
Abstract
Although Ghana has developed institutional frameworks and has enacted legislations which among other things seek to guarantee the cooperation and coordination of key stakeholders in disaster prevention, compliance is still a mirage. This has resulted in increased susceptibility of national assets to preventable disasters. This article discusses what might have caused the inferno that razed down one of West Africa’s largest medical storage facilities—the Central Medical Store (CMS). The disaster did not only manifest in property lost, basic medical supplies to neighboring countries were also severely interrupted. By exploring the responses of key stakeholders, the emerging evidence indicates that preventive measures that could have potentially averted the disaster or reduced its impact were not in place. The results further highlighted the apparent weak institutional arrangements toward disaster risk prevention, preparedness, and mitigation, viewed as cross-cutting themes in disaster management. The article argues that the scale of losses from this catastrophe epitomizes how the neglect for building risk reduction can consign an entire region to the mercy of disaster events.
Introduction
One subject matter that has enjoyed extensive academic discourse since the dawn of civilization is disaster. For example, Hanner (2012) has published extensive literature on disasters such as the breakup of the “Challenger” in 1986, the sinking of the Titanic in 1912, the destruction of the Hindenburg as it tried to land in Lakehurst in 1937, the Bhopal Chemical disaster in India in 1984, and the 1944 fire disaster that killed 169 people and destroyed the Ringling Brothers and Barnum and Bailey circus. There are other natural disasters such as earthquakes, storms, floods, famines, and diseases (International Federation of Red Cross and Red Crescent Societies [IFRC], 2001; Pelling, 2010; Wisner, Blaikie, Cannon, & Davies, 2004) that have also equally disrupted the smooth functioning of society. Beyond these natural disasters, other human-initiated disasters—wars, invasions, massacres, riots, and terrorism (Archer & Somsook, 2011; UN-HABITAT, 2008)—have had a devastating toll on humanity. What is important here is that these disasters connote negative feelings and images. Their effects do not only manifest in the number of lives and property lost but also the vital livelihood support systems are perpetually ruined. What is more, the basic infrastructure necessary to respond to the disasters is severely damaged or destroyed. As opined by Amanda Ripley (Time, Inc., 2012), “learning from these disasters means taking a deep breath, long after the satellite trucks have gone home—and reflecting on what we can do better” (p. 1).
In the past few decades, Ghana has experienced memorable disasters (both natural and man-made) with disastrous consequences: They include the earthquake in James Town and its environs in 1939, which recorded 17 fatalities (see Amponsah, 2004); the 1983 drought that battered Ghana’s economy (Institute of Statistical, Social and Economic Research [ISSER], 2010); the 2010 floods in Accra and Swedru, which 42 people lost their lives; the collapse of a six-story Melcom Shopping Centre in Accra that trapped 82 people and caused 14 deaths; the 2014 cholera outbreak that affected more than 22,000 people and claimed more than 200 lives in 5 months (May-September 2014; Ghana Health Service [GHS], 2014); and the June 2015 flood and fire disaster, which claimed more than 158 lives are stark reminders that disasters can leave an indelible mark on human development (Songsore et al., 2009).
Irrespective of the sources of vulnerability in the Central Medical Store (CMS) fire disaster, one question remains unresolved: What might have caused the fire that destroyed such a sensitive facility which not only have national security implications but was also the center of health delivery to millions across the West African subregion? Answering this question is important because, to date, the cause of the disaster has not been established leaving room for and encouraging occasional sensational castigation by the media, politicians, and disaster management experts and organizations who discuss the issue in a unidirectional manner. The objective of this article is to interrogate the range of factors that might have led to the inferno that gutted the CMS, one of West Africa’s largest medical storage facilities. The disaster did not only manifest in property lost, basic medical supplies to neighboring countries were also severely interrupted. The study is divided into six sections. The introductory section is followed by a brief literature on disasters. The third section is devoted to the methodology employed in the data collection and analysis. The next section presents the results, and it is followed by the discussions of the empirical results of the study. The final section of the article presents the summary and conclusion of the study.
Understanding Disasters: A Literature Review
The occurrence of disasters (both natural and anthropogenic) and its implications on development in particular have received increasing attention from academics and policy makers in the past two decades, as demonstrated by the wealth of literature (see, for example, Beall & Fox, 2009; Cretney, 2014; Parnell, Simon, & Vogel, 2007; Pelling, 2003a; UN-HABITAT, 2010). As noted by Pantuliano, Metcalfe, Haysom, and Davey (2012), the increasing interest in disaster research is related to the recognition of surging urbanization in crisis-affected countries, the prevalence of natural disasters in urban areas, and the difficulties confronting humanitarian actors in responding to such situations. “Interest has also been spurred, however, by greater understanding of several interrelated factors that are exacerbating acute and chronic vulnerabilities in such contexts, including climate change and long-term underdevelopment” (Pantuliano, Buchanan-Smith, Metcalfe, Pavanello, & Martin, 2010, p. 1).
Beatley (1989) observes that until recently, scholars in the past perceived disasters to be one-off, unpredictable and natural events. For example, Fritz defined disasters as events that are concentrated in time and space, in which a society, or a relatively self-sufficient subdivision of a society, undergoes severe danger and incurs such losses to its members and physical appurtenances that the social structure is disrupted and the fulfillment of all or some of the essential functions of the society is prevented (Fritz, 1961; Picou & Martin, 2006; Pyles, 2007). This understanding means that the future was virtually treated as independent of the present and perhaps a situation which relegates the two most important concepts in disaster management, “Disaster Resilience” and “Disaster Risk Reduction” (DRR), to the background. Resilience which was first used by Holling (on the ability of environmental systems to absorb impact and reorganize to regain full functionality; Holling, 1973) is used in disaster field as a way of understanding the ability of a system to avoid damage as a result of natural hazard impact. DRR, on the contrary, is defined by the United Nations International Strategy for Disaster Reduction (UNISDR) as
the concept and practice of reducing disaster risks through systematic efforts to analyze and manage the causal factors of disasters, including through reduced exposure to hazards, lessened vulnerability of people and property, wise management of land and the environment and improved preparedness for adverse events. (van Manen, 2014, p. 70)
Consequently, disaster management, which is intended to include building resilience to risk and preventing disasters from occurring (DRR) so that it offers a collective safety net that has the ability to protect the general society from the devastating consequences that may arise from disasters when they occur and that may eventually affect national developments, was envisioned to be a postdisaster activity focusing mainly on rescue, relief, and rehabilitation with emphasis on state-centric approaches (Cohen, 2004). In line with this old thinking, governments were conscientiously infested with this erroneous idea and started creating national disaster management systems, usually of a civil politically tainted nature, to fulfill this mandate (Quarantelli, 1993). In Ghana, for example, the National Disaster Management Organization (NADMO) was established in 1996 to manage disasters and emergencies (Oteng-Ababio, 2013). This was after the country had responded to the UN Declaration, General Assembly Declaration (GAD) 44/236, of 1989 declaring 1990 to 1999 as the International Decade for Natural Disaster Reduction (IDNDR). As these interventions tend to be response-orientated (reactive), authorities ended up spending substantially more in responding to emergencies than on measures that would have helped anticipate and manage risk (World Bank, 2010).
However, in recent times, literature on disasters have focused more on resilience and risk reduction following the launch of the UNISDR and the adoption of the Making Cities Resilient Campaign (Cassidy & Blackburn, 2014), which began in 2010 and runs concurrently with the Hyogo Framework of Action (UNISDR, 2011), which seeks attention to DRR. The Making Cities Resilient Campaign aims at promoting building resilience in cities from several perspectives such as raising awareness of DRR among both national and local governments through high-profile events; providing tools, technical assistance, and training to local authorities; and facilitating city-to-city support networks and learning opportunities (Cassidy & Blackburn, 2014).
The focus of disasters has therefore moved toward consideration of the situation created by such events rather than simply of the origin, nature, size, and speed of onset and other physical attributes of the hazard or event. Undertaking risk assessment as part of a routine comprehensive development process has received much attention especially after some pioneering studies by natural scientists (Intergovernmental Panel on Climate Change [IPCC], 2011; UNISDR, 2011). The World Bank also created a multi-hazard Urban Disaster Risk Index (UDRI) as a tool for baseline risk mapping. Furthermore, the IPCC (2011) has also called for a mix of incremental and transformational changes to reduce the risk from climate extremes. Emerging studies (Gaillard, Liamzon, & Villanueva, 2007; Hilhorst & Bankoff, 2008; Holloway & Roomoney, 2008) consistently demonstrate that the causes of most disasters are embedded in human social, economic, and environmental practices. In other words, the raison d’être of most disasters today have been traced to be the outcome of cumulative risk processes rooted in patterns of human behavior, manifesting in poor land-use practices, ill-conceived development projects, and lack of rules and guidelines. The cornerstone of the Resilient City Campaign, the Hyogo Framework for Action, and the Sendai Framework for Disaster Risk Reduction (United Nations’s post-2015 policy on disasters) is the need to have an institutional basis for implementing risk reduction and the need to involve all sectors and stakeholders. The three frameworks suggest that instead of creating a new sector, expanding the mandate of existing bodies beyond emergency preparedness and response to a coordinating role, bringing together the various functions and expertise of existing government departments to focus on hazard risks can be a priority. This is where many governments in developing countries including Ghana are faltering.
Method
The CMS
The CMS, which is the largest repository of medical supplies in Ghana and serves other West African nations, is located at Tema, the industrial hub and Port city of Ghana and 17 km away from the national capital, Accra. The CMS distributes drugs to all the regional medical stores in supply chain that reaches over 216 districts in Ghana alone. The strategic location of the facility makes it accessible to both locally manufactured and imported pharmaceutical products from all over the world. The facility caught fire on Tuesday, January 13, 2015. The inferno razed to the ground, the entire warehouse destroying equipment and drugs including those for malaria, HIV/AIDS, tuberculosis, and Ebola, among others. The fire which started at about 9:45 a.m. was intense and proved difficult to fight due to the fact that the mix of items stored in the warehouse kept exploding. Second, the fire outbreak coincided with the strong “harmattan winds” (a dry rarefied North East Trade Winds), which also fanned the flames and kept changing the direction of the fire, a situation which hampered efforts at dousing out the fire.
Last, the noticeably lack of water supply in the fire hydrant on the premises also hindered efforts of the firefighters who had to rely on members of the Tema Water Tankers Association (private water suppliers) who carted volumes of water from a nearby hydrant to replenish firefighting vehicles. It took firefighters nearly 30 hr (a day and more) to bring the inferno under control.
Data Collection and Analysis
The fieldwork was conducted in two stages: The first set of data collection was conducted 2 weeks after the incidence has occurred. This was the time memories of the incidence were fresh in the minds of many a Ghanaian and was the time stakeholders were prepared to give untainted information on the perceived causes, officials’ complicities, respond strategies, and the way forward. Again, it was the time when hard core empirical evidence (exhibits) was available. Twenty in-depth interviews were conducted at this level. The interviewees were made up of nine workers from the CMS, five National Fire Service officials, four eyewitnesses, and two policemen.
The second set of interviews was conducted 6 months after the incident and involves semistructured interviews with 10 experts and key stakeholders engaged in DRR at the national, regional, and metropolitan levels. They included two officials from NADMO, two officials from the Ministry of Health (MOH), two from the GHS, two from the Bureau of National Investigations (BNI), and two independent disaster management experts. In addition, the research team analyzed secondary data collected from various sources: examination of reports from state agencies and civil society groups, workshop and conference proceedings, and incident reports. The study also benefited from personal observations and interactions with organizational participants during the rescue exercise. Additional data were obtained from verified transcripts of initial investigative reports and media accounts. The field study allowed an opportunity to understand the disaster scene, and the interviews generally explored respondents’ responsibilities and level of preparedness and challenges. In addition, the respondents’ perceptions about Ghana’s level of preparedness and possible causal factors of the incident were explored and analyzed.
Some of the key questions for those who had direct responsibility for DRR—NADMO, fire service, city authorities, and so on—included their role in the quest for disaster prevention and how past experiences influence future policy formulation and interinstitutional relationship. One common question that ran through all the interviews was, “Do you think the incident could have been avoided (Why or why not)?” Depending on the participant, further questions were asked pertaining to how the quest for a reduction in future disaster events can be realized? Each interview lasted for approximately 1 hr, and all were audio recorded, subsequently transcribed, and finally thematically coded (Chang-Seng, 2013; Taylor-Powell & Renner, 2003). The clear emotional resonances of some of the interviews and the subsequent in-depth empirical analysis of the narratives allowed the author to gauge how official inaction, negligence, or perhaps connivance triggered the disaster. Data triangulation with the datasets provided context for the study and allowed for a greater point of comparison. For the purposes of confidentiality, most of the quoted materials in the article are taken from our personal interviews or culled from literature.
Results
The Genesis of the Inferno
In the event of disaster incident, the first thing is to establish the cause and second to establish whose actions or inactions might be responsible for the disaster. This is important as it helps in developing shocks to reduce its impact as a first response strategy; later, it helps to build appropriate preparedness strategies; and in the long term, prevention capacities are built. The study revealed that the cause of the inferno is hard to pin down. This is because different respondents, depending on their background, gave varied reasons for the cause of the fire disaster (see Table 1).
Responses of Key Informants on the Cause of the Fire.

Note. CMS = Central Medical Store.
At the official level, there was widespread focus on blame games, firmly directed at shadowy political opponents. Rather than finding the cause of the disaster, the scene became the center of intense political activity (see Figure 1).

The disaster scene with intense political activity.
Blaming political opponents for disasters is common practice in Ghana and other African countries. This thinking resonates with the scholarly works of Mileti (1999) and Eiser and Sutton (2012) when they observed in their study that seeking insights into the causes of disasters cannot be properly understood or prevented without attention to the critical role of human agency and societal processes. As observed by disaster scholars (see Lewis & Kelman, 2010), such (mis)conception of the complexities in appreciating, conceptualizing, and understanding disaster risks may blight effort to develop preventive capacities for such disasters.
On the contrary, workers from the CMS believed that the real cause of the inferno which has been described as “mysterious” from the professional point of view was caused by naked and protected fire outside but near the facility. One of such workers revealed in an interview,
The fire may have started when we engaging in our routine burning of some of the expired drugs.
This situation was corroborated by an eyewitness, who mentioned that he saw some men burning some boxes of drugs with petrol, and in the process the fire exploded and got out of hand. He could not, however, confirm whether the “men” were workers from the CMS or that what they (the men) were burning were expired drugs. Other workers from the CMS gave a different account. The workers believed that there was an unprotected fire in the neighborhoods whose source was not known. This fire extended to the highly flammable facility. From all indications, the cause of the fire was not readily known, a situation which also played well into the hands of the spiritual world. A popular spiritual leader in Ghana attributed the cause of the inferno to the gods and agents of the spiritual world (see Table 1).
Fire Safety Standards at the Facility
The Acting Head of Public Relations of the Ghana National Fire Service (GNFS) confirmed the existence and knowledge of well-crafted fire safety regulations both for public and private properties at the national and local levels such as the National Building Regulations of 1996. This notwithstanding, available statistics show that authorities managing such facilities blatantly contravene these statutory regulations. Besides the fire safety procedures, such sensitive and public interest property is also required by law to have a well-secured insurance package. This is part of the resilience building process so that in case of unexpected catastrophe, their impact could be minimal.
The study shows that all state assets are to be insured with the State Insurance Company (SIC) under flexible terms and that there are also simple processes of acquiring fire safety requirements. Among the processes is the approval for planning schemes, and architectural and engineering designs. In addition, installations including fire safety measures and hydrants and the installation of closed-circuit television cameras at all sensitive government installations are to be inspected and certified by the appropriate agencies before permission for occupancy is granted. Our results show that these safety requirements had not been followed through. The research revealed that the fire hydrant at the CMS was out of order at the time the incident occurred. The fire safety certificate for the premises had long expired and fire extinguishers had no foams that could quench any preliminary naked fires. In an interview with an NADMO official, he intimated,
It was obvious this was going to happen, it was so obvious.
He questioned why a facility like the CMS was not well equipped with the latest technology such as smoke detectors and automatic sprinklers which could have mitigated the severity of the damage. Similarly, a BNI official also observed,
The mere fact that the property belong to the government of Ghana implies that the principle of shared risk is applied because all the 25 million people of Ghana have a stake in that property; why did the government not insure the property on behalf of Ghanaians, giving the sensitive nature of the facility.
The General Secretary of the Ghana Chamber of Pharmacy, in an interview, chastised the authorities of the MOH and the GHS for not learning from the numerous devastating effects of recent fire outbreaks to put in appropriate policies to forestall future disasters. He intimated that the recurring disasters including recent fires at public institutions such as the Ministry of Foreign Affairs, the Economic and Organized Crime Unit, and the Public Account Commission should have been a wake-up call for state institutions to put in the necessary measures including enforcing the appropriate laws to avert such incidences. He maintains,
There are several lessons that could have been gleaned from the events before CMS which were blatantly overlooked. Clearly, this incident and many of such nature are due to systemic structural failure, rooted deep in the current poor governance structure, a situation which could have been averted if those responsible have enforced fire safety regulations.
The Acting Head of Public Relations of the GNFS again attributed the poor housekeeping in the warehouse to the spread of the fire. Flammable cylinders and other combustible materials were kept together at the warehouse, a situation which smacks of lack of proper supervision and monitoring. He stated passionately,
What we are seeing are signs of non-conformity to professional practice in warehouse keeping. Items are suppose to be kept in rolls with well demarcated lanes so that in case of any unexpected situation, it does not easily cause great harm to the other items in the same warehouse. As it is now, it looks like no one cared about it.
An opinion leader in Tema who witnessed the incident described the fire disaster as emblematic of the authorities’ inability to enforce fire safety standards. He specifically faulted authorities of CMS, who he opined regularly burn expired drugs close to the warehouse without regard for the health and safety of the nearby residential properties. He suggested that the public would stand to benefit if candid examination of leadership complicities or otherwise at many levels have been included in past disaster inquiries. He explained that, typically, such incidents provoke a big fuss about fire safety standards that ultimately yields no systematic reform.
A Test for Institutional Collaboration and Coordination
The CMS fire also brought to the fore the lack of apparent institutional collaboration and coordination that exist in the disaster management circles in Ghana. At the national level, while the NADMO is mandated by Act 517 of 1996 to coordinate, command, and execute functions in disaster management, it is supposed to do so with the collaboration of other institutions (see Ministry of Local Government and Rural Development [MLGRD], 1996). In addition, a National Disaster Risk Reduction Platform for DRR and National Disaster Management Plan (NDMP) were created in 2005, for which NADMO is the focal point but with representation at all levels of government. However, there is a lack of sufficient institutional coordination, training, and funds and capacity building. Table 2 indicates some of the agencies and their roles in disaster management in Ghana.
Institutional Responsibilities in Disaster Management in Ghana.
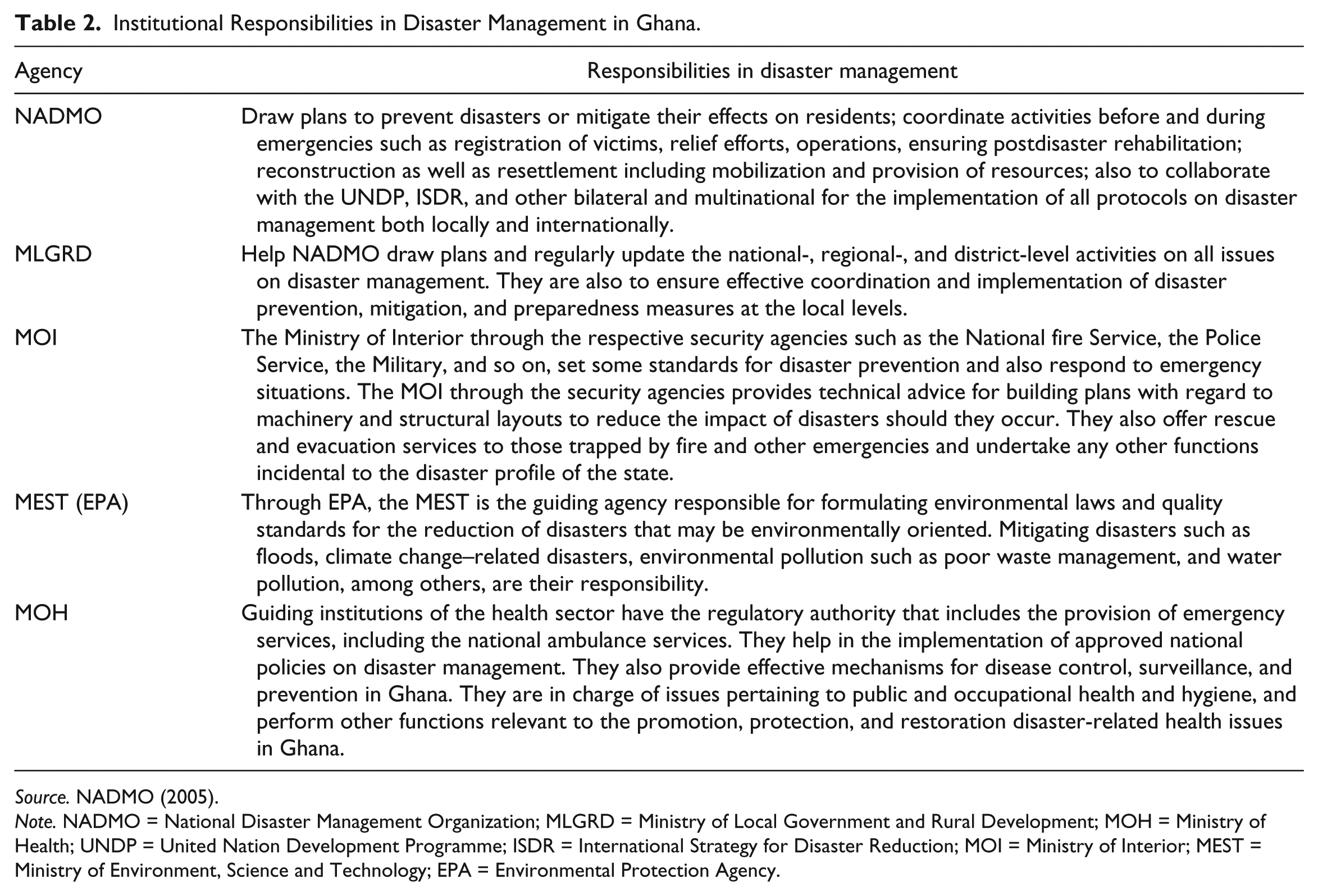
Source. NADMO (2005).
Note. NADMO = National Disaster Management Organization; MLGRD = Ministry of Local Government and Rural Development; MOH = Ministry of Health; UNDP = United Nation Development Programme; ISDR = International Strategy for Disaster Reduction; MOI = Ministry of Interior; MEST = Ministry of Environment, Science and Technology; EPA = Environmental Protection Agency.
The list of agencies involved in disaster management is not exhaustive in Table 2. The study showed some basic problems in the implementation of disaster management framework among the institutions. The major problems identified included lack of effective coordination, limited integration and harmonization of sectoral plans, and limited funds to effectively implement disaster prevention plans. The connections between national sector ministries and other state bodies were not sufficiently developed—such as links between NADMO, the MLGRD, and the Ministry of Interior (MOI). Moreover, NADMO receives limited government support in terms of engaging relevant sector agencies in disaster management. Although legislation in areas related to DRR exists, such as the Millennium Development Authority Act (2006), Administration of Lands Act (1962), and over 26 laws on environmental issues, their coordination and implementation seem to be a problem.
The extent to which these laws are to be rolled out and enforced would require the support of all allied institutions; this was corroborated in an interview with a key informant (an officer from the National Fire Service). He intimated,
Disaster risk management which is supposed to be a collective responsibility is still being treated as an individual affair by NDAMO. This tendency defeats NADMO’s mandate of improving upon its role of coordinating and harnessing all resources both human and material from all partners for timely and effective response emergencies. Not tapping the expertise of the GNFS, Ghana Ambulance Service, and Ghana Police has resulted in a dispersion of effort and an ineffective use of the scare resources of the nation. Consequently, the needed political support for DRR has also gradually waned.
He stressed further that providing tools to enable translating national policies into mainstreaming planning processes would help the nation in understanding the options that are available for managing risks and for planning and implementing local-level DRR strategies. This situation defeats the purpose and implementation of the Hyogo Framework for Action. The key informant concluded that if the institutional efforts had been harnessed together in the management of the CMS, the fire may not have occurred or its effects would have been minimized. In any case, that is the essence of DRR.
Early Warning Systems and Signs
The study further revealed that early warning systems (mostly in the form of smoke and fire detection devices, regular maintenance and inspection of safety procedures) were not adhered to. The study also revealed that officials whose duty it was to manage the facility were not abreast with the combustible nature of the drugs in the stores. The study could not cite any report on monitoring and assessing disaster risks preparedness of the facility through the different systems in place. Risk assessment data, including classification of chemicals at the facility, were not readily available. In terms of human capacity, official workers at the facility lacked the needed disaster preparedness skills to emergency disaster services, a situation which further aggravates the development of any early warning system. Although no lives were lost, the emotional storylines of some workers at the CMS, most of whom belong to the lower tier on the institution’s management structure alleged that before the disaster, they repeatedly alerted top management of the fact that most of the fire extinguishers had expired and also warned against the regular burning of expired drugs near the facility but to no avail. A respondent, for example, angrily shared his experience in response to a question on what he thinks went wrong:
It is unbelievable that top managers of this facility who take huge salaries at the end of the month will not listen to us anytime we make a report. On several occasions, we reported to the managers to bring the fire service people to bring new extinguishers but they will not listen. There were also plans to train us on how to handle some of the emergency equipments but this has also not taken place. It looks like they [management] do not care about the safety of the place; all they think about is their monthly salaries. But for their [management] greed and selfishness, they could have averted this calamity. If only they had listened to our many complaints.
An insurance consultant blamed management of CMS for negligence. He intimated that it is the government’s responsibility to ensure the safety of such national asset. To him, management, and for that matter government, was guilty for what had happened. An engineer consultant and former public official questioned the structural integrity and quality of the building and blamed the “red-tapism” for the nonconformity to fire safety standards. As part of measures to prepare against future incidences (and develop early warning system), he advocated for an “urgent streamlining of physical planning and building regulations” and the retraining and improving the capacity of officials responsible for managing the facility. Contributing, a private safety coordinator stated emphatically that the CMS disaster could have been avoided if management had been proactive by going the extra mile to address the observed deficiencies in the structure.
Counting the Cost of the Disaster
Like the economic effects of many fire disasters in Ghana, the study revealed that CMS disaster destroyed hundreds of thousands worth of medicines, equipment, and hospital facilities belonging to Ghana and the World Health Organization. The study further revealed that medical supplies worth GHS 237 million (US$68 million) were destroyed and that the country lost 3 months drug reserve and the ability to replenish the lost stock in time is very questionable, meaning lives are at risk. While the direct cost was not easy to equate, the indirect cost was very difficult to estimate as our study revealed that more than 10 highly placed staff connected with CMS were interdicted. What is clear is that the indirect cost will take years to manifest and Ghana will over the years go on paying for the impact of this fire incident. From all indications, the CMS fire disaster has a greater significance and disproportionate impact on the health care delivery in Ghana. The direct and the indirect costs of the CMS fire disaster were very astronomical, and Ghana being a lower middle-income country whose budget is financed by subsidy allocations from donor countries cannot afford to lose such national asset through a cause that could have been avoided. Conservatively, the cost of preventing the fire incident could have been far lower than the current situation of restoration. It is therefore prudent that the state takes proactive measures to reduce the risk of fire incidents in the country, if sustainable development is to be achieved.
Discussion
After the CMS fire disaster, the government of Ghana and the entire society profoundly reflected on the precautions that were not taken against such an incident. Again, national discourse also centered on how new measures can be taken to provide a solid foundation so that Ghana can cope with or prevent future occurrences of such disaster events. The national introspection highlighted the apparent weak institutional arrangements toward disaster risk prevention, preparedness, and mitigation in Ghana, a situation that has also been giving extensive attention in some previous studies. Building disaster risk prevention is viewed as cross-cutting themes in disaster management and therefore requires proper coordination of all institutions concerned with disaster management (Chang-Seng, 2013; Oteng-Ababio, 2011; Pelling, 2003). The framework for disaster management in Ghana which is placed under the MOI also mandates the Ministry to work with the Ministries of Finance, Health, Environment, and Works and Housing, among others, to deliver proper disaster prevention services.
The framework further enjoins such institutions as the National Fire Service, Ambulance Service, the Ghana Police Service, the SIC, and other allied institutions to work in a coordinated effort to build resilience to disasters. It is therefore baffling that given the evidence of these well-established institutions with the mechanisms and capacities, such state asset could not be protected against the unexpected disaster. It is even more baffling to come to the realization that there are many examples from the global north which typify how institutions have collaborated to prevent the occurrence or reduce the impact of disasters of which the disaster management institutions in Ghana could have learnt from (Satterthwaite, 2011). In principle, the fundamental goal that underpins disaster management as suggested by Pelling (2003) which is to reinforce the centrality of all disaster concerns and adopt preventive strategies and practical measures to reduce its potential human and property losses should not be the responsibility of one institution but should be an activity of several institutions with one common interest—the building of resilience.
As opined by Oteng-Ababio (2013), sustaining effective disaster risk preparedness unequivocally demands strong political commitment and durable institutional capacities, which among other things will guarantee the cooperation, coordination, and collaboration among key stakeholders and developmental activities (see also Morrice, 2013). However, the CMS disaster as well as the increased frequency and destructiveness of recent disasters in urban Ghana have come to question the political commitment and institutional capacities in preventing disasters. These disaster events seem to suggest that disaster management institutions are working at worlds apart. The CMS disaster has brought to the fore the need to understand the institutional and legislative systems for building preventive mechanisms against disasters. The disaster has also highlighted the inextricable links between disasters and human development as its impact has a devastating toll on health care delivery not only in Ghana but also in other countries in the West African subregion. Events and the national discourse on the disaster seemed to suggest that there appears to be a lack of platform that enables stakeholders in disaster management to cooperate, coordinate, and reconcile agendas; negotiate share-knowledge; or critically reflect on lessons learnt from past incidents of such nature.
DRR is regarded as a critical component of any sustainable development as evidence with the passage Sendai Framework for Disaster Risk Reduction document to guide nations on their DRR programs for the next 15 years (2015-2030) coinciding with the targets of the Sustainable Development Goals (World Bank, 2006). The Sendai Framework for Disaster Risk Reduction among other things articulates the need for improved understanding of disaster risk in all its dimensions of exposure, vulnerability, and hazard characteristics; the strengthening of disaster risk governance, including national platforms; accountability for disaster risk management; preparedness to “Build Back Better”; recognition of stakeholders and their roles; mobilization of risk-sensitive investment to avoid the creation of new risk; resilience of health infrastructure, cultural heritage, and workplaces; strengthening of international cooperation and global partnership; and risk-informed donor policies and programs, including financial support and loans from international financial institutions. This increased recognition has been fueled by the seemingly intrasectoral fragmentation of disaster risks preparedness framework, a challenge which Chang-Seng (2013) describes as not providing mechanisms for feeding back into capacity building toward the formulation of disaster management policy and guidance. The CMS fire incident severely exceeded the capacity of city authorities to provide emergency services. Among the factors accounting for this include the nonenforcement of statutory state building regulations and the lack of early warning signs toward disaster. In the main, the management failed to reorganize and learn from many of the past fire incidences in Ghana. Public agencies’ disaster preparedness activities and efforts appeared rather ad hoc, fragmented, and uncoordinated, while their cooperation across levels and scales was basically lacking.
The scale and magnitude of losses from the CMS disaster defy easy generalization. The study further revealed that even with the ratification of the Hyogo Framework for Action in 2005 (United Nations, 2005), which mandates Ghana to build DRR strategies against fire disasters, designing and implementing fire DRR strategies into all programs and policies was not well articulated. The CMS disaster connotes the prize the country paid for paying inadequate attention fire risk. Although Ghana is making some progress with the actualization of the Hyogo Framework for Action (NADMO, 2015), reducing fire risks to public assets seems to be a mirage. This is evidence from the many public facilities that have suffered preventable disasters. In Accra, for instance, the outbreak of fires in the two largest markets, Makola and Kantamanto, has become almost weekly affairs (Oteng-Ababio, Ohene Sarfo, & Owusu-Sekyere, 2015). About 352 fire events were recorded between 1990 and 2002 with an estimated loss of about US$5.4 million (Oteng-Ababio et al., 2015). In the case of the Kumasi Central Market, which is the largest open-air market in West Africa, the market experienced four devastating fire outbreaks within a spate of 3 years: May 28, 2009; January 2, 2010; and December 30, 2012. Such distressful experiences leave deep and indelible scars in the minds of the fire victims. What is even more distressful relates to when the populace begin to count their losses and also come to the realization that the possible causes of the incident could have been avoided.
Again, the study indicates that the scale and magnitude of the CMS fire was due to the physical morphology and governance structure of the facility. The disaster inevitably cause upheavals not only in the physical environment but also in the social and economic context. Close examinations of the facility reveal that it carried physical vulnerabilities due to its location or construction practices. Physical examination revealed that the facility had many structural defects, and many of the inner chambers where medical supplies were kept were just temporal compartments without adequate fire risk reduction safeguards. This situation is in sync with UN-HABITAT (2008) describes as “structures derived from village prototypes but are modified by the requirements of space and the availability of materials—plastic, tin, bits of cloth, wood and bricks, which draw on past and present materials” (p. 69). Available data at the GNFS show an annual increasing incidence of urban fire in Ghana (GNFS, 2013). The increasing frequency of fire outbreaks in the face of escalating demographic pressures pose a significant challenge to the extant institutional and urban governance structures, which have tended in most cases, to deal with the problem in a reactive, ad hoc and often ambiguous manner.
Summary and Conclusion
The study set out to investigate the multiplicity of factors that led to the fire that destroyed the CMS, one of the largest storage facilities for medical supplies in the West African subregion. From all indications, the CMS disaster evokes some element of institutional failure and ineptitude. While the technocrats believed the incidence resulted from nonenforcement of disaster prevention procedures and standards, civil society and other individuals identified corruption and inefficiencies as a major bane. Irrespective of the source of vulnerability, the study highlights the fact that noncompliance with institutional and governance framework contributed to the disaster.
The after events and discourse on the CMS fire disaster revealed that the incident could have been potentially averted if all key players in disaster management had played their respective roles diligently. By engaging the available documents and exploring the responses of eyewitnesses about the root causes of the incident, the study sheds more light on how the fundamental policies underpinning DRR and disaster preparedness were virtually nonexisting or, in some cases, overlooked. Generally, the thinking and understanding of disaster risk management is changing. The subject is being increasingly recognized as a major factor in achieving sustainable development. Emphasis is now being laid on risk reduction with the ultimate aim of taking a holistic view of DRR and the importance of linking with diverse stakeholders, taking a cue from the Hyogo Framework for Action and the Sendai Framework for Disaster management. In implementing the frameworks in Ghana, there will be the need to enhance the capacity of emergency response organizations. There is also the need for major state institutions to vigorously integrate DRR interventions into their development plans and projects. As a recommendation, there should be periodic (preferably, monthly or bimonthly) risk assessment of all sensitive public assets to gauge the measures that are being taken to reduce the impact of any risk, should there be one.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.