
Abstract
The current study adapts the Information-Motivation-Behavioral Skills (IMB) model of health behavior to injection drug using risk behaviors and risk for Hepatitis C (HCV). Briefly, this model postulates that prevention behaviors are directly influenced by an individual’s knowledge about a disease, their motivation to avoid the disease and their skills and capacity to engage in prevention behaviors, while information and motivation also directly influence behavioral skills. Scales for HCV information, motivation and behavioral skills were included in the New Orleans arm of the National HIV Behavioral Surveillance (NHBS) of Injection Drug Use study. A structural equation model was tested on a sample of 108 current injection drug users recruited in December 2012. Results showed good fit of the IMB model. Although participants had high levels of information and knowledge about HCV transmission, information was not found to relate to either behavioral skills or needle sharing. Higher levels of skills were directly related to lower levels of needle sharing. In addition, motivation had an indirect effect on needle sharing that was mediated through skills. Many approaches to HIV and HCV prevention focus on increasing awareness and information about HIV and risk behaviors. This model, however, appears to indicate that increasing awareness may not be as effective as interventions or programs that increase behavioral skills or motivation coupled with skills building. Although some HIV/STD prevention interventions, such as motivational interviews do attempt to capitalize on this relationship, more efforts should be made to incorporate this important link into high impact prevention programs.
Keywords
Hepatitis C (HCV) remains a serious health concern globally and within the United States. In the United States alone, it has been estimated that more than three million people are living with chronic HCV (Centers for Disease Control and Prevention [CDC], 2012; Ly et al., 2012) and that annual mortality due to HCV has now surpassed deaths due to HIV (Smith et al., 2012). Although the CDC has declared HCV a generalized epidemic and recommends screening for persons above 55 (Smith et al., 2012), injection drug use remains the main route of transmission for HCV. Prevention of and understanding needle sharing and other unsafe injection practices therefore is critical to reducing the spread of HCV.
J. D. Fisher and Fisher (1992) originally proposed the Information-Motivation-Behavioral Skills (IMB) model describing HIV prevention behaviors. This model postulated a direct relationship between HIV prevention behaviors and three independent constructs (factors). The first construct is the amount of prevention-related information an individual possesses, such that information about prevention behaviors is a necessary but not sufficient condition for engaging in the behaviors themselves. Second, motivation to engage in prevention behaviors increases the likelihood of performing the behavior. Finally, an individual’s skill in performing the behavior is directly related with behavioral completion. In addition to these direct paths, the effect of information and motivation is mediated through behavioral skills such that both may affect skill acquisition and therefore behavior.
A number of studies conducted in a diverse variety of populations have demonstrated the success of this model in describing these factors and their relation to HIV prevention behaviors most commonly using condom use (Bryan, Fisher, Fisher, & Murray, 2000; Cai et al., 2013; Crosby et al., 2008; Walsh, Senn, Scott-Sheldon, Vanable, & Carey, 2011) or adherence to antiretroviral medication (Ferrer, Morrow, Fisher, & Fisher, 2010; J. D. Fisher, Amico, Fisher, & Harman, 2008; Starace, Massa, Amico, & Fisher, 2006) as behavioral outcomes. Although initially developed within the context of HIV prevention behaviors, the model has also been successfully generalized to a number of health-related topics including sexual and reproductive health such as HPV vaccination (W. A. Fisher, 2012), abstinence (Bazargan, Kelly, Stein, Husaini, & Bazargan, 2000), as well as broader general health topics including nutrition, diabetes, and dieting behaviors (Gao, Wang, Zhu, & Yu, 2013; Goodell, Pierce, Amico, & Ferris, 2012; Osborn & Egede, 2010), tuberculosis (Peltzer, Naidoo, Matseke, & Zuma, 2011), substance use, and smoking cessation (Shell, Newman, Perry, & Folsom, 2011).
Some of these studies have met with limited success at demonstrating all theorized relationships (i.e., paths) predicted by the IMB model leading some to suggest that the utility of the model is best suited as a framework for intervention development (Kalichman, Picciana, & Roffman, 2008). Many studies have either adapted portions of the model for use in intervention research (Konkle-Parker, Amico, & McKinney, 2014; Kudo, 2013; Laisaar, Uuskula, Sharma, DeHovitz, & Amico, 2013) or used path analytic approaches to test the relationships in the model (Amico, Toro-Alfonso, & Fisher, 2005). Few studies have applied the model to specific risk factors of needle sharing and unsafe injection practice. None, however, have included needle sharing behavior or hepatitis disease risks as outcome constructs. The purpose of the current study then is to adapt the IMB model to injection behaviors and HCV risk and to test the fit of the resultant model within a structural equation modeling (SEM) environment.
Method
Participants
Five hundred four persons who inject drugs were surveyed as part of the New Orleans Louisiana arm of the CDC NHBS system during August to December 2012. Eligibility requirements were that participants were 18 years of age or older, were a residents of the New Orleans seven parish metropolitan area, were able to take the survey in English, and had injected drugs within the past 12 months. Current injector status was carefully screened using visible signs of recent injection and/or detailed knowledge of injection practice.
Recruitment
Participants were recruited through the NHBS of Injection Drug Use study using respondent driven sampling (RDS) procedures, which have been described elsewhere (Lansky et al., 2007). RDS is a modified chain referral approach that uses a dual incentive structure, which has been shown to have success recruiting members of hidden populations such as persons who inject drugs (Abdul-Quader et al., 2006; Robinson et al., 2006). Following these procedures, a set of eight known members of the target population acted as initial “seeds,” were surveyed, and were offered a free HIV and HCV test. Each seed was then given the opportunity to recruit up to five members of their social network who were known by them to be current injectors. Each respondent was then also surveyed, offered an HIV test, and given the opportunity to recruit up to five respondents. Recruitment proceeded in this fashion until both a sufficient number of waves to reach equilibrium and the desired sample size was reached. Respondents received a US$20 value gift card for survey participation and an additional US$20 gift cart for HIV testing. An additional US$10 gift card was provided for each successfully recruited additional respondent.
Instruments
The NHBS core survey instrument was administered to each participant. The approximately 40-min survey covers a wide spectrum of questions on sexual behavior, substance use, and HIV testing behaviors as indicators of HIV risk. An additional set of scales for the information, motivation, and behavioral skills constructs were developed by adapting items from the literature. These items were asked to a subset of respondents during the last month of the survey; therefore only the 108 individuals who completed the survey in December 2012 were used for purposes of these analyses.
HCV transmission information (Cronbach’s α = .64) was indicated by a set of five knowledge items on the ways HCV is transmitted adapted from Balfour’s HCV knowledge scale (Balfour et al., 2009). Although some IMB studies have conceptualized the information factor as containing domains of prevention knowledge as well as generalized knowledge about the disease of interest, only transmission information was included in this study. Questions were a set of statements such as ‘HCV is a virus transmitted by blood’ that participants were asked to rate as true or false. Correct answers were coded at unity while incorrect answers and responses of “don’t know” were coded as zero. Table 1 presents all question wording.
Questionnaire Item Means, Standard Deviations, and Ranges.

Note. HCV = Hepatitis C virus. Original wordings are underlined.
Motivation (Cronbach’s α = .74) to avoid HCV infection included four items such as “I would never share needles or works with anyone who had hepatitis.” These items were coded on a 5-point Likert-type scale of agreement (i.e., 0 = strongly disagree; 1 = disagree; 2 = neither agree nor disagree; 3 = agree; 4 = strongly agree).
The HCV Behavioral Skills scale (Cronbach’s α = .87) consisted of five Likert-type items on perceived behavioral control of personal injection practices adapted from Kang, Deren, Andia, Colon, and Robles (2004). Example questions included “I am sure that I could always use a clean needle to inject with.” Questions were worded such that higher scores reflected greater certainty in risk behavior avoidance (0 = very unsure, 1 = unsure, 2 = neither sure nor unsure, 3 = sure, 4 = very sure).
The endogenous risk construct of the IMB model was defined in terms of Needle Sharing Behaviors (Cronbach’s α = .86), which was operationalized by four core survey items describing frequency of sharing needles, sharing injection equipment, sharing cotton, and sharing water. Each item was measured on a 5-point Likert-type scale with end and midpoints describing frequency of each behavior within the past 12 months (1 = never, 2 = rarely, 3 = about half the time, 4 = most of the time, 5 = always). Higher levels indicate more frequent risk behaviors (e.g., “In the past 12 months how often did you use needles that someone else had already injected with?”).
Each respondent was also offered a free rapid HIV test with a Clearview Complete HIV-1/2 screening performed on blood obtained by fingerstick, which was followed by confirmatory Western blot if needed. Respondents were also offered a rapid OraQuick Rapid HCV antibody screening test. Based on the result of the rapid HCV test and self-reported previous HCV diagnosis, HCV status was collapsed into a single categorical variable (HCV negative, previous HCV positive, newly detected HCV). All respondents received the results of their HIV and HCV screening tests and appointments were made for individuals who received confirmatory exams to receive their results within 2 weeks. All participants received appropriate referrals for services based on the responses to the survey and test results.
Analyses
The hypothesized IMB model was tested using Mplus Version 7 (Muthen & Muthen). Figure 1 displays a graphic representation of the model with the two covarying exogenous constructs of information and motivation with direct paths leading to the behavioral skills and risk behavior constructs. In addition, direct paths from behavioral skills onto risk behavior and from risk behavior to HCV disease outcome were included. Total, direct and indirect effects from information and motivation onto risk were assessed. Because the model included dichotomous items identifying the information construct and the categorical disease outcome measure, robust weighted least squares (WLSMV) estimation methods were used to obtain model estimates. The specified model was overidentified with 58 degrees of freedom and converged normally.

IMB structural model of injection-related risk and HCV infection.
Results
Respondent Characteristics
The majority of respondents were male (76%) and the average age was 43. Fifty-nine percent of respondents were African American, 34% were White, and 3% were Hispanic. Previously diagnosed HIV positive individuals comprised 6.5% of the sample, and 1.8% were newly identified based on HIV confirmatory testing. One quarter of participants (25%) had been ever told by a doctor that they had HCV (also confirmed by screening), and 29.6% were newly detected HCV cases. Table 2 presents the full correlation matrix between indicator variables.
Inter Item Correlation Matrix of Manifest Variables in the IMB Structural Model.
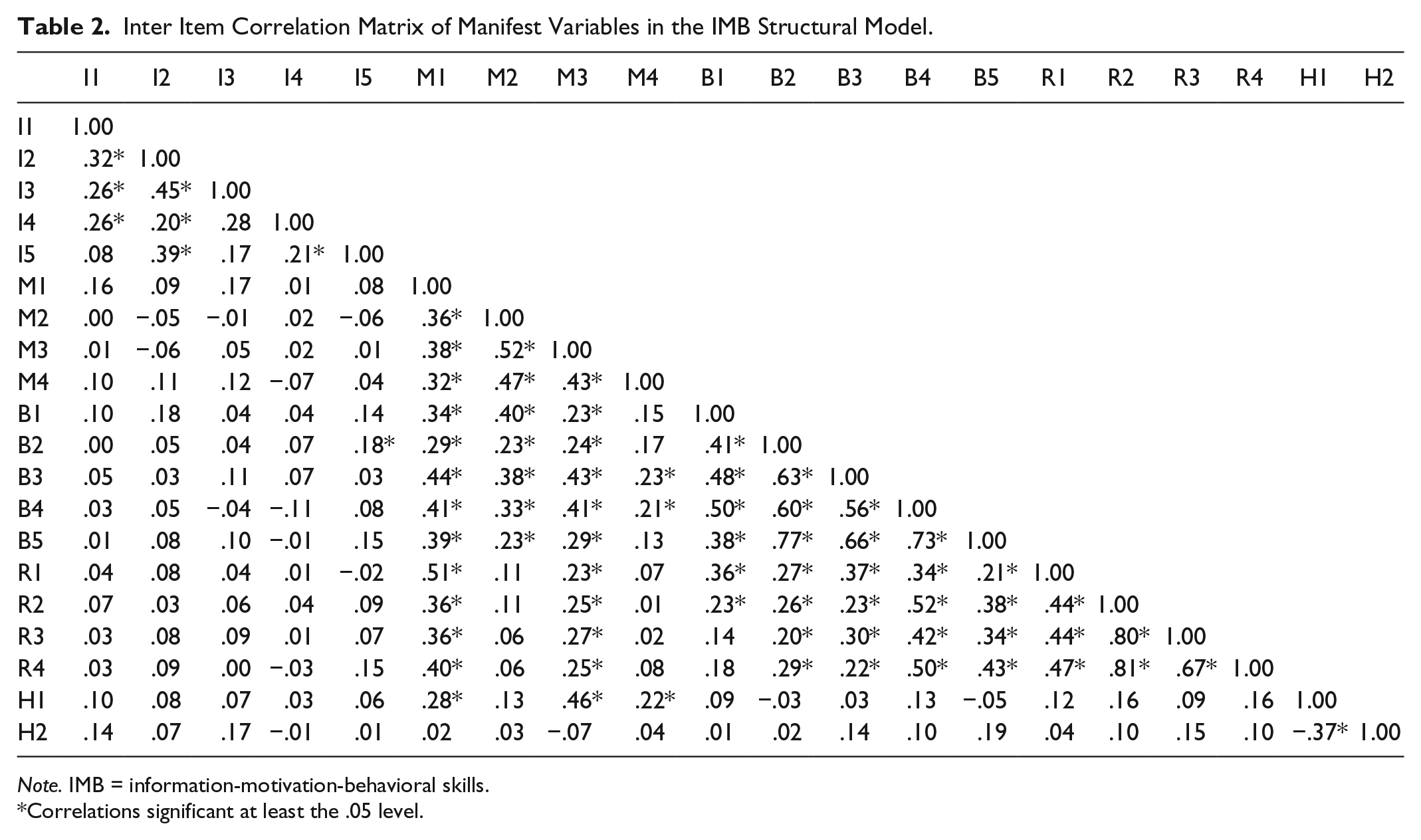
Note. IMB = information-motivation-behavioral skills.
Correlations significant at least the .05 level.
Measurement Model
The overall model fit was good with several standard measures indicating good fit of the model. Chi-square for the initial model was not significant at the .05 level, χ2(146) = 166.6, p = .11. Also comparative fit index (CFI = .908) and Tucker–Lewis fit index (TLI = .892) were adequate. The root mean square error of approximation was .036 (confidence interval [CI] = [.000, .06]), which was both less than .05 and satisfied the tests of closeness of fit (p = .815) and exactness of fit. All paths from latent constructs to the manifest indicators in the measurement model were found to significantly load on their respective construct with the exception of the previously diagnosed HCV variable (H1 see Figure 1).
Structural Model
The standardized direct structural path from the behavioral skills construct (γ = −.42, SE = .12, t = −3.38, p < .001) to the injection risk construct was found to be significant (see Figure 1). Motivation directly influenced behavioral skills (γ = .58, SE = .07, t = 7.65, p < .001) but was not significantly related to injection risk through the direct pathway (γ = −.16, SE = .14, t = −1.13, p = .255). The total direct and indirect contribution of motivation on injection behavior was significant, however (γ = −.24, SE = .08, t = −3.16, p = .002). Information was not found to be significantly related to either behavioral skills or the needle sharing risk behavior, nor did it covary with motivation. Injection-related sharing behaviors significantly predicted hepatitis infection (γ = .32, SE =.12, t = 2.61, p = .009).
Removal of the non-significant knowledge structural paths did not significantly improve the fit of the model, χ2(3) = 2.43, n.s., and was not called for by modification indices, therefore only the original model is presented here.
Discussion
The current study adapts the Information Motivation Behavioral Skills model of HIV prevention behaviors to hepatitis risk and injection practice. Overall fit of the model was good. The structural paths from behavioral skills as well as the mediational path from motivation through behavioral skills were found to be significant while knowledge did not meaningfully contribute to the structural model. Furthermore, the path from HCV risk behaviors to detection of HCV through a rapid screening procedure was found to be significant.
One interesting aspect of this study may be the inclusion direct measures of HCV disease status as well as behavioral risk factors as outcomes in an IMB SEM model. An exploratory model including the additional outcome of HIV infection was considered, however, was discarded because all question domains were specific to HCV rather than HIV risk and infection and because inclusion of the HIV indicator led to linear dependencies within the model due to small cell sizes.
Although the current model fit the data adequately, some weaknesses of the current study should be noted both in terms of methodology as well as measurement. These include the standard methodological issues with self-report and cross sectional nature of the NHBS parent study. This is especially relevant given the possible differential in timeframes between HCV infection and risk behavior in the past 12 months. It should also be noted that, while the RDS sampling procedure should yield asymptotically correct population parameter estimates after applying adjustments for homophily and network size (Heckathorn, 2002), these adjustments were not made. This was due to the fact that the additional IMB questions were administered to a subset of respondents thus interrupting the recruitment chains needed to achieve the equilibrium needed by RDS estimation procedures. Furthermore, the primary interest in this study is to model the associations between manifest variables and underlying factor patterns rather than the point prevalence estimates and methods for adjusting these correlational measures have not yet been fully developed.
In terms of measurement error, other studies using longer scales have shown higher reliability as well as lower levels of HCV knowledge in the injection population (Heimer et al., 2002; Larios et al., 2014; Strauss et al., 2007). This low difficulty of items may have resulted in range restriction and could have contributed to the lack of observed relationship between the knowledge construct and other hypothesized factors. J. D. Fisher and Fisher (1992) specifically caution about this, warning that specialized knowledge in high risk populations may make finding this relationship difficult stating,
Finally, in some relevant populations (e.g., urban gay men who belong to homophile organizations, college students), extant levels of the type of knowledge measured on such ecologically invalid instruments are extremely high, and ceiling effects make a knowledge-prevention relationship difficult to detect.
Furthermore, it is possible that the factors as measured in this study did not fully capture the domains of the IMB model. For example, information was operationalized specifically as knowledge about HCV transmission whereas the construct has been conceptualized elsewhere as more global disease-related knowledge. Similarly, the motivation construct was indicated by items that centered more heavily on behavioral intentions and less so on other domains such as social norms. Finally, the behavioral skills items have also been operationalized differently in other studies in that these questions are related to perceived behavioral control (i.e., “How sure are you . . . ?”) rather than perceived ability (i.e., “How easy would it be . . . ?). Ultimately, the current study provides valuable information on the utility of the IMB model in describing the relationships between a person’s motivation, knowledge, and behavioral skills to avoid injection risk behaviors. Other studies have begun to examine socio-cognitive models such as this in closer detail and even comparing models side by side (Espada, Morales, Gullen-Riquelme, Ballester, & Orgiles, 2016).
Implication of this work highlights the value of increasing a person’s perceived efficacy and capacity to negotiate refusal to share needles and injection equipment. Similarly, addressing motivation may be key to reducing injection-related risk behaviors. Some STD and HIV interventions that are focused on sexual behavior have already used techniques including motivational interviews to this end with some success (Fishbein et al., 2001; Hackler, Pinho, & McKinnon, 2013; Jaworski & Carey, 2001; Kalichman et al., 2005). Other interventions on prevention sharing behaviors could be developed or adapted to increase motivation and behavioral efficacy to avoid risk.
Footnotes
Author’s Note
The contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention (CDC).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The author would like to acknowledge support through the Centers for Disease Control and Prevention (CDC) for National HIV Behavioral Surveillance (NHBS) Cooperative Agreement 5U1B/PS003252.