
Abstract
Many persons with leg amputations experience that using a prosthesis enriches their quality of life. However, there is an ongoing concern with underuse and non-use of artificial limbs in lower limb prosthetic rehabilitation. Studies have identified an initial critical stage among potential prosthetic users. The aim of this study was to explore the lived experience of becoming a prosthetic user as seen from the perspective of patients. The study is based on the phenomenological framework of Reflective Lifeworld Research (RLR). Data were collected through three in-depth interviews with each of the eight participants during the first year post-amputation. Data were analyzed according to the guidelines given in RLR. The findings showed that the participants found themselves in a state of in-between existence. They felt disconnected from their usual lives and not yet integrated in a new and different life. In this in-between existence, the participants oscillated between experiences of victory and defeat. The study adds to increased understanding of the initial critical stage of becoming a prosthetic user by showing that this in-between existence is inherent in the process of becoming a prosthetic user. To become a prosthetic user requires a high degree of stamina and resilience as this in-between existence takes its toll on patients’ recovering process.
Keywords
An ageing population and lifestyle-related illnesses, such as diabetes and peripheral vascular disease, have increased the prevalence of leg amputations internationally (Schaffalitzky, Gallagher, Maclachlan, & Ryall, 2011). Regardless of etiology, a leg amputation is usually followed by major physical and psychosocial challenges that severely influence the person concerned (Murray & Forshaw, 2013; Norlyk, Martinsen, & Kjaer-Petersen, 2013; Ostler, Ellis-Hill, & Donovan-Hall, 2014; Washington & Williams, 2016). Reduced quality of life (Davidson, Khor, & Jones, 2010; Remes et al., 2010), significantly higher levels of social isolation, depression, and post-traumatic disorder (Horgan & MacLachlan, 2004; Remes et al., 2010) are reported particularly in the first year after the amputation (Phelps, Williams, Raichle, Turner, & Ehde, 2008). Furthermore, a leg amputation includes an existential dimension that refers to limitation of action space and loss of freedom experienced as an exclusion from life (Norlyk et al., 2013).
The prescription of a prosthesis is a key component of the rehabilitation process for persons with lower limb amputation (Schaffalitzky et al., 2011; Webster, Hakimi, & Czerniecki, 2012). Several studies have shown a direct link between locomotor capabilities with prosthesis and increased levels of autonomy, self-esteem, and improved social life (Jefferies, 2015; Murray, 2009; Murray & Forshaw, 2013; Schaffalitzky et al., 2011; Senra, Oliveira, Leal, & Vieira, 2012; Zidarov, Swaine, & Gauthier-Gagnon, 2009). However, not everyone will benefit from the provision of a lower limb prosthetics or will learn to master its use. Reported rates of prosthetic use can vary from 49% to 95% (Schaffalitzky et al., 2011), and there is an ongoing concern in lower limb prosthetic rehabilitation with underuse and non-use of artificial limbs (Murray, 2009; Schaffalitzky et al., 2011). A growing number of studies highlights the importance of psychosocial support together with physical rehabilitation in facilitating patients’ prosthesis use (Coffey, Gallagher, Horgan, Desmond, & MacLachlan, 2009; Ostler et al., 2014; Schaffalitzky et al., 2011). Ostler et al. (2014), for example, pointed to a need for psychoeducation interventions and concluded that, within prosthetic rehabilitation, “more time should be dedicated to talking, rather than just walking” (p. 1174).
Many persons with leg amputation experience that using a prosthesis enriches their quality of life and greatly increases their psychological health and well-being (Liu, Williams, Liu, & Chien, 2010; Murray, 2004, 2009; Murray & Forshaw, 2013). Murray (2004) found that adapting to a prosthesis was an ongoing activity and that initial problems became more manageable over time. However, Murray (2004) underlined that for potential prosthetic users, there is a critical period between an initial experience of prosthesis use as unnatural to the subsequent feeling of prosthesis use as natural. If this initial critical period is unsuccessful, Murray (2004) argues, patients may tend toward rejection of prosthesis use. In a later study on prosthetic users and their experiences, Murray (2009) found participants describing the process of learning to use an artificial limb as painful and arduous. Some participants even talked about hating their prosthesis initially.
This finding of an initial critical period among potential prosthetic users is further supported in a recent qualitative meta-synthesis aiming to identify issues of key concern among people who undergo an amputation and begin using prosthesis (Murray & Forshaw, 2013). The meta-synthesis showed that prosthesis use required both a physical and a psychological adjustment. Facing prosthesis use was an emotional challenge and an ambiguous experience for patients; they often felt both dependent on and limited by the prosthesis. The patients appreciated the benefits that a prosthesis could offer such as independence and freedom; however, they still experienced a profound loss of limb and their former physical capacity (Murray & Forshaw, 2013). Focusing on patients’ expectations of undergoing prosthetic rehabilitation following a leg amputation, Ostler et al. (2014) found that patients experienced many unknown aspects of the process that followed. They wondered about the rehabilitation process and whether they would eventually learn to master using the prosthesis.
The rehabilitations process for potential prosthetic users focuses on establishing a higher quality of life for the individuals concerned. One of the main goals is to enable potential prosthetic users to regain mobility (Murray, 2004, 2009; Zidarov et al., 2009). To improve support and care for potential prosthetic users following a leg amputation, the experience of being supplied with a prosthesis needs further investigation. In-depth knowledge is needed about the process of becoming a prosthetic user, that is, from a perspective characterized by “insiderness” (Todres, Galvin, & Dahlberg, 2014, p. 1). Consequently, the aim of this study was to explore the lived experience of becoming a prosthetic user as seen from the perspective of persons who have lost a leg.
Method
The study was conducted within the framework of Reflective Lifeworld Research (RLR). This approach builds on epistemological assumptions from continental lifeworld theory developed by phenomenological philosophers such as Husserl, Heidegger, and Merleau-Ponty (Dahlberg, Dahlberg, & Nyström, 2008). Fundamental assumptions within this methodology are that life manifests itself in experience and that the human body can never be understood merely as a biological thing controlled by the mind. The body is an entity of subject and object; it is a living whole. Human existence means “being-in-the-world” and “the body is the vehicle of being in the world” (Merleau-Ponty, 2005, p. 94). Through our bodily existence, we relate with things, others, and the world itself, and we constitute meanings through our engagement in the world (Dahlberg et al., 2008). Meaning refers to an original givenness and to how the things present themselves for us in our interrelationship with the world (Dahlberg et al., 2008). In RLR, the question of lifeworld meanings is the focus. Describing the lifeworld meaning is feasible when the researcher approaches participants with an open mind taking nothing for granted. The researcher works by way of a bridled process of understanding to be surprised rather than imposing personal ideas on the material (Dahlberg et al., 2008). Hence, the phenomenological approach opens up the possibility to capture the meanings of becoming a prosthetic user as experienced by the persons themselves prior to any application of theory.
Participants and Setting
The participants of the present study were recruited from a Danish university hospital. When their physical condition allowed for prosthetic training, participants received 2 weeks of individualized training by a physiotherapist while staying at the hospital’s patient hotel. The follow-up training was not standardized. Training was planned depending on the participants’ individual needs and the training offers available in the participants’ local community.
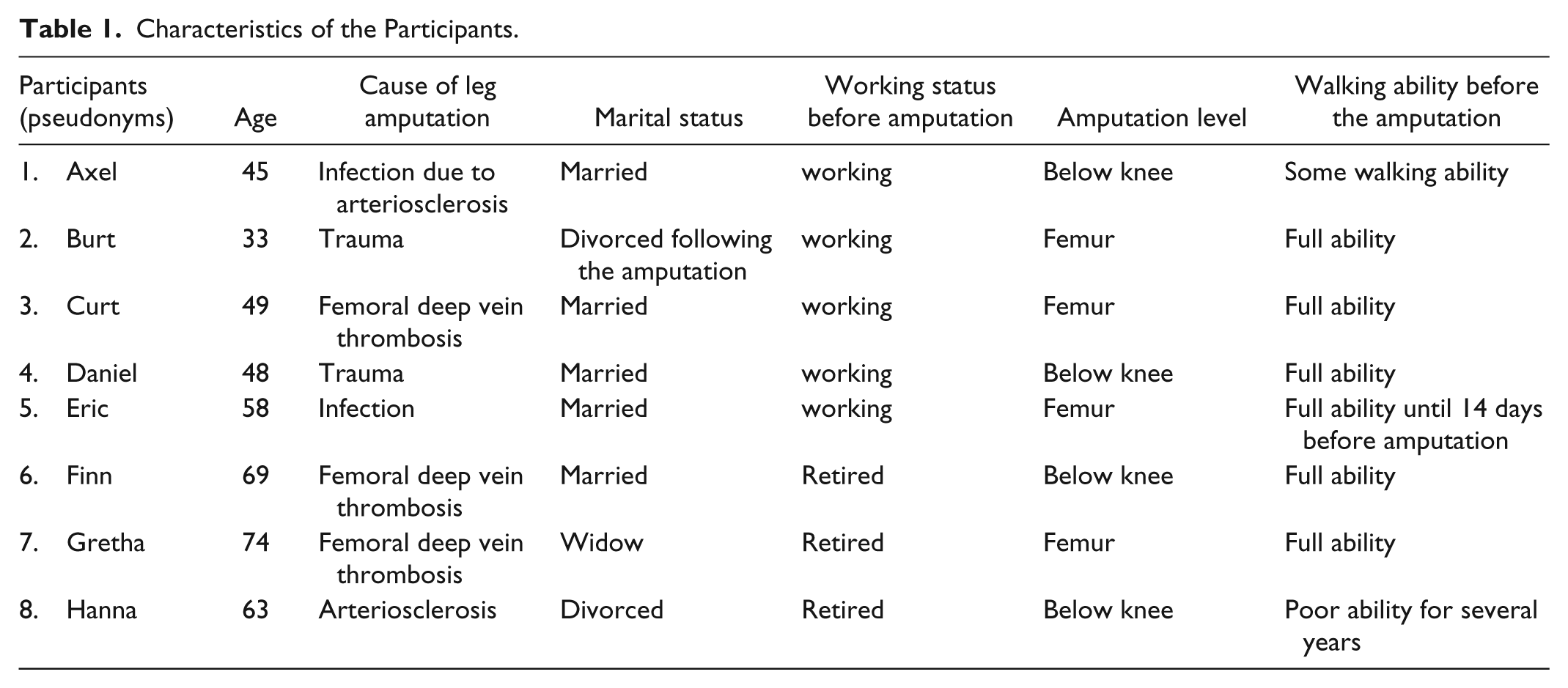
Inclusion criteria were Danish patients who had undergone a non-malignant leg amputation, discharged to their private homes, and referred to prosthetic training. Six men and two women, aged between 33 and 74 years, participated in the study. The participants had undergone amputation of different etiologies. The characteristics of the participants are shown in Table 1.
Characteristics of the Participants.
Participants were invited to participate in the study by their physician or nurse. Subsequently, the first author contacted participants who had accepted to participate. Variations in the patients’ physical condition meant that the start of prosthetic training was based on individual assessments.
To study patients’ experiences of becoming a prosthetic user while they were living through the process, data were collected through three in-depth interviews with each participant during the first year post-amputation.
Interviews
The first interview took place about 4 weeks post-discharge, while the second interview was conducted 4 to 5 months later. The third interview took place approximately 1 year after the amputation. The researchers had no clinical experience as concerns prosthetic rehabilitation. The first author (A.N.) conducted all the interviews in the participants’ homes. The interviews were meanings-directed and characterized by a dialogue in which the researcher sought to facilitate the participants’ description of the lived experience as detailed as possible (Dahlberg et al., 2008). The first interview focused on participants’ experience of how the amputation had influenced their daily life and on their expectations of the prosthesis. In accordance with the phenomenological approach, the interview questions were not predefined. The researcher approached the participants with an open mind taking nothing for granted. The participants were encouraged to use their own words and to talk about what really mattered to them in the process of becoming a prosthetic user. In the first interview, for example, the opening question was “Please tell me how living with one leg influences your everyday life?” Additional questions were asked to deepen participants’ description such as “What happened next?” or “Please give another example of this?” The second and the third interviews focused on participants’ experiences of becoming a prosthetic user. In all interviews, the participants were encouraged to describe and elaborate on concrete situations from their everyday life. The interviews were audio recorded and transcribed verbatim.
Ethical Considerations
Ethical considerations followed the basic principles for research given in the Helsinki Declaration and the Northern Nurses’ Federation (2003), and the study was approved by the Danish Data Protection Agency (ID No.116028312). The participants received verbal and written information about the purpose of the study, the right to withdraw, and the confidentiality of the data given. According to Danish law, formal ethical approval of the study was not required.
Data Analysis
Interviews were analyzed according to the RLR guiding principles. The researchers focused on discovering patterns of meanings and variations to describe the essential meaning of the phenomenon (Dahlberg et al., 2008).
The analysis began with repeated readings of all transcripts to get an overall sense of the descriptions. Then followed a process of carefully exploring each transcript and dividing it into meaning units. Subsequently, each meaning unit was the subject of reflection to discover meanings that disclosed experiential aspects of becoming a prosthetic user. An intensive dialogue with the text characterized this search for meanings exemplified by questions such as “What is being said?” “How is it said?” and “What is the meaning?” These questions were supplemented by critical and reflective questions such as “Is this the actual meaning or is there a different meaning?”
The emerging meanings were clustered into a preliminary pattern of meanings. Subsequently, a process of open reflection followed to synthesize the meaning units into a new whole that clarified the essential meaning of the participants’ descriptions. As described by Dahlberg et al. (2008), this open and critical attitude aimed at achieving scientific objectivity during the research process. The researchers took on this attitude and discussed the emerging understandings of participants’ descriptions of becoming a prosthetic user. Quotes from the interviews are provided as examples of explicated meanings.
Findings
The essential meaning of becoming a prosthetic user after a leg amputation is characterized by the experience of being in an in-between phase. The participants are neither living their usual life nor are they integrated in the life changes that require them to cope with daily life in new ways. The participants experience the reduced mobility as a reduction of their former life, and the prosthesis symbolizes the lifeline back to their previous active life.
Becoming a prosthetic user means that the very act of walking changes from being a natural bodily movement to a planned movement with the prosthesis. Walking with a prosthesis eventually becomes a natural movement as the participant learns to master the use of the prosthesis and acquires the necessary new skills and habits. The ability to move around with the prosthesis is associated with a sense of freedom, independence, and the re-conquering of daily life. However, the participants also experience that becoming a skilled prosthetic user requires committed training, courage, and stamina. In this process, the participants oscillate between victory and defeat.
The essential meaning is further elaborated in the five constituents described as follows: Living on Standby, Standing on Your Own 2 Feet Again—Tall and High, Becoming One With the Prosthesis, A Test of Stamina, and Re-Conquering the World.
Living on Standby
After the amputation, participants experienced feelings of living on standby in the waiting time between the amputation and the start of prosthetic training. To the participants, the loss of a leg was a major life change, which limited their daily lives. They looked forward to using a prosthesis. The loss of mobility and the dependence on help and walking aids led to feelings of isolation and restricted freedom. Consequently, the participants experienced missing out on life and they frequently despaired. They feared that they would be unable to live the lives they had lived before the amputation. The support from family was important in participants’ daily struggles, and they emphasized that their families also experienced major changes and new demands. Participants were afraid of becoming a burden to their partner, and some feared that their relationship could not sustain the change. Normal everyday actions turned into problems, which influenced participants’ self-perception negatively.
It is terrible to no longer to be able to do what you used to . . . you get into situations, where you get sad when the wife for instance says: “The handle fell off the bathroom door.” I am a skilled labourer, and have always been able to fix things around the house, and now I suddenly cannot do very much . . . all I think about is to begin wearing the prosthesis and to walk again. (Finn, first interview)
The participants hoped that prosthetic training would enable them to resume former daily routines. Waiting for the prosthetic training was exhausting. It was like being in limbo marking time, doing monotonous exercises, and living on standby.
Occasionally I have days where I don’t get anything done. I just turn on the TV and do absolutely nothing . . . it is as if my life is reduced to exercises and more exercises and getting help with everything . . . (Hanna, second interview)
The experience of being in limbo was especially emphasized by participants, who had experienced complications such as prolonged wound healing, which delayed the training. These participants experienced the prolonged waiting time as extremely frustrating and demotivating especially as concerned the preparatory exercises. However, once a fixed time for the start of the prosthetic training had been set, these participants experienced a new surge of energy.
Because it took such a long time for the wounds to heal, I have had some serious psychological issues . . . however, now I have an appointment for prosthetic training in a couple of weeks and I just cannot wait . . . However, there was a long phase where I did not have the energy to do my exercises because the prosthetic training seemed to be way into the future. (Finn, second interview)
Standing on Your Own 2 Feet Again—Tall and High
Participants experienced the world differently from an upright position. Wearing the prosthesis and standing upright for the first few times was a very emotional experience, which reminded participants that the world is designed for people who walk upright. Being in an upright position signaled normality and contributed at a concrete level to the experience that walking again was a real possibility. Furthermore, standing up meant that the symmetry of their personal relationships could be re-established. Standing up and taking the first few steps with the prosthesis was experienced as a victory and a turning point.
I feel tall as well as high . . . tall because I’m standing up and not in a wheelchair and high because I can do it. (Hanna, third interview)
Standing up by wearing the prosthesis gave rise to both pride and anxiety. The participants experienced the shorter leg as a considerable bodily change; they needed to familiarize themselves with their new body to re-establish physical confidence and a regain a new sense of balance.
The first time I stood up was challenging (laughs) or something (cries) . . . suddenly I was no longer sitting down, but standing on that stilt (laughs) . . . and I was very anxious to see if I would fall over immediately or if my legs would collapse. (Axel, second interview)
Being able to stand and walk again was an experience of both concrete and symbolic significance. The symbolic significance was associated with the meaning of being physically at eye level with other people. To stand up meant re-establishing the experience of relating to other people on an equal basis in contrast to communicating from the lower position of a wheelchair.
These days, when talking to the neighbour, it is completely different from when I was in the wheelchair. When you are not at eye level . . . it is like . . . people do not address you 100% . . . but now that I am standing up, it is a completely different experience. (Eric, second interview)
Life in a wheelchair created asymmetric relationships. Moreover, participants experienced that the wheelchair limited their opportunity to have physical contact with their loved ones. Standing up and being able to walk meant that they could take the initiative and show their partner love or gratitude.
The world is suddenly perceived in an entirely different perspective . . . that is when you have sat down for nearly a year and you then suddenly get up . . . then it is like wow . . . and to stand up and look my wife in the eyes . . . and give her a kiss, hurrah . . . instead of just leaning back and tilting your head to receive a kiss. Now I can also give a kiss . . . and when she cooks and I go to her on my crutches, then she is so happy (moved to tears) . . . (Curt, third interview)
Becoming One With the Prosthesis
Although standing up and taking the initial steps represented the first milestone, the participants experienced that the main challenge was to become confident with the prosthesis and to integrate it as a natural extension of the leg. Walking with the prosthesis changed from being a conscious act to eventually becoming a new habit that did not require attention. The participants experienced the previously automatic act of “walking” as a new learning process. First of all, they needed to divide the walking movements into many smaller sections they had to remember.
You don’t just click on the prosthesis and take off . . . suddenly you need to consider walking in a new perspective . . . Putting one foot ahead of the other, lifting the foot, then stretch the knee and tighten your muscles. All of a sudden there are a number of things you need to control, things that used to be second nature . . . This is probably the hardest thing; the fact that you must think so much about the process of walking . . . previously you just moved your feet. (Axel, second interview)
An unstable balance could be frightening and discourage the participants from trying to walk without the use of a walking stick. In contrast, feeling safe and secure could stimulate participants’ courage to challenge themselves. Participants, who had had the appropriate physiotherapeutic training in the use of a prosthesis in their own home, experienced that this training was of special significance as it helped them to address the hurdles in the home, and to incorporate skills they could not define. Through conducive pressure, the physiotherapist could stimulate the participants’ courage in a way that gave them a sense of victory.
When I first crossed our doorstep I felt victorious because I had been looking at it many times. The threshold kept getting higher and higher (laughs) . . . but then the physiotherapist said: “try lifting first one leg and then the second leg across the threshold,” . . . and then I dared to try, when he was around. (Eric, second interview)
As the participants incorporated the new walking routines, the prosthesis no longer required their full attention. At first, the participants experienced this situation in flashes of insight, as they suddenly realized they had moved around without paying attention to the prosthesis. This only occurred when the prosthesis did not cause pain or discomfort. Having faith in the skills of the surgical appliance maker and being taken seriously about problems with the prosthesis became decisive to the participants’ experience of the fit of the prosthesis.
Not until the various daily routines of the use of the prosthesis became second nature did the participants experience the prosthesis as a fully integrated aid.
You need to create a day-to-day life, where you do not think so much about it anymore. It needs to become a routine that you need to put on a sock in the morning, and remember to wash it before going to bed in the evening . . . it should be like brushing your teeth. Something you do without even thinking about it. (Daniel, third interview)
A Test of Stamina
The participants experienced that becoming a prosthetic user required stamina. The building up of muscle mass and the training in using the prosthesis were constant focal points in their daily lives. Professional support helped them optimize the experience of becoming increasingly capable and the training program at home became very significant. However, participants could occasionally experience that the prosthetic training became too dominant as illustrated below.
I do not intend to spend my entire life learning to walk with the prosthesis . . . after all, I am 77 years old and, you know, I feel that there are other things in life as well . . . My physiotherapist now seems to think that I should also wear the leg in the afternoon . . . but then there will be no time for anything else but walking with the prosthesis, . . . so I will not (emphasis) do that . . . there should also be time left for other activities. (Gretha, third interview)
Even if the participants expected to adapt to the prosthesis, they were often surprised that several types of prosthesis adaptations could occur, had high expectations of every single adaptation, and were disappointed if problems with the prosthesis recurred. For participants who had pains in the remains of the leg or who needed several prosthesis adaptations, these ongoing adaptations were experienced as particularly challenging. Recurring adaptations affected both participants’ stamina and belief in the prosthesis negatively.
Participants, who experienced adaptation difficulties and temporarily had to make do without their prosthesis, feared that their training was wasted. They experienced feelings of extreme adversity and doubted they would ever succeed in becoming adept at using the prosthesis. This further challenged the stamina necessary to resume the prosthesis training. In those situations, the wheelchair could become a tempting alternative to the challenge of the prosthesis. The wheelchair was an easy option; it offered comfort and made no demands.
It has been a long summer because I had just begun walking and then the prosthesis was torn away from me for 6 weeks . . . that broke my spirit somewhat and I have been fairly defaitistic. (Curt, second interview) . . . This is my third leg in 4 months and every time I have been so disappointed . . . because . . . it did not work after all and then began another long waiting period . . . I am at a standstill again. I just start walking and then I am back to sitting down . . . and finally the wheelchair becomes a kind of a refuge . . . because you know you can trust it . . . But now that I have my leg again, my mood improves. But it is like starting all over again . . . It is hard work . . . It is like pulling yourself up by the bootstraps, because I must (emphasis) move on. (Curt third interview)
Participants who sought information about this difficult part of the process found that the information accessible tended to give an unrealistic picture of becoming a prosthetic user and of the stamina required.
On YouTube you see the start-up, then you see how quickly persons with leg amputations succeed . . . then you think it is going to be a piece of cake to get to that stage. You do not get an impression of the roadmap and how difficult the process has been for these successful people . . . you only see the beginning and the end . . . you are not told of the phase between (emphasis) beginning and end . . . and I wasn’t aware of that middle phase. (Finn, third interview)
Re-Conquering the World
Depending on the degree of regained mobility the participants strived to re-conquer a daily life that resembled their previous lives. Being able to walk with the prosthesis, however, regenerated experiences of freedom and independence. Succeeding in resuming previous activities or traditions was a victory. The participants experienced they were moving toward the re-conquering of everyday life although it was a different kind of everyday life.
Some participants regained a high degree of mobility and were able to walk without stick, while others had to use a walking stick. Walking without any aids at all remained the ultimate dream for some participants.
I dare not have too high hopes . . . But I do have a dream that I can walk down the street without a stick for support, that is a big dream (emphasis) . . . and it would be a major victory for me to go shopping without anyone realizing that I walk with an artificial leg. (Hanna, third interview)
Other aids such as a handicap car or a crosser also contributed to the participants’ mobility and helped them to regain their former everyday life. The participants experienced their dialogue with the municipality as a struggle if they needed to justify evident needs such as the need for training or necessary aids.
After seven months the municipality thought I would be walking normally . . . and that I would no longer be needing my electric scooter or my wheelchair! . . . And then I thought, but hello . . . I need to sit in the wheelchair to rest if I get a pain in my leg . . . But that is what they assumed! I quickly get annoyed with them. (Burt, second interview)
To recapture everyday life, participants continually had to conquer their fears and challenge their skills in terms of using the prosthesis. When unexpected hurdles occurred, their newly gained confidence with the prosthesis was challenged, and once again, the unconscious use of the prosthesis became a conscious act.
Recently we were in the theatre . . . and there was a hell of a lot of people there, and God help me if all those people were not sitting on the stairs next to the railing . . . and I had to walk up those stairs. I was just standing there . . . I could not just tell those people to move . . . so I simply plucked up my courage and walked up the stairs without talking hold of the railing . . . It turned out not to be a problem . . . but occasionally I get a bit, you know, out of sorts. (Daniel, third interview)
In spite of the many positive aspects, the participants had to reconcile themselves to the fact that life with a prosthesis would never be the same as before.
When I waited for the wound to heal, I thought, well, when I get the prosthesis, then I will be able to do everything again . . . but it is just not true, because you are still handicapped . . . So even if you get the aid, and it works out well, it is still a downer. (Finn, third interview)
Discussion
By exploring participants’ lived experiences, the findings of the present study highlight the existential nature of becoming a prosthetic user. The main finding is that the participants were in a state of in-between existence. They felt disconnected from their usual lives and not yet integrated in a new and different life with dependency of prosthesis or appliances. In this in-between existence, the participants were oscillating between experiences of victory and defeat. They hoped to be able to return to their former, normal life; however, they were also vulnerable. To become a prosthetic user required a high degree of stamina and resilience particularly if prolonged healing of wounds or several adaptionprocesses of the prosthesis delayed the training.
Congruent with previous studies (Jefferies, 2015; Liu et al., 2010; Murray, 2009; Murray & Forshaw, 2013), the present study found that beginning to use a prosthesis limb was of deep personal significance and constituted a turning point for participants. Being in an upright posture meant more than equality in interpersonal relations. Being upright gave a sense of normality and made participants’ hope of walking again a real possibility. With reference to Strauss’s philosophy, Abrams (2014) and Rusczek (2014) argued that the upright posture is what characterizes the human species. It is linked to being autonomous connoting independence, mobility, and physical strength. Other studies exploring persons’ experiences of living with a prosthesis point out that prosthesis use provides autonomy, independence, and freedom (Dunne, Coffey, Gallagher, Desmond, & Ryall, 2015; Hafner, Morgan, Abrahamson, & Amtmann, 2015; Murray & Forshaw, 2013). Exploring how walking is understood among healthy people Darker, Larkin, and French (2007) found that walking is obviously a primary form of transport for human beings; however, walking was also constituted as “an experience which takes one out of the world, and into an inner realm” (p. 2178). This indicates that walking refers to a more profound existential dimension as also demonstrated in the present study.
Our main finding of the in-between existence contributes to increased understanding of the initial critical stage among prosthetic users as previously reported (Murray, 2004; Murray & Forshaw, 2013; Ostler et al., 2014). Murray and Forshaw (2013) found that the use of prosthesis use was an emotionally ambivalent experience. The users appreciate the benefits of the prosthesis while experiencing a profound loss. As demonstrated in the present study, the process of becoming a prosthetic user involves existential and conflicting experiences of being betwixt and between the former life and a new life. The state of being betwixt and between is addressed within an anthropological perspective (Turner, 1987). Turner (1987) related the position to cultural changes such as social position and age. He builds on Van Gennep who proposed a tripartite structure of rites of passage explaining how individuals pass through different phases of transition. First, a pre-liminal phase of separation from the old position; second, a liminal phase referring to mid-transition; and finally, a post-liminal phase in which individuals become assimilated and socialized into the new position (Turner, 1987). Turner (1987) pointed out that the liminal state represents an in-between and vulnerable position in which the individual is disengaged from one role, and has not yet engaged in a new role. Turner (1987) characterized the liminal phase as a no-place in which individuals are in limbo. Although becoming a prosthetic user does not necessarily imply that all patients pass through Turner’s three phases, the present study highlights that the liminal phase in particular seems integral to the process of becoming a prosthetic user. More importantly, the findings highlight the critical stage related to the incorporation of new skills and roles as well as identity changes. This critical stage is characterized by uncertainty and the experience of being in a void. The present findings demonstrate that potential prosthetic users are particularly vulnerable in the liminal phase especially if several adaptions occur and they have to do without the prosthesis for a period of time. In these situations, patients might lose their belief in the prosthesis as a future appliance, and the wheelchair becomes a tempting alternative. In this context, the findings contribute to a potential explanation of the underuse and non-use of artificial limbs (Murray, 2009; Schaffalitzky et al., 2011).
Furthermore, the present study highlights that for patients to benefit from prosthetic use requires resilience to overcome hurdles and challenges especially during the in-between transitional process. Although resilience is seen as an important concept in the transitional process of learning to cope and adapt to life in chronic illness (Aburn, Gott, & Hoare, 2016; Kralik, van Loon, & Visentin, 2006; Quale & Schanke, 2010), resilience is given less attention in research addressing the concerns experienced by persons who have undergone a leg amputation. A number of studies have been carried out to understand how patients adapt to the new life situation. Focus has been on coping strategies (Couture, Desrosiers, & Caron, 2012; Oaksford, Frude, & Cuddihy, 2005) and patient’s psychological reaction to the artificial limb (Donovan-Hall, Yardley, & Watts, 2002; Grobler, 2008; Senra et al., 2012). These studies report dominant themes such as low self-esteem, changes in self, and struggles to accept a new identity as disabled. These aspects all point to the complexity of the transitional process among prosthetic users.
One study, however, reports resilience as the main finding (Livingstone, Mortel, & Taylor, 2011). This particular study, however, refers to patients who have undergone a diabetes-related foot or leg amputation rather than prosthetic users in general. The authors found that despite the participants’ sense of grief and loss post-operatively, participants revealed remarkable ability to endure and remain sufficiently resilient to perpetuate hope (Livingstone et al., 2011). Similarly, the present findings show that resilience is an important factor in the process of becoming a prosthetic user. The findings point out that participants’ resilience was under pressure if they constantly experienced challenges. Examining the resilience of patients in physical rehabilitation settings, Quale and Schanke (2010) found that resilience is the most common response to a severe physical injury and point to a need for identifying the strengths of an individual when faced with adversity rather than his or her weaknesses. The findings of the present study support this suggestion and point to a need to direct attention beyond mere physical and medical aspects. The findings stress the importance of addressing patients’ experiences of the in-between existence that seems to be inherent in the process of becoming a prosthetic user. This implicates a need for health care professionals to meet these patients from the perspective of lifeword-led care (Galvin & Todres, 2013; Todres, Galvin, & Dahlberg, 2007). This perspective rests on a phenomenological framework to caring that acknowledges the complexities of the individual patient’s lifeworld and emphasizes the importance of being sensitive to existential issues concerning the patient’s world (Dahlberg, Todres, & Galvin, 2009; Galvin & Todres, 2013). Embedded in this approach is an existential view of well-being that focuses on the experience of well-being as an inner resource important to patients facing health-related challenges (Dahlberg et al., 2009; Galvin & Todres, 2013). This resource-oriented approach to care is particularly relevant to support patients in the initial critical phase in which they have lost their former life and need to re-conquer life as a prosthetic user.
Study Limitation
The present study is limited by the fact that all participants are from a country in which they can be referred to prosthetic training regardless of income. This fact may have resulted in experiences potentially different from experiences of patients from other cultural backgrounds. The number of participants corresponds with the notion that within a phenomenological framework, sampling is concerned with gathering depth and richness of the experience rather than demographic variation and size (Giorgi & Giorgi, 2003; Norlyk & Harder, 2010). However, the fact that most of the participants had full walking ability prior to the amputation may have influenced the findings. Consequently, persons with long-term walking impairment prior to an amputation may experience the process differently.
Conclusion
The study contributes to existing knowledge by providing insights into the existential nature of patients’ experiences of becoming a prosthetic user following a leg amputation and adds to increased understanding of the initial critical stage of becoming a prosthetic user. After the amputation, the participants felt disconnected from their usual lives. They had not yet adapted to a new life in which their quality of life depended on their ability to master using a prosthesis. As found in the present study, the in-between existence was inherent in the process of becoming a prosthetic user. This in-between existence takes its toll on patients’ recovering process.
In summary, the present phenomenological study highlights that for patients, a prosthesis is not merely a technological fix. To benefit from prosthetic use requires resilience to overcome challenges during the in-between transitional process.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.