
Abstract
This study examined associations between main references Anglophone and Francophone men and women refer to when learning healthy eating, and their knowledge of best food habits (KBFH), body mass index (BMI) status, sex, age, education, and household income. Data were obtained from a 2012 Statistics Canada survey (Canadian Community Health Survey: Rapid Response, Canada’s Food Guide). A greater number of women reported high KBFH than men. Regardless of the language group, “general search on the Internet,” “TV programs,” and “family and friends” were referred to the most for learning about healthy eating. However, those who refer more often to “health organizations” or “weight loss programs” had significantly higher KBFH and lower BMI rates.
Keywords
Introduction
Recent evidence has confirmed the influence of diet and nutrition on populations’ health (Brug, 2008). The role of healthy eating in good health is well recognized, and people’s health is affected greatly by what they choose to eat (Michaelidou, Christodoulides, & Torova, 2012). Notably, unhealthy eating habits contribute to the onset of diet-related diseases (Schwartz, Scholtens, Lalanne, Weenen, & Nicklaus, 2011). Several studies show that obesity rates in Canada have increased between 2000 and 2011 (Gotay et al., 2012). Also, statistics indicate that 1.37 million Canadians suffer from heart diseases, which are the second leading cause of death in Canada (Statistics Canada, 2015). Thus, food selection is undoubtedly seen as an important consumer behavior with many long-term consequences on both individual and societal levels (Deshpande, Basil, & Basil, 2009). Healthy eating is defined by dietary recommendations providing guidelines that are related to high fruit and vegetable consumption, and high fiber and low fat intake (Conner, Norman, & Bell, 2002). Healthy eating is not a diet; it refers to the strategies that can be adopted by individuals to live and enjoy life. It starts with changing one’s dietary habits, for instance, adding more fresh fruits and vegetables, and whole grains and cutting back on foods that have a lot of fat, salt, and sugar (Healthwise Staff, 2015). Hence, food choice is a process behavior, and as such complex strategies are required to enable one to make appropriate choices among available alternatives (Hausman, 2012). Availability of foods in post-industrial societies provides opportunities for the large majority of people to acquire food, basically anywhere at any time (Sobal & Bisogni, 2009). Therefore, to moderate stimuli from food abundance, there exist government-issued dietary guidelines providing food and beverage recommendations that are intended to help individuals achieve and maintain optimal health (Tom, Fischbeck, & Hendrickson, 2016). However, few Canadians prefer to utilize the dietary guidelines proposed by governmental public health agencies. Loney (2015) explains that much of the under-utilization of Canada’s Food Guide (CFG) can be attributed to the fact that despite being familiar with the tool, most people do not actually know how to use it. More specifically, confusion lies in the fact that the recommendations belong to different ages, genders, and serving sizes. This can be especially confusing for people with low literacy or those with poor mathematical skills.
There have been a plethora of messages from various sources advising consumers to choose healthy eating alternatives. Health professionals from various specialties are often considered to play an important role in individuals’ healthy eating habits, with dietitians being perceived as the most reliable (van Dillen, Hiddink, Koelen, de Graaf, & Van Woerkum, 2003). Interestingly, people are more likely to seek dietary advice outside the healthcare sector. For example, many people rely on weight loss programs, family, friends, media, and food corporations to learn about healthy eating habits (Healthwise Staff, 2015). This study aims to (a) provide background on the major informational resources mentioned above, (b) study the main references used by both Anglo- and Franco-Canadians to learn about healthy eating habits, and (c) examine the associations between the use of these references and the knowledge of best food habits (KBFH), body mass index (BMI) status, education, and income levels. Canada comprises two formal language groups, Francophones and Anglophones. The differences between these groups go beyond simply the language used; there is a well-established cultural difference. These differences have the potential to influence eating habits; as such it is important to study these groups separately and to make comparisons among them. In Canada, Francophones are “North Americans” who speak French. Culturally, they are different from French people; however, they do share some cultural similarities, such as similar religious traditions, valuing strong united family orientation and community ties (Murphy, 1981; Ross, 1954).
In terms of their eating habits, few studies have investigated differences in eating habits of both Anglophones and Francophones in Canada. Schaninger, Bourgeois, and Buss (1985) found that Francophone families consumed soft drinks and sweet instant beverages and less dietary beverage and alcohol (domestic wine and beers) than English-speaking families. In addition, Francophones use more staples associated with original cooking (Schaninger et al., 1985). Francophone women tend to have a more negative attitude toward convenience foods. In Quebec, the quality of cooking ingredients and preparing meals at home as a family tend to be culturally important. Tigert (1972) argues that the Francophones consume more sweet products compared with Anglophones. Moreover, he found that Anglophones are more concerned with calorie intake when compared with Francophones (Crosby, 1969).
Health Organizations
Medical institutions and practitioners help consumers to determine what types of food they should consume (Inniss, Bahlo, & Kardinaal, 1999). By presenting comprehensible nutritional information, they assist consumers in making healthier food choices (Watson et al., 2014). Moreover, health policy makers hope to reduce the incidence of chronic diseases through the modification of individual dietary patterns. For example, Health Canada’s “Eating Well with Canada’s Food Guide” includes health recommendations that suggest appropriate norms regarding specific quantities of different types of foods that Canadians should consume daily. The discussion of the medicalization of eating and feeding is pertinent to the current debate. It is defined as a process whereby non-medical problems, such as food choices, are redefined and treated as medical problems, usually in terms of illness or disorders (Conrad & Schneider, 1980). Currently, medical professionals make a direct connection between industry and consumers, where the former is responsible for an increased amount of nutrition-based pharmaceutical products available to individuals (Camargo, 2013). For instance, functional foods are used as medicalized foods, which can be defined as enhanced and enriched foods that influence the consumers’ health (Heasman & Mellentin, 2001). These foods are unique in their ability to increase health beyond basic nutrition (Katan & Roos, 2004). As such, health is seen as the main objective, which has contributed to the increasing development of functional foods (Nestle, 2013).
Family and Friends
Beyond the influence of medical professions, family and friends (FF) contribute to individuals’ eating habits. Health behaviors of individuals are first shaped at home, where parents or caregivers encourage positive eating habits in children (Borra, Kelly, Shirreffs, Neville, & Geiger, 2003). According to Slusser et al. (2011), parents acquire personal knowledge about healthy foods by retrieving information from different resources. This is used to encourage the healthy patterns in their children. In general, parents’ attention to the health of their children is considered to be a positive attribute; nonetheless, in certain circumstances, the strategies used to encourage children to follow healthy habits can serve as a source of conflict due to unequal power relations between parent and child (Valentine, 1999). For young children, the family unit is the most influential aspect of their social environment, yet other individuals, such as friends and teachers, can also play an influential role (Vereecken, Maes, & De Bacquer, 2004). For example, schools, both elementary and secondary, increase students’ awareness of health outcomes by implementing healthy lifestyle programs. These programs promote physical activity, healthy diet, and weight management methods (Lowry et al., 2000).
Media
Media also play an active role in shaping individuals’ eating habits. The Internet and other communication technologies became prevalent during the second half of the 20th century and are now easily accessible and widespread. These outlets provide various online programs that promote healthy food choices. The findings from a recent study show that web-based healthy programs are immediately transferred to the viewers’ consciousness (Cullen, Thompson, Boushey, Konzelmann, & Chen, 2013). In addition, a study by Williamson et al. (2006) on African American adolescents and their parents found that initially Internet-based weight loss programs did help promote weight loss; however, as website use decreased over time, positive outcomes were not found to be sustainable in the long term. Other mass media outlets have both negative and positive impacts on individuals’ eating behaviors and bodies, and this is especially true for television. Media are responsible for influencing the public’s perception of what is considered to be a desirable body shape (Kirk, 2004). Appearance and body image tend to be particularly important for women (Haworth-Hoeppner, 2000). To achieve these “ideal,” yet often unrealistic, appearances, individuals often alter their eating behaviors. This can contribute to the development of eating disorders, such as bulimia and anorexia nervosa (Mond & Arrighi, 2012). Thus, it is not surprising that dieting is strongly linked to the essence of femininity in the contemporary era (Meyer, Blissett, & Oldfield, 2001). On a societal level, both broadcast and interactive techniques have accelerated the transmission of information in societies. Theories of communications highlight the hegemonic status of cultural industry makers who direct individuals’ consciousness according to their objectives, which can be seen in the realm of health and nutrition promotion (Holmes, 2005).
Study Population
The analyses for the current article were based on data from 2012 “Canadian Community Health Survey: Rapid Response, Canada’s Food Guide” (N = 10,265). 1 This rapid response module was added to collect specific information on the knowledge and use of the Canadian Food Guide by the Canadian population. The CCHS is representative of the Canadian population 12 years of age and over (data from all 10 provinces and three territories; Statistics Canada, 2012).
The sample was subdivided into two cultural language groups based on individuals’ responses to the following survey question: “What is the language that you first learned at home in childhood and still understand?” Weighted data were used in all analyses; however, two different weighting factors were used depending on the nature of statistical analyses. For the descriptive analyses, the data were weighted to be representative of the population of Canada (Anglophone, N = 15,488,691; Francophone, N = 6,017,835). For the bivariate and regression analyses, as recommended by Statistics Canada, a weighting formula was used to normalize the data (Anglophone, N = 22,507; Francophone, N = 7,864; refer to the appendix). This approach is used to mitigate the risk of Type I error. The respondents who did not identify English or French as their first language were excluded from this analysis.
Outcome Variables
Eight questions about the use of main healthy eating references are included in the CCHS data. These questions were presented as followed: “In the past 6 months, did you consult any of the following sources to learn more about healthy eating”: (a) health professional such as a family doctor or dietician, (b) health or community center or local community services centers (CLSCs), (c) health organizations such as Heart and Stroke, (d) fitness programs, (e) weight loss programs such as Weight Watchers, (f) your family or friends, (g) TV programs about healthy eating, and (h) general research on Internet.
Using these data, four dependent variables were created for use in bivariate and regression analyses. They were recoded as followed: (a) health organizations (“health professional,” “CLSCs,” and “health organizations”); (b) weight loss programs (“fitness programs” and “weight loss programs”); (c) media (“TV programs” and “Internet”; and (d) family or friends. The value labels for these variables were “low” and “high.”
Exposure Variables
This study analyzed the association between various independent variables and the dependent variables. Independent variables include knowledge of best food habits (KBFH), BMI rates, education, and income levels. The variable KBFH was created by summing an individual’s responses to the following questions from questionnaire: (1) “Eating out for order meals from restaurant/cafeteria,” (2) “Type of food groups needs most servings per day,” (3) “Eating dark green veggies or greens,” (4) “Eating orange-colored veggies,” (5) “When did you looke to Canadian Food Guide.” The Cronbach’s alpha internal consistency was 0.889 between the questions used for summing. Raw scores were then recoded into three categories: “low” (0-1), “moderate” (2), and “high” (3-5). BMI status was computed and categorized into four categories (underweight, normal weight, overweight, and obese) by Statistics Canada based on each respondent’s self-reported height and weight.
Statistical Analyses
For all statistical analyses, the sample was stratified by language group (Anglophone and Francophone). Descriptive statistics explored the main socio-demographic characteristics, including sex, age, marital status, household education, and income levels, as well as the original eight references for learning healthy eating.
Binary logistic regression analyses were performed to identify which of the four dependent variables showed a significant association with independent variables. Adjusted logistic regressions controlled for sex, age, education, KBFH, and BMI rates. It should be noted that due to the higher collinearity between income and education, it was removed from the logistic regression analyses.
Results
Socio-demographic characteristics of Anglophones and Francophones are presented in Table 1. An almost equal proportion of men and women (50%) responded to the survey, and the majority were between the ages of 40 and 74. Around 55% of both Anglophones and Francophones were “married/common-law.” A large percentage of both language groups had only completed a diploma, college, or CEGEP 1 (approximately 60%), whereas 12% of Anglophones and 10% of Francophones had completed a graduate degree. In terms of household income levels, findings indicated that over 35% of Anglophones and 26% of Francophones lived in families with an annual income of $100,000 (CAN) or more.
Anglophone and Francophone Socio-Demographic Characteristics.

Source. Micro-data analysis of the Canadian Community Health Survey: Rapid Response.
Results of KBFH are represented in Table 2. The findings show that women were more likely to report higher KBFH (over 70%) compared with men; however, for both men and women, only a small difference exists between Francophones and Anglophones in terms of reporting higher KBFH.
Anglophone and Francophone Men and Women’s Knowledge of Best Food Habits.

Source. Micro-data analysis of the Canadian Community Health Survey: Rapid Response CFG on awareness and usage of Canada’s Food Guide, 2012.
In terms of self-reported BMI status (Table 3), approximately 47% of women, regardless of language groups, were classified by Statistics Canada as being normal weight, and approximately 28% of them were overweight. Very little difference was found between Anglophone and Francophone men and women in terms of obesity rate; however, Francophone women had a lower percentage of obesity rate (19%) compared with others.
Anglophone and Francophone Men and Women’s BMI Rates.

Source. Micro-data analysis of the Canadian Community Health Survey: Rapid Response CFG on awareness and usage of Canada’s Food Guide, 2012.
Note. BMI = body mass index.
Findings of the main references for learning healthy eating are in Table 4. Most men and women reported referring to “general search on the Internet,” “family/friends,” and “TV programs.” Interestingly, among Francophones, more men (9%) sought out healthy eating advice from health professionals (doctors, dietitians, etc.), whereas the opposite was witnessed among Anglophones. More Anglophones reported to referring to FF to learn healthy eating habits than Francophones. A considerable difference was found between two language groups in terms of referring TV programs and search on the Internet, with Anglophones relying more heavily on these.
Percentage of Anglophone and Francophone Men and Women’s Main References to Learn Healthily Eating Habits.

Source. Micro-data analysis of the Canadian Community Health Survey: Rapid Response CFG on awareness and usage of Canada’s Food Guide, 2012.
Note. CLSC = local community services center.
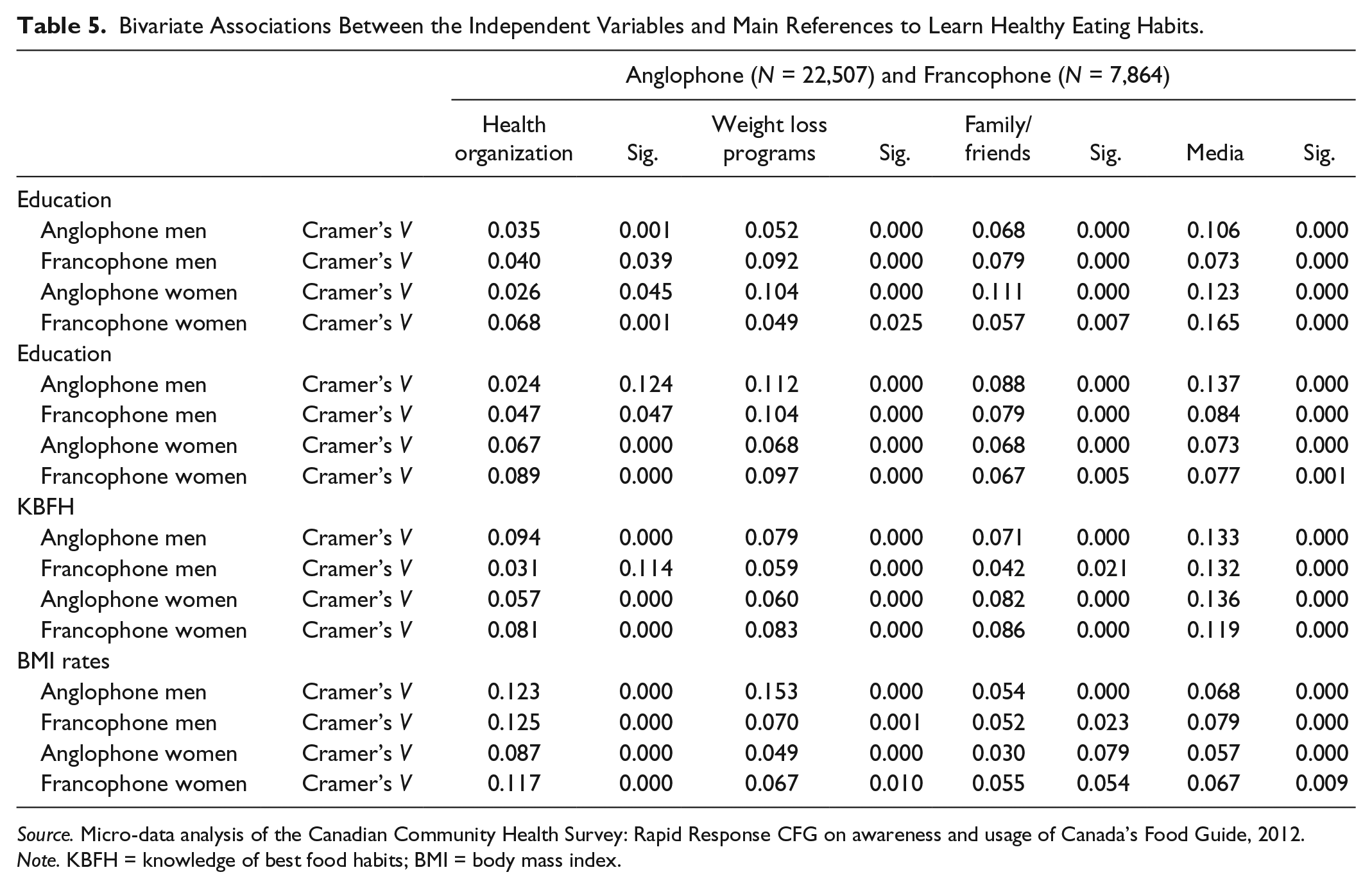
Cramer’s V coefficients of association for Anglophone and Francophone men and women are presented in Table 5. Anglophone men and women’s higher KBFH were positively associated with all the references to learn healthy eating; however, the strength of association was strongest with regard to using “media” among Anglophone men (0.133, p = .001), and Anglophone women (0.136, p = .001).
Bivariate Associations Between the Independent Variables and Main References to Learn Healthy Eating Habits.
Source. Micro-data analysis of the Canadian Community Health Survey: Rapid Response CFG on awareness and usage of Canada’s Food Guide, 2012.
Note. KBFH = knowledge of best food habits; BMI = body mass index.
BMI status was positively related to Anglo-Canadian men’s references to health organizations (0.123, p = .001) and weight loss programs (0.153, p = .001). Among Anglophone women, higher educational status was positively associated with the use of media (0.123, p = .001). In addition, higher income levels for Anglo-Canadian men was positively associated with weight loss programs (0.112, p = .001) and media (0.137, p = .001).
Like Anglophones, higher KBFH had positive significant linkage with media among Francophone men (0.132, p = .001), and women (0.119, p = .001). Having higher BMI status was positively associated with referring to health programs for both French-Canadian men (0.125, p = .001) and women (0.117, p = .001). No strong associations were found between education and the main references for learning healthy eating; however, media, in comparison with the others, was stronger for Francophone women (0.165, p = .001). Similarly, the association between income level was not strongly associated with the reference to learn healthy eating habits, except weight loss programs (0.104, p = .001) among Francophone men.
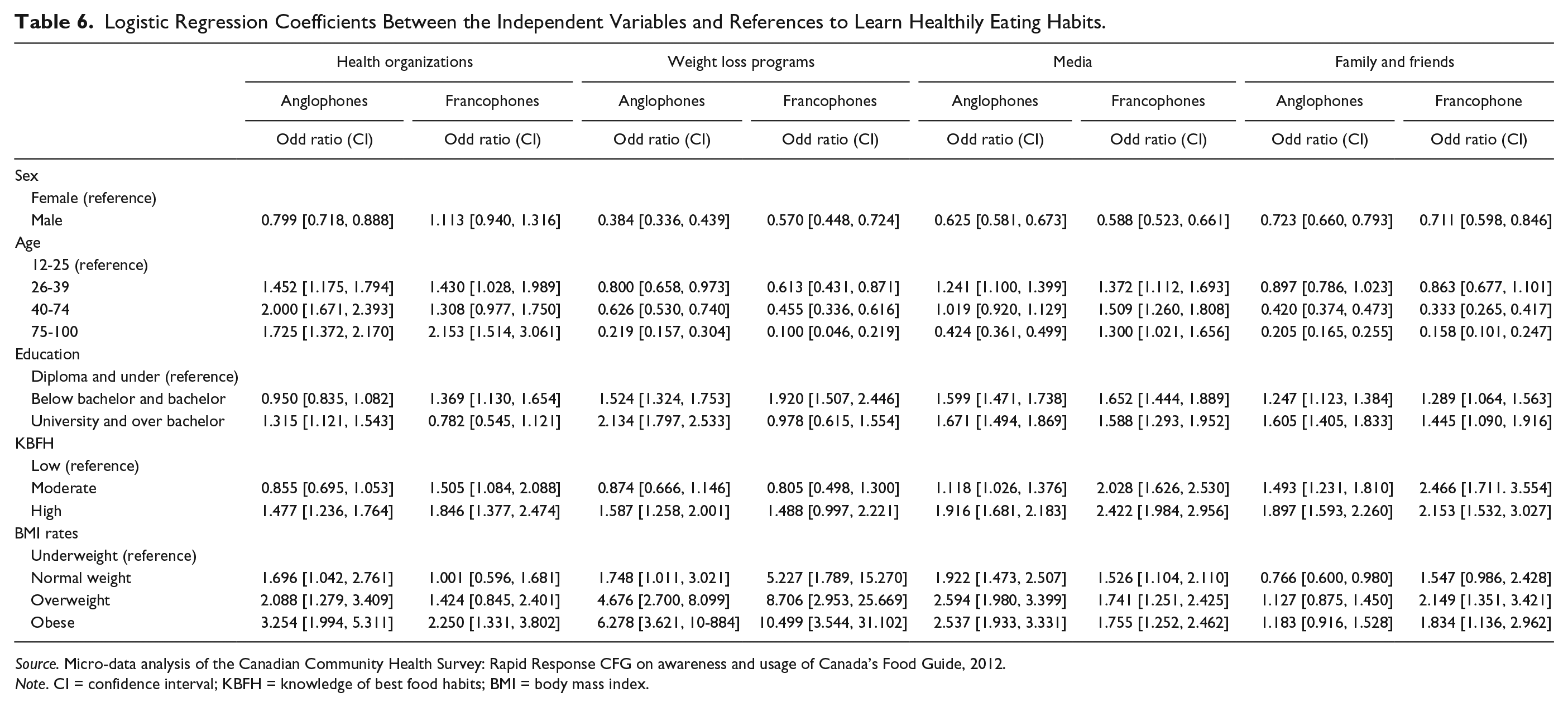
Results of the binary logistic regressions for the four reference frameworks, and adjusting for all socio-demographics 2 are shown in Table 6. Referring to health organizations (RHO) among Anglophones was higher among obese individuals (3.254, p = .000), with higher KBFH (1.477, p = .000), and higher education levels (1.298, p = .004), between 40 and 74 years of age (2.000, p = .000). However, RHO was lower among men (0.799, p = .000) compared with women. Similarly, RHO among Francophones was higher among obese people (2.250, p = .004), with higher KBFH (1.846, p = .000), and below bachelor and bachelor education (1.369, p = .004), between 75 and 100 years of age (2.153, p = .000). More interestingly, being obese increased probability of RHO among Anglophones versus their Francophone counterparts.
Logistic Regression Coefficients Between the Independent Variables and References to Learn Healthily Eating Habits.
Source. Micro-data analysis of the Canadian Community Health Survey: Rapid Response CFG on awareness and usage of Canada’s Food Guide, 2012.
Note. CI = confidence interval; KBFH = knowledge of best food habits; BMI = body mass index.
Referring to weight loss programs (RWLP) among Anglophones was lower among men (0.384, p = .000), between 26 and 39 years of age (0.800, p = .040). However, RWLP was associated positively with higher education levels (2.134, p = .000), higher KBFH (1.587, p = .000), and higher BMI rates (6.278, p = .000). For Francophones, RWLP was lower among men (0.570, p = .000), between 75 and 100 years of age (0.100, p = .000). But RWLP was higher among individuals with below bachelor and bachelor degree (1.92, p = .000), higher KBFH (1.488, p = .040), and obese individuals (10.499, p = .000). More importantly, being obese doubled the likelihood of RWLP among Francophones compared with Anglophones.
Referring to media was lower among Anglophone men (0.625, p = .000), between 75 and 100 years of age (0.424, p = .000). More importantly, referring to media was higher among the age group of 26 to 39 (1.241, p =.000). The probability of referring to media increased among Anglophones with higher education levels, higher KBFH (1.916, p = .000), and overweight and obese individuals. However, the probability of using media increased among Francophones with higher education levels, higher KBFH, and higher BMI rates.
In terms of the FF as the main references to learn healthy eating habits among Anglophones, lower odds ratio was found among men (0.723, p = .000), between 75 and 100 years of age (0.205, p = .000). Like the above references, odds ratio increased with high education levels (1.605, p = .000) and higher KBFH (1.897, p = .000). More interestingly, referring to FF was lower among Anglophones with normal weight (0.766, p = .000).
Referring to FF was negatively associated among Francophone men (0.711, p = .000), between ages 75 and 100 (0.158, p = .000). Referring to FF was higher among Francophones with higher education levels (1.445, p = .000), with moderate KBFH (2.466, p = .000), and with overweighting (2.149, p = .000).
Discussion
The main objective of this study was to investigate respondents’ self-reported references for learning healthy eating, such as health organizations, weight loss programs, media, family, and friends. More specifically, we focused on the association between mentioned references and KBFH, BMI status, education, and income by controlling variables such as sex and age for both Anglo- and Franco-Canadians.
Results indicated that Anglophone women had higher KBFH than their Francophone counterpart. Whereas the opposite was found among men, Francophone men reported higher KBFH than Anglophone men. The prevalence of obesity was slightly lower among Francophone women than the others. More importantly, there seems to be a difference in the resources that individuals refer to for healthy eating practices in relation to their primary language. For instance, referring to the Internet was higher among English-Canadians than French-Canadians, while referring to TV was higher among Francophones. A study argued that many Canadians are actively searching for information on the Internet to support health behavior change (Richardson, Hamadani, & Gotay, 2013).
Overall, the majority (three quarters) of the women had a higher percentage of having higher knowledge regarding best food habits (KBFH). A significant difference was found between men and women in terms of having higher KBFH. This is in line with the previous studies showing that women are generally more knowledgeable than men and have better nutritional knowledge (Hansbro, Bridgwood, Morgan, & Hickman, 1997; Levy, Fein, & Stephenson, 1993; Parmenter, Waller, & Wardle, 2000). The present findings suggest that there are some gender-related differences for reported reference frameworks. The results showed that majority of men and women reported referring “family/friends,” “general search on the Internet,” and “TV programs.” However, in terms of mentioning health organization as one of the main references, the results of this study showed that there is a significant difference between men and women, as well as among English-Canadians and French-Canadians with higher KBFH and different BMI rates. Social environment, including relationships with parents, spouses, friends, and more, affects personal dietary habits. Families and households provide a broad range of opportunities to influence food choices (Lawrence & Barker, 2009). Although the KBFH was significant and higher for Anglophones, in terms of referring to the media, no significant difference for BMI status was found for Anglophones. By contrast, among Francophones, we also found the higher odd ratio for KBFH and BMI rates referring FF, as a reference to learn healthy eating. Previous studies have indicated that better eating habits are related to better nutritional knowledge (Barreiro-Hurlé, Gracia, & de-Magistris, 2010; Beydoun & Wang, 2008; Stroud, 2013).
The advantage of this study was the large sample size (n = over 10,000); however, we recognized some limitations. The main references were based on self-reported measures, which may have been over- or understated by the respondents. More research is needed to find appropriate tools to measure the main reference frameworks used to learn about healthy eating. Furthermore, to construct KBFH, we also used self-reported questions concerning eating habits of respondents. The development of standardized questions is required to better measure the impact of KBFH. Finally, due to lack of questions measuring daily calorie, fruit and vegetable, sugar, and fat intake, we could not analyze the association between having knowledge about healthy food habits and actual food consumption.
An important implication of this study is its contribution to our understanding of the main areas to which people refer to in order to form their eating habits. This information can help inform public health policies, which may ultimately have a profound impact on the population’s health status. It is suggested that future research tests of nutrition knowledge and knowledge structures in relation to eating behaviors, such as fruit and vegetable intake, physical activities, and more.
Conclusion
There were no significant differences in language groups for levels of nutrition KBFH, so the considerable difference was found between women and men. No difference was observed between Anglophones’ and Francophones’ obesity rates; however, the disparity in overweight prevalence among men was higher than women. Internet, TV, and FF were main references both language groups referred to in learning about healthy eating. Specifically, a general search on the Internet for Anglophones and TV programs for Francophones were considered the main references to learn healthy eating. In addition, Anglophone women also relied heavily on FF to learn about healthy eating. All independent variables were consistently significant for reference frameworks among both language groups. However, the strength of the associations was not high. In comparison with men, women were more likely to refer to all references for learning healthy eating. Furthermore, seniors were more likely to mention health organizations. In addition, BMI rates were associated with individuals’ references to health organizations, weight loss programs, media, and FF. The findings showed that weight loss programs have a higher impact on individuals with higher BMI rates. Although both language groups with higher BMI rates referred to weight loss programs, the strength of the association was strongest for Francophones.
Theories indicate that media, which includes all information from books, magazines, television, Internet, plays an important role in the contemporary era with regard to shaping individuals’ attitudes, beliefs, and behaviors. This study’s findings support these theories in that individuals consistently relied on media to help them learn about healthy eating. Besides media, health organizations also play the leading role in health knowledge by informing and influencing the consumption of healthy foods and the acquisition of a healthy lifestyle (Jovicic, 2015).
Footnotes
Appendix
Normalizing weight: Normalizing weights is not necessary when analysts use computer software (i.e., STATA) capable of correctly accounting for the survey design in an analysis, and when suitable survey design information is available to the analyst. If analysts have a survey weight and corresponding bootstrap weights, and if they have appropriate analytical software for survey data, there is no reason to perform any weight normalization. This means that the survey weight of each respondent in a subpopulation being analyzed is divided by the mean of the survey weights for all members of the sample in the subpopulation (Gagné, Roberts, & Keown, 2011).
1
Pre university college in province of Quebec
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.