
Abstract
This exploratory study investigated child sleep in a sample of maltreated children living in foster care and examined its associations with placement conditions and history of maltreatment. Participants included 25 foster children and their foster caregiver. Children were on average 60.24 months of age (SD = 18.70). Foster mothers completed questionnaires assessing parenting stress and quality of child sleep while maltreatment/placement history was retrieved from children Child Protection Services (CPS) records. Shorter nocturnal sleep duration and parasomnias were related to placement at a younger age. The non-restorative sleep index was significantly related to time spent in the foster home and parenting stress and marginally related to number of placements and sexual abuse and neglect. Poor sleep was associated with past experience of sexual abuse and neglect and parenting stress. No relationships were found between sleep characteristics and past experiences of physical abuse or type of foster family. These findings provide an opportunity to uncover how foster children experiences are related to sleep disturbances.
Evidence generally supports the notion that children placed in foster care are at heightened risk of maladjustment owing to past experiences of maltreatment (physical or sexual abuse, or neglect) and placement related-risk conditions (Taussig, 2002). However, information about foster children quality of sleep is sparse. Given that foster children have experienced chaotic and inconsistent care prior to placement, they may be particularly frightened at night and not view foster caregivers as sources of regulation of fears (Tininenko, Fisher, Bruce, & Pears, 2010). In particular, there is a need to identify sleep habits of young foster children and determine how experiences of maltreatment and placement conditions might be related to sleep quality and disruptions.
Sleep Disorders in Young Children
Sleep disorders are highly prevalent in children, as shown in epidemiologic studies indicating that up to 50% of children experience a sleep problem (Carter, Hathaway, & Lettieri, 2014). The most prevalent sleep disorders in children are behavioral insomnia and parasomnias. The former is mostly characterized by bedtime resistance, frequent nighttime awakening, and/or an inability to sleep alone, whereas the latter are characterized by awakenings from deep sleep, such as sleepwalking, bruxism, enuresis, sleep terrors, and nightmares (American Academy of Sleep Medicine [AASM], 2014).
Multiple factors related to individual and relational characteristics are associated with child sleep (Touchette, Petit, Tremblay, & Montplaisir, 2009). For instance, sleep disturbances are linked to child internalizing and externalizing disorders (Gregory & Sadeh, 2012) and to greater psychological distress in mothers (Martin, Hiscock, Hardy, Davey, & Wake, 2007). Low quality of mother-child interactions and stressful family life events are associated with poor sleep in non-clinical samples (Bélanger, Bernier, Paquet, Simard, & Carrier, 2013; Sadeh, Raviv, & Gruber, 2000). A low socioeconomic status is also associated with poorer sleep, including sleep-onset difficulties (Petit, Paquet, Touchette, & Montplaisir, 2010). Taken together, these studies suggest that sleep is sensitive to not only child or parent characteristics but also to the exposition of adverse environmental conditions.
Sleep Characteristics of Children in Foster Care
Children placed in foster care face an alarming combination of risk conditions, including experiences of early maltreatment and separations from their primary caregivers, which can result in emotional and behavioral disturbances (Villodas, Litrownik, Newton, & Davis, 2016). Yet, to our knowledge, only one study has specifically assessed sleep of young foster children. In this study, sleeping behavior was assessed using sleep actigraphy and parent-report measures among groups of children (3-7 years of age) living in foster care or community settings (Tininenko et al., 2010). Results showed that foster children have greater difficulty initiating sleep than community children. However, children living in treatment foster care (receiving preventive intervention addressing socio-emotional needs) had a longer sleep duration than those living in regular foster care or in a low-income community. Sleep duration did not differ between children in regular foster care and those of the community. Overall, this study suggests that parental status and placement type relates to child sleep characteristics. However, it did not assess foster children’s living conditions that could be affecting sleep, such as placement conditions and past experiences of maltreatment. Moreover, no information related to parasomnias was reported.
Studies assessing the impact of maltreatment on quality of child sleep are very limited. Whereas one study has found that sexually abused children (mean age 5.9 years) had more sleep problems as reported by parents (e.g., being overtired, sleeping less or more than most children, and having trouble sleeping) than the comparison group (Dubowitz, Black, Harrington, & Verschoore, 1993), another showed that experiences of physical abuse but not sexual abuse were related to poor quality of sleep in children (7-14 years of age) as assessed by actigraphy (Sadeh et al., 1995). Finally, prepubertal abused children were twice as active at night as control and depressed children and had prolonged sleep latency and decreased sleep efficiency (Glod, Teicher, Hartman, & Harakal, 1997). No study has yet confirmed the hypothesis that neglect should impact on child sleep.
The present exploratory study is the first report on multiple indicators of sleep, including sleep difficulties and parasomnias, in a sample of young children placed in foster care after being exposed to parental maltreatment. The investigation of child history of maltreatment is an opportunity to uncover how these life experiences can relate to child sleep. The tested hypothesis was that past experiences of abuse and placement-related risk conditions, including foster caregiver psychological distress, would be related to poor quality of child sleep.
Method
Participants
Twenty-eight foster mothers and children (19 boys) were recruited through Child Protection Services (CPS) in a small urban community in the province of Québec (Canada) to participate in a study evaluating the efficacy of a home-visiting relationship-based intervention program. CPS agencies were asked to refer foster families who (a) were fostering a child between 36 and 84 months of age, (b) had been fostering the child for at least 2 months, and (c) were engaged in long-term foster care or in an eventual adoption. Only children with severe organic developmental problems (e.g., cerebral palsy) were excluded from the study. Identification of families was accomplished through liaison with an employee of the CPS who had legal access to family records. Between the initial contact with foster mothers and the assessment, three children were removed from their foster family. Therefore, the final sample included 25 dyads.
Children were on average 60.24 months of age (SD = 18.70, range: 36 to 84 months of age), and foster mothers were on average 44.16 years of age (SD = 8.63, range: 32 to 57 years). All participants were Caucasian. Thirty-six percent of foster families had an income below Can$40,000, 24% earned between Can$40,000 and Can$75,000, and 40% earned Can$75,000 or more. Mean income in Canada was Can$78,500 at the time of data collection, and the poverty threshold was Can$27,844 (Gouvernement du Québec, Institut de la statistique, 2012). Eighty-four percent of foster families were composed of two parents (84% in the Canadian population), and 60% of foster mothers had completed a postsecondary education level (73.2% of woman in the Canadian population).
Measures and Procedure
CPS employees initially approached eligible families and obtained their consent to transfer personal information to a research assistant. Those who accepted were contacted by a research assistant and received information about the research purposes. Prior to data collection, written consent was obtained from foster and biological mothers who consented to their own and their child participation. The protocol was approved by the Université du Québec à Trois-Rivières’s research ethics committee. Participating families completed initial measures during a 1-hr laboratory visit in which foster mothers filled different questionnaires including child sleep.
Quality of foster child’s sleep
Foster caregivers were asked to complete Your Child Sleep, a questionnaire that was used in a preschool sample of adopted children (Tessier, Larose, Moss, Nadeau, & Tarabulsy, 2005). This questionnaire provided information on total sleep time at night and during the day and on different child sleep characteristics that were rated by foster mothers on a 0 to 3 Likert-type scale (never/rarely, sometimes, most of the time, always). Three theoretically driven indexes of sleep were computed by summing the score (0-3) for each behavior/symptom included in the indexes: (a) the non-restorative sleep index includes difficulties waking-up in the morning, sleepiness after final morning awakening, tiredness during the day, and falling asleep during the day; (b) the poor sleep index includes having difficulty falling asleep, difficulty getting back to sleep following an awakening, and being anxious at night/afraid of darkness; (c) the parasomnia index includes body rocking, sleep bruxism, enuresis, bad dreams/nightmares, night terrors, and irregular breathing during sleep (see International Classification of Sleep Disorders–Third Edition [ICSD-3]; AASM, 2014).
Parenting Stress Index (PSI–Short Form)
Foster mothers completed the 36-item PSI–Short Form, a maternal self-report measure focusing on sources of perceived stress related to the parental role (Abidin, 1995). Items are rated on a 0 to 5 Likert-type scale and are summed to generate three scales: parental distress, parent-child dysfunctional interaction, and difficult child. The PSI shows excellent internal consistency and convergent validity with respect to prenatal stress, other indices of postnatal stress, and the quality of parent-infant interactions (Abidin, 1995). Good internal consistency was found for the three scales in the current study (Cronbach’s alpha between .77 and .89).
History of maltreatment and placement conditions
This information was retrieved from each child CPS record and included reasons for initial placement (i.e., substantiated abuse and/or neglect), age at initial placement, and total number of placements. Age at the time of placement in the current foster family, type of foster home, and characteristics of the foster home (income, marital status, number of children) were obtained from foster mothers who completed a sociodemographic questionnaire. Type of foster home included regular non-kin foster care (placed with unknown adults), kinship foster care (placed with relatives), and foster-to-adopt families (placed to potentially be adopted). Table 1 presents characteristics of placement conditions and history of maltreatment.
Descriptive Statistics for Placement Conditions and History of Maltreatment.
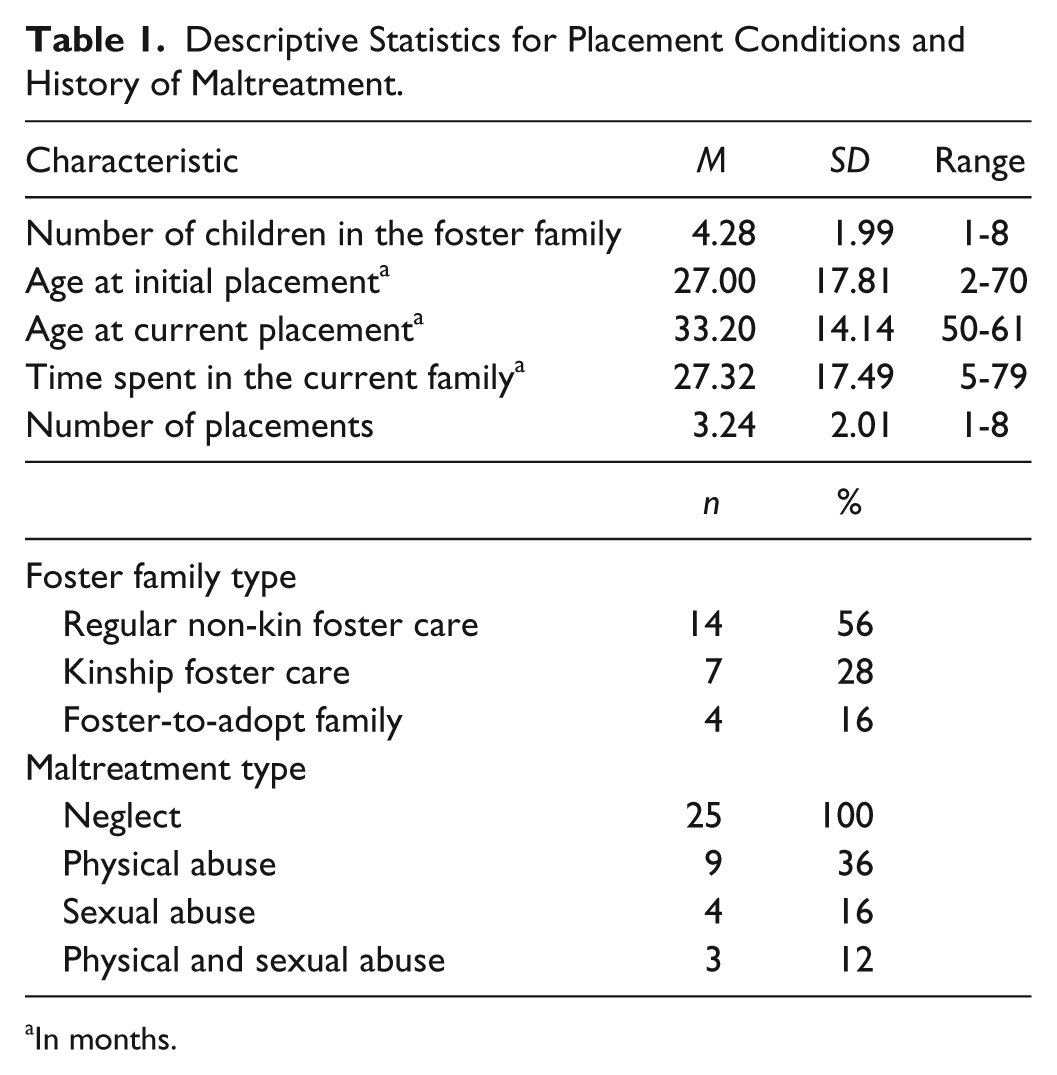
In months.
Statistical Analyses
Data manipulation and analysis was performed using the SPSS (Version 21.0.0.1; SPSS windows). Pearson correlation analyses were undertaken to evaluate associations between child sleep, history of maltreatment/placements, and foster mother parental stress. Given that all children in our sample were exposed to neglect, analyses on maltreatment were only performed on physical and sexual abuse. According to Cohen, Cohen, West, and Aiken (2003), effect sizes, which provide a better interpretation of the results weight are preferred to statistical significance tests and are as follows: r ≥ .1 represents a small effect size; r ≥ .3 represents a medium effect size, and r ≥ .5 represents a large effect size. Marginal results (ps > .05 < .10; see Pritschet, Powell, & Horne, 2016) with medium to large effect sizes were reported.
Results
Sleep Characteristics of Foster Children
Table 2 presents the proportions of sleep conditions (habits and disturbances) in our sample. Proportions of participants having specific sleep conditions occurring sometimes to always vary from 8% to 54%. Mean nocturnal sleep duration was 10.32 hr, and mean total sleep duration per 24 hr, including daytime sleep, was 11.22 hr. Scores on the indexes were normally distributed and suggest that in average, children in our sample did not present high levels of sleep problems.
Descriptive Statistics for the Sample.
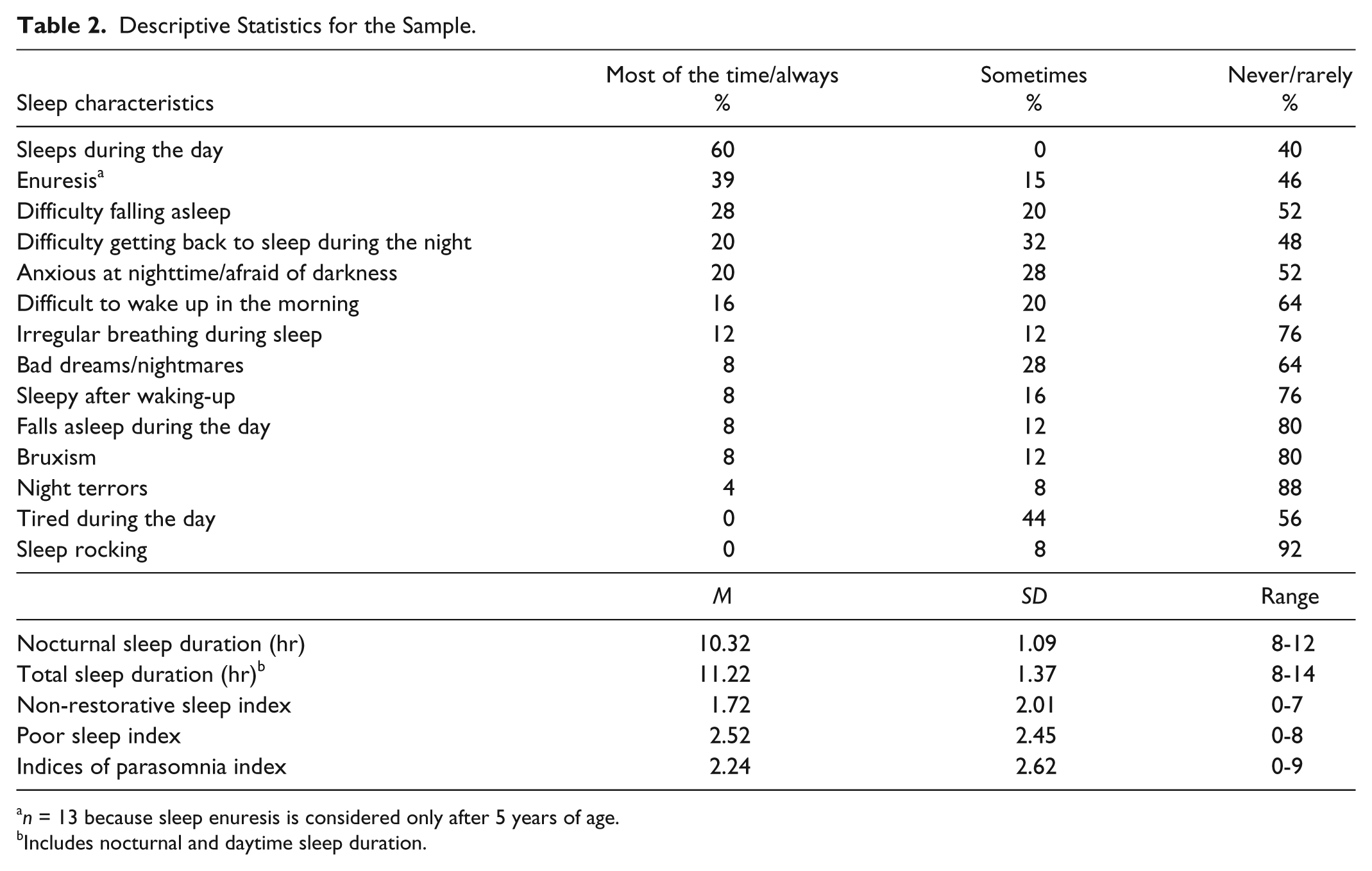
n = 13 because sleep enuresis is considered only after 5 years of age.
Includes nocturnal and daytime sleep duration.
ANOVAs revealed no significant differences in sleep (duration and indexes) as a function of child gender, marital status, or income. Correlations revealed no significant associations between sleep (duration and indexes) and foster mother age, or number of children in the foster family. Child age was significantly related to the parasomnia index, r = .53, p < .01, and marginally related to total sleep duration, r = −.36, p < .10, but unrelated to the other sleep variables. To account for the impact of age on child sleep, subsequent analyses were covaried with age.
Associations Between Sleep Characteristics, History of Maltreatment, and Placement Conditions
Partial correlation controlling for age were conducted between sleep characteristics, history of maltreatment, and placement conditions. Several significant and marginally significant associations (medium to large effect sizes) were found between sleep variables and maltreatment and placement conditions.
Correlation analyses showed that the parasomnia index scores were significantly related to total sleep duration (r = −.45, p < .05) and marginally related to poor sleep index scores (r = .37, p < .10) but were not associated with the non-restorative index scores. The non-restorative and poor sleep indexes were marginally interrelated (r = .36, p < 10) but were not associated with sleep duration.
Shorter nocturnal sleep duration was related to earlier placement and longer stay in the foster family (marginal), r = .44, p < .05 and r = −.41, p < .10, respectively. Sleep duration (nocturnal or over a 24-hr period) was not related to other placement conditions or to history of abuse. Greater non-restorative sleep index scores were significantly related to time spent in the foster family (r = .44, p < .05) and two of the parental stress scales (maternal distress: r = .47, p < .05; difficult child: r = .56, p < .01), and marginally related to number of placements and sexual abuse, r = .41, p < .10. Higher scores on the poor sleep index were associated with past experiences of sexual abuse (r = .50, p < .05) and with greater parenting stress (caregiver distress: r = .39, p < .10; difficult child: r = .47, p < .05; dysfunctional interactions: r = .47, p < .05). Higher parasomnias index scores were related to earlier placement (r = −.42, p < .05) but unrelated to other placement conditions. Foster children sleep (duration and indexes) was not significantly related to past experiences of physical abuse and neglect or to type of foster family.
Past experiences of physical abuse were marginally related to experiences of sexual abuse (r = .35, p < .10) and to children seen as being more difficult (r = .37, p < .10). Past experiences of sexual abuse were also related to greater parenting stress pertaining to child difficulty and dysfunctional interactions, r = −.42, p < .05. Longer stay in the actual foster family was related to earlier initial placement (r = −.54, p < .01), and time spent in the foster home was associated with foster parent distress (r = .55, p < .01).
Discussion
This exploratory study is the first to describe the association between history of maltreatment and caregivers reports of parenting stress and sleep quality and parasomnias of young children placed in foster families. Foster children in our study had a mean total sleep duration of 11.22 hr and a mean nocturnal sleep duration of 10.32 hr, which is more than what was found in another sample of foster children (3-7 years of age; Tininenko et al., 2010) but similar to numbers found in a large normative sample (2.5-8 years of age; Petit et al., 2010). These results could suggest that after being placed in a safe and stable environment, previously neglected children present with adequate sleep duration. To that effect, it was shown in Tininenko et al. (2010) study that children living with foster caregivers who received a preventive intervention addressing child socio-emotional needs had a longer sleep duration than children living in a regular foster family. In our study with children living in a non-treatment foster family, shorter nocturnal sleep duration was related to earlier placement and longer stay in the foster family. It is possible that children exposed at an earlier age to very problematic home environments have more difficulty to recoup sleep duration. Information about placement age was not available in Tininenko et al. (2010) study but earlier placements could possibly account for their sample’s shorter nocturnal sleep duration. These results support the association between an insecure and inconsistent environment and sleep disruption.
Our results showed that greater non-restorative sleep index scores were marginally related to more placements. Children with multiple placements experienced more instability and relationship disruptions, factors that have been associated with anxiety (Taussig, 2002) and sleep disruptions (El-Sheikh, Buckhalt, Mize, & Acebo, 2006). In our study, higher scores on the non-restorative sleep index were significantly related to foster mothers’ distress and children difficult behaviors. Because of its impact on behavioral regulation and control, inadequate amounts of sleep may affect children’s behavioral and social adjustment during the day and vice versa (Touchette et al., 2009). It has been shown that children with disrupted sleep schedules had less positive and more negative adjustment in preschool, even after considering the roles of family stress and parenting practices (Bates, Viken, Alexander, Beyers, & Stockton, 2002). Not only does children’s sleep disruption being related to their adaptation but it is also associated with their parents’ functioning. Mothers of children who had significant sleep disruptions reported more parenting stress and caregiving overload (Meltzer & Mindell, 2007), similar to results found in our study.
Findings of the current study also indicate that foster children showing higher scores on the non-restorative sleep and poor sleep indexes were more likely to have experienced sexual abuse. The latter association is quite impressive considering its large effect size. Observed behaviors related to the poor sleep index can be associated with inappropriate sleep associations in children or to inadequate limit setting by the caregiver. Given that nighttime and darkness may be directly associated with experiences of abuse (Sadeh, 1996), it is not surprising that foster children who were sexually abused show more anxiety and difficult behaviors around bedtime and during the night. Foster mothers of sexually abused children reported having more dysfunctional interactions with them and described them has being more difficult in general, which is consistent with findings of other studies (Taylor & Brook, 1986). Because child abuse and neglect increases risk of developing posttraumatic stress disorder (PTSD) and trauma symptoms in childhood (Milot, Éthier, St-Laurent, & Provost, 2010), it is possible that sexually abused and neglected children in our sample are more likely to experience emotional and behavioral disturbances both during the day and the night because of such vulnerability.
Foster children showing greater scores on the poor sleep index were also more likely to have dysfunctional interactions and to show difficult behaviors, which is consistent with findings from children living with their biological parents (Adam, Snell, & Pendry, 2007; Bélanger et al., 2013). Taken all together, these studies show that sleep is sensitive to family context. Conversely, children’s poor sleep may also impede on the foster mother-child relationship. For these families, fostering a child with difficulties falling asleep or who is demanding because of sleep anxiety constitutes an additional burden.
In our study, the parasomnia index was related to earlier placements, suggesting, for these children, an earlier exposition to pathogen family environments (e.g., domestic violence, neglect, abuse). It is noteworthy that these children were exposed at a younger stage of development to maltreatment, a condition that is known to affect brain development (Cicchetti & Toth, 2005). One could hypothesize that the associations found in the present study between sleep and placement age or time spent in the foster home may be explained by child age. Because age was included as a covariate, the variance pertaining to child age was excluded from the equation, suggesting that placement age and time spent in the foster home have a unique influence on sleep.
Limitations
This study has several limitations that are important to note. First, the assessment of child sleep relied on foster mother report. Given that foster mothers may underestimate children sleep disturbances (Tikotzky & Sadeh, 2001), further studies should include objective measures of sleep. Second, because of the cross-sectional nature of our data, the directionality of our findings is subject to debate. Third, the relatively small number of participants affected statistical power. It will be important to replicate the study findings on a larger sample and to follow children over a period of time to assess change in foster children sleep.
Conclusion
The current exploratory study sheds light on sleep quality and habits of young children placed in foster care after being exposed to child maltreatment. Age at initial placement, number of placements, past experiences of sexual abuse and neglect, and foster caregiver’s level of parenting stress were all associated with poor quality of sleep. The significance of our findings is strengthened by the medium to large effect sizes, indicating statistical robustness despite the small sample size. Considering the impact of sleep disturbances on multiple aspects of development, sleep disturbances could exacerbate developmental problems in foster children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This was not an industry-supported study. This research was supported by grants received from the Fonds de recherche du Québec – Société et culture (FRQ-SC).