
Abstract
Patients suffering from chronic pain such as fibromyalgia (FM) not only experience change in their physical bodies but also in their embodiment. There are two forms of disturbed body awareness (BA), namely, “disembodiment” and “hyper-embodiment.” This study describes how patients with FM experience their body and whether there is a difference in BA with or without alexithymia. Based on two self-report questionnaires (Toronto Alexithymia Scale [TAS]-20 and Hospital Anxiety and Depression Scale [HADS]), a purposeful sample of FM patients with and without alexithymia was included. Two focus groups were conducted with nine alexithymic and six nonalexithymic FM patients and were analyzed by a Interpretative Phenomenological Analysis. Body experience appeared in two themes: “the lived body as hyper present” and “alienation from the lived body.” A third theme emerged as “the lived body in interaction with others” and indicates the importance of the interpersonal aspect of BA. We found no differences regarding BA between the alexithymic and nonalexithymic patients. These results suggest that BA in FM patients cannot exclusively be classified under the constructs of hyper- or disembodiment. The authors suggest to consider embodiment in FM, subjected to intra- as well as interindividual influences, as a dimensional construct whereby the equilibrium tends to hyper-embodiment. Still, a temporary shift of this equilibrium from hyper- to disembodiment due to certain emotional state or stress is possible. As alexithymia had no influence on the description of BA, it seems that FM patients primarily fail to express their BA without in fact being disembodied.
Introduction
The prevalence of medically unexplained symptoms (MUS) is high, estimated at 15% to 30% of all primary care consultations (Kirmayer et al., 2004; Steinbrecheret al., 2011). The most common unexplained symptoms in medical and paramedical practice are musculoskeletal pain, abdominal pain or gastrointestinal symptoms, ear, nose, and throat symptoms, dizziness and fatigue (Kirmayer et al., 2004). Together with bodily symptoms, patients with MUS often show a lack of self-confidence and trust in their body (Gyllensten et al., 2010). Despite high medical consumption behavior and corresponding attention, MUS patients do not often recover (Smith et al., 2005). This can be due to the health care system where there is a strong tendency to conceptualize the body as an objective, pure physical body and to interpret symptoms as an underlying biological dysfunction (Bullington, 2009). Yet, for a therapist, it seems to be important to not merely pay attention to the physical or objective body of the patient but also to the subjective or experienced body (Bullington, 2009; Wilde, 2003).
According to the phenomenology of Merleau-Ponty, the body is simultaneously objective and subjective. The body as an object is the body we have, the pure physical body. The body as a subject is the body we are, our body as interpreter (Bullington, 2009; Wilde, 2003). This makes a phenomenological approach fundamental in understanding MUS (Ter Meulen & Van Woerkom, 2009). The concept used by Merleau-Ponty to describe this human experience of having and being a body at the same time, is called “embodiment.” Embodiment conceptualizes the body as a dynamic, organic place of meaningful experience rather than a physical object distinct from the self or the mind (Mehling et al., 2011).
Fibromyalgia (FM) is part of a broad category of “functional somatic symptoms” (FSS) or MUS (Kanaan, Lepine, & Wessely, 2007; Sarzi-Puttini et al., 2012). In the former diagnostic criteria, FM was characterized—in addition to the sensitivity on at least 11 of 18 tender points—by chronic widespread musculoskeletal pain. Recently, the criteria have been adapted with less emphasis on tender points (Wolfe, 2010). Patients with FM also report symptoms of fatigue, sleep disorders, stiffness and cognitive dysfunctions (Sarzi-Puttini et al., 2012; Van Houdenhove & Luyten, 2008). Patients suffering chronic pain such as FM not only experience changes in their physical body but also in their embodiment (Wilde, 2003). In general psychiatry, there are two forms of disturbed body awareness described in relation to (chronic) pain, namely “disembodiment” and “hyper-embodiment.” Disembodiment refers to an individual who is not connected with his or her body. In case of hyper-embodiment, the person is totally immersed in pain (Wilde, 2003). In this state of hyper-embodiment, psychological experiences are experienced as “too real.” Such concrete thinking makes psychological pain being felt as physical pain (Luyten & Fonagy, 2011). However, in a state of hyper-embodiment, the body can also be experienced as very pleasant, comfortable, and as a source of pleasure (Zeiler, 2010). In literature, hyper- and disembodiment are already described in the context of respectively, melancholic depression and schizophrenia (Fuchs & Schlimme, 2009). Table 1 shows the characteristics of both concepts according to Fuchs and Schlimme (2009). In addition, chronic pain not only has a negative influence on the perception of the self but also on the experiential world in which the individual lives (Afrell et al., 2007; Bullington, 2009).
Characteristics of Hyper- and Disembodiment.
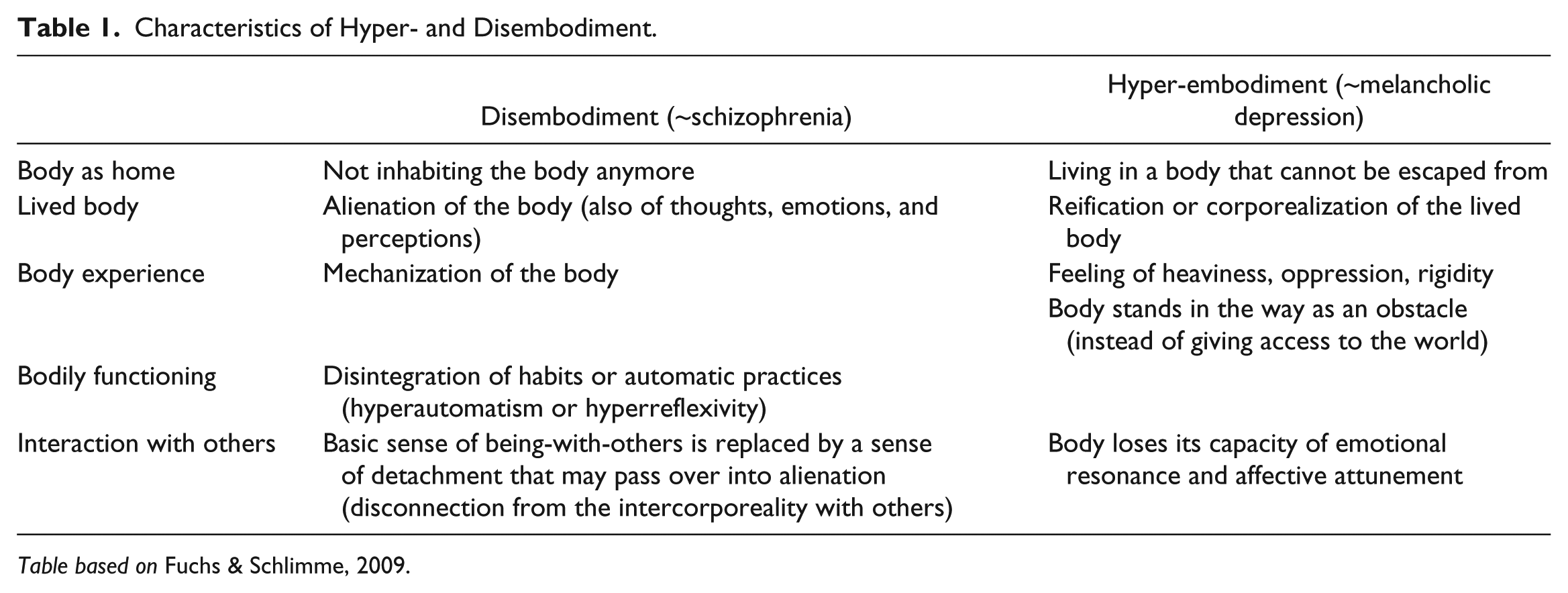
Table based on Fuchs & Schlimme, 2009.
Alexithymia is a personality trait that is characterized by difficulties in recognizing, differentiating, and verbalizing emotional states, by an externally oriented cognitive style and poor fantasy. Literally, alexithymia means “no words for feelings.” Related to these central features, the alexithymic individual is thought to be characterized by a disembodied state of being in the world, unable to contact with his body and the bodily or emotional state he is in, which in turn could be related to poor mentalization capacity (Maclaren, 2006; Spaans et al., 2009; Vanheuleet al., 2011). Alexithymia is considered as a continuous or dimensional trait, which is also found in general population, and is studied in relation to MUS. Important to note is that alexithymia is not considered a disorder itself, nor is it typical for a specific disorder (Lumley et al., 2007). Alexithymia is rather seen as a personality trait that is associated with a higher vulnerability to mental disorders, mainly depression and anxiety (Leweke et al., 2012; Rief & Broadbent, 2007). The latter are two common comorbidities in MUS (Castelli et al., 2012; Henningsen et al., 2003; Sayar et al., 2004; Steinweg et al., 2011).
FM has not yet been described in terms of hyper- or disembodiment. Taking into account the characteristics of hyper- and disembodiment (as described in Table 1), a number of studies have explored the “lived experience” in FM patients (Hellström et al., 1999; McMahon et al., 2012; Paulson et al., 2002; Råheim et al.,1999, 2002), which usually describes both concepts. Characteristics that endorse hyper-embodiment are the lived body that becomes disrupted, apprehended as a physical entity and experienced as hyper present (Söderberg et al., 1999, 2002); the body is described as an obstacle, a barrier that prevents access to the world (idem); completely absorbed by the pain, the body is pain (Råheim & Håland, 2006). Related to disembodiment, the following characteristics are present: the body is experienced at a distance and the body as an alien presence impossible to control (idem).
The primary purpose of the study is to describe how FM patients experience their body. Secondly, possible differences between body awareness in FM patients with and without alexithymia are explored. The objective is to understand the meaningful experience of the body in FM patients and not to search for a causal relationship.
Method
A phenomenological-hermeneutic approach, namely, the Interpretative Phenomenological Analysis or IPA was used for this study as phenomenology emphasizes the immediacy of experience and not the measurability of reality as such (Howitt, 2013). The primary concern of IPA is with how individuals experience phenomena and the psychological interpretations of these experiences. This study was approved by the ethics committee of the Hospital Zuid Oost-Limburg Genk, in collaboration with the ethics committee of the University of Hasselt.
Measurements Sampling Strategy
The 20-item Toronto Alexithymia Scale (TAS-20) is a self-report scale that contains 20 items, divided into three subscales: (a) difficulties in identifying feelings (DIF), (b) difficulties in describing feelings (DDF), and (c) externally oriented thinking (EOT). The TAS-20 has been translated into 18 languages. The Dutch version also shows strong psychometric properties (Kooiman et al., 2002; Tayloret al., 2003). Cutoff points were used to label patients as nonalexithymic (sum score ≤ 51) and alexithymic (sum score ≥ 61).
Levels of anxiety and depression were measured with the Hospital Anxiety and Depression Scale (HADS). This questionnaire contains two subscales, a seven-item depression scale (HADS-D) and a seven-item anxiety scale (HADS-A). For both subscales, scores ≥8 indicate a possible depression or anxiety disorder (Snaith & Zigmond, 1994). The HADS is seen as a valid and reliable tool in assessing the symptom severity of anxiety disorders and depression in a healthy, somatic, psychiatric, and primary care patient population (Bjelland et al., 2002; Herrmann, 1997). The Dutch version also shows good psychometric properties.
Population
The population was selected with a purposeful sampling strategy. This sampling strategy was directed toward FM patients with both high and low scores for alexithymia. Other variables, such as sociodemographic data and the number of years since diagnosis, were allowed to differ. Figure 1 shows the recruitment process. The FM patients were recruited in “Ziekenhuis Oost-Limburg” (ZOL) in Belgium (Genk) and in 10 different physical therapist practices. A total of 75 self-report questionnaires (TAS-20 and HADS) were distributed, which the patients had to return to the researchers. The response rate was 40%. Based on this, patients were selected with a score of ≥61 on the TAS-20 (n = 11). However, the patients who scored low—that is, a score of ≤51—on the TAS-20 (n = 7)—were also selected. The selected patients were contacted by phone to ask for their willingness to participate in a focus group. Nine alexithymic and five nonalexithymic patients gave permission. Finally, four patients with a score of ≤53 on the TAS-20 were contacted and agreed to participate. These four patients were classified in the nonalexithymic group. In this last group, three participants did not show up.

Flowchart recruitment process.
All participants were women diagnosed with FM (according to the American College of Rheumatology [ACR] criteria). The mean age was 43 years in the nonalexithymic group and 46 years in the alexithymic group. The number of years since diagnosis ranged from 1 to 11 years (mean = 8.5 years) in the nonalexithymic group and from 2 to 20 years (mean = 5.8 years) in the alexithymic group. The results from the two questionnaires are shown in Table 2. The average anxiety and depression scores for the alexithymic patients were situated above the cutoff score (i.e., 8). The average HADS-score of 12.7 for anxiety and 13 for depression indicate a moderate depressive disorder and a moderate anxiety disorder (Snaith & Zigmond, 1994; Spinhoven et al., 1997). There is a moderate anxiety disorder present in the nonalexithymic group but no depressive disorders. In another study in which the HADS is conducted in a sample of 301 FM patients, the mean score on the anxiety scale was 12.69 and 10.12 on the depression scale (Vallejo et al., 2012).
Results Questionnaires (TAS-20 and HADS).

Note. TAS = Toronto Alexithymia Scale; HADS = Hospital Anxiety and Depression Scale; DIF = difficulty identifying feelings; DDF = difficulty describing feelings; EOT = externally oriented thinking; HADS-A = HADS-anxiety; HADS-D = HADS-depression.
Data Collection
Focus groups were used as they are well suited for producing broad information on patients’ perceptions, feelings, thoughts, and experiences about the selected topics. The power of the focus group is situated in the interaction between respondents and in identifying their feelings and motives. As the interview takes place in a group setting, the data are strongly dependent on the interaction between the participants (Howitt, 2013). Both focus groups were guided by the same experienced moderator who used a semi-structured interview (see appendix). Each focus group had an average duration of 60 minutes and was audiotaped and transcribed verbatim. All participants gave written informed consent and were assured of anonymity and confidentiality.
Data Analysis
The process of data analysis involved a typical pattern of open coding, axial coding, and identifying themes and subthemes (see Appendix Table A1). First, the interview transcripts were read several times to become familiar with the data. During the open encoding, texts were broken down into discrete parts, which form a meaningful whole and were labeled. Axial encoding involves connecting these open codes and creating a concept (i.e. a description of related codes). Finally, the concepts were grouped in themes and subthemes (Howitt, 2013). Results were continuously compared with literature and adjusted during analysis. Two independent researchers analyzed data and discussed on themes and subthemes. In case of different interpretation, a third experienced clinician was consulted (triangulation). Theoretical saturation was not reached.
Results
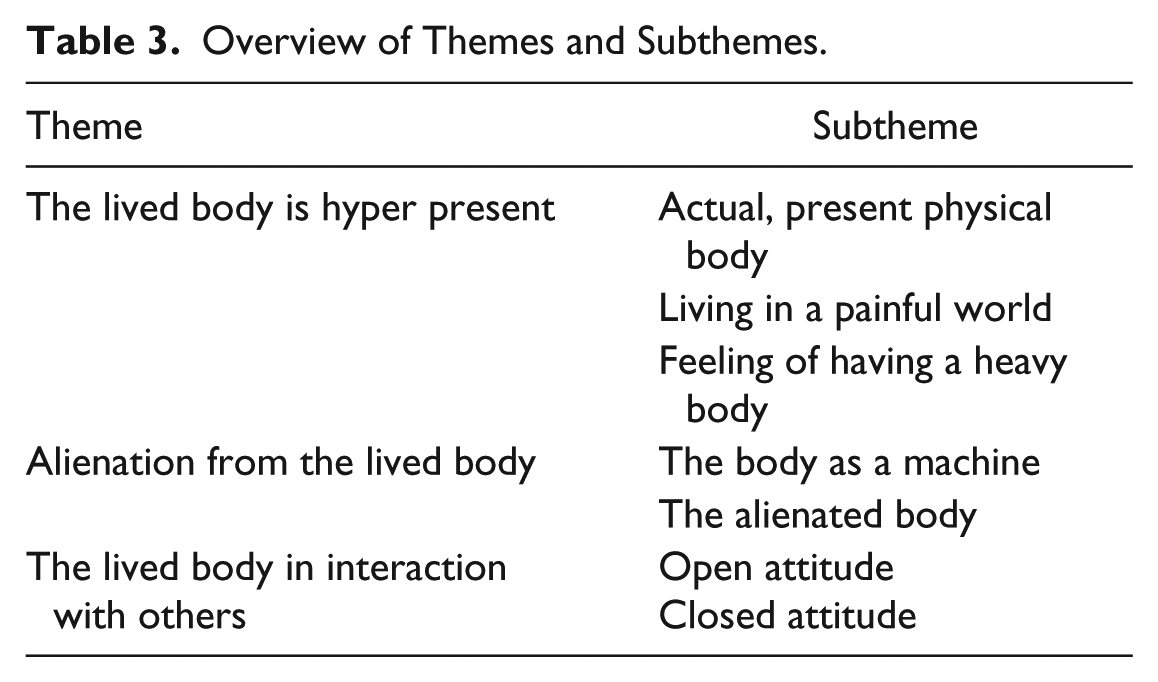
Descriptions on how the included FM patients experience their body can be classified into three themes: the lived body is hyper present, alienation of the lived body, and the lived body in interaction with others. These themes are presented below, along with corresponding subthemes (see Table 3 for an overview).
Overview of Themes and Subthemes.
Theme 1: The Lived Body Is Hyper Present
The theme, “the lived body is hyper present” was constructed from the following subthemes: (a) an actual, present physical body; (b) living in a painful world; and (c) feeling of having a heavy body.
An actual, present physical body indicates a body that becomes apprehended as a biological entity. The entire body, from the tip of the finger to little toe, appears on the foreground in the subjective experience of the patient.
Any piece of my trunk hurts. It is like an inflammation, as if all my nerves are exposed.
Before diagnosis or onset of symptoms, the body was present without being aware of it. Participants described this as an “obvious and fluent body,” which can be defined as an invisible embodied body or a body at the background of attention.
Living in a painful world indicates the impact of chronic pain and associated fatigue. Activities of daily life, such as cooking, ironing and cleaning, can no longer be performed effortlessly. Climbing stairs, for example, becomes the focus of the attention.
In going up or down the stairs at home, now I should pull myself up to the railing, step by step.
The feeling of having a heavy body means that the body is experienced as a weight that has to be dragged. The participants described this as if their body always remains a few steps behind, as if the body cannot follow the mind.
Before I had no idea of my body. Although it was there, I just got up, did all I had to do throughout the day. And now I get up and I need to drag myself out of that bed and drag myself day after day.
Theme 2: Alienation of the Lived Body
The feeling of having a heavy body is described by another participant as follows: I feel like I’m riding with a Ferrari to a mountaintop: a lot of accelerating, but not moving forward. It’s as if you’re driving with the brakes on.
This mechanical expression is in line with the theme “alienation from the lived body.” Here, we can distinguish two subthemes: (a) the body as a machine and (b) the alienated body.
The body as a machine refers to mechanical descriptions of the body. The body is seen as a “faltering machine” or a “car that is used up.” Something does not work properly anymore and should be restored by the therapist.
There is something blocked in my body and because of this I have more pain. This should be mobilized or loosened.
The alienated body refers to a body that is experienced as “not mine.” The body that I am is different than it used to be before the onset of symptoms.
That’s another body, that’s no longer my body, that’s no longer me.
Theme 3: The Lived Body in Interaction With Others
The third theme, “the lived body in interaction with others” refers to the importance of interindividual aspect of body awareness. Although both themes, “the lived body is hyper present” and “alienation of the lived body,” concern the individual experience of the body, these data suggest a remarkable influence of the interactions with significant others. This is surprising as in literature more focus is placed on intraindividual aspects such as cognition (e.g., Gard, 2005) and proprio- or interoceptive processing (e.g., Cameron, 2001; Craig, 2003; Tsakiris, 2010). However, the participants report that the physical complaint in itself is not the problem but its consequencesfor their daily interactions with others are. The feeling of being judged and having to defend themselves because their illness is “medically unexplainable” seems to influence their bodily experience to large extent. The present data suggest that people with FM are constantly looking for an optimal coping between how they want to express themselves and how they think they should behave.
On the one hand, they want to adopt an open attitude in interaction with others. They try to be single-hearted and brave while indicating what they are able to and where they feel limited. Although this is often not the case, they want to be understood, seen, and heard. Therefore, they consider it essential to be able to express how they experience their daily life and not to hide their feelings of tiredness as well as joy from others. This expressing and not hiding is also and even foremost experienced on a bodily level where “standing up” literally is about feeling strong legs to stand on and having a firm look while interacting with people.
I have learned to express myself to other people. This is who I am, these are my limits, this is what I can do, I can have a meeting in the morning, but not the same day also in the evening, I can function like this and I keep on doing it this way. Before I always pretended—although feeling small—but now I just look and say it and it’s the other one who should adapt. Why should it always be me who must fit in? Since I’ve been power training, my stance has changed dramatically and it is as if my legs are rooted in plain ground now . . . once I had an argument with a colleague and I really felt that I was standing strong!
On the other hand, they express that others should not always notice (e.g., “everyone should see that I am going well”) or understand them (e.g., “there is nothing to see, people can’t understand”). This is what makes them actually prefer not to talk about their situation anymore, indicating a closed attitude. In addition, a private space in which one feels safe seems to be important. This can be obtained by retreating in a personal “cocoon” or by isolating themselves completely from the environment.
I feel most secure when I would be alone on an island. That seems a safe situation. Occasionally I need to sit down in my couch, under a blanket, wearing my pajamas. Then, others may not sit on my couch. That is my place. Actually I live in my own territory, my own space. I accept who I want to, when I want to. I’m tired of constantly having to explain myself, it makes me so tired, I feel so exhausted in my body. My husband knows when he has to leave me alone for a while . . . the only thing I can bear at that moment is my body around me.
The behavior or responsiveness of the environment also seems to be an important factor affecting the physical symptoms of the patient. Little understanding, not being seen or heard by significant others results in more stress and contributes to an increase of the physical complaints.
People don’t understand that you want to. They say you’re lazy or trying to attract some attention. Thereby I feel more stressed, and I am doing less well. When my husband or kids are at home, I’m trying real hard not to sigh or moan, I even walk taller as when my father told me when I was young to be a big girl.
Alexithymia
The themes and subthemes are applicable to both the alexithymic and nonalexithymic group. The personality trait alexithymia had no influence on how these FM patients experience their body. Based on the qualitative analysis, some differences can nevertheless be noticed: verbal reactions indicating a lack of mentalization, experiencing more misunderstanding from the environment and preferring exercise therapy to a touch-based therapy are more present in the alexithymic group in comparison with the nonalexithymic group. These differences are described and illustrated below.
A first difference with the nonalexithymic group is the limited ability to express the inner world of feelings, emotions, and mainly focussing on physical sensations. Verbal reactions indicating a lack of body mentalizationare no words, empty words, body absolutism, and emphasis on physical labels (Table 4).
Verbal Reactions Indicating a Lack of Body Mentalization (According to Spaans, Veselka, Luyten, & Bühring, 2009).

They also indicate the need to be heard, seen, and understood by the environment. Just because they fail to express their inner world and to indicate their limits, they experience more misunderstanding from the environment in comparison with the nonalexithymic group.
I can’t say what I feel, I can only say that I have pain at the moment. So for someone else in your environment, it’s even more difficult. They can’t estimate that at all, if I can’t even describe how I feel.
Whereas the nonalexithymic FM patients prefer the combination of hands-on therapy and psychotherapy, the FM patients with alexithymic characteristics prefer exercise therapyto a therapy in which touch is central. According to them, the advice and guidance of the psychotherapist offers little progress (e.g., “After all, we have to do it all by ourselves”), whereas movement-based therapy seems to have a more suitable treatment objective. They focus a lot on stabilizing their complaints, on recovery, and improvement of their quality of life without being dependent on others, in this case the therapist.
My physical therapist teaches me things I can do by myself. This is important, knowing I am not dependent on someone else.
Discussion
Based on the qualitative data analysis, these FM patients show characteristics of hyper-embodiment as well as disembodiment. Patients’ experiences suggested a lived body, experienced as a heavy body and living in a painful world, which was thematically clustered as the lived body is hyper present. However, there is an alienation of the lived body, because the body is described as a machine and as strange, not belonging to the individual. This specific phenomenological experience of not being one’s own body could be in line with the paradoxical experience of being in pain while not feeling it as described by Valenzuela-Moguillansky (2013) in patients with FM. The modification of pain which these authors label as paradoxical, could be referring to a process of coping by alienating from one’s body as in disembodiment. A kind of experiential distance or filter is created between the individual and the body, which results in a deafened effect on the pain. These occurred especially when patients were suddenly or intensely confronted with stress as in anxiety or panic and could—on a bodily level—be in line with the mechanism of derealization in traumatized people. However, hyper-embodiment seemed to be more present during normal daily life when patients have to deal with less unexpected disturbing arousal. Here they described to be absorbed by their body, experiencing it as a burden or heavy weight that has to be dragged.
This possibility of the lived body moving back and forth is why it is more appropriate to consider embodiment as a dimensional construct with hyper- and disembodiment at each end of a spectrum (Figure 2). Although, in both conditions, the body is present in the forefront of the subjective experience, hyper-embodiment is about an oppressing and solid body object, where the patient is trapped in, whereas in disembodiment, the body is an alienated apparatus that cannot be inhabited anymore (Fuchs & Schlimme, 2009). It is important to emphasize that hyper- and disembodiment also have a normal range and should not be interpreted as pathological concepts as such. Typical example here is the fight/flight state in which an individual is normally and functionally detached from his body awareness to cope with a possible situation, whereas a sensual massage invites to a more intensive aware experience of the body. So to escape or enjoy, a normal fluctuation or shift in dis- or hyper-embodied states is needed. The problem, however, with a more dysfunctional appearance of embodiment appears when the normal flow on the hyper- and disembodiment spectrum got stuck to some level. In that case, the lived body cannot adept properly to any given situation in daily life.
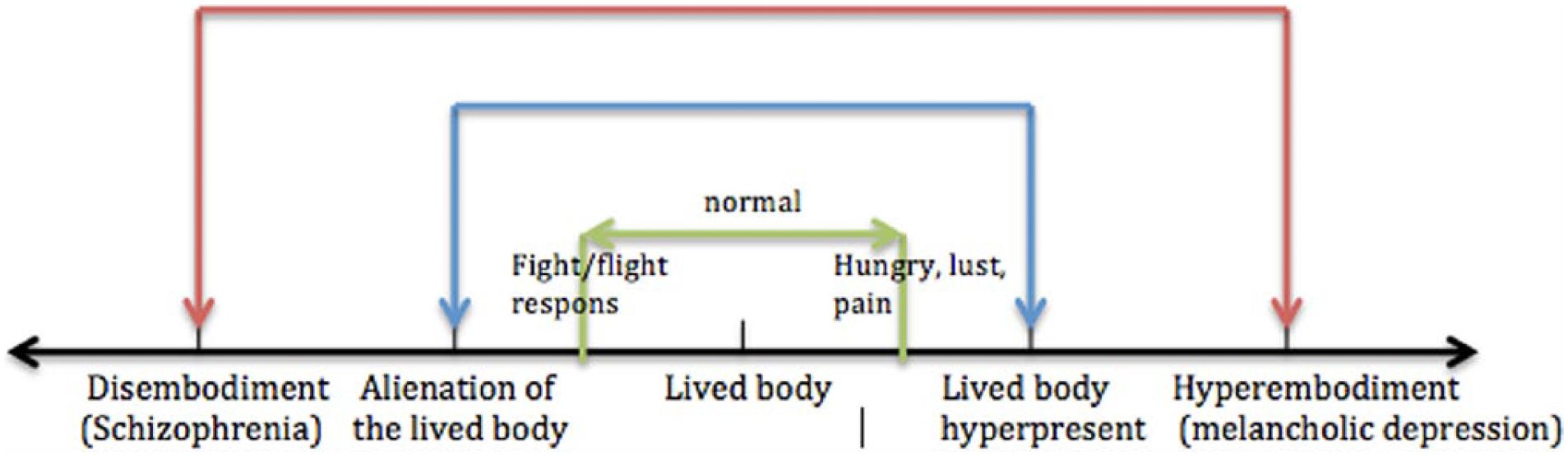
Embodiment as a dimensional construct.
Moreover, in general health, the lived body is implicitly present in every action (Söderberg et al., 2002) and so the body “dis-appears” from the attention (Zeiler, 2010). Only in specific situations—such as in case of hunger, thirst, desire, fatigue, or pain—the body becomes present as a biological entity (Denys & Meynen, 2011; Seligman, 2010; Wilde, 2003). Otherwise, attention is not always directed toward the body and, as stated—for example, in acute danger—attention is more focused on the environment instead of the body. So an explanation for both the hyper- and disembodied experiences of the FM patients in this study could be the ability to make a temporarily shift or switch from hyper- to disembodiment due to certain emotional state or stress. Still, the present data suggest that the equilibrium tends to hyper-embodiment in FM.
The third theme—the lived body in interaction with others—is a remarkable interindividual aspect of body awareness. Merleau-Ponty defines this as intercorporeality, indicating that the experience to be embodied is always mediated by our continuous bodily interaction with others (Stanghellini, 2009). Being in the world and interacting with others occurs first and foremost on a bodily level as we contact as “body to body,” mostly on an unconscious level in an embodied space. That is why Merleau-Ponty states that intercorporeality or embodiment is in particular prereflective and can be seen as a kind of unconscious attunement (Stanghellini, 2009). This prereflective attunement and body-mediated intercorporeality seem to find—at least to some extent—their neurobiological substrate in mirror neurons as is increasingly demonstrated in literature. Not only higher order decision making, language, or cognition in general are rooted in the mirror neuron system of a person but also embodiment itself is mirror neuron–based as stated by Gallese and Ebisch (2013): “In other words, by exploiting the same neural circuits as those recruited for first-person bodily experiences, a direct intersubjective link is established between self and other allowing an experiential understanding of others bodily feelings” (p. 279). Focused on social cognition, this embodied understanding also appears in what is called embodied simulation where people are thought to reuse their own mental states represented with a bodily format in functionally attributing them to others (Gallese & Sinigaglia, 2011; Kyselo, 2014; Winters, 2008). These key notions on the embodied basis of intersubjective attunement or evaluation are reflected in the third theme, where on one hand, the participants want to be understood, seen, and heard by their environment (i.e., open attitude). On the other hand, they also state that the environment not often understands their preference not to speak about themselves (i.e., closed attitude). In general, they are confronted with misunderstanding from others. A number of studies attribute this misunderstanding to the invisibility of the symptoms, a general lack of knowledge about FM and the perception that the illness is “psychological” and therefore not legitimate (McMahon et al., 2012). This theme reflects the “intercorporeality” dimension of the lived body, where people not only try to cope on a bodily level with their surrounding by, for example, standing tall and having a firm gaze. But also the consequences of this prereflective and bodily attunement appear in this third theme as in “feeling tired of being judged.” Interesting and striking at the same time is that both the open and closed attitude appear in an embodied way in their narrative and behavior, for example, when a participant tells that the couch where she is sitting on, wrapped in her blanket, is her space and territory where her body cannot bear anyone close.
Alexithymia
Based on literature, the alexithymic individual was thought to be characterized by a disembodied state of being in the world. Many theorists have explained alexithymia as a disconnection between the objective mind and the emotional experienced body, in short, a disconnection between body and mind. An alexithymic individual is thereby characterized by a lack of emotional involvement in the world. Instead, this person is in an objective and instrumental way involved in the world and seems to be disconnected from his or her body (Maclaren, 2006). This was not confirmed by the qualitative data from this study. The way alexithymic FM patients describe how they experience their body is surprisingly similar to these in the nonalexithymic group. Alexithymic patients are primarily failing in expressing their bodily experiences without actually being disembodied could be a possible explanation.
Compared with the nonalexithymic group, some differences could nevertheless be noticed: (a) verbal reactions pointing to a lack of mentalization, (b) more misunderstanding from the environment, and (c) preferring exercise therapy instead of hands-on therapy. Clinical observations and controlled studies have confirmed that psychotherapeutic treatments of alexithymic patients are difficult (Vanheule et al., 2011). Alexithymia seems a negative prognostic indicator for many psychological treatments, particularly those focusing on emotional awareness and a close relationship with the therapist (Lumley et al., 2007; Vanheule et al., 2011). Behavioral treatments are more appropriate because of a more structured, externally oriented and concrete approach (Baranowsky et al., 2009). Also mentalization-based therapy may be suitable for alexithymic patients (Baranowsky et al., 2009; Vanheule et al., 2011). Still, it is important to note that therapists not always have to use verbalization to stimulate the mentalization process. For example, body awareness interventions, emphasizing on being aware of the body without the need to be verbalized, can be an option. In this type of interventions, therapists can choose to use a hands-on or hands-off approach. The efficacy of these treatment methods in FM patients is still under debate (Gard, 2005; Ogrodniczuk et al., 2011).
Conclusion
In the literature, authors distinguish two forms of disturbed body awareness: “disembodiment” and “hyper-embodiment.” These concepts are already described in the context of melancholic depression and schizophrenia. To date, both concepts are not used in the context of FM. This study describes how FM patients experience their body and explores whether these patients can be categorized in dis- or hyper-embodiment).
Characteristics of both concepts were established and classified in two themes: the lived body is hyper present (hyper-embodiment) and alienation from the lived body (disembodiment). As both characteristics were present, we can conclude that FM patients cannot exclusively be classified in hyper- or disembodiment. The phenomenology of the hyper-embodied state seemed to be more present during normal daily life when patients have to deal with less unexpected or disturbing situations. In contrast with this hyperembodiment, the state of disembodiment occurred particularly when patients were suddenly or intensely confronted with stress (for exampleanxiety or panic). So considering embodiment as a dimensional construct with hyper-embodiment and disembodiment on both sides of the spectrum, the equilibrium tends to hyper-embodiment, including the possibility of a temporary, state-dependent shift of this equilibrium from hyper- to disembodiment. Finally, these qualitative data also showed an important interpersonal aspect in body awareness (the lived body in interaction with others), in line with Merleau-Ponty’s concept of intercorporeality as a prereflective and unconscious attunement on a bodily level.
In addition, a difference in body awareness between FM patients with and without alexithymic characteristics was investigated. Based on the literature, it was hypothesized that an alexithymic individual was characterized by a disembodied state. Nevertheless, this study illustrates that the personality trait alexithymia has no influence on how FM patients experience their body.
Alexithymic patients primarily failing in expressing their bodily experiences without actually being disembodied could be a possible explanation. Compared with the nonalexithymic group, some differences characterizing the alexithymic participants can nevertheless be noticed: the presence of verbal reactions pointing to a lack of mentalization, experiencing more misunderstanding from the environment and preferring exercise therapy instead of hands-on therapy.
Strengths and Limitations
Two independent researchers discussed the present findings until agreement (investigator triangulation). Data were discussed in a transdisciplinary way and approached from different theoretical perspectives. A first methodological limitation is the number of participants in the study, causing a lack of theoretical saturation. This implies that certain aspects remain questionable and that the relationship between the different themes is not yet fully elaborated. In addition, it is possible that the presence of individuals with depressive characteristics in both focus groups biased the results because depression has an influence on how the body is experienced (Luyten & Fonagy, 2011). Finally, two respondents with a score ≤53 on the TAS-20 were classified in the nonalexithymic group, whereas the cut-off score is 51.
Implications for Clinicians
Hands-on interventions, aiming at improving body awareness, such as Fascia Therapy Method Danis Bois, Feldenkrais, Rolfing, or Rosen Method Bodywork can be seen as recommendable therapeutic approaches in FM. We suggest that hands-off body awareness interventions are more appropriate in case of alexithymic FM patients. In addition, therapists must be aware of embodiment as a result of both individual and inter-individual processing adding up to the first person experience of a lived body. This is why techniques focusing on expressing how the body is lived and improving body mentalization can be used in alexithymic FM patients because they fail to describe their bodily signals in a clear way, leading to misunderstanding from the environment, which in turn can affect overall body experience. It is important to note that therapists should treat FM patients using a staged or phase-oriented approach, starting with bodywork and gradually working toward verbalization, but always starting from the lived body experience of being in and interacting with the world.
Recommendations for Future Research
More comprehensive research on this topic is needed. Not only exploring in more detail what elements determine a state of hyper- or disembodiment in FM or how they are described and experienced in several different contexts but also researching the factors that could influence or cause a shift between hyper- and disembodiment remain largely unknown.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.