
Abstract
The aim of this study was to document the incidence, sources, and effects of workplace physical violence against Ghanaian nurses. Self-report questionnaires were completed by 592 nurses employed in public general hospitals in Ghana. Participants were selected using a combination of purposive and random sampling techniques. Nine percent of the participants experienced physical violence in the 12 months preceding the study. The majority of perpetrators were relatives of patients. Chi-square tests suggested significant relationships between type of hospital and workplace physical violence, and between intention to quit the nursing profession and workplace physical violence. Workplace violence had several negative effects on nurses including having disturbing memories about the incident and being “super alert” and vigilant. Strategies to curb workplace violence could include awareness creation among health care workers and the general public. Policies and legislations must also be put in place to address this social problem.
Introduction
Workplace physical violence is a phenomenon that confronts many countries (Blanchar, 2011). It undermines the safety, dignity, well-being, and happiness of workers (Bowie, Fisher, & Cooper, 2012; Hershcovis & Barling, 2010; Magnavita & Heponiemi, 2011). Besides, it can also affect organizations adversely through the payment of compensations, absenteeism, low productivity, dissatisfaction, and high employee turnover rates among others (Bowie et al., 2012). According to Kerr (2010), workplace violence is a leading cause of workplace deaths in the United States, particularly for women. Severe injuries or death resulting from workplace physical violence may seem remote in many countries but its other impacts cannot be underestimated (Kerr, 2010). The aim of this study was to document the incidence, sources, and effects of workplace physical violence against Ghanaian nurses.
Workplace violence has become an endemic problem in health care (Berry, 2013; Nelson, 2014), and nurses are particularly at a higher risk of abuse (AbuAlRub & Al-Asmar, 2011; Gacki-Smith et al., 2009; Joa & Morken, 2012). About a quarter of the world’s workplace violence occurs in that sector (Azodo, Ezeja, & Ehikhamenor, 2011). Numerous studies conducted across different countries such as Australia (Bakker, 2012; Hilliar, 2008; Hinchberger, 2009), Japan (Fujita et al., 2012), United States (Child & Mentes, 2010; Gacki-Smith et al., 2009; Hanson, Perrin, Moss, Laharnar, & Glass, 2015), United Kingdom (Lepping, Lanka, Turner, Stanaway, & Krishna, 2013), China (Kwok et al., 2006), Switzerland (Hahn et al., 2010), Egypt (Samir, Mohamed, Moustafa, & Abou Saif, 2012), Jordan (AbuAlRub & Al-Asmar, 2014; Albashtawy, 2013), and South Africa (Khalil, 2009) suggest that workplace violence is a problem for health care workers in both developed and developing countries.
Workplace physical violence against nurses may vary across departments/units with emergency, psychiatric, and intensive care units reputed to have the highest rates of physical assaults (Darawad, Al-Hussami, Saleh, Mustafa, & Odeh, 2015; Fujita et al., 2012; Hahn et al., 2013; Hahn et al., 2010; Park, Cho, & Hong, 2015). This has been attributed largely to the nature of cases that these units usually attend to. Depending on the unit where nurses work, they may experience more physical violence than other nurses within the same hospital (Hahn et al., 2013; Hahn et al., 2010).
Workplace violence may adversely affect the personal and professional well-being of nurses. Victims of workplace violence may suffer from posttraumatic stress disorder, impaired work performance, and insomnia (AbuAlRub & Al-Asmar, 2011; Gates, Gillespie, & Succop, 2011; Shahzad & Malik, 2014). Workplace violence has also been found to influence nurses’ turnover and turnover intentions (Boafo, Hancock, & Gringart, 2016; Dithisawatwet, Sawaengdee, Tangcharoensathien, Teerawit, & Thinkamrop, 2014).
In spite of the fact that workplace violence against health care professionals have become a topical issue in the last couple of decades (Gabe & Elston, 2008), there is a paucity of research on the problem in Ghana. Until 2016, when we (Boafo et al., 2016) published the incidence of verbal abuse and sexual harassment against Ghanaian nurses, no literature existed on workplace violence against nurses in the country. To date, no study has been conducted on the prevalence of physical violence against nurses in Ghana. However, media reports on speeches by prominent people in the health care sector point to the fact that violence against health care professionals indeed happens in many Ghanaian health care facilities. These reports suggest that workplace violence is not concentrated in psychiatric hospitals but is becoming a general problem for health care professionals in public hospitals (allAfrica.com). On August 21, 2001, Modern Ghana, an electronic media organization reported that the Akatsi District chairperson of the Ghana Registered Nurses Association (GRNA) stated during the nurses’ week celebration that Ghanaian nurses leave the country to seek greener pastures in other countries “because we face some risk of violence coupled with poor salaries and wages” (“Only 9,000 Nurses in the Country,” 2001). This is an indication of the prevalence and importance of violence as a variable to the retention of the already inadequate number of nurses in the country (Ghana Health Service, 2010). Furthermore, in a symposium organized as part of the health service week celebrations in 2010 by the Health Services Workers’ Union, the parliament of Ghana was implored to consider enacting laws on violence against health care workers to ensure that health care personnel worked in an atmosphere of peace. It was noted that violent attacks on health care workers were appalling, and there was the need for legislation on the issue to ensure maximum health care delivery (“Health Personnel Want Legislation,” 2010). There has indeed been a situation where the health workers of a hospital have gone on strike to protest against assault on some of their colleagues by sections of the public (“Doctors at LEKMA Stay Away From Duty,” 2011). Furthermore, Boafo et al. (2016) reported high incidence of nonphysical violence among the sample reported in this article.
These reports give a cause to worry considering the fact that workplace violence is associated with intentions to leave the nursing profession (Boafo et al., 2016; Dithisawatwet et al., 2014). In Ghana, the nurse–patient ratio is low, and it is still worsening, a situation that is described in the 2012 annual progress report on the implementation of the Ghana Shared Growth and Development Agenda (“Ghana’s Doctor-to-Patient Ratio Worsens,” 2014). The report showed that the nurse–population ratio for the country worsened from one nurse to 1,240 people in 2011 to 1,251 people in 2012. This was against the backdrop that the set target for the year 2012 was one nurse to 900 people. In fact, the World Health Report (2006; as cited in Gyamfi, 2011) classified Ghana among 57 countries which suffer a critical shortage of health care professionals including nurses. Moreover, added to these problems is that a significant number of nurses are lost through emigration (Buchan & Dovlo, 2004). It therefore becomes imperative to address the issue of violence against nurses so that it does not exacerbate the situation of there being an insufficient number of nurses in the country.
Any policy or legislation seeking to address the problem of workplace physical violence in the health care sector must, however, be based on evidence regarding the sources and magnitude of the problem. It has been suggested that governments’ failure to collect data on violence against nurses accounts for the inability to make effective policies to address the problem (Boafo et al., 2016; International Council of Nurses [ICN], 2000). Although numerous studies have been conducted on the phenomenon in different countries, it is only possible to apply their results to Ghana to a limited extent. The reasons for this, among others, may be found in the differing organizational structures of health care, and in differing training and qualification of health care staff, as well as varying sociocultural context. The risk of violence, for instance, may be understood differently by people depending on their cultural backgrounds and position within the health care institution. It is in relation to these that the current article documents the incidence and distribution of physical violence against nurses in Ghana. Three main research questions are addressed:
Definition of Workplace Violence
The study upon which this article is based adopts the internationally recognized definition by the World Health Organization (WHO) for workplace violence. It defined workplace violence as “incidents where staff are abused, threatened, or assaulted in circumstances related to their work . . . involving an explicit or implicit challenge to their safety, well-being or health” (Wang, Hayes, & O’Brien-Pallas, 2008, p. 31). This definition incorporates all the forms of workplace violence such as physical violence, verbal violence, sexual abuse, and so on.
The definition further provides descriptions of actions that constitute each of the various types of violence. The subject of this article, physical violence, includes “beating, slapping, shooting, pinching, scratching, and biting that cause physical, sexual or psychological harm to the worker” (Di Martino, 2002, p. 11).
Method
Sampling and Procedures
A multistage sampling technique was used in the current study. Data were collected between September 2013 and April 2014 through the use of questionnaires. A total of 12 hospitals were involved in the study.
The first stage of the sampling procedures involved purposively selecting two teaching hospitals. Korle Bu and Tamale Teaching Hospitals were selected to ensure that there was a southern–northern balance. Five regional hospitals were selected from five randomly selected regions of Ghana. The final stage of hospital selection involved randomly selecting one district hospital from each of the chosen regions. To ensure that nurses working on all shifts were covered, the data collection took place between 12:00 p.m. and 9:00 p.m. Data were collected by the corresponding author and four trained research assistants.
In each hospital, nurses were selected from the various units/departments through simple random sampling. The inclusion criteria for the study were as follows: (a) a participant should be a qualified nurse, and (b) a participant should have at least 1 year nursing experience. A total of 1,021 nurses were requested to get involved in the study, and 685 accepted to be part by completing a questionnaire. However, 89 of the questionnaires were not properly completed, and were not included in the analyses. Four participants were found to be deputy directors of nursing services and were also removed from the analyses because they were too few in number for any significant statistical analysis. At the end, the data presented here are that received from 592 participants.
Measures
The International Labour Organization, ICN, the WHO, and the Public Services International’s (ILO/ICN/WHO/PSI, 2003) Health Sector Workplace Violence Questionnaire was adapted for the current article. Sections in the questionnaire such as bullying and racial harassment and other items which fell outside the purview of the study were removed. The adjusted questionnaire was reviewed by five professional nurses for face validity, clarity, and sensitivity of items. Physical violence was recorded using a single-item scale. Participants were asked “In the last 12 months, have you been physically attacked in your workplace?” (yes/no). In view of this, it was not possible to determine its reliability by Cronbach’s alpha. However, before the start of the study, the instrument was tested on 20 nurses who were not part of the study on two occasions with a 2-week interval. The test–retest correlation coefficient (Nagy, 2002) for physical violence was 1.00.
This questionnaire was adopted because it has been used in several studies across different countries such as Iran (Esmaeilpour, Salsali, & Ahmadi, 2011), Jordan (AbuAlRub & Al-Asmar, 2011), Brazil, Lebanon, Portugal, Bulgaria, and Thailand (Di Martino, 2002). In Africa, it has been used in South Africa (Steinman, 2003) and Mozambique (Adam, Caldas, Aly, & Capece, 2003). The current study is, therefore, comparable with other studies within and outside Africa.
The research instrument was also used to collect data on nurses’ intentions to quit the nursing profession. It adopted the approach of Kankaanranta and Rissanen (2008) by using single-item categorical (dichotomous) variable to measure intention to quit. Participants were asked, “Do you have the intention of quitting your job as a nurse in the near future?” The structure of this item is also the same as the one which was used to measure Ghanaian nurses’ emigration intentions (Anarfi, Quartey, & Agyei, 2010). The test–retest correlation coefficient for the intention to quit variable was .9. Details of the methods used for the study have been published elsewhere (Boafo et al., 2016).
Ethical Issues
Ethical clearances were given by the Edith Cowan University Human Research Ethics Committee (HREC) and the Ghana Health Service Ethics Review Committee. Permissions were also given by the medical superintendent or hospital administrator (where appropriate) and the head of nursing services of each hospital prior to the commencement of data collection. The aim of the study was explained to all participants, and they were assured of confidentiality. Participants were not allowed to write their names or any other information that could be used to trace them on the questionnaire. They were asked to retain the questionnaires until the researcher or research assistants came around to collect them. Participation in the study was voluntary, and participants were at liberty to pull out of the study without any consequences.
Data Analyses
The data were analyzed using IBM SPSS Version 20. Frequencies, means, and standard deviations (SDs) were used to describe the sociodemographic and workplace characteristics of participants and to establish the incidence and sources of workplace violence. Chi-square test was used to test the association between workplace physical violence and sociodemographic characteristics. It was also used in testing the association between workplace physical violence and intention to quit the nursing profession.
Results
Demographic and Workplace Characteristics
The demographic and workplace characteristics of the research participants are presented in Table 1. The sample consisted of 592 nurses. More than a third (42.1%) were nurses in the Greater Accra Region and 22% worked in the Eastern Region. One third (32.9%) of the participants worked in teaching hospitals, 38.7% worked in regional hospitals, and a further 28.4% were nurses in district hospitals.
Sociodemographic and Workplace Characteristics (N = 592).

In terms of gender, 79.2% of the sample were females and 20.8% were males. The majority (52.5%) of the participants were not married. The mean age of the sample was 31.76 years (SD = 9.53); the minimum and maximum ages were 21 and 60 years, respectively. In all, 61.3% of participants had a diploma qualification, and 52.0% were staff nurses. On the average, participants had worked in nursing for 7.38 years (SD = 9.53). Less than a fifth (16.9%) worked in the outpatient department (OPD), and more than a quarter (35.3%) were employed in the medical and surgical units.
In relation to established protocol for reporting workplace violence against nurses, 72.1% reported that such protocols existed, and 80.1% of these reported they know how follow through these procedures. The mean score for nurses’ concern over workplace violence suggested that nurses were moderately concerned about workplace violence; however, the mode revealed a contrary view. A relative majority of the sample were extremely concerned about workplace violence (minimum = 1, maximum = 5, M = 3.05, SD = 1.51, mode = 5). The demographic and workplace characteristics of the study sample have also been published elsewhere (Boafo et al., 2016).
Incidence and Sources of Physical Workplace Violence
The results as presented in Table 2 showed that, of the 592 nurses included in the study, 53 (9.0%) had experienced physical violence in the 12 months prior to the study. Of these, 42 (79.2%) were females and 11 (20.8%) were males. Chi-square analysis showed that this difference was statistically not significant. In terms of regional distribution of the incidence of workplace physical violence against nurses, 32.1% of victims were nurses in the Greater Accra region, and 22.6% in the Eastern and Ashanti regions. Regional differences in exposure to physical violence were also not statistically significant.
Incidence, Distribution, and Sources of Physical Workplace Violence Against Nurses (n = 53).
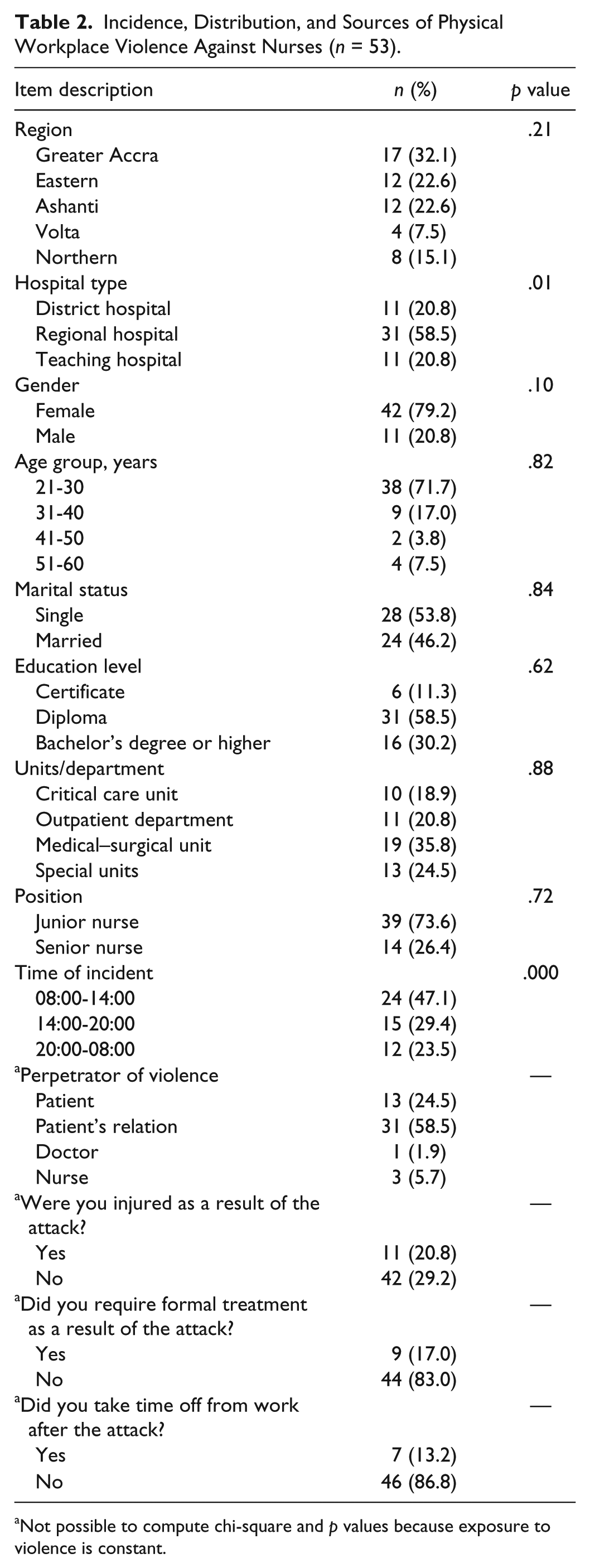
Not possible to compute chi-square and p values because exposure to violence is constant.
Workplace physical violence against nurses was perpetrated by patients and their relatives, other nurses, and doctors. The results showed that relatives of patients were the most frequent perpetrators of physical violence against nurses. They were responsible for more than half (58.5%) of physical violence perpetrated against nurses. The analyses further showed that 20.8% of those who were physically abused got injured, and 17% were given formal treatment following the attack. Nurses who were physically abused took an average of 11.5 days off (SD = 20.05, mode = 2), and had worked for an average of 5.96 years (SD = 7.54).
It is also noteworthy that more than two thirds of the victims were within the age range of 21 to 30 years. Correspondingly, junior nurses formed almost three quarters (73.6%) of victims. Although statistically there was no significant association between position or rank and physical violence, it is worth noting that physical violence was far less for senior nurses (nursing officer and above) compared with their junior counterparts.
In terms of incidence across units, it was found that 35.8% (19) of nurses who suffered workplace physical violence worked at the medical and surgical units. This was followed by the special units (24.5%) and then the OPD (20.8%). However, chi-square test showed no statistically significant association between unit where one worked and physical violence. There was, however, a statistically significant association between physical workplace abuse and the type of hospital, with nurses in the regional hospitals being more likely to be abused physically in the workplace, χ2(N = 592, df = 2) = 9.720, p = .01.
Effects and Reactions to Workplace Physical Violence
As shown in Table 3, reactions to physical violence ranged from taking no action to pursuing prosecution. Encouragingly, the most frequent (35.8%) response to physical violence was reporting to a senior staff member/unit in charge. This was followed by telling a colleague about the incident (32.1%) and then taking no action (18.8%). Thirty-one percent of the respondents who have been abused indicated that action was taken to investigate the causes of the incident. All investigations were initiated by the nursing administration/unit in charge.
Reactions to Physical Workplace Violence.
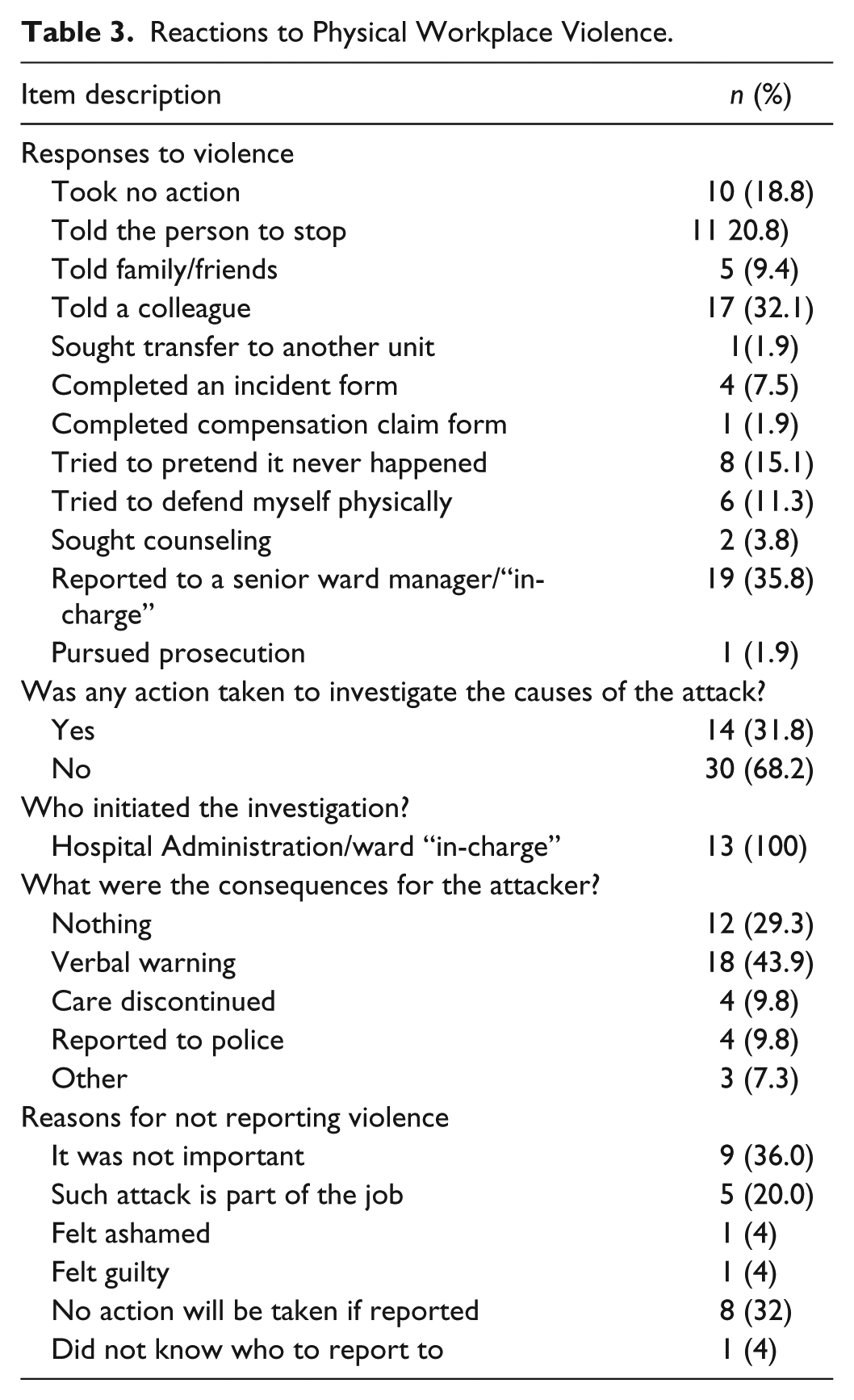
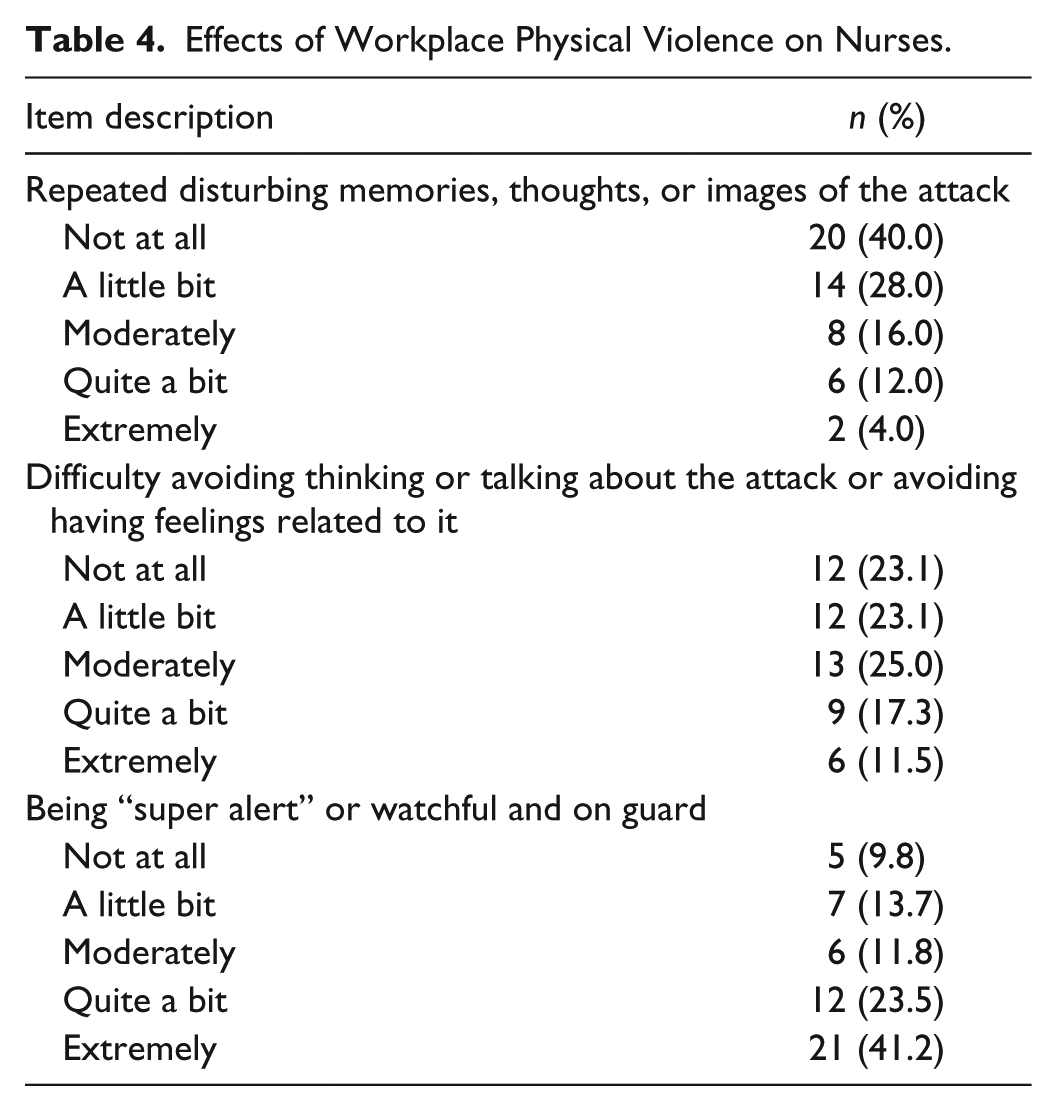
Only 9.8% of cases were reported to the police. A relative majority (43.9%) of attackers were given verbal warning. Those who did not report the incident provided various reasons for doing so; more than one third (36%) believed it was not important to report, and 32% thought no action will be taken if reported. Indeed, if no action will be taken if reported, then it is not important to report. Being extremely “super alert” or watchful and on guard was the most frequently reported effect of workplace physical violence. Data on the reactions to workplace physical violence and its effects are presented in Table 4.
Effects of Workplace Physical Violence on Nurses.
One fifth (19.9%) of participants in the entire sample indicated they had intentions of quitting the nursing profession (not shown in table). Chi-square test showed a statistically significant association between the experience of physical violence and intention to quit the nursing profession, χ2(N = 586, df = 1) = 11.22, p = .001. The unadjusted odds ratio computed from the cross-tabulations indicated that nurses who experienced physical violence were 2.7 times more likely to have the intention to quit the nursing profession than those who have not been victims of workplace physical violence.
Discussion
The current article corroborates the findings of several studies that indicate that nurses are exposed to high rates of workplace violence, and that the phenomenon has the tendency to negatively affect nurses and the health delivery system in general (AbuAlRub & Al-Asmar, 2011; Esmaeilpour et al., 2011). Although the incidence of physical workplace violence found among Ghanaian nurses (9.0%) was lower than what has been reported by many other studies on the subject (17%-27%; e.g., AbuAlRub & Al-Asmar, 2011; Darawad et al., 2015; Gacki-Smith et al., 2009; Natan, Hanukayev, & Fares, 2011; Samir et al., 2012; Steinman, 2003), the impact was no less, as 41.2% of participants who suffered physical violence reported that they became extremely “super alert” and on guard. This finding, which is consistent with studies such as AbuAlRub and Al-Asmar (2011) and Esmaeilpour et al. (2011) (who also reported that a significant proportion of participants in their studies who were exposed to physical violence became extremely super alert), is disturbing and necessitates the formulation of policies to address the problem. This is because quality care partly depends on the quality of the relationship between nurses and clients. Obviously, nurses cannot deliver high quality service if they are overly alert as a result of the experience of violence. It has been confirmed by research that workplace physical violence negatively affects the services nurses provide (Gates et al., 2011).
The article also showed that workplace physical violence has implications for the retention of the already insufficient number of nurses in Ghana. A statistically significant association was found between physical violence and intention to quit the nursing profession. This finding corroborates the results of several studies (e.g., Dithisawatwet et al., 2014; Nachreiner et al., 2007; Sofield & Salmond, 2003) which have linked workplace violence to nurses leaving the profession.
Unlike what has been reported in several studies, there was no statistically significant association between physical violence and the unit where one worked. This suggests that physical violence is a generalized phenomenon in general hospitals in Ghana, and not concentrated in any particular unit or department. However, there was a statistically significant association between hospital type and the incidence of violence with regional hospitals recording the highest incidence. This situation may be due to the inadequate security coupled with the high number of patients that regional hospitals attend to. In a Jordanian study, Darawad et al. (2015) reported overcrowding and workload to be the most common cause of violence against nurses.
About a tenth (9.0%) of the participants reported to have experienced physical violence. Most of the violent incidents which occurred in the workplace were perpetrated by patients and their relatives, and a significant number of such incidents were not reported. The two most frequent reasons given for not reporting physical violence was “it was not important,” and “I thought no action will be taken if reported.” Certainly, it is not important to report an incident if one thinks that nothing will be done after a report is made. It is therefore important that clear measures are put in place to address the problem. Necessary action must be taken against perpetrators of violence, and nurses who report violence against them should be informed of what action has been taken against the offender.
Limitations
This study excludes nurses working in clinics and health posts located in rural and or remote areas of the country. Nurses working in private hospitals were also not included in the study. The findings of the current study may thus not be generalizable to these sections of Ghanaian nurses. As an inherent weakness of cross-sectional surveys, no cause and effect relationships can be established from the current study.
Recommendations for Future Research and Practice
Future studies could explore whether there are differences in violence exposure among nurses in the private and public health sectors. It will also be useful to have longitudinal studies conducted to ascertain whether intention to quit leads to actual quitting behavior among Ghanaian nurses, considering the fact that unemployment rates are high in the country.
On how to curb the phenomenon of workplace physical violence against Ghanaian nurses, the current article recommends the following:
Educational campaigns could be carried out to conscientize the public on the matter. Legislations and “zero tolerance” of violence policies must be formulated to combat the problem.
Clear reporting procedures must be established by hospitals, and nurses encouraged to report violence against them.
Reports of violence must be acted upon in a timely manner, and affected nurses given necessary support.
Finally, it is important that security is boosted at the various government hospitals, especially the regional hospitals.
Conclusion
The findings in this article are consistent with several studies which have found workplace violence to be a major problem for nurses. The most frequent perpetrators of physical violence were patients’ relations. It is recommended that educational programs are designed to foster awareness on the phenomena and their impacts on nurses and the health care delivery. It is also recommended that clear policies are instituted to address the problem.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.