial resources to pay the premium (Aryeetey et al., 2013; Durairaj et al., 2010a; Jehu-Appiah et al., 2011). Although this strict income norm of exemption excludes the marginally poor, existing social intervention programs by international and local civil society organizations such as International Labour Organisation (ILO) and local nongovernmental organizations (NGOs) have helped this category of Ghanaians to pay for the NHIS premium (Durairaj, D’Almeida, & Kirigia, 2010a, 2010b). These financial interventions may account for the relatively high use of professional biomedical care by the residents in the study who perceived their economic status as poor.
The effect of distance on patients’ treatment-seeking behavior is well noted in geographic and social science research. Distance as a barrier to access and use of health care services is not only confined to physical proximity but also pertains to the ability to overcome the cost of travel in getting to treatment location (Buor, 2003; Rosenberg, 1983; Yantzi & Rosenberg, 2008). Studies on Ghana’s biomedical health care system increasingly point to the influence that distance to care facilities and cost of travel exert on the poor and rural dwellers in their access biomedical care (Jørgensen, 2008; Kissah-Korsah, 2008). These studies acknowledge that patients especially the poor and vulnerable prefer to travel shorter distances for care (Aikins & Marks, 2007; Leonard, 2003). It is generally asserted that longer distance and cost of travel to biomedical care facilities promote preference for indigenous medicine (de Wet & Ngubane, 2014; Gyasi, Mensah, Adjei, & Agyemang, 2011). The findings of this study similarly indicate that residents’ perception on the proximity of the nearest biomedical care facility influences the type of care sought for last illness experienced prior to this study. Residents who opined that biomedical services were close were more than twice likely to have sought professional biomedical care rather than self-care for the last illness they experienced compared with those who viewed such services as far (RRR = 2.776, p < .05). Whereas the influence of distance on access and use of biomedical care is widely recognized in studies, its effect on the new professional indigenous care system is less known. Nevertheless, this study can infer from Van Andel, Myren, and Van Onselen (2012) that, distance as a barrier to care has a similar effect on the use of professional indigenous care services. In their study on Ghana’s herbal market, they found out that products transported from long distances were quite expensive (Van Andel et al., 2012). There is the need, therefore, to deeply and critically examine the effect of distance as geographic and economic factors on the use of professional indigenous medical care services given the changes that have characterized the indigenous health care system.
This study has few conceptual and methodological limitations which presents avenues for future studies. The first limitation relates to the conceptual model used in statistical and analytical discussion. In this present study, respondent’s health need and how it may have influenced their care-seeking behaviors is not captured. Thus, further studies are necessary to explore the influence of self-rated health status, and existence of chronic illness on last seeking behaviors of Ghanaians within this pluralistic perspective. In addition, respondents were not asked the severity of the last illness experienced prior to the study; hence it is difficult to assert whether the severity may have contributed to the difference in care–seeking behavior (general care seeking and last illness care–seeking behavior). The second limitation concerns the cross-sectional nature of the study and the small sample size. The former limits the ability of this study to make causal relationship among the study variables. However, this limitation is overcome by cross-referencing findings of this study with others of similar theme or topic. Finally, the number of total respondents in this quantitative study was not large enough, hence the response categories of the study variables were collapsed to into dichotomous responses. This was done to address the issue of no response or small number of responses for certain categories.
Conclusion
This study to the best of my knowledge, is the first to investigate the treatment seeking behaviors of Ghanaians in a pluralistic health system perspective by conceptualizing self-care as a health care sector in modern Ghanaian health care system. The study argues for the inclusion of self-care or self-medication in any pluralistic health system analysis especially in a Ghanaian and sub-Saharan Africa context, given the transformations that have occurred in both the biomedical and indigenous health care systems. The findings of this study show that residents in Asikuma-Odoben-Brakwa district of Ghana have a distinction general care–seeking behavior and last illness care–seeking behavior. Whereas, majority of the resident tend to indicate self-care as their general care–seeking behavior, a significantly high proportion used professional biomedical services for the last illness they experienced prior to this study. Self-care as a predominant avenue of treatment in Ghana has been acknowledged in a number of studies (Asenso-Okyere et al., 1998; Biritwum, Welbeck, & Barnish, 2000; Dzator & Asafu-Adjaye, 2004; Sato, 2012b; Waddington & Enyimayew, 1989), though not from a pluralistic health systems perspective as done in this study.
The study further reveals that policy and planning interventions in the biomedical health care system has improved access and use of its services in the study area. The NHIS for example was seen to have influence on the general care–seeking behavior of residents, as members tend to use biomedical care services due to the financial cushion the scheme provides in access to services. Similarly, location of CHPs health center in deprived areas has also boost access and use of biomedical care services compared with self-care and professional indigenous care in terms of the type of treatment residents sought for their last illness. The study further demonstrates that the commercialization and professionalization of the indigenous health care system has significantly introduced economic burdens in it access and use, especially among the poor and urban dwellers. In view of this study opens a pathway for the need critically re-examine Ghana’s indigenous medical care system and how contemporary transformations are influencing access to services in the professionalized sector. It is my hope that the findings of this study will guide and inform discourse on Ghana’s pluralistic health care systems from a triple sector perspective rather than the dual system approach advocated by Good et al. (1979), Twumasi (1979), Sato (2012a) and others.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author acknowledges the Norwegian Quota Scheme for financial support for the research.